
Abstract
Aim
To identify the interaction of instrumented gait analysis (IGA) training, expertise, and application in gait-related management of cerebral palsy.
Methods
Semi-structured interviews with 20 purposively sampled clinicians with varying professional backgrounds, expertise, and training, analyzed using the framework method.
Results
Fifteen sub-themes were identified within three domains: training, equipment/outputs, and roles/reasons under the core theme IGA practice. Findings were illustrated using the Experience/Equipment/Roles/Training (Exp-ERT) Framework which identifies four user categories – based on influencing factors, beset by barriers, with experience reported as a common enabling factor. Clinicians who encountered barriers in one of the domains were categorized as either “frustrated” or “hesitant” users. Those who were no longer using IGA for clinical decisions were designated “confident non-users”. Finally, the ‘confident experts’ reported the required level of training and access to interpret IGA outputs for clinical decision-making. Expertise gained at any level of clinical practice was shown to initiate advancement within domains.
Conclusions
Clinicians encounter a multitude of barriers to IGA practice that can result in failure to progress or impact on clinical decision-making. The Exp-ERT Framework emerges strongly from the data and could serve as an evaluation tool to diagnose barriers to confident expertise and support IGA-related professional development planning.
Introduction
Instrumented gait analysis (IGA) provides the facility to quantify human movement and influence clinical decisions as a clinical and research measure (Wren et al., Citation2011; Wren, Elihu, et al., Citation2013; Wren, Otsuka, et al., Citation2013; Wren, Lening, et al., Citation2013; Rasmussen et al., Citation2019; Wren et al., Citation2020). Despite being available for more than three decades, IGA tends to be associated with large research institutions (Reid et al., Citation2011). Clinically, IGA has gained a prominent place in the management of ambulant children and young people with cerebral palsy (CYPwCP) where gait-related goals are amongst the most important for children and their families (Capjon & Bjork, Citation2010; Vargus-Adams & Martin, Citation2011). In this context, IGA has been supporting surgical decision-making and measuring intervention outcomes (Gage, Citation1994; Wren et al., Citation2005; Lofterod et al., Citation2007; Gough & Shortland, Citation2008; Wren, Elihu, et al., Citation2013; Wren, Otsuka, et al., Citation2013; Wren, Lening, et al., Citation2013). National Institute for Clinical Excellence (NICE) refers to the IGA assessment as a preferable choice prior to gait-improving orthopedic surgery (NICE Citation2016a, Citation2016b) Despite this, standardized access pathways for CYPwCP to IGA are yet to be established (Gaston, Citation2019; Rasmussen et al., Citation2019). Furthermore, access to IGA for other professionals involved in gait management like physiotherapists or orthotists (Franki et al., Citation2012) and their formal IGA education remains limited (Toro et al., Citation2003). Although the impact of IGA on treatment choices and their outcomes in Allied Health Professions (AHP) is less established, gait analysis is considered as interprofessional – as knowledge, discipline, and as a clinical tool. For this reason, a wide variety of skills and educational needs should be expected in clinical practice. This undoubtedly enriches the gait analysis community but makes common training pathways difficult to establish. There is guidance and a set of requirements specific to the profession of clinical gait analyst (Baker et al., Citation2016), however, in the area of child neurodisability, where there is no such thing as “one size fits all”’ (for both patients and clinicians) an interprofessional gait analysis competency framework has not been constructed.
Although the interprofessional character of gait-related practice seems to be commonplace, there is a gap in understanding its clinical landscape, the wide range of users’ needs, access opportunities, and their diverse skill sets. As a discipline, IGA requires a wide spectrum of knowledge and skills, making it hard to learn or successfully integrate into undergraduate curricula (Baker et al., Citation2016). The interprofessional character of this field and variety of available tools can cause confusion around terminology (Baker, Citation2013). In context of this work, authors refer to gait analysis as a general concept of assessment of walking differentiating clinical (observational) from IGA (using instrumentation and software).
