
ABSTRACT
The Pulfrich phenomenon, originally described in normal observers, is a treatable disorder of the perception of movement in depth in cases of unilateral or asymmetric optic neuropathy. Treatment is highly bespoke and factors influencing treatment response and failure remain unclear. We assessed 25 adults with suspected Pulfrich phenomenon due to a range of conditions in two tertiary referral centres. Monocularly tinted spectacles were successful in reducing symptoms of the Pulfrich phenomenon under daylight conditions in nine subjects, eight of whom had optic neuritis. These spectacles were not effective at night and in patients with visual field defects due to ischaemic optic neuropathy, glaucoma, optic disc drusen or severe peripapillary retinal nerve fibre loss on optical coherence tomography.
Introduction
Impaired perception of movement in depth is a visual illusion which was discovered by Carl Pulfrich, a German physicist and renowned expert on stereoscopy.Citation1,Citation2 A normal subject perceives an object (e.g. a pendulum swinging from side to side) moving along an illusory 3D pathway because of an inter-eye discrepancy of illumination.Citation1,Citation3 The difference in retinal illumination (usually achieved by placing a neutral density [ND] filter in front of one eye) results in a difference in the time course of retinal processing, with the increased latency in the filtered eye resulting in an apparent displacement in depth of an object moving in the fronto-parallel plane.Citation4 This displacement is exaggerated with a darker filter as the disparity in retinal illumination between the two eyes is further increased (see A&B).Citation1,Citation5,Citation6
Figure 1. (A) Illustration of the Pulfrich phenomenon and how the pendulum is perceived either closer or further away than it really is. (B) The Pulfrich phenomenon viewed obliquely. An object moving in the plane AB to the viewer’s left approaching the filtered eye is perceived as travelling along the plane CD towards that eye.
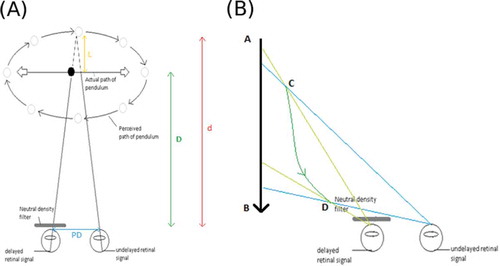
The magnitude of the displacement has been shown to increase as object velocity is increased.Citation7,Citation8 As the pendulum motion is fastest at the centre of the swing, the apparent displacement will therefore be greatest at this point. The displacement is zero when the pendulum pauses momentarily before switching direction, which results in the perception of an elliptical path followed by the object.Citation1,Citation4 The curve of the ellipse is perceived to be nearer to the observer when the object is moving toward the covered eye and further from the observer when moving toward the uncovered eye.Citation1,Citation6
The latency or lag distance between the eyes can be calculated using the following equation:
where L = latency or lag distance behind the unfiltered eye, D = distance from viewer to actual pendulum, d = distance from actual to apparent position and PD = subject inter-pupillary distance (see ).
A crucial factor in visualising the provoked Pulfrich phenomenon is the structure of the background to the object. The viewer’s eye movements track the motion of the pendulum and this movement in conjunction with the viewer simultaneously observing a stable background results in this displacement. The background requires features enabling the exploitation of disparity in order to achieve the illusion of depth and for the Pulfrich effect to be optimally demonstrated.Citation9
The Pulfrich phenomenon has been found to occur in individuals with ocular or neurological conditions in which the visual pathway or retinal illumination is affected. During typical binocular viewing, the eyes are separated by approximately 6 cm resulting in a disparity as the two eyes perceive the world slightly differently. This normal degree of disparity allows dynamic three-dimensional viewing as images are fused into a single percept to provide single vision and stereopsis.Citation10 However, dynamic visual perception is compromised if the rate of input of information from either optic nerve is not the same. If conduction along one optic nerve is slower (as can be demonstrated by a delay in the visual evoked potential, VEP) than the other, for example, then moving objects are seen to have illusory trajectoriesCitation10 (see A&B). Experimentally, a delay in VEP latency can also be achieved by use of ND filters.Citation11 A grey filter, like an ND filter, reduces the intensity of all wavelengths equally, giving no change in the colour of the perceived image. For example, a particular grey filter might transmit 50% of the visual spectrum ( A&B). Another filter, for example a green filter, transmits more of the green part (around 510 nm) of the spectrum than of the other parts (red and blue). A green filter would change the perception of the image by interfering with the colour of the image. ND filters delay VEP latency less than 40 m/s between ND = 0 (transmission 100%) and ND = 1.5 (transmission 3%).Citation12
The Pulfrich phenomenon gives rise to symptoms that can be disturbing and cause difficulties with tasks involving judgement of moving objects, such as playing certain sports, crossing roads or driving.Citation6 Conditions which have previously been found to elicit these symptoms include optic neuritis, cataract and anisocoria.Citation5,Citation13 It has been reported that the Pulfrich phenomenon can be managed with a tinted lens in front of the better eye, for example with the use of uniocular tinted spectacles or a tinted contact lens.Citation13 The principle behind this being that the retinal illumination reduction from the tinted lens or filter in the better eye counteracts the disparity from the other eye. Here, we revisit the effect of a monocular ND filter as a management option for patients presenting with symptoms of the Pulfrich phenomenon.
