
ABSTRACT
Hormonal contraceptive (HC) users have a different ovarian hormonal profile compared to eumenorrheic women. Due to the prevalence of HC use amongst sportswomen, there has been increased research efforts to understand their impact on exercise performance. The aim was to audit this research. Studies identified were assessed for HC type, athlete calibre, performance outcome, study design, and quality of methodological control regarding ovarian hormonal profiles. Sixty-eight different HCs were reported across 61 studies. Monophasic combined oral contraceptive (OCP) pills represented 60% of HCs, followed by other pills [34%, phasic-combined, progestogen-only, and un-specified], phasic and long acting reversible contraceptives [5%, vaginal ring, patch, implant, injection, intrauterine system] and unspecified HCs (1%). Eleven percent of participants using HCs were classified as highly trained or elite/international with no participants being classed as world class. Whilst the number of studies involving HCs has increased two-fold over the past decade, the number of studies ranked as gold standard has not increased (HC; 2003–57%, 2011–55%, 2022–43%. OCP; 2003–14%, 2011–17%, 2022–12%). Future research assessing HCs and exercise performance should adopt high-quality research designs and include a broader range of HCs in highly trained to world-class populations to increase the reach and impact of research in this area.
Introduction
Hormonal contraceptives (HCs) disrupt the eumenorrheic ovarian hormonal profile by introducing exogenous synthetic hormones that act via negative feedback on gonadotrophic hormones. This chronic interference leads to the downregulation of the hypothalamic-pituitary-ovarian axis and the endogenous ovarian sex hormones, more specifically, oestrogen and progesterone. Contraceptive effects are achieved through the thickening of cervical mucus, thinning of the endometrial lining, and suppression of ovulation (Rivera et al., Citation1999). Consequently, the majority of HCs remove the endogenous cyclic ovarian hormonal fluctuations of the menstrual cycle, which is replaced with an exogenous hormonal profile and a suppressed endogenous profile. The exogenous profile varies depending on the specific type of HC used (). The intrauterine system [IUS], however, can have a more localised response to the exogenous progestogen, which means that some IUS users may present with regular menstruation and ovulatory cycles, as opposed to the suppressed endogenous profile seen with other HCs.
Table 1. Hormonal contraceptives (HCs) considered for inclusion in the audit paper.
The use of HCs is prevalent among women across different athletic backgrounds, with varying types being favoured among these populations. For example, amateur, sub-elite, and elite female athletes playing a variety of sports from multiple countries have reported using HCs at rates ranging from 34% to 63% (Brown et al., Citation2023; Clarke et al., Citation2021; Ekenros et al., Citation2022; Langan-Evans et al., Citation2023; D. Martin et al., Citation2018; Oxfeldt et al., Citation2020). In a UK-based study, up to 64% of amateur, 58% of sub-elite, and 63% of elite athletes used combined oral contraceptive pills (OCPs) (Langan-Evans et al., Citation2023). Other forms, such as cyclic combined contraceptives (e.g., vaginal rings and patches) and long-acting reversible contraceptives (e.g., intrauterine systems, implants, injections), were also employed by approximately 40% of these athletes (Langan-Evans et al., Citation2023). Similar results were seen in a study conducted on elite athletes in Denmark, where ~72% used combined OCPs, and ~28% used other forms such as progestogen-only pills, cyclic contraceptives and long acting reversible contraceptives (Oxfeldt et al., Citation2020). Despite the range of contraceptive usage amongst active women, current research exhibits a notable bias towards studying the effects of combined OCP, particularly monophasic formulations (Elliott-Sale et al., Citation2020). These contraceptives may be favoured in the literature due to their prevalence among athletic populations and well-established characteristics and hormonal profiles. Nevertheless, data indicate that approximately 28–40% of amateur, sub-elite, and elite female athletes using HCs use long-acting HCs and progestogen-only contraceptives (Langan-Evans et al., Citation2023; D. Martin et al., Citation2018; Oxfeldt et al., Citation2020). Given the distinctive properties of long acting and progestogen-only contraceptives and their relatively high usage rates, it is essential to comprehensively understand their impact on exercise performance.
The quality of the design and implementation of studies involving HCs (i.e., the standard of methodological control regarding ovarian hormonal profiles) is a topical theme to consider. A systematic review and meta-analysis conducted in 2020 assessing the influence of OCPs on exercise performance showed that 83% of studies demonstrated medium, low, or very low methodological quality (Elliott-Sale et al., Citation2020). Many of these articles failed to provide sufficient detail about the type of OCP used and the formulations of the contraceptive or length of usage, thus limiting study replication and the advancement of knowledge in the field. In 2022, an audit framework was developed to assess the representation of female athletes in sport science research (Smith et al., Citation2022). Within this audit, a tier system was created to rank studies using women based on the quality of methodological reporting for menstrual cycles, HCs, OCPs, and menstrual irregularities (Smith et al., Citation2022). This framework aligns with best practice recommendations from Elliott-Sale et al. (Citation2021).
Therefore, the aim of this audit was to assess the representation of HCs in research examining exercise performance in women. The secondary aim was to assess the quality of methods used in research on HCs and exercise performance. With the complex ovarian hormonal profiles of HCs and high usage of HCs among athletic women, this project provides a greater understanding of their representation and methodological quality within the exercise performance literature.