With this qualitative study, we aim to identify the interaction of IGA training, expertise, and application in gait-related management of ambulant CYPwCP. A qualitative approach was chosen because of the variability and the interdisciplinarity of clinical settings in which gait problems of this patient group are assessed and treated (Ritchie J. Citation2014). This study explores the question from the perspective of the varied clinical professions and settings in which IGA is used, to gain an understanding of needs and possible barriers to clinicians’ engagement with IGA to inform self-assessment, service design, and the development of educational interventions.
Methods
Design
This study used a qualitative design, underpinned by the realist approach (Blaikie, Citation2007) and located within a interpretivist frame (Ritchie J. Citation2014). The opinions and experiences of participants were explored to understand process of clinical decision-making based on gait analysis in ambulant CYPwCP and its contextual reality in clinical practice. Semi-structured interviews were employed and the framework approach utilized for data analysis using a semi-deductive approach (Ritchie J. Citation2014). The Standards for Reporting Qualitative Research (SRQR) and Consolidated Criteria for Reporting Qualitative Research (COREQ) were followed to ensure rigorous reporting of the study components (O'Brien et al., Citation2014).
Participants
Participants were recruited via email using a purposive sampling method. The sample included clinicians with variable backgrounds, level of training, seniority, and experience of gait-related clinical decision-making for CYPwCP in the UK. They were recruited from a range of practice settings including community practice, tertiary centers, gait laboratories, and education, the National Health Service and from the private sector. 6 of the clinicians roles spanned across multiple practice settings i.e. community and tertiary center or gait lab, private clinic and education. An initial sample of 11 clinicians was expanded to 20 until data saturation was reached (Morse, Citation1995) (). The study gained approval from [masked] Ethics of Research Committee (QMREC2014/24/99) prior to the data collection. The voluntary basis of the study was explained, anonymity of the data assured, and informed consent sought from all participants.
Table 1. Classification of 20 Participants Portrayed in Relation to the Purposive Sampling Frame
Data Collection and Processing
Twenty semi-structured interviews were conducted by two interviewers (AHB, AA). AHB is a clinician experienced in managing ambulant CYPwCP, therefore, measures were put in place to overcome the potential participant bias (feeling obliged to give a “correct answer” rather than own opinion) and researcher’s bias (arising from own beliefs about the IGA practice) to ensure trustworthiness – comprehensive sample frame, investigator triangulation, prolonged involvement, respondent validation were implemented during the data analysis, researcher also kept a reflective diary and had access to de-brief meetings (Korstjens & Moser, Citation2018). Participants chose the time and location of the interviews (face-to-face, telephone, or on-line via Skype). Interviews were 40–90 min long, audio-recorded then transcribed verbatim by investigators to allow for deeper immersion in the data and prolonged engagement (Korstjens & Moser, Citation2018). All transcripts were cross-checked with recordings to ensure dependability and confirmability of findings. Data collection and analysis were iterative and parallel processes with repeated returns to the transcripts to ensure the contextual anchoring (Ritchie J. Citation2014).
Topic Guide
The topic guide was informed by a literature search, discussion within the research team and adjusted after a pilot interview (not used in data analysis). The topic guide served as an aide-memoire, ensuring the consistency and focus of data collection. It included open-end questions embedded in five areas (1) Background; (2) IGA practice; (3) Patients and families; (4) IGA Training; and (5) IGA reports. Follow-up probing questions were used to clarify and elaborate on responses (Table 2 – Supplementary material).
Data Analysis
The framework analysis approach was used for data management, abstraction, and interpretation (Ritchie J. Citation2014). During active familiarization, the textual data were coded, codes organized into themes and subthemes to construct a thematic framework matrix in Microsoft Excel where columns represented themes/sub-themes, and rows represented participants. Throughout the indexing stage, phrases, sentences, and paragraphs of raw data were labeled accordingly to the thematic framework. The linkages and patterns of association were investigated during the explanatory analysis stage and considered alongside current literature.
To ensure rigor and consistency the analysis process underwent investigator triangulation (AHB, BZ, and AA), thematic framework, and labeling process reviews at de-briefing meetings.
