
Abstract
This study investigated the effect of universal adhesives on the resin composite–composite adhesion for immediate and aged repair with and without air-borne particle abrasion. Composite resin specimens were fabricated by placing multiple increments of resin composite (Clearfil Majesty Posterior) into cylindrical cavities (diameter: 4 mm, height: 2 mm) and photo-polymerized. Specimens (N = 720) were randomly assigned to 4 groups (fresh dry specimens, 24 h and 6 months water storage and thermocycled). These four main groups (n = 180) were further assigned to 2 groups (n = 90) according to the surface conditioning procedures; (a) Al2O3 air-abrasion and (b) No air-abrasion. Then, all subgroups were divided into six subgroups due to the adhesive procedures (a) All Bond Universal: AB (Bisco Inc.), (b) Monobond Plus: MP (Ivoclar Vivadent), (c) G-Premio Bond: GP (GC), Gluma Bond Universal: GB (Heraus Kulzer), Clearfil Universal Bond: CU (Kuraray), Clearfil Universal Bond Quick: SK (Kuraray). All bonding systems were applied according to the manufacturer’s instructions and new composite blocks were bonded to the specimens for shear bond strength testing at the Universal Testing Machine (0.5 mm/min). Al2O3 air-abraded groups showed significantly higher bond strength values compared to non-treated groups (p < 0.0001). CU and SK groups showed higher bond strength values and the worst values were observed for the groups of MP. Conditioning with Al2O3 air-abrasion and silane in universal adhesives improves the bond strength of universal adhesives in composite repair.
Introduction
Adhesive systems have been developed over several decades in order to implement minimally invasive treatment procedures in dentistry. Therefore, to reduce the technique sensitivity that decreases the bonding performance of adhesive systems and to increase monomer diffusion, more simplified materials with fewer steps were established for dentists with improved chemical and mechanical properties, long term adhesive performance and biocompatibility [Citation1,Citation2]. Recently, universal adhesive systems or multi-purpose adhesive systems are known as one-step self-etching systems that are also considered as the eighth generation of adhesive systems. Such adhesive systems are available as a single bottle, requiring no mixing and they could not only be used in the etch and rinse, but also etch and dry and selective-etching mode in adhesive dental treatments [Citation2].
The preference for resin composites in dental clinics became routine with the improvement of adhesive technology. However, resin-based restorations have still some drawbacks such as fractures, chipping kind of failures, or wear, resulting in repair requirement. In cases of failures of a resin composite restoration, the repairing protocol generally provides a conservative technique instead of the replacement of such a restoration. The adhesion between resin layers is realized in the existence of the oxygen inhibition layer [Citation3]. However, during the repairing procedures, it is likely that the resin composite restoration has been exposed to a humid environment for a longer period of time under function. In this situation, it is known that the water saturation of resin composite has been completed and free radical activity has ended. Water sorption of resin composite restorations softens the resin matrix, leads to microcracks and resin degradation [Citation3]. Due to aging, the free radical activity ends and the oxygen inhibition layer disappears.
Several techniques are suggested to enhance the adhesion for repairing resin composites since aged resin composite restorations do not include an unpolymerized layer. These techniques generally include mechanical surface conditioning, the use of silanes and adhesive systems that can enhance the adhesion between the repaired substrate and the repairing resin composites. Increasing the surface roughness [Citation4] can be accepted as surface pretreatment and the other surface treatment options such as the application of silane and the adhesive systems are generally aim to increase the adhesion of filler particles or cross-linked polymer matrix of repaired resin composite [Citation3,Citation5–8]. It has been previously reported that increased surface roughness by using airborne particle abrasion and acid etching is required for better adhesion between resin composite surfaces [Citation4]. Many researchers worked different protocols of aging techniques for better adhesion between the substrate and the repairing resin composites such as thermocycling [Citation9], water storage [Citation10], citric acid immersion [Citation11] and boiling [Citation3].
In the literature, there is no common way for the aging protocol that simulates the intraoral conditions. Water storage is accepted as the most commonly used aging protocol. However, it is known to have detrimental effects because the absorbed water causes hydrolysis and the release of filler particles from the resin matrix [Citation12]. The amount of absorbed water increases over time while the bond strength between resin composites decreases [Citation13]. During thermocycling protocol, water uptake can also degrade the physical and structural features of resin composites which are considered a more aggressive aging method [Citation12].