Materials and methods
Patients were recruited from two centres, Moorfields Eye Hospital (MEH) NHS trust and the VU Medical Centre Amsterdam between May 2013 and July 2017. The study was in accordance with the World Medical Association (WMA) Declaration of Helsinki and national ethics (http://www.ccmo.nl/nl/uw-onderzoek-wmo-plichtig-of-niet) and approved by MEH Research and Development (study ID: ROAD 17/036).
All participants were adults who reported difficulties with visual perception of movement in depth. All participants were assessed for the best corrected visual acuity (BCVA given in LogMAR), colour vision, visual fields, pupil reactions and retinal optical coherence tomography (OCT) following consensus guidelines.Citation14
The Pulfrich effect was assessed in the MEH Optometry department or the AMC Orthoptic department. The Pulfrich assessment consisted of a questionnaire relating to typical Pulfrich symptoms and appropriate refractive error was worn before presenting the swinging pendulum.
There is no validated questionnaire for assessment of the Pulfrich phenomenon or its implications for a patient’s quality of life (QoL). Even the 25 vision targeted questions of the NEI-VFQ-25 which is widely used in ophthalmological research do not specifically address difficulties with this potentially disabling visual illusion.Citation15 In the absence of a validated outcome questionnaire for the Pulfrich phenomenon, we therefore attempted to collect anecdotal information from patients on what daily activities are affected. This was done by interview in clinic and in-house questionnaires. The questionnaire addressed difficulties for acquired perception of movement in depth as relevant for daily living activities: escalators, pouring liquids, traffic, handling objects, sports, writing, doors, locks, cupboards, walking, details and ability to watch 3D films. For each of these domains, feedback was requested after treatment.
Pulfrich test setup
Presence of the Pulfrich phenomenon was assessed by demonstrating a swinging weighted pendulum (fishing weight on a line) against a 300 cm × 90 cm background picture (London, ) or a black-white pattern background (Amsterdam, ) viewed from 3 m. A patterned background was used because this had been reported to be preferable to a non-patterned stimulus.Citation9
Figure 2. (A) Photograph of Pulfrich experimental test material at Moorfields Eye Hospital. A coloured jungle scene with a monkey (green arrow, still on this photograph) is shown. (B) Photograph of Pulfrich experiment at VU Medical Centre Amsterdam. A black and white tablecloth is shown with a swinging black ball (green arrow, in motion giving impression of a blur on this photograph).
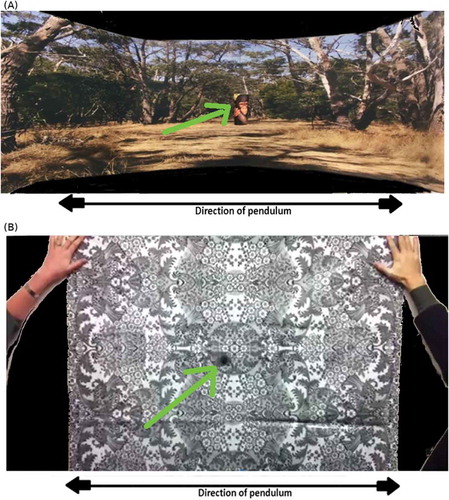
Appropriate refractive correction was worn. The pendulum was a monkey faceCitation16 in London and a plain black ball in Amsterdam. Pulfrich-positive patients were identified as those who reported a circular or rotational movement of the pendulum while in their habitual visual state, as opposed to a veridical linear movement.