Illustrative Framework
Further exploratory analysis focused on exploration of linkages across the data, similarities, and differences between participants, domains, and subthemes. Each individual participant’s account has been mapped across the domains with potentially reported barriers to practice superimposed over the domains. Reoccurring patterns of association were investigated across the data set and each user category tested individually. Patterns and categories were debated during team meetings. This process resulted in more abstract classificatory system. To display the findings figuratively and provide our explanation for our observations the illustrative framework has been proposed.
Respondent Validation
Selected participants were approached via email to review the study findings. None of the data was retracted. No new themes emerged during respondent validation.
Results
The experiences of participants emerged under two core themes: IGA practice and barriers; which were concluded with confidence.
Theme 1. GAIT Analysis Practice
Factors influencing use of gait analysis practice were grouped in 15 subthemes within 3 domains (Table 3 – Supplementary material).
Domain 1: Roles and Reasons
The ways that IGA is utilized and accessed in clinical practice is versatile and will depend on the clinicians’ in-role requirement for gait-related decision-making.
One of the main reasons for utilizing gait analysis in management of ambulant CYPwCP was assessment. This was considered as routine, however, its technique and content varied. Clinicians reported that not every ambulant CYPwCP and not every clinical query will require use of instrumentation. Participants favored IGA over other methods because of its reliability and biomechanical detail.
The added value of the gait analysis is in depth analysis of what the problems are, why they express themselves the way they do and I don’t think that you can do that with simple observation or clinical examination. You can by going in-depth into biomechanics of gait. TS0545
In their practice, clinicians also used IGA for monitoring the trajectory of a patient’s gait over time or after interventions (surgery, orthotics, and therapy). Video-recording was more frequently used for monitoring in community settings.
They have it every year and then we compare all those outcomes to last year and think if they are improving, deteriorating and especially if they have CP we can compare that to the trajectory of their growth. MP0518
Clinicians who had access to IGA often used it for pre- and post-operative follow-up - usually in tertiary centers led by orthopedic surgeons. Although many participants highlighted the value that IGA offers in planning physiotherapy programs and orthotic provision, surgical decision-making for CYPwCP was a strongly expressed reason for considering IGA.
I think in children where at some point you have to decide whether to do certain interventions like surgical interventions, I think it is mandatory to get gait analysis. PS0251
For big intervention you want to be confident that you make the right decision. RC0728
Some of the IGA outputs such as reports and videos were used to liaise within interprofessional teams, or with patients and families. Participants often emphasized the importance of information-sharing and reported its absence as frequent and difficult to overcome.
It’s quite frustrating (…) we try to communicate with the tertiary centre the best we can, but sometimes they don’t communicate back to us. VP0413
Domain 2: Training
This domain concerned the training, development of IGA knowledge, and skill acquisition reported by participants.
IGA education was thought to be limited at the undergraduate level especially for physiotherapists, who did not feel well prepared for IGA-related practice after undergraduate study.
It is useless, isn’t it? physios come out of universities with one hour. EP0753
No I don’t think I was prepared for my current role. I had one lecture (…) and I had a placement (…) it was not till I started working that I have learned. CP0427
Amongst those with greater undergraduate exposure, the evolving technology made it difficult to keep IGA knowledge up-to-date. All participants continued professional development by accessing learning delivered by higher education institutions (as part of taught or research degrees) or private providers (professional bodies and specialist associations) within the UK and internationally. Many clinicians (across experience and seniority levels) reported problems with gait-related knowledge transfer into practice.
So, I came back still not really understanding what all the different graphs mean and different moments and forces and vectors and all of these (…) And how they relate to the child in front of me. DS0378
Knowledge and skills gained whilst ‘on the job’ were viewed as being important component of learning, with the inter-professional character of IGA practice well recognized.
It’s just putting yourself out there and finding out what facilities are around you (…) ‘It’s purely by exposure. CO0601
I have essentially been taught by the physiotherapists that I am working with. DS0378
Self-study was considered a successful strategy to improve understanding of gait and one’s own practice.
Reports can be a learning tool; the more you see the more it make sense, especially if you can picture how that child walks. PP0368
I think that experience that one accumulates is to learn what kind of child is going to do well through surgery and which not. And this is where gait analysis is very helpful. TS0545
Domain 3: Equipment and Outputs
This domain concerned types of equipment and IGA outputs accessed by the participants in their practice. IGA was reported to be most desirable gait assessment method, however often difficult to access and requiring specialist knowledge.