The objective of the present investigation was to assess the influence of multimode adhesives on the resin composite–composite adhesion for immediate and aged repair with and without air-borne particle abrasion. The following null hypothesis tested were tested: (a) there would be no significant difference between the aging procedures in terms of bond strength, (b) Al2O3 air-borne particle abrasion would have no effect on shear bond strength of repaired resin composites and (c) there would be no significant difference between the adhesive systems in terms of bond strength.
Materials and methods
The brands, chemical compositions and manufacturers of the materials used in this study are listed in . The distribution of experimental groups based on the substrate type and test methods and sequence of experimental procedures are presented in .
Figure 1. Flow-chart showing experimental sequence and allocation of groups regarding combinations of the adhesives and surface treatments.
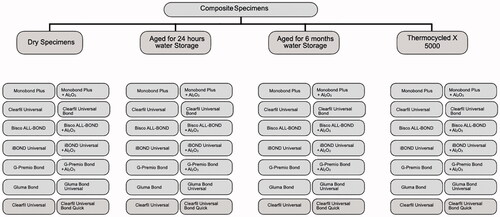
Table 1. Brands, abbreviations, manufacturers and chemical compositions of the materials used in this study.
Specimen preparation
Standardized disc-shaped resin composite substrates (Clearfil Majesty Esthetic, Kuraray, Japan) of 2 mm height and 4 mm diameter were prepared using cylindrical hollow stainless-steel. Teflon molds were set on a glass plate in order to get a flat surface of the specimen after polymerization and resin composites were carefully condensed into the hole to a height of 4 mm. A mylar strip was used to achieve flat-surfaced specimens. Polymerization of the resin composite specimens was achieved using a light-emitting diode (LED) polymerization device for 20 s (LED Elipar 2, 3 M ESPE, St. Paul, USA). The light intensity of the polymerization unit was higher than 800 mW/cm2, and the intensity was measured with a radiometer (Optilux Model 100, SDS Kerr Danbury, USA) after every 32 resin composite specimens. After the preparation of the substrates, the specimens (N = 720) were randomly assigned into 4 main groups: (a) fresh dry, (b) 24 h water storage, (c) 6 months water storage and (d) thermocycling
Aging procedures and surface conditioning
In the first group, adhesive procedures were performed immediately on the substrate surfaces. In the second and the third groups, the specimens were stored in distilled water at 37 °C for 24 h and 6 months, respectively. Thermal cycling (5000 cycles, 5–55 °C, dwell time: 20 s, transfer time: 10 s) was applied to the fourth test group prior to conditioning procedures.
These four main groups (n = 180) were randomly divided into 2 subgroups (n = 90) according to the surface conditioning procedures: Al2O3 air-abrasion group and the specimens that were not treated. Air-abrasion was performed perpendicularly with 50 μm Al2O3 at a distance of 10 mm at 2.8 bar air pressure (AirSonic Mini Sandblaster, Hager Worldwide, Inc., Hickory, USA) for 4 s [Citation14,Citation15]. Following air-abrasion procedures, the sand remnants were removed with air-blow.
Application of adhesive systems
All of the adhesive systems (All Bond Universal: AB (Bisco Inc., IL, USA), G-Premio Bond: GP (GC, Tokyo, Japan), Gluma Bond Universal: GB (Heraus Kulzer, Germany), Clearfil Universal Bond: CU (Kuraray, Tokyo, Japan), Clearfil Universal Bond Quick: SK (Kuraray, Tokyo, Japan) and the primer Monobond Plus: MP (Ivoclar Vivadent, Schaan, Liechenstein) were applied according to the manufacturer’s recommendations for the repair of resin composite. Following polymerization of the adhesives, a teflon matrix with the same dimensions of the repairing resin material (height: 2 mm; diameter: 4 mm) was placed over the aged resin composite specimens and filled in two increments with the repair composite (Clearfil Majesty Esthetic, Kuraray, Japan). Resin composites photo-polymerized with the same polymerization device for 20 s for each increment and the repair resin composite specimen was removed from the matrix with slight pressure. One operator completed all adhesive procedures.