Methods
Study search and selection
An electronic literature search was initially conducted in June 2023 using PubMed, SPORT discus and Web of Science followed by a repeat search in July 2023. Citation tracking on Google Scholar was used to identify any missed studies. Studies considered for inclusion were original peer reviewed articles (review and conference abstracts excluded), written in English and full text accessible with no date restriction. Population, intervention, study outcomes, and design are detailed in and were used as the pre-defined inclusion criteria.
Table 2. Inclusion criteria based on population, intervention, study outcomes, and study design.
Search terms
Searches were conducted with the following terms: (“hormonal contraceptive” OR “oral contraceptives” OR “contraceptive injection” OR “contraceptive implant” OR “intrauterine system” OR “vaginal ring” OR “contraceptive patch” OR “hormone releasing intrauterine device” or “contraceptives”) AND (“athletic performance” OR “sport performance” OR “muscular strength” OR “strength training” OR “muscular force” OR “power” OR “anaerobic” OR “anaerobic power” OR “anaerobic performance” OR “anaerobic capacity” OR “aerobic” OR “aerobic capacity” OR “aerobic power” OR “aerobic performance” OR “endurance” OR “endurance capacity” OR “endurance power” OR “endurance performance” OR “fatigue” OR “recovery”).
Screening and selection
Rayyan software (https://www.rayyan.ai/) was used for the initial screening of the title and abstract. Searches from PubMed, SPORT discus and Web of Science were imported into the software and duplicates removed. Two researchers (TF, EC) independently screened each paper based on the predefined criteria (). Any conflicts were discussed and resolved between the two researchers; any continued conflicts were resolved by an independent researcher. Both researchers conducted full-text reviews.
Audit outcomes
The current study follows the recently published audit framework by Smith et al. (Citation2022), with the following additions – type of HC and study design – and exceptions – study impact. These amendments were made to satisfy the current research question (i.e., with a greater focus on HCs than overall menstrual status).
Outcome 1. Type of hormonal contraceptive (HC)
The type of HC(s) used by study participants was extracted from each paper. The options were taken from with the addition of options for un-specified HCs and un-specified OCPs (i.e., no further details were provided). To align with recent methodological recommendations for HC reporting (Elliott-Sale et al., Citation2021), brand and/or formulation and time since start of use was reported for each HC. In addition, a frequency count of the number of hormonal contraceptives included in the study is presented.
Outcome 2. Sample size and calibre of athlete
The number of women using each form of HCs was extracted from every paper alongside the total sample size. In addition, all details about participant training calibre were extracted from each paper. Using the information identified in the studies, each population was allocated an athlete calibre tier using an established framework (McKay et al., Citation2022). If no information was provided about athlete calibre, the sample was classified as “did not state”. For reference, the athlete calibre system has 5 tiers (see full text for inclusion criteria): Tier 0 (sedentary); Tier 1 (recreationally active); Tier 2 (trained/developmental); Tier 3 (highly trained/national); Tier 4 (elite/international); and Tier 5 (world-class) (McKay et al., Citation2022).
Outcome 3. Outcome of the study
The performance outcome of the study was extracted from each paper and classified into the categories stated in .
Outcome 4. Study design
How the use of HCs was incorporated within the research design of the study was extracted for each paper which specified HC type, which resulted in four categories (listed below with examples).
HCs separated into single groups (For example: separate groups of women using monophasic OCPs and progestogen only pills).
Grouped with other HCs (For example: women taking monophasic OCPs grouped with women using vaginal rings or progestogen only pills).
Grouped with eumenorrheic women (For example: women taking OCPs grouped with eumenorrheic women).
Grouped with men (For example: All participants in the study grouped together).
Outcome 5. Quality of methodological control
The quality of methodological control was assessed by two authors using an adapted version of the tier ranking system designed by Smith et al. (Citation2022), both authors independently assessed all papers to ensure agreement. All studies were ranked using both the specific criteria for HC reporting (n = 61 studies ranked) and for OCP reporting (n = 60 studies ranked). Studies were ranked with both, to highlight the stricter criteria for OCP research to ensure homogeneity within participants using OCPs (). Based on the criteria in , studies were awarded either Gold, Silver, Bronze, or ungraded Tier. The annual cumulative paper count was calculated by summing the number of studies each year, while the methodological quality over time was assessed by calculating the percentages of gold, silver, bronze, and ungraded studies.
Table 3. Criteria for each tier system for quality of methodological control adapted from Smith et al., Citation2022 based on Elliott-Sale et al., Citation2021.
Results
The results from the identification and search strategy are presented in . summarises the studies included in the audit and the main outcomes.
Figure 1. Flow diagram of studies.
Table 4. All studies included in the audit and the outcomes.