But it’s a bit of a chicken and egg. You don’t have technology to do things so easily and therefore we don’t do it in the volume to understand it. DP0517
There was, an overarching belief that IGA equipment is expensive to purchase and time-consuming to use. Many believed that more routine referrals to motion laboratories would be uneconomic for the number of potential candidates.
It costs £1000 a time and I don’t think that we can necessarily afford that on the NHS unless we got good reasons for doing it.(…) I think we have to work a little bit harder on just trying to justify what works what we spending money on. DS0378
Amongst participants reporting lack of access to IGA most strongly were physiotherapists working in community settings, for whom the most common tool used to record gait was videography, especially to rewind and slow down patient’s walk for more thorough observation. The use of software was not reported, so videography was purely observational – systematic, but qualitative in nature. Few participants reported access to other gait analysis systems e.g. camera and force plate setups.
It’s not going to provide you with information and or accuracy of 3D-motion analysis it is much better than simple observation in clinic (…) You have to take the best substitute which would be a good quality video which you can take on your phone and you at least can observe child’s walking pattern repeatedly and in slow motion look at the foot contact. TS0545
Many participants aimed to make their clinical assessment of walking as systematic as possible, however, use of gait-specific scales was rarely reported.
Theme 2 – Barriers
This theme comprised of 5 subthemes, aimed at categorizing and grouping barriers under two domains (Table 3 – Supplementary material).
Domain 1: External Barriers
Barriers external to the clinician were frequently reported and included economic issues related to the high cost of equipment, training and extra staff time for IGA.
It’s expensive and when assessment is as expensive as the treatment, that becomes difficult equation for institutions to manage. AC0528
Amongst the institutional barriers were information governance, increasing workloads resulting in lack of time to change practice, broken equipment and unsupportive departmental improvement culture.
We have a force plate in the centre but have not used it because of broken computer or software. CP0427
Participants also believed that lack of communication between institutions is a barrier to practice.
I think that there is a separation between expert gait lab and people on the ground with the child’s need. In the end there’s just conflict and lack of understanding. EP0753
A less strongly reported barrier was families’ compliance, nonattendance rate, or possible inconvenience to attend additional appointments, sometimes far away.
Sometimes they [families] think that it is too far to go and not very helpful. DS0528
Domain 2: Internal Barriers
Internal barriers to participants’ engagement with gait analysis within this domain were personal or cognitive in origin). This included lack of initiatives to create interprofessional links or to improve practice and services.
I tried to use the outcome measure in the community. I thought that if I can use it, then I can make other people use it. But I struggled and I gave up. VP0413
Lack of skills and limited knowledge were amongst the barriers to practice and included lack of understanding of outputs or how to use equipment, sometimes originating from incorrect training or equipment choices which were poorly matched to clinicians’ needs.
I have done the course with use of force plate, but I have never been in a clinical setting where I could put it all into practice. CP0427
Analysis showed that even very senior participants with a lot of gait-related training, questioned their IGA abilities.
I don’t teach much about gait analysis I really do not think that I am the right person to do this. DS0378
Some people get very interested in it [IGA] and that’s fine and there’s lots of people over there that don’t have the training nor the innate talent. AC0528
Exp-ERT Framework
The synthesis of themes, domains, and subthemes enabled construction of an explanatory model illustrating the results and explaining our observations. Each circle within the model represents domains of the Gait Analysis Practice theme: training, roles and reasons, and equipment and outputs. The corresponding boxes provide a list of subthemes collectively representing findings within each domain. Areas where circles intersect represent the user categories. The Experience-Equipment/Roles/Training (Exp-ERT) Framework () shows linkages between the domains of training, roles and reasons, and equipment and outputs of gait analysis from participants’ descriptions. Analysis across the data sources found four explanatory user categories represented at different intersection areas of domains. Intersection of all three domains represents confident experts. Our analysis showed that these relationships can be impacted by a multitude of factors, beset by barriers, with experience reported as an enabling factor to confident expertise in gait-related practice. Areas where only two domains intersect (due to presence of barrier within the third domain) represent hesitant users, frustrated users, and confident non-users.