Shear bond strength test
For the shear bond test, the specimens were mounted in the jig of the Universal Testing Machine (Shimadzu Autograph AGS-X, Japan) and the shear force was applied using a shearing blade to the adhesive interface until failure occurred. The load was applied to the adhesive interface, as close as possible to the surface of the substrate at a crosshead speed of 0.5 mm/min. The maximum load (N) was converted into megapascal (MPa) by dividing it by the bonding surface area of the resin cement.
Statistical analysis
The statistical analysis was executed using the statistical software (SPSS Software V.20, Chicago, IL, USA). Three-way analysis of variance (ANOVA), Bonferroni correction, and Tamhane’s T2 tests were used where the bond strength was the dependent variable and substrates types (2 levels: aged versus non-aged), conditioning method (air-abrasion versus no abrasion) universal primer systems (6 levels: AB, GP, GB, CU, SK, MP) as the independent variables. p-Values less than 0.05 were considered to be statistically significant in all tests.
Results
The mean shear bond strength values (MPa) of all tested groups in the present study are shown in . The results from 3-way ANOVA indicated a statistically significant effect of each factor namely, ‘aging procedures’, ‘surface treatments’ and ‘adhesive systems’ (p < 0.0001). Interactions were significant between the two factors ‘aging procedures’ and ‘adhesive systems’, ‘surface treatments’ and ‘adhesive systems’ and the three factors ‘aging procedures’, ‘adhesive systems’ and ‘surface treatments’ (p < 0.0001). There were no significant interactions observed between ‘aging procedures’ and ‘surface treatments’ (p = 0.283).
Table 2. The mean shear bond strength values (MPa) of all experimental groups.
Regarding the effect of aging procedures, the mean bond strength values of the thermo-cycled groups were significantly higher than those of the groups incubated in 37 °C distilled water for 24 h (p < 0.0001) or for 6 months (p = 0.0001). There were no significant differences between 24 h and 6 months of water storage (p = 0.163). Fresh dry specimens presented the lowest mean bond strength values but there were no significant differences between these specimens after 24 h or 6 months of water storage.
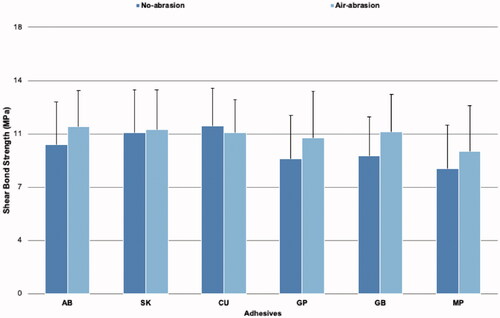
As regards to surface treatments, Al2O3 air-abraded groups showed higher bond strength values than non-treated groups (p < 0.0001). AB, CU and SK adhesive systems showed higher bond strength values and the worst values were observed for the groups of MP (p < 0.0001).
Considering the interaction between the two factor ‘aging procedures’ and ‘adhesive systems’, the lowest bond strength values were observed for MP applied on fresh dry specimens. CU and AB applied on thermocycled specimens showed higher bond strength values (). Considering the interaction between the two-factor ‘surface treatments’ and ‘adhesive systems’, while MP applied onto non-treated specimens showed decreased bond strength values, AB applied on Al2O3 air-abraded groups presented the highest bond strength values ().
Figure 2. The mean shear bond strength values (MPa) of all groups as a function of aging procedures and adhesive systems.
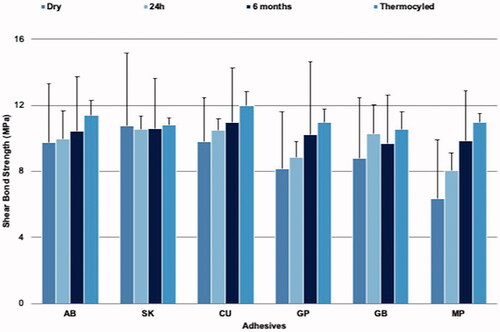
Figure 3. The mean shear bond strength values (MPa) of all groups as a function of surface conditioning and adhesive systems.