Outcome 1. Type of hormonal contraceptive
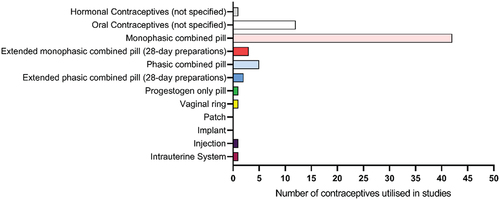
In total, the 61 studies involved 68 separate investigations of HC use (). The most commonly investigated HCs were monophasic combined OCPs, which were reported 41 times (60% of studies) followed by un-specified OCPs, which were reported 12 times. Other OCPs were reported sparingly (extended monophasic combined pills (28-days) = 3, phasic combined = 5 and extended phasic combined (28-day) = 2 and progestogen only pills = 1). Cyclic contraceptives were reported once (vaginal ring = 1) and long acting reversible contraceptives twice (Injection = 1, Intrauterine system = 1). One paper provided no details of type of HC, so was categorised as un-specified HCs. Brand of HC was provided for 21 out of 68 investigations of contraceptives. When the brand was not recorded, the composition or formulation of the HC was provided for 27 out of 47 contraceptives. Time since start of use was included in 54 out of 61 studies. Out of the 60 studies which specified HC type (including un-specified oral contraceptives), n = 54 reported one type of HC, n = 5 reported two types and n = 1 reported three types.
Figure 2. Types of HCs investigated in the studies within the audit.
Outcome 2. Sample size and calibre of athlete
In total, 773 participants used HCs out of 1564 participants who participated in the 61 studies (49%). Out of 61 papers included in the audit, 13 assessed only women using HCs, whilst 48 assessed women using HCs, alongside either women not using HCs or men. The lowest sample size of HC users was n = 5 from a total of 15 participants, which the highest involved n = 43 from a total of 82 participants. Out of 773 participants, 83 participants (11%) were unable to be classified into an athlete calibre tier. Out of the remaining 690 participants: 178 (26%) were classified as Tier 0 (sedentary); 272 (39%) were classified as Tier 1 (recreationally active); 159 (23%) were classified as Tier 2 (trained/developmental); 59 (9%) were classified as Tier 3 (highly trained/national); 22 (3%) were classified as Tier 4 (elite/international); and 0 were classified as Tier 5 (world-class).
Outcome 3. Outcome of the study
In total, 8 different outcomes were investigated across the 61 studies. From highest to lowest, 17 studies had endurance performance/capacity outcomes, 17 had muscular strength outcomes, 10 had sports performance outcomes, 5 had anaerobic power/performance outcomes, 4 had strength training outcomes, 4 had aerobic power/performance outcomes, 4 had fatigue/recovery outcomes.
Outcome 4. Study design
shows the breakdown of the studies by study design; 85% of studies included in the audit (including studies with un-specified HC and OCPs) split different types of HCs into individual groups, with 11% of studies grouping different contraceptives together, 3% grouping HCs with eumenorrheic women, and 0% grouping HCs with men. In addition, although no studies grouped HCs with men, some studies did include men who were grouped separately.
Figure 3. Study design: how the HCs were incorporated within the research design of the study.
Outcome 5. Quality of methodological control
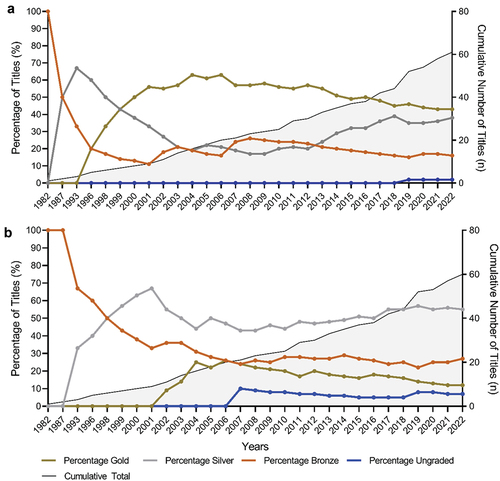
Quality of methodological control was assessed using the criteria outlined by Smith et al. (Citation2022) for HCs () and specifically for OCPs (). When assessed against the HC criteria, 43% of studies were awarded gold tier, 38% silver tier, 16% bronze tier, and 3% ungraded. When assessed against the OCP criteria, 12% of studies were awarded gold tier, 55% silver tier, 27% bronze tier, and 7% ungraded. shows the yearly distribution of tier rankings for HCs () and specifically for OCPs () alongside the yearly distribution frequency of publications since 1982. Percentage of gold rankings has not improved since 2003. When assessed against the HC criteria, gold rankings accounted for in 57% in 2003, 55% in 2011, 43% in 2022. When assessed against the OCP criteria gold rankings accounted for in 14% in 2003, 17% in 2011, 12% in 2022.
Figure 4. Standard of methodological control when assessed by (a) HC tier system and (b) OCP tier system.
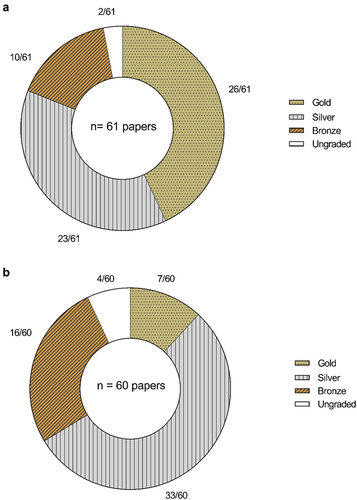
Figure 5. Yearly distribution of tier rankings for (a) HCs and (b) OCPs specifically alongside the cumulative total of papers.