Figure 1. The Experience-Equipment/Roles/Training (Exp-ERT) Framework illustrates linkages between the domains, experience of four explanatory user categories within the context of gait-related clinical practice.
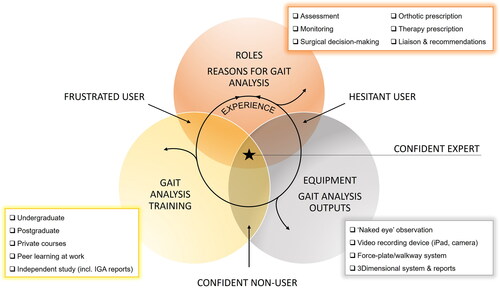
The circular arrow bisecting the domains represents experience within the practice domains at the complementary levels. Smaller arrows pointing toward individual domains signify reports of confident users feeding back into the domains of practice i.e. teaching others (Training domain), service development (Equipment and outputs domain), and advancing clinical practice (Role and responsibilities domain).
Discussion
The study shows the explanatory domains relating to IGA practice are multifactorial, interlinked, and illustrated using the Exp-ERT Framework ().
The confident experts were participants who had training matched with adequate equipment, which could be confidently used for in-role clinical decision-making. It is important to note that confident expertise was not inevitably determined by seniority of position or overall years of clinical practice. Our study shows that confidence and expertise in gait analysis practice are achieved by gaining experience within the domains at the complementary levels. Furthermore, findings of this study suggest that confident practice within matched domains can initiate a virtuous circle of continuous advancement of an individual clinician’s practice, which may transfer benefit to others through teaching or service development.
Participants gave a rich account of issues affecting their practice within domains. The cost related to use of IGA and gaps in gait-related training are suggested as frequent barriers to engagement with gait analysis (Toro et al., Citation2003, Wren et al., Citation2011, Citation2020). Our findings show broad array of possible obstacles encountered in clinical practice by gait analysis users – external barriers, arising from institutions, service providers and service users, and those internal to the clinician (i.e. reduced motivation, lack of knowledge, choosing equipment, or training courses inadequately matched to their needs or needs of their service). Overlaying barriers reported by participants on domains of their individual practice allowed for deeper understanding of clinicians and context within which gait-related practice occurs. Participants often found it difficult to be at complementary levels across all domains. Some reported facilitators in two domains, but barriers within the third affecting their practice and leading to compromised treatment decisions.
Clinicians who were practicing in roles that required gait-related decision-making and who had access to appropriate equipment or outputs but, did not have appropriate training (including self-perceived lack of training) would practice as hesitant users (). In our study, access to training was shown to be important and impact directly on practice. However, there was no single IGA training route and frequent problems with knowledge transfer were experienced by clinicians. Recent evaluative research of IGA training is sparse and limited to students’ satisfaction and knowledge without consideration of impact on behaviors, services, or patient outcomes (Baskwill et al., Citation2017; Malone et al., Citation2017). However, while the literature provides examples where IGA outputs directly influence clinicians’ decisions, it does not investigate long-term attitude or behavior change. The existing literature on the impact of clinicians’ training and experience on engagement with IGA outputs is inconclusive (DeLuca et al., Citation1997; Filho et al., Citation2008).
Participants in a position of confident non-users were those who were no longer actively using IGA for CYPwCP but were highly trained with access to IGA equipment. Rather than being related directly to background or profession, these were usually professionals who had changed roles, for example from clinical research to management, and despite having training and access to IGA were no longer involved in gait-related decision-making for ambulant CYPwCP. This important group of highly skilled users may be at risk of their gait-related skill set being lost or degrading. These skilled and trained individuals make up a potential loss to the IGA community.