Discussion
In reparative dentistry, meaning e repair of restorations instead of replacement, for successful resin composite repair procedures, achieving reliable adhesion to the resin composite restoration is the most important factor [Citation16]. Although several repairing procedures are recommended for resin composite restorations, some drawbacks are still reported [Citation17,Citation18]. Several techniques are used to improve the adhesion of repaired restorations such as chemical adhesion and mechanical interlocking of resin composite restoratives but there is no certain agreement about the protocol or materials that should be used for repairing procedures [Citation17,Citation18]. Thus, it was relevant to estimate the effect of different surface conditioning protocols and adhesive procedures on the fresh and aged resin composite restorations repaired with conventional resin composites. The present study examined the effect of universal adhesives on the resin composite–composite adhesion for immediate and aged repair with and without airborne particle abrasion with shear bond strength tests.
Repair procedures are generally evaluated in vitro based on different bond strength measurement methods all representing specific stress distributions that make comparisons difficult [Citation19]. It was mentioned in the literature that the shear bond strength test revealed clinically more relevant than the other tests such as tensile or flexural tests since elements of shear stresses mostly occur during chewing function. Consequently, a shear bond test was preferred in the present study [Citation20].
Regarding the aging procedures, significant variations in shear bond strength values were found and thus, the first null hypothesis of the present study that there would be no differences in bond strength between different aging procedures, could not be accepted. The repair performance between aged and freshly polymerized resin composite restorations generally are related to several factors. The chemical adhesion to exposed fillers on the polymerized resin composite surface, remaining unreacted monomers in previously polymerized resin composite and micromechanical adhesion occurred by the infiltration of monomers into the repaired resin composite essentially affects the repair bond strength values [Citation21,Citation22].
In this study, lower shear bond strength values were observed for fresh dry specimens. The existence of unreacted C=C double bonds is an important factor in the adhesion of fresh polymerized resin composites. Higher bond strength values of fresh resin composite repairs might have been observed as a result of numerous unreacted monomers in polymerized resin composites. The oxygen inhibition layer forms on polymerized resin composites affect the chemical and mechanical properties of the adhesion of repairing restorations as unreacted monomers in this layer can copolymerize with the unreacted monomers of repairing resin composite [Citation22]. In the present study, repaired resin composites were prepared and polymerized after covering resin composite surfaces with a transparent strip to reduce the formation of the oxygen inhibition layer. In addition, when plastic films or glass slides were used during polymerization procedures, the fillers were not exposed at the top of surfaces and thus, it can be anticipated that the filler particle exposure on the repaired resin composite surfaces was minimum [Citation23]. The limited amount of the oxygen inhibition layer and unreacted monomer on the repaired resin composites might be the reason for the lower shear bond strength values of fresh dry specimens in the present study.
Altinci et al. [Citation24] reported that the bond strength values of the repaired aged resin composites were lower than the fresh composites differently from the present study. However, they concluded that among the fresh specimens of their in vitro study; the roughened specimens to remove the oxygen inhibition layer showed significantly lower bond strengths values than the other fresh specimens similar to the present study. Both 24 h and 6 months water stored groups showed higher shear bond strength values however the difference was not statistically significant. Water sorption inhibits further polymerization of resin composites that leads to the increased adhesion of composite to composite [Citation21]. Contrary to this knowledge, thermocycled specimens showed significantly higher bond strength values in the present study which could be explained by the higher degree (55°) of thermal cycling that might enhance the polymerization rate and physical properties at the repair interface. The high degree of conversion of the substrate makes the adhesion of a repair composite more difficult. However, enhanced mechanical properties could increase the shear bond strength values [Citation25]. To date, there is no consensus for a protocol of repairing procedures. The controversial outcomes of the present study put the real aging effect of thermocycling or the other aging procedures in question.
In repairing procedures in order to create a mechanical interlocking, air-abrasion of the resin composite surfaces with aluminum oxide (Al2O3) particles or using diamond burs are generally preferred as mechanical surface treatments. Micro-retentive features created by air-abrasion on the aged resin surfaces have been reported as the gold standard protocol to achieve higher repair bond strength values [Citation26–28]. In addition, surface abrasion was reported as the most important feature in repairing procedures by Söderholm et al. [Citation29] Thus, in the present study the effect of Al2O3 air-abrasion surface treatment on repair bond strength was evaluated. The second null hypothesis of the present investigation that air-abrasion surface treatment procedure would not affect the shear bond strength of repaired resin composites, was not accepted. Al2O3 air-abraded groups showed higher bond strength values than non-treated groups similar to the previous studies [Citation17,Citation30,Citation31].