Discussion
The study aimed to assess the representation of HC use by female participants involved in research examining exercise performance, with a secondary objective of evaluating the quality of methods used in research on HCs and exercise performance. The main finding of this audit is the predominant focus on monophasic combined OCPs in research, while cyclic and long-acting reversible contraceptives are notably underrepresented, being investigated in less than 5% of all studies of HCs. In addition, female athletes are underrepresented in the literature examining HCs and exercise, the majority (70%) of research participants in the available literature were either unclassified, sedentary (Tier 0) or recreationally active (Tier 1). Indeed, elite athletes (Tier 4) account for only 3% of the populations studied and no studies have included world-class athletes (Tier 5).
Monophasic OCPs represented 60% of the HCs investigated in the studies included in the audit, with ~34% being other forms of OCPs [phasic, extended, progestogen-only, or unspecified]. Conversely, less than 5% of the HCs used in the studies included in the audit were long-acting reversible or cyclic contraceptives. This is noteworthy, given that recent studies, such as Langan-Evans et al. (Citation2023), have indicated a substantial uptake of the use of non-OCPs in athletic populations sampled in the UK (42%), including intrauterine devices/systems (IUD/IUS): 21%; implants (17%); injections (3%); and vaginal rings (1%). Similar numbers were shown in studies in other countries: Denmark; ~20% (Oxfeldt et al., Citation2020), Australia ~20% (Clarke et al., Citation2021), Sweden ~44% (Ekenros et al., Citation2022). Given the unique properties of each type of HC (i.e., variability in delivery methods and exogenous hormone profiles), there is an imperative need to expand future research to include a broader range of HC types, including cyclic and long-acting reversible options that are currently prevalent. This comprehensive approach is vital for understanding the distinct influences of each contraceptive method on exercise performance.
It should be noted that the studies included in this audit span 37 years and therefore include a range of older and newer HC formulations. Any obsolete HCs included in this audit are not intended to represent or to be considered in the same way as current HCs, rather their inclusion charts the historical timeline of research in this area and highlights the need for future research to not just consider the trend in the types of HCs used by active women but also the advances and evolution of HC formulations.
Most studies included in this audit focussed on sedentary and recreationally active participants (Tier 0 and Tier 1 ~ 58% overall participants); compared with 21% trained/development (Tier 2), 8% highly trained/national (Tier 3) and 3% elite athletes (Tier 4). However, 11% of participants were unable to be classified due to the lack of information on athlete training status, potentially over or underestimating the reported categories. Therefore, it is crucial that future research provides sufficient information regarding participant characteristics and training level (see McKay et al. (Citation2022) for full details). Several studies (Clarke et al., Citation2021; Langan-Evans et al., Citation2023; Oxfeldt et al., Citation2020; Parker et al., Citation2022), have reported varying usage rates of HCs in elite athletes, with Langan-Evans et al. (Citation2023) indicating a prevalence of 37% among the elite population. This disparity raises concerns, given the physiological and training discrepancies between elite athletes and recreational participants and the lack of research in elite populations (3%). Consequently, findings from research involving sedentary or recreational populations may not be directly applicable to elite athletes (Burden et al., Citation2021). Therefore, there is a compelling need for future research, specifically tailored to elite athletes using HCs, to comprehensively understand the physiological effects of HC on high-level exercise performance. Such research is essential for providing evidence-based guidelines that are directly relevant to all athletic populations.
Over the past decade (2011–2022), there has been a notable surge in the annual publication of research studies in this area, averaging approximately 3 studies per year, compared to the preceding 15 years (1996–2010), which showed an average of approximately 1.5 studies per year (). Here, we note that the first study for inclusion in the audit was published in 1987; more than two decades after the introduction of HCs to market in most countries. Despite this surge in research output, the number of studies achieving a gold ranking has not improved since 2003. When assessed against the HC criteria, gold rankings accounted for 57% of studies published in 2003, 55% in 2011, and 43% in 2022. When assessed against the OCP criteria, gold rankings accounted for 14% in 2003, 17% in 2011, and 12% in 2022. Notably, within the reviewed literature, one paper omitted the specification of the HC type employed in the study, and twelve studies omitted the specification of OCP type emphasising the need for comprehensive reporting of HC details. Another study included a participant using a vaginal ring with a group of participants using monophasic OCPs; however, despite both being combined contraceptives, they have distinct differences in concentrations of exogenous hormones and delivery/timing of these hormones. These findings highlight the opportunity for improvement in methodological quality and reinforce the imperative for future research to encompass all relevant information regarding HC usage.