Clinicians who reported adequate training and were practicing in the decision-making role but did not have access to equipment or outputs matched to training and their role – would be frustrated users. Cost was a strong barrier to IGA access in our sample. IGA is perceived as an expensive assessment with the costs often difficult to justify within services or professional groups i.e. AHPs (Toro et al., Citation2003; Wren et al., Citation2011, Citation2020). However, multiple studies have shown that IGA has the potential to change and decrease the amount of surgery planned for CYPwCP which has a positive economic impact on services (DeLuca et al., Citation1997), so it may be that the apparent saving – or avoidance of expenditure - is false when considered in the wider sense. In our study, frustrated users (often very senior AHPs working in the community settings) reported institutional inertia leading to a lack of communication and sharing of IGA outputs. Literature shows that direct affiliation with gait laboratories plays an important role in utilizing IGA outputs (Wren et al., Citation2005; Lofterod & Terjesen, Citation2008; Wren, Elihu, et al., Citation2013; Wren, Otsuka, et al., Citation2013; Wren, Lening, et al., Citation2013). Lack of interprofessional links and poor communication between centers has been reported amongst barriers to gait-related practice in our study. With increasing demands on clinicians and services for inter-professional partnerships and shared decision-making, there is an increasing need for broader and more inclusive collaborations and information sharing (NICE Citation2016a, Citation2016b; Harden, Citation2017). The advent of accessible digital records provides the opportunity to meet that need.
Limitations
Our initial sample was relatively small, sampling, however, continued until thematic saturation was reached. The aim of the approach was to achieve the depth of data, and to reach saturation rather than enable sub-samples to be analyzed. We acknowledge that there may be groups of professionals who are less often involved in gait-related decision-making of CYPwCP (for example pediatricians and neurologists), who were not included in the sample. Some of these professionals may have access to IGA outputs, training or play a role of a stakeholder in management of ambulant CYPwCP. Further scoping of these professional groups could be investigated further in future research.
Limitations arising from data which represent meanings are that it cannot be tested for validity using quantitative measures (Johnson & Waterfield, Citation2004). Here the credibility and transferability of findings have been established by demonstrating methodological rigor, dense methodological and contextual descriptions and the use of triangulation methods. (Daniel, Citation2018; Hebda-Boon & Poole, 2019) The data are most transferable to Western European healthcare settings.
Conclusions
The clinical networks managing gait-related problems of ambulant CYPwCP are broad and diverse and face a multitude of barriers. These barriers hinder clinicians’ practice – may affect their progress and lead to compromised decision-making.
Our study introduces the Exp-ERT Framework – an analysis tool that can be used to diagnose factors obstructing confident expertise in clinical practice. Factors impacting use of IGA in practice are multidimensional and interlinked. Barriers in one or more domains of practice may result in compromised decision-making and impact professional progress. Confident expertise does not equal seniority of position or duration of experience in clinical practice.
The efforts should be focused on empowering clinicians at different levels of seniority and expertise to actively and critically apprize their gait-related practice. The Exp-ERT Framework can support professional development planning, service evaluation, and underpin development of complex educational interventions related to IGA.
Supplemental Material
Download MS Word (26.4 KB)Supplemental Material
Download MS Word (21.7 KB)Supplemental Material
Download MS Word (39 KB)Disclosure statement
The authors report no conflicts of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Related Research Data
References
- Baker, R. (2013). Measuring walking: A handbook of clinical gait analysis. Mac Keith Press.
- Baker, R., Esquenazi, A., Benedetti, M. G., & Desloovere, K. (2016). Gait analysis: Clinical facts. European Journal of Physical and Rehabilitation Medicine, 52(4), 560–574.
- Baskwill, A. J., Belli, P., & Kelleher, L. (2017). Evaluation of a gait assessment module using 3D motion capture technology. International Journal of Therapeutic Massage & Bodywork, 10(1), 3–9.
- Blaikie, N. (2007). Approaches to Social Inquiry. 2nd ed. Cambridge.