In the present study, considering the interaction between the two factors ‘surface treatments’ and ‘adhesive systems’, AB, CU and SK applied on Al2O3 air-abraded specimens showed the highest shear bond strength values. Several studies suggested Al2O3 air-abrasion and following application of first a silane and then using an adhesive system as effective pretreatment methods during repairing procedures [Citation9,Citation32,Citation33].
Numerous surface conditioning methods and adhesive systems have been developed to improve the adhesion between repair and substrate resin composites. While some studies reported increased repair bond strength values with the application of adhesive systems [Citation3,Citation5], other studies showed better results with mechanical conditioning of substrate resin composite surfaces [Citation34,Citation35]. Mechanical surface treatments aim to improve micromechanical retention between the repair and substrate resin composites, whereas adhesive systems aim of improving chemical adhesion [Citation17]. Investigations assessing the influence of different adhesive systems for repair procedures have shown a difference in bond strength values depending on the adhesive systems. Accordingly, filled adhesive systems showed favorable bond strength values than those of unfilled ones [Citation26]. On the contrary, Brosh et al. [Citation36] explained that un-filled bis-GMA (bisphenol A-Glycidyl Methacrylate) resin was the most effective agent for better adhesion during repairing procedures.
The chemistry of matrix ingredients of adhesive systems might be more effective than the matrix chemistry of resin composite restoration on the success of repair procedures. The monomer and solvent in the adhesive systems depend on the chemical affinity of these materials and the degree of hydration of repaired resin composites. Most resin composites are hydrophobic and they absorb some amount of water that may increase the surface penetration by hydrophilic adhesives [Citation37].
More recent multimode adhesive systems called ‘universal one-bottle adhesive systems’ are recently introduced for use as either etch and rinse or self-etch adhesive systems. These adhesives are also declared to show adhesion to all kinds of materials and/or hard dental tissues [Citation38]. They generally include silane and do not need additional primer application to adhere to a different substrate. Therefore, the use of these adhesive systems may enhance the adhesion during repair procedures [39]. Universal adhesive systems have similar content to one-step etch and dry adhesive systems as specific carboxylate and/or phosphate monomers such as 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP) which bond chemically to calcium in hydroxyapatite lead to the formation of non-soluble calcium salts [Citation40]. The adhesive systems including 10-MDP are effective in repairing procedures. Furthermore, this functional monomer can diffuse into the cross-linked network and provide trapped C=C that may show adhesion to the substrate resin composite [Citation41,Citation42].
In the present study, the third null hypothesis that there would be no statistically significant difference between the adhesive systems in terms of bond strength was rejected. All universal adhesives include the functional monomer 10-MDP, AB, CU and SK showed higher bond strength values. CU and SK belong to the adhesive systems that contain silane and it is mentioned in the literature that silane containing adhesive systems increase the bond strength of resin composites during repair procedures. [Citation9,Citation17,Citation33–40,Citation43,Citation44]. High bond strength values of these two adhesive systems could be explained by the fact that bifunctional silane molecules adhere to the resin composite surfaces after being hydrolyzed to silanol. Silanol groups react with the monomers of the resin composite and increase bond strength. AB showed higher bond strength values than CU and SK but the difference in the bond strength of these adhesives was not statistically significant. It has also been reported that the solvents affect the wetting ability and bond strength of adhesive systems. Due to the better wetting ability of ethanol and 10-MDP, adhesives including these components might have enhanced bond strength values during repair procedures [27]. High bond strength values of the AB system could relate to the ingredients such as ethanol and 10-MDP. The worst bond strength values were observed for the groups of the primer MP.
Conclusions
From this study, the following could be concluded:
The limited presence of an oxygen inhibition layer decreased shear bond strength values of fresh dry repaired resin composite but thermocycle aged specimens showed better adhesion.
Physical surface conditioning using Al2O3 air-abrasion enhanced the composite–composite adhesion in repair procedures.
10-MPD and silane containing universal adhesive systems increased the composite–composite adhesion.
Air abrasion followed by silane or primer application appears to be essential to achieve the durable composite repair.