All studies were evaluated using the HC and OCP guidelines (Smith et al., Citation2022). When evaluated using only the HC guidelines, 43% of studies achieved a gold-tier rating. In contrast, only 12% of studies attain a gold-tier rating when assessed against OCP guidelines. This discrepancy highlights the stricter criteria of the OCP guidelines, twenty studies were demoted from gold to silver ranking when assessed against the OCP guidelines. Within these twenty, three studies failed to account for active/inactive days (Bryner et al., Citation1996; Gordon et al., Citation2017; Vaiksaar et al., Citation2011), thirteen studies included more than one contraceptive generation (Elliott et al., Citation2005; Isacco et al., Citation2015; Joyce et al., Citation2013; Lynch & Nimmo, Citation1998; Lynch et al., Citation2001; Mackay et al., Citation2019; Mattu et al., Citation2020; Rechichi & Dawson, Citation2012; Rechichi et al., Citation2008; Sunderland & Nevill, Citation2003; Sunderland et al., Citation2011; Thompson et al., Citation2021) and four studies did both (Dalgaard et al., Citation2019; Giacomoni & Falgairette, Citation1999; Giacomoni et al., Citation2000; Lei et al., Citation2019). This implies that the number of studies ranked as gold could potentially have increased from 7 to 27, which would equate to nearly 45% of studies achieving a gold ranking if authors had included details about active and inactive pill phases and had separated different generations of pills. Separation of pill generations is recommended due to variations in endogenous hormone concentrations, progestin potency, androgenic and antiestrogenic properties (Elliott-Sale et al., Citation2013, Citation2021). Furthermore, it is crucial to emphasise that achieving a gold ranking in reporting criteria does not require time-consuming or resource-intensive procedures. Researchers can meet these criteria by providing essential information on HCs, including details such as type, formula, brand, duration of usage, and specification of active and inactive pill phases. Additionally, research quality significantly benefits from avoiding the combination of different generations of OCPs within the same group. We acknowledge that, with the many formulations of OCPs available to women, restricting participants to one generation of combined monophasic OCP may limit the potential sample size, increase the time taken to recruit and complete the study, and possibly inflate study costs, however, by restricting to one generation methodological quality (i.e., homogeneity) will be improved. There is a compelling need to enhance the quality and reporting standards of HC research. The limitations identified during this audit can provide valuable insight to inform decisions for shaping the direction of future research methods and ensuring the production of high-quality information on HCs and exercise performance which can be effectively utilised.
Another limitation in the current body of research on HCs and exercise performance is the predominant focus on certain outcome measures; specifically, out of the 61 total studies included in the audit, a high percentage were focused on endurance performance (28%) and muscular strength (28%) outcomes. The high concentration of research into these areas may not provide a comprehensive understanding of the potential effects of HCs on various aspects of exercise performance such as fatigue, recovery, and training. In addition, only three studies included HCs other than OCPs (n = 1 intrauterine system, n = 1 injection and n = 1 vaginal ring), in two of these studies these HCs were grouped with a form of OCP, which may limit our insights into the unique impacts phasic and long acting reversible contraceptives. To further advance knowledge in the field, researchers should diversify their approach to include various types of HCs across a broader range of outcome measures, this comprehensive approach will contribute to our understanding of how HCs may influence various types of exercise performance.
In conclusion, this audit highlights the need for greater diversity in the types of HCs investigated or included in exercise research, particularly the inclusion of cyclic and long-acting reversible options. It also underscores the importance of conducting research on all populations, including elite populations, to ensure findings are applicable to these specific population requirements. Furthermore, the audit emphasises the value of improving reporting standards and methodological rigour in HC research, with recognition that achieving these standards often requires small and simple adjustments. These improvements are essential to enhance the quality and comparability of future findings.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Ali, A., O’Donnell, J., Foskett, A., & Rutherfurd-Markwick, K. (2016). The influence of caffeine ingestion on strength and power performance in female team-sport players. Journal of the International Society of Sports Nutrition, 13(1), 1–9. https://doi.org/10.1186/s12970-016-0157-4