- Capjon, H., & Bjork, I. T. (2010). Ambulant children with spastic cerebral palsy and their parents' perceptions and expectations prior to multilevel surgery. Developmental Neurorehabilitation, 13(2), 80–87. https://doi.org/https://doi.org/10.3109/17518420903373511
- Daniel, B. (2018). Empirical verification of the “TACT” framework for teaching rigour in qualitative research methodology. Qualitative Research Journal, 18(3), 262–275. https://doi.org/https://doi.org/10.1108/QRJ-D-17-00012
- DeLuca, P. A., Davis, R. B., Õunpuu, S., Rose, S., & Sirkin, R. (1997). Alterations in surgical decision making in patients with cerebral palsy based on three-dimensional gait analysis. Journal of Pediatric Orthopedics, 17(5), 608–614. https://doi.org/https://doi.org/10.1097/00004694-199709000-00007
- Filho, M. C. d M., Yoshida, R., Carvalho, W. d S., Stein, H. E., & Novo, N. F. (2008). Are the recommendations from three-dimensional gait analysis associated with better postoperative outcomes in patients with cerebral palsy? Gait & Posture, 28(2), 316–322. https://doi.org/https://doi.org/10.1016/j.gaitpost.2008.01.013
- Franki, I., Desloovere, K., De Cat, J., Feys, H., Molenaers, G., Calders, P., Vanderstraeten, G., Himpens, E., & Van Broeck, C. (2012). The evidence-base for basic physical therapy techniques targeting lower limb function in children with cerebral palsy: A systematic review using the International Classification of Functioning, Disability and Health as a conceptual framework. Journal of Rehabilitation Medicine, 44(5), 385–395. https://doi.org/https://doi.org/10.2340/16501977-0983
- Gage, J. (1994). The role of gait analysis in the treatment of Cerebral Palsy. Journal of Pediatric Orthopaedics, 14, 701–702.
- Gaston, M. (2019). CPIPS: Musculoskeletal and hip surveillance for children with cerebral palsy. Paediatrics and Child Health, 29(11), 489–494. https://doi.org/https://doi.org/10.1016/j.paed.2019.07.013
- Gough, M., & Shortland, A. P. (2008). Can clinical gait analysis guide the management of ambulant children with bilateral spastic cerebral palsy? Journal of Pediatric Orthopaedics, 28(8), 879– 883. https://doi.org/https://doi.org/10.1097/BPO.0b013e31818e197c
- Harden, B. (2017). Person-centred approaches: Empowering people in their lives and communities to enable an upgrade in prevention, wellbeing, health, care and support. S. f. H. Health Education England, and Skill for Care. Health Education England, Skills for Health, and Skill for Care 2017. https://www.skillsforhealth.org.uk/images/pdf/Person-Centred-Approaches-Framework.pdf
- Hebda-Boon, A., & Poole, M. (2019). Qualitative research methodology in paediatric physiotherapy practice. Part 1: Qualitative rigour and ethical considerations. APCP Journal, 10(1), 20– 29.
- Johnson, R., & Waterfield, J. (2004). Making words count: The value of qualitative research. Physiotherapy Research International: The Journal for Researchers and Clinicians in Physical Therapy, 9(3), 121–131. https://doi.org/https://doi.org/10.1002/pri.312
- Korstjens, I., & Moser, A. (2018). Series: Practical guidance to qualitative research. Part 4: Trustworthiness and publishing. The European Journal of General Practice, 24(1), 120–124. https://doi.org/https://doi.org/10.1080/13814788.2017.1375092
- Lofterod, B., & Terjesen, T. (2008). Results of treatment when orthopaedic surgeons follow gait-analysis recommendations in children with CP. Developmental Medicine and Child Neurology, 50(7), 503–509. https://doi.org/https://doi.org/10.1111/j.1469-8749.2008.03018.x
- Lofterod, B., Terjesen, T., Skaaret, I., Huse, A. B., & Jahnsen, R. (2007). Preoperative gait analysis has a substantial effect on orthopedic decision making in children with cerebral palsy: Comparison between clinical evaluation and gait analysis in 60 patients. Acta Orthopaedica, 78(1), 74–80. https://doi.org/https://doi.org/10.1080/17453670610013448
- Malone, J., Burns, J., Belthur, M., & Karlen, J. (2017). The value of motion lab training in the orthopaedic residency curriculum. Developmental Medicine & Child Neurology, 59(S3), 57–59.
- Morse, J. M. (1995). The significance of saturation. Qualitative Health Research, 5(2), 147–149. https://doi.org/https://doi.org/10.1177/104973239500500201
- NICE. (2016). Clinical guideline [CG145] spasticity in under 19s: Management. https://www.nice.org.uk/guidance/cg145/chapter/1-guidance.