Clinical relevance
Surface conditioning with air-borne particle abrasion enhances the composite to composite adhesion during repairing procedures regardless of the universal primer used. Clinicians should consider the 10-MPD and silane-containing universal adhesive systems for increased composite–composite adhesion in repair procedures.
Acknowledgement
The authors acknowledge Kuraray Europe GmbH, Hattersheim am Main, Germany, for the generous provision of the materials used in this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Araujo CTP, Prieto LT, Costa DC, et al. Active application of primer acid on acid-treated enamel: influence on the bond effectiveness of self-etch adhesives systems. Microsc Res Tech. 2017;80(8):943–949.
- Fu J, Saikaew P, Kawano S, et al. Effect of air-blowing duration on the bond strength of current one-step adhesives to dentin. Dent Mater. 2017;33(8):895–903.
- Tezvergil A, Lassila LV, Vallittu PK. Composite-composite repair bond strength: effect of different adhesion primers. J Dent. 2003;31(8):521–525.
- Kupiec KA, Barkmeier WW. Laboratory evaluation of surface treatments for composite repair. Oper Dent. 1996;21(2):59–62.
- Shahdad SA, Kennedy JG. Bond strength of repaired anterior composite resins: an in vitro study. J Dent. 1998;26(8):685–694.
- Teixeira EC, Bayne SC, Thompson JY, et al. Shear bond strength of self-etching bonding systems in combination with various composites used for repairing aged composites. J Adhes Dent. 2005;7:159–164.
- Fawzy AS, El-Askary FS, Amer MA. Effect of surface treatments on the tensile bond strength of repaired water-aged anterior restorative micro-fine hybrid resin composite. J Dent. 2008;36(12):969–976.
- Padipatvuthikul P, Mair LH. Bonding of composite to water aged composite with surface treatments. Dent Mater. 2007;23(4):519–525.
- Staxrud F, Dahl JE. Role of bonding agents in the repair of composite resin restorations. Eur J Oral Sci. 2011;119(4):316–322.
- AlJehani YA, Baskaradoss JK, Geevarghese A, et al. Shear bond strength between fiber-reinforced composite and veneering resin composites with various adhesive resin systems. J Prosthodont. 2016;25(5):392–401.
- Özcan M, Barbosa SH, Melo RM, et al. Effect of surface conditioning methods on the microtensile bond strength of resin composite to composite after aging conditions. Dent Mater. 2007;23(10):1276–1282.
- Duran I, Ural Ç, Yılmaz B, et al. Effects of Er:YAG laser pretreatment with different energy levels on bond strength of repairing composite materials. Photomed Laser Surg. 2015;33(6):320–325.
- Belli R, Sartori N, Peruchi LD, et al. Slow progression of dentin bond degradation during one-year water storage under simulated pulpal pressure. J Dent. 2010;38(10):802–810.
- Loomans B, Özcan M. Intraoral repair of direct and indirect restorations: procedures and guidelines. Oper Dent. 2016;41:68–78.
- Özcan M, Corazza PH, Marocho SM, et al. Repair bond strength of microhybrid, nanohybrid and nanofilled resin composites: effect of substrate resin type, surface conditioning and ageing. Clin Oral Invest. 2013;17(7):1751–1758.
- Tyas MJ, Anusavice KJ, Frencken JE, et al. Minimal intervention dentistry-a review. FDI Commission Project 1-97. Int Dent J. 2000;50(1):1–12.
- Martos R, Hegedüs V, Szalóki M, et al. A randomised controlled study on the effects of different surface treatments and adhesive self-etch functional monomers on the immediate repair bond strength and integrity of the repaired resin composite interface. J Dent. 2019;85:57–63.
- Flury S, Dulla FA, Peutzfeldt A. Repair bond strength of resin composite to restorative materials after short- and long-term storage. Dent Mater. 2019;35(9):1205–1213.
- Kanzow P, Baxter S, Rizk M, et al. Effectiveness of a universal adhesive for repair bonding to composite and amalgam. J Oral Sci. 2019;61(2):343–350.
- Sau CW, Oh GS, Koh H, et al. Shear bond strength of repaired composite resins using a hybrid composite resin. Oper Dent. 1999;24(3):156–161.
- Nagano D, Nakajima M, Takahashi M, et al. effect of water aging of adherend composite on repair bond strength of nanofilled composites. J Adhes Dent. 2018;20:425–433.