- Anderson, L. J., Baker, L. L., & Schroeder, E. T. (2017). Blunted myoglobin and quadriceps soreness after electrical stimulation during the luteal phase or oral contraception. Research Quarterly for Exercise and Sport, 88(2), 193–202. https://doi.org/10.1080/02701367.2017.1300229
- Armstrong, L. E., Maresh, C. M., Keith, N. R., Elliott, T. A., Vanheest, J. L., Scheett, T. P., Stoppani, J., Judelson, D. A., & de Souza, M. J. (2005). Heat acclimation and physical training adaptations of young women using different contraceptive hormones. American Journal of Physiology: Endocrinology and Metabolism, 288(5), E868–75. https://doi.org/10.1152/ajpendo.00434.2004
- Bell, D. R., Troy Blackburn, J., Ondrak, K. S., Hackney, A. C., Hudson, J. D., Norcross, M. F., & Padua, D. A. (2011). The effects of oral contraceptive use on muscle stiffness across the menstrual cycle. Clinical Journal of Sport Medicine, 21(6), 467–473. https://doi.org/10.1097/JSM.0b013e318230f50a
- Bozzini, B. N., McFadden, B. A., Elliott-Sale, K. J., Swinton, P. A., & Arent, S. M. (2021). Evaluating the effects of oral contraceptive use on biomarkers and body composition during a competitive season in collegiate female soccer players. Journal of Applied Physiology, 130(6), 1971–1982. https://doi.org/10.1152/japplphysiol.00818.2020
- Brown, N., Roldan-Reoyo, O., Williams, G. K. R., Stodter, A., Izzy, S., Mackintosh, K. A., McNarry, M. A., & Williams, E. M. P. (2023). Profiling hormonal contraceptive use and perceived impact on training and performance in a global sample of women rugby players submission type: Original investigation Applied Sports, Technology, Exercise and Medicine (A-STEM) research centre, swans. International Journal of Sports Physiology & Performance, 18(9), 937–943. https://doi.org/10.1123/ijspp.2023-0137
- Bryner, R. W., Toffle, R. C., Ullrich, I. H., & Yeater, R. A. (1996). Effect of low dose oral contraceptives on exercise performance. British Journal of Sports Medicine, 30(1), 36–40. https://doi.org/10.1136/bjsm.30.1.36
- Burden, R. J., Shill, A. L., & Bishop, N. C. (2021). Elite female athlete research: Stop searching for the ‘magic P ’. Experimental Physiology, 106(10), 2029–2030. https://doi.org/10.1113/EP089884
- Casazza, G. A., Suh, S. H., Miller, B. F., Navazio, F. M., & Brooks, G. A. (2002). Effects of oral contraceptives on peak exercise capacity. Journal of Applied Physiology, 93(5), 1698–1702. https://doi.org/10.1152/japplphysiol.00622.2002
- Clarke, A. C., Bruinvels, G., Julian, R., Inge, P., Pedlar, C. R., & Govus, A. D. (2021). Hormonal contraceptive use in football codes in Australia. Frontiers in Sports and Active Living, 3(February), 1–7. https://doi.org/10.3389/fspor.2021.634866
- Dalgaard, L. B., Dalgas, U., Andersen, J. L., Rossen, N. B., Møller, A. B., Stødkilde Jørgensen, H., Jørgensen, J. O., Kovanen, V., Couppé, C., Langberg, H., Kjær, M., & Hansen, M. (2019). Influence of oral contraceptive use on adaptations to resistance training. Frontiers in Physiology, 10(July), 1–14. https://doi.org/10.3389/fphys.2019.00824
- Dam, T. V., Dalgaard, L. B., Sevdalis, V., Bibby, B. M., Janse De Jonge, X., Gravholt, C. H., & Hansen, M. (2022). Muscle performance during the menstrual cycle correlates with psychological well-being, but not fluctuations in sex hormones. Medicine and Science in Sports and Exercise, 54(10), 1678–1689. https://doi.org/10.1249/MSS.0000000000002961
- Drake, S. M., Evetovich, T., Eschbach, C., & Webster, M. (2003). A pilot study on the effect of oral contraceptives on electromyography and mechanomyography during isometric muscle actions. Journal of Electromyography and Kinesiology, 13(3), 297–301. https://doi.org/10.1016/S1050-6411(03)00024-5
- Ekenros, L., Hirschberg, A. L., Heijne, A., & Fridén, C. (2013). Oral contraceptives do not affect muscle strength and hop performance in active women. Clinical Journal of Sport Medicine, 23(3), 202–207. https://doi.org/10.1097/JSM.0b013e3182625a51
- Ekenros, L., von Rosen, P., Solli, G. S., Sandbakk, Ø., Holmberg, H. C., Hirschberg, A. L., & Fridén, C. (2022). Perceived impact of the menstrual cycle and hormonal contraceptives on physical exercise and performance in 1,086 athletes from 57 sports. Frontiers in Physiology, 13(August), 1–13. https://doi.org/10.3389/fphys.2022.954760
- Elliott, K. J., Cable, N. T., & Reilly, T. (2005). Does oral contraceptive use affect maximum force production in women? British Journal of Sports Medicine, 39(1), 15–19. https://doi.org/10.1136/bjsm.2003.009886
- Elliott-Sale, K. J., McNulty, K. L., Ansdell, P., Goodall, S., Hicks, K. M., Thomas, K., Swinton, P. A., & Dolan, E. (2020). The effects of oral contraceptives on exercise performance in women: A systematic review and meta-analysis. Sports Medicine, 50(10), 1785–1812. https://doi.org/10.1007/s40279-020-01317-5
- Elliott-Sale, K. J., Minahan, C. L., Janse de Jonge, X. A. K., Ackerman, K. E., Sipilä, S., Constantini, N. W., Lebrun, C. M., & Hackney, A. C. (2021). Methodological considerations for studies in sport and exercise science with women as participants: A working guide for standards of practice for research on women. Sports Medicine, 51(5), 843–861. https://doi.org/10.1007/s40279-021-01435-8