Those who experienced the Pulfrich effect were shown a selection of ND filters in front of the better eye and the most effective filter decided. Filter densities included grey 80% light transmission factor (LTF), (0.1 log units), grey 65% LTF (0.2 log units), and grey 50% LTF (0.3 log units). In-house tinted filters were used at MEH and commercially available filters (Zeiss, Jena, Germany) in Amsterdam. A prototype of the spectacles for assessment is shown in . Filters were changed during the assessment and the optimal filter selected based on which density the patient felt gave a linear movement or which gave the least amount of circular or rotational movement. Patients were also asked to move around with their trial spectacles to get a feeling for impact during auto locomotion. Only those whose symptoms reduced were then dispensed uniocular tinted spectacles including a prescription to correct any refractive error where necessary. At MEH, a feedback questionnaire (written/verbal) was completed following a trial period of at least 6 weeks.
Figure 3. Prototype of spectacles for the Pulfrich phenomenon.
Statistical analysis
All statistical analyses were performed using SAS software (version 9.4, SAS Institute, Inc., Cary, North Carolina, USA). Data were assessed visually for normal distribution. Because of non-Gaussian distribution, the non-parametric Wilcoxon test was used for comparing two independent variables. The Chi Square test was used for comparison of categorical variables. The linear correlation between continuous variables was evaluated using the Spearman correlation coefficient. Linear regression analysis was performed using the least squares method. A p value < 0.05 was considered as significant.
Results
The characteristics of the 25 patients included are summarised in . There was no centre effect regarding the demographic data (age, p = 0.47; gender p = 0.65). Presence of the Pulfrich phenomenon could only be demonstrated in 9/25 (36%) patients who reported difficulties with perception of movement in depth. There was no significant centre effect for confirmed Pulfrich cases (p = 0.97). The pick-up rate of the Pulfrich phenomenon was 5/14 (36%) in London and 4/11 (36%) in Amsterdam.
Table 1. Patient characteristics.
Most patients in whom the Pulfrich phenomenon could be demonstrated suffered from unilateral optic neuritis 8/9 (89%). In addition, the Pulfrich phenomenon was present in one patient who suffered from a retinal tear and epiretinal membrane. In all other patients, subjective difficulties with perception of movement in depth could not be explained by the Pulfrich phenomenon or at least our test was not sensitive enough to provide supportive evidence. Neither the questionnaire nor the interview was helpful to identify a core set of questions suitable to reliably identify the Pulfrich phenomenon in all patients (data not shown).
Presence of the Pulfrich phenomenon was not related to age (p = 0.53), inter-eye difference of BCVA (p = 0.61), BCVA in the affected eye (p = 0.7).
In addition, there was no correlation between dyschromatopsia, visual field defects or presence of an RAPD in demonstrating the Pulfrich phenomenon.
Retrospectively, it emerged that transient gaze evoked visual difficulties in patients with multiple sclerosis were also related to presence of an inter-nuclear opthalmoplegia or an impaired vestibulo-ocular reflex. These patients typically experienced their symptoms either on rapid lateral eye movements for example in traffic or strictly with auto locomotion.
OCT
The median pRNFL in the affected eye was significantly thinner in patients without Pulfrich phenomenon (69 µm, interquartile range [IQR] 52–69 µm) compared to patients in whom the Pulfrich phenomenon was confirmed (88 µm, IQR 73–100 µm; p < 0.01).
Treatment
All patients in whom the Pulfrich phenomenon could be demonstrated were fitted with monocularly tinted spectacles. The grey filter density ranged from 10% to 65%. There was no correlation between filter density and visual acuities, presence of an RAPD or pRNFL thickness. There was a positive correlation of filter density with age (R = 0.73, p = 0.027); therefore, older patients required stronger filters.
All patients with confirmed Pulfrich phenomenon noted an improvement on treatment with a ND filter. In one patient, recovery from optic neuritis continued and her Pulfrich phenomenon resoled spontaneously rendering tinted spectacles unnecessary. Improvement was marginal in the one patient with the retinal tear and epiretinal membrane.
The patient reported outcomes frequently mentioned improved perception of the floor, such as
“Floor comes up less and very helpful with stairs”.
“Found taken away feeling of floor being uneven”.