- Alqarni D, Nakajima M, Hosaka K, et al. The repair bond strength to resin matrix in cured resin composites after water aging. Dent Mater J. 2019;38(2):233–240.
- Shawkat ES, Shortall AC, Addison O, et al. Oxygen inhibition and incremental layer bond strengths of resin composites. Dent Mater. 2009;25(11):1338–1346.
- Altinci P, Mutluay M, Tezvergil-Mutluay A. Repair bond strength of nanohybrid composite resins with a universal adhesive. Acta Biomater Odontol Scand. 2018;4(1):10–19.
- Magne P, Malta DAMP, Enciso R, et al. Heat treatment influences monomer conversion and bond strength of indirect composite resin restorations. J Adhes Dent. 2015;17(6):559–566.
- Yesilyurt C, Kusgoz A, Bayram M, et al. Initial repair bond strength of a nano-filled hybrid resin: effect of surface treatments and bonding agents. J Esthet Restor Dent. 2009;21(4):251–260.
- Wendler M, Belli R, Panzer R, et al. Repair bond strength of aged resin composite after different surface and bonding treatments. Materials. 2016;9(7):547–574.
- Blum IR, Hafiana K, Curtis A, et al. The effect of surface conditioning on the bond strength of resin composite to amalgam. J Dent. 2012;40(1):15–21.
- Söderholm KJ, Roberts MJ. Variables influencing the repair strength of dental composites. Scand J Dent Res. 1991;99(2):173–180.
- da Costa TR, Serrano AM, Atman AP, et al. Durability of composite repair using different surface treatments. J Dent. 2012;40(6):513–521.
- Papacchini F, Dall’Oca S, Chieffi N, et al. Composite-to-composite microtensile bond strength in the repair of a microfilled hybrid resin: effect of surface treatment and oxygen inhibition. J Adhes Dent. 2007;9:25–31.
- Hickel R, Brüshaver K, Ilie N. Repair of restorations-criteria for decision making and clinical recommendations. Dent Mater. 2013;29(1):28–50.
- Staxrud F, Dahl JE. Silanising agents promote resin-composite repair. Int Dent J. 2015;65(6):311–315.
- Swift EJ, Le Valley BD, Boyer DB. Evaluation of new methods for composite repair. Dent Mater. 1992;8(6):362–365.
- Bouschlicher MR, Reindhardt JW, Vargas MA. Surface treatment techniques for resin composite repair. Am J Dent. 1997;10:279–283.
- Brosh T, Pilo R, Bichacho N, et al. Effect of combinations of surface treat- ments and bonding agents on the bond strength of repaired composites. J Prosthet Dent. 1997;77(2):122–126.
- Cavalcanti AN, De Lima AF, Peris AR, et al. Effect of surface treatments and bonding agents on the bond strength of repaired composites. J Esthet Restor Dent. 2007;19(2):90–98.
- Perdigão J, Loguercio AD. Universal or multi-mode adhesives: why and how? J Adhes Dent. 2014;16:193–194.
- de Medeiros TC, de Lima MR, Bessa SC, et al. Repair bond strength of bulk fill composites after different adhesion protocols. J Clin Exp Dent. 2019;11:e1000.
- Çakir NN, Demirbuga S, Balkaya H, et al. Bonding performance of universal adhesives on composite repairs, with or without silane application. J Conserv Dent. 2018;21(3):263–268.
- Ritter AV, Sulaiman TA, Altitinchi A, et al. Composite-composite adhesion as a function of adhesive-composite material and surface treatment. Oper Dent. 2019;44(4):348–354.
- Van Meerbeek B, Yoshihara K, Yoshida Y, et al. State of the art of self-etch adhesives. Dent Mater. 2011;27(1):17–28.
- Lima AD, de Vicente Leite T, Palialol AM, et al. Effect of surface conditioning methods, adhesive systems and resin composite on repair strength of dimethacrylate and silorane resin composites. J Adhes Sci Technol. 2016;30(24):2736–2744.
- Mumcu E, Erdemir U, Özsoy A, et al. Effect of surface conditioning methods on the microtensile bond strength of repair composite to indirect restorative materials. J Adhes Sci Technol. 2019;33(21):2369–2384.