- Elliott-Sale, K. J., Smith, S., Bacon, J., Clayton, D., McPhilimey, M., Goutianos, G., Hampson, J., & Sale, C. (2013). Examining the role of oral contraceptive users as an experimental and/or control group in athletic performance studies. Contraception, 88(3), 408–412. https://doi.org/10.1016/j.contraception.2012.11.023
- Giacomoni, M., Bernard, T., Gavarry, O., Altare, S., & Falgairette, G. (2000). Influence of the menstrual cycle phase and menstrual symptoms on maximal anaerobic performance. Medicine and Science in Sports and Exercise, 32(2), 486–492. https://doi.org/10.1097/00005768-200002000-00034
- Giacomoni, M., & Falgairette, G. (1999). Influence of menstrual cycle phase and oral contraceptive use on the time-of-day effect on maximal anaerobic power. Biological Rhythm Research, 30(5), 583–591. https://doi.org/10.1076/brhm.30.5.583.1407
- Gordon, D., Hughes, F., Young, K., Scruton, A., Keiller, D., Caddy, O., Baker, J., & Barnes, R. (2013). The effects of menstrual cycle phase on the development of peak torque under isokinetic conditions. Isokinetics and Exercise Science, 21(4), 285–291. https://doi.org/10.3233/IES-130499
- Gordon, D., Scruton, A., Barnes, R., Baker, J., Prado, L., & Merzbach, V. (2017). The effects of menstrual cycle phase on the incidence of plateau at V˙O2max and associated cardiorespiratory dynamics. Clinical Physiology and Functional Imaging, 38(4), 689–698. https://doi.org/10.1111/cpf.12469
- Grucza Pekkarinen, H., Titov, E., Hanninen, A., & Kononoff, O. R. (1993). Influence of the menstrual cycle and oral contraceptives on thermoregulatory responses to exercise in young women. European Journal of Applied Physiology, 67(3), 279–285. https://doi.org/10.1007/BF00864229
- Hicks, K. M., Onambele-Pearson, G., Winwood, K., & Morse, C. I. (2017). Oral contraceptive pill use and the susceptibility to markers of exercise-induced muscle damage. European Journal of Applied Physiology, 117(7), 1393–1402. https://doi.org/10.1007/s00421-017-3629-6
- Isacco, L., Thivel, D., Pereira, B., Duclos, M., & Boisseau, N. (2015). Maximal fat oxidation, but not aerobic capacity, is affected by oral contraceptive use in young healthy women. European Journal of Applied Physiology, 115(5), 937–945. https://doi.org/10.1007/s00421-014-3075-7
- Joyce, S., Sabapathy, S., Bulmer, A., & Minahan, C. (2013). Effect of long-term oral contraceptive use on determinants of endurance performance. Journal of Strength and Conditioning Research, 27(7), 1891–1896. https://doi.org/10.1519/JSC.0b013e3182736935
- Joyce, S., Sabapathy, S., Bulmer, A. C., & Minahan, C. (2014). The effect of prior eccentric exercise on heavy-intensity cycling: The role of gender and oral contraceptives. European Journal of Applied Physiology, 114(5), 995–1003. https://doi.org/10.1007/s00421-014-2832-y
- Langan-Evans, C., Hearris, M. A., McQuilliam, S., Burke, L. M., Stellingwerff, T., Elliott-Sale, K. J., & Morton, J. P. (2023). Hormonal contraceptive use, menstrual cycle characteristics and training/nutrition related profiles of elite, sub-elite and amateur athletes and exercisers: One size is unlikely to fit all. International Journal of Sports Science and Coaching, 19(1), 113–128. https://doi.org/10.1177/17479541231163088
- Lebrun, C. M., Petit, M. A., McKenzie, D. C., Taunton, J. E., & Prior, J. C. (2003). Decreased maximal aerobic capacity with use of a triphasic oral contraceptive in highly active women: A randomised controlled trial. British Journal of Sports Medicine, 37(4), 315–320. https://doi.org/10.1136/bjsm.37.4.315
- Lee, H., Petrofsky, J. S., Daher, N., Berk, L., & Laymon, M. (2014). Differences in anterior cruciate ligament elasticity and force for knee flexion in women: Oral contraceptive users versus non-oral contraceptive users. European Journal of Applied Physiology, 114(2), 285–294. https://doi.org/10.1007/s00421-013-2771-z
- Lei, T. H., Cotter, J. D., Schlader, Z. J., Stannard, S. R., Perry, B. G., Barnes, M. J., & Mündel, T. (2019). On exercise thermoregulation in females: Interaction of endogenous and exogenous ovarian hormones. Journal of Physiology, Paris, 597(1), 71–88. https://doi.org/10.1113/JP276233
- Loureiro, S., Dias, I., Sales, D., Alessi, I., Simão, R., & Fermino, R. C. (2011). Efeito das diferentes fases do ciclo menstrual no desempenho da força muscular em 10RM. Revista Brasileira de Medicina do Esporte, 17(1), 22–25. http://www.scielo.br/pdf/rbme/v17n1/en_v17n1a04.pdf
- Lynch, N. J., de Vito, G., & Nimmo, M. A. (2001). Low dosage monophasic oral contraceptive use and intermittent exercise performance and metabolism in humans. European Journal of Applied Physiology, 84(4), 296–301. https://doi.org/10.1007/s004210000380
- Lynch, N. J., & Nimmo, M. A. (1998). Effects of menstrual cycle phase and oral contraceptive use on intermittent exercise. European Journal of Applied Physiology and Occupational Physiology, 78(6), 565–572. https://doi.org/10.1007/s004210050462