Two patients commented that the effect was better in bright compared to dim light. One patient also found tinted spectacles to help with walking on a busy pavement putting keys into locks and credit cards into machines as well as judging moving objects. At 18 months follow-up, she was so satisfied with daily use of the unilateral tinted spectacles that she requested them to be incorporated into a new set of spectacles, which she required because of change of refraction.
Discussion
The data presented come from a comparatively large case series of patients suffering from impaired perception of movement in depth compared to earlier reports (four cases in referenceCitation5). We found that tinted spectacles could be helpful only in a minority of our participants, most of whom suffered from optic neuritis.
Our prevalence figure of Pulfrich phenomenon in 36% of those reporting difficulty with depth was less then what was expected from the literature.Citation5 However, this may be caused by the broad inclusion criteria and the rigorous assessment requiring that only those patients who gave unambiguous responses when shown the swinging pendulum and had a corresponding improvement with a precise ND filter were categorised as suffering from the Pulfrich phenomenon. Only these patients were issued with trial spectacles. If present, the Pulfrich phenomenon affected almost exclusively patients with optic neuritis. Only one patient with alternative pathology, a retinal tear, reported marginal improvement. This was consistent with a previously reported case of retinal detachment.Citation17 Patient with severe unilateral optic atrophy as quantified by pRNFL thickness on OCT did not experience the Pulfrich phenomenon. This suggests that patients successfully achieved suppression of the image from the worse eye for perception of motion in depth.
Two of the patients who found the uniocular tinted spectacles helpful found them less so in dimmer lighting. The Pulfrich effect has been shown to increase greatly during dark adaptation as the perceptual latency increases.Citation18 It is possible that the spectacles will be less useful under mesopic (twilight) and scotopic (dark) conditions due to the onset of dark adaptation. Alternative explanations include insufficient density of the tint in darker conditions or increased difficulty with visibility when viewing through a tinted lens in the dark. To the best of our knowledge, this limitation of efficacy of the treatment for Pulfrich phenomenon has not been described before. We think it is relevant particularly for those patients who use the spectacles for driving, as they need to be aware that the effect will diminish with twilight and in dark.
One limitation of our study is that assessment of stereopsis was only performed systematically in Amsterdam. This may be relevant to prediction of treatment response. Likewise, we were unable to identify a reliable set of questions which clearly identify the phenomenon and can be used as an outcome measure for a treatment trial. Clearly, more work will be required to quantitatively assess the implications of the Pulfrich phenomenon for a patients visual QoL.
Another shortcoming of our study is that we have not systematically assessed the influence of pendulum brightness in this study. This may be relevant because brightly lit highly reflective objects have been argued to be best at demonstrating the Pulfrich phenomenon.Citation5 We therefore cannot exclude that the Pulfrich phenomenon could have been confirmed in a larger number of patients. Whether or not increased test sensitivity will have practical implications would need to be tested prospectively. Such future studies should also consider a new grading system for the Pulfrich phenomenon as suggested by the work from the group of Teresa and Elliot Frohman.Citation19
The most commonly documented influence on the effect of the Pulfrich phenomenon is the velocity of the stimulus.Citation7,Citation8 It is reasonable to assume that many of the patients seen may have had true symptoms which were not demonstrated during the Pulfrich assessment as the pendulum did not move at a great enough speed to elicit their symptoms. The velocity of the pendulum was unfortunately not something that could be measured or controlled in the clinic and it is therefore possible that those with milder symptoms were not detected.
Acknowledging these limitations, it should be pointed out that, from a patient’s perspective, the usefulness of unilateral tinted spectacles for their Pulfrich phenomenon in daily life will determine success. Such a pragmatic approach had been adapted in both centres and demonstrates that even with limited resources, testing from Pulfrich phenomenon can be adopted in a clinical setting.
Noteworthy, assessment of the Pulfrich phenomenon was quick, taking less than 10 min per patient. In addition, the patient could be issued with monocular tinted spectacles at very low cost. In fact at MEH, spectacles were tinted in-house and were supplied to the patient. Some may argue that from a cosmetic point of view, the appearance of a unilaterally tinted lens might look unusual. Practically, this only affected one of our patients who then decided to incorporate the tinted spectacles in mirrored lenses to mask the difference.