- NICE. (2016). Community engagement: Improving health and wellbeing and reducing health inequalities. https://www.nice.org.uk/guidance/ng44.
- O'Brien, B. C., Harris, I. B., Beckman, T. J., Reed, D. A., & Cook, D. A. (2014). Standards for reporting qualitative research: A synthesis of recommendations. Academic Medicine: Journal of the Association of American Medical Colleges, 89(9), 1245–1251. https://doi.org/https://doi.org/10.1097/ACM.0000000000000388
- Rasmussen, H. M., Pedersen, N. W., Overgaard, S., Hansen, L. K., Dunkhase-Heinl, U., Petkov, Y., Engell, V., & Holsgaard-Larsen, A. (2019). Gait analysis for individually tailored interdisciplinary interventions in children with cerebral palsy: A randomized controlled trial. Developmental Medicine and Child Neurology, 61(10), 1189–1195. https://doi.org/https://doi.org/10.1111/dmcn.14178
- Reid, S., Held, J. M., & Lawrence, S. (2011). Reliability and validity of the Shaw Gait assessment tool for temporospatial gait assessment in people with hemiparesis. Archives of Physical Medicine and Rehabilitation, 92(7), 1060–1065. https://doi.org/https://doi.org/10.1016/j.apmr.2011.02.014
- Ritchie, J. (2014). Qualitative research practice: A guide for social science students and researchers. Sage.
- Toro, B., Nester, C., & Farren, P. (2003). The status of gait assessment among physiotherapists in the United Kingdom. Archives of Physical Medicine and Rehabilitation, 84(12), 1878–1884. https://doi.org/https://doi.org/10.1016/S0003-9993(03)00482-9
- Vargus-Adams, J. N., & Martin, L. K. (2011). Domains of importance for parents, medical professionals and youth with cerebral palsy considering treatment outcomes. Child: Care, Health and Development, 37(2), 276–281. https://doi.org/https://doi.org/10.1111/j.1365-2214.2010.01121.x
- Wren, T., Elihu, K. J., Mansour, S., Rethlefsen, S. A., Ryan, D. D., Smith, M. L., & Kay, R. M. (2013). Differences in implementation of gait analysis recommendations based on affiliation with a gait laboratory. Gait & Posture, 37(2), 206–209. https://doi.org/https://doi.org/10.1016/j.gaitpost.2012.07.008
- Wren, T. A. L., Otsuka, N. Y., Bowen, R. E., Scaduto, A. A., Chan, L. S., Dennis, S. W., Rethlefsen, S. A., Healy, B. S., Hara, R., Sheng, M., & Kay, R. M. (2013). Outcomes of lower extremity orthopedic surgery in ambulatory children with cerebral palsy with and without gait analysis: Results of a randomized controlled trial. Gait & Posture, 38(2), 236–241. https://doi.org/https://doi.org/10.1016/j.gaitpost.2012.11.018
- Wren, T., Woolf, K., & Kay, R. (2005). How closely do surgeons follow gait analysis recommendations and why? Journal of Pediatric Orthopaedics, 14, 202–205.
- Wren, T. A., Gorton, G. E., Ounpuu, S., & Tucker, C. A. (2011). Efficacy of clinical gait analysis: A systematic review. Gait & Posture, 34(2), 149–153. https://doi.org/https://doi.org/10.1016/j.gaitpost.2011.03.027
- Wren, T. A., Lening, C., Rethlefsen, S. A., & Kay, R. M. (2013). Impact of gait analysis on correction of excessive hip internal rotation in ambulatory children with cerebral palsy: A randomized controlled trial. Developmental Medicine and Child Neurology, 55(10), 919–925. https://doi.org/https://doi.org/10.1111/dmcn.12184
- Wren, T. A., Tucker, C. A., Rethlefsen, S. A., Gorton, G. E., & Ounpuu, S. (2020). Clinical efficacy of instrumented gait analysis: Systematic review 2020 update. Gait & Posture, 80, 274–279. https://doi.org/https://doi.org/10.1016/j.gaitpost.2020.05.031