In conclusion, ND filters can be an effective way of minimising the symptoms of the Pulfrich phenomenon in some patients. Assessment and treatment of the Pulfrich phenomenon may be particularly rewarding in patients recovering from optic neuritis. Patients should be aware that the spectacles will mainly be useful during daylight.
Acknowledgements
The research was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
References
- Pulfrich C. Die Stereoskopie im Dienste der isochromen und heterochromen Photometrie. Naturwissenschaften. 1922;10:553–564. doi:10.1007/BF01571319.
- Petzold A, Pitz E. The historical origin of the Pulfrich effect: a serendipitous astronomic observation at the border of the Milky Way. Neuroophthalmology. 2009;33:39–46. doi:10.1080/01658100802590829.
- Sokol S. The Pulfrich stereo-illusion as an index of optic nerve dysfunction. Surv Ophthalmol. 1976;20:432–434. doi:10.1016/0039-6257(76)90068-0.
- Anzai A, Ohzawa I, Freeman RD. Joint-encoding of motion and depth by visual cortical neurons: neural basis of the Pulfrich effect. Nat Neurosci. 2001;4:513–518. doi:10.1038/87462.
- Heron G, Dutton G. The Pulfrich phenomenon and its alleviation with a neutral density filter. B J Ophthalmol. 1989;73:1004–1008. doi:10.1136/bjo.73.12.1004.
- Heron G, McQuaid M, Morrice E. The Pulfrich effect in optometric practice. Ophthalmic Physiol Opt. 1995;15:425–429. doi:10.1016/0275-5408(95)00054-H.
- Lit A. The magnitude of the Pulfrich stereophenomenon as a function of target velocity. J Exp Psychol. 1960;59:165. doi:10.1037/h0047488.
- Nickalls RW. The influence of target angular velocity on visual latency difference determined using the rotating Pulfrich effect. Vis Res 3. 1996;6:2865–2872. doi:10.1016/0042-6989(96)00039-9.
- Ono H, Steinbach MJ. The Pulfrich phenomenon with eye movement. Vis Res. 1983;23:1735–1737. doi:10.1016/0042-6989(83)90191-8.
- McGowan G, Ahmed TY, Heron G, Diaper C. The Pulfrich phenomenon; clumsiness and collisions which can be ameliorated. Pract Neurol. 2011;11:173–176. doi:10.1136/practneurol-2011-000013.
- Fimreite V, Ciuffreda KJ, Yadav NK. Effect of luminance on the visually-evoked potential in visually-normal individuals and in mTBI/concussion. Brain Inj. 2015;29:1199–1210. doi:10.3109/02699052.2015.1035329.
- Heravian-Shandiz J, Douthwaite W, Jenkins T. Binocular interaction with neutral density filters as measured by the visual evoked response. Optom Vis Sci. 1991;68:801–806. doi:10.1097/00006324-199110000-00009.
- Heron G, Thompson KJ, Dutton GN. The symptomatic Pulfrich phenomenon can be successfully managed with a coloured lens in front of the good eye–a long-term follow-up study. Eye. 2006;21:1469–1472. doi:10.1038/sj.eye.6702459.
- Petzold A, Wattjes MP, Costello F, et al. The investigation of acute optic neuritis: a review and proposed protocol. Nat Rev Neurol. 2014;10:447–458. doi:10.1038/nrneurol.2014.108.
- Raphael BA, Galetta KM, Jacobs DA, et al. Validation and test characteristics of a 10-item neuro-ophthalmic supplement to the NEI-VFQ-25. Am J Ophthalmol. 2006;142:1026–1035. doi:10.1016/j.ajo.2006.06.060.
- http://howafrica.com/wp-content/uploads/2016/06/monkey-meaning-and-symbol.jpg
- Hofeldt AJ, Leavitt J, Behrens MM. Pulfrich stereo-illusion phenomenon in serous sensory retinal detachment of the macula. Am J Ophthalmol. 1985;100:576–580. doi:10.1016/0002-9394(85)90684-1.
- Standing L, Dodwell P, Lang D. Dark adaptation and the Pulfrich effect. Atten Percept Psychophys. 1968;4:118–120. doi:10.3758/BF03209521.
- Sobhanian MJ, Agarwal R, Meltzer E, et al. Identification and treatment of the visual processing asymmetry in MS patients with optic neuritis: the Pulfrich phenomenon. J Neurol Sci. 2018;387:60–69. doi:10.1016/j.jns.2018.01.029.