- Mackay, K., González, C., Zbinden Foncea, H., & Peñailillo, L. (2019). Effects of oral contraceptive use on female sexual salivary hormones and indirect markers of muscle damage following eccentric cycling in women. European Journal of Applied Physiology, 119(11–12), 2733–2744. https://doi.org/10.1007/s00421-019-04254-y
- Martin, A. C., Heazlewood, I. T., Kitic, C. M., Lys, I., & Johnson, L. (2019). Possible hormone predictors of physical performance in adolescent team sport athletes. Journal of Strength and Conditioning Research, 33(2), 417–425. https://doi.org/10.1519/JSC.0000000000002014
- Martin, D., Sale, C., Cooper, S. B., & Elliott-Sale, K. J. (2018). Period prevalence and perceived side effects of hormonal contraceptive use and the menstrual cycle in elite athletes. International Journal of Sports Physiology and Performance, 13(7), 926–932. https://doi.org/10.1123/ijspp.2017-0330
- Mattu, A. T., Iannetta, D., MacInnis, M. J., Doyle-Baker, P. K., & Murias, J. M. (2020). Menstrual and oral contraceptive cycle phases do not affect submaximal and maximal exercise responses. Scandinavian Journal of Medicine and Science in Sports, 30(3), 472–484. https://doi.org/10.1111/sms.13590
- McKay, A. K. A., Stellingwerff, T., Smith, E. S., Martin, D. T., Mujika, I., Goosey-Tolfrey, V. L., Sheppard, J., & Burke, L. M. (2022). Defining training and performance caliber: A participant classification framework. International Journal of Sports Physiology and Performance, 17(2), 317–331. https://doi.org/10.1123/ijspp.2021-0451
- Minahan, C., Joyce, S., Bulmer, A. C., Cronin, N., & Sabapathy, S. (2015). The influence of estradiol on muscle damage and leg strength after intense eccentric exercise. European Journal of Applied Physiology, 115(7), 1493–1500. https://doi.org/10.1007/s00421-015-3133-9
- Myllyaho, M. M., Ihalainen, J. K., Hackney, A. C., Valtonen, M., Nummela, A., Vaara, E., Hakkinen, K., Kyrolainen, H., & Taipale-Mikkonen, R. S. (2021). Hormonal contraceptive user does not affect strength, endurance, or body composition adaptations to combined strength and endurance training in women. The Journal of Strength & Conditioning Research, 35(2), 449–457. https://doi.org/10.1519/JSC.0000000000002713
- Nichols, A. W., Hetzler, R. K., Villanueva, R. J., Stickley, C. D., & Kimura, I. F. (2008). Effects of combination oral contraceptives on strength development in women athletes. Journal of Strength and Conditioning Research, 22(5), 1625–1632. https://doi.org/10.1519/JSC.0b013e31817ae1f3
- Nicolay, C. W., Kenney, J. L., & Lucki, N. C. (2007). Grip strength and endurance throughout the menstrual cycle in eumenorrheic and women using oral contraceptives. International Journal of Industrial Ergonomics, 37(4), 291–301. https://doi.org/10.1016/j.ergon.2006.11.004
- Notelovitz, M., Zauner, C., McKenzie, L., Suggs, Y., Fields, C., & Kitchens, C. (1987). The effect of low-dose oral contraceptives on cardiorespiratory function, coagulation, and lipids in exercising young women: A preliminary report. Obstetrical and Gynecological Survey, 43(5), 304–305. https://doi.org/10.1097/00006254-198805000-00018
- Oxfeldt, M., Dalgaard, L. B., Jørgensen, A. A., & Hansen, M. (2020). Hormonal contraceptive use, menstrual dysfunctions, and self-reported side effects in elite athletes in Denmark. International Journal of Sports Physiology and Performance, 15(10), 1377–1384. https://doi.org/10.1123/ijspp.2019-0636
- Parker, L. J., Elliott-Sale, K. J., Hannon, M. P., Morton, J. P., & Close, G. L. (2022). An audit of hormonal contraceptive use in women’s super league soccer players; implications on symptomology. Science and Medicine in Football, 6(2), 153–158. https://doi.org/10.1080/24733938.2021.1921248
- Peters, C., & Burrows, M. (2006). Androgenicity of the progestin in oral contraceptives does not affect maximal leg strength. Contraception, 74(6), 487–491. https://doi.org/10.1016/j.contraception.2006.08.005
- Quinn, K. M., Billaut, F., Bulmer, A. C., & Minahan, C. L. (2018). Cerebral oxygenation declines but does not impair peak oxygen uptake during incremental cycling in women using oral contraceptives. European Journal of Applied Physiology, 118(11), 2417–2427. https://doi.org/10.1007/s00421-018-3968-y
- Rebelo, A. C. S., Zuttin, R. S., Verlengia, R., Cesar, M. D. C., de Sá, M. F. S., & da Silva, E. (2010). Effect of low-dose combined oral contraceptive on aerobic capacity and anaerobic threshold level in active and sedentary young women. Contraception, 81(4), 309–315. https://doi.org/10.1016/j.contraception.2009.11.005
- Rechichi, C., & Dawson, B. (2009). Effect of oral contraceptive cycle phase on performance in team sport players. Journal of Science and Medicine in Sport, 12(1), 190–195. https://doi.org/10.1016/j.jsams.2007.10.005
- Rechichi, C., & Dawson, B. (2012). Oral contraceptive cycle phase does not affect 200-m swim time trial performance. Journal of Strength and Conditioning Research, 26(4), 961–967. https://doi.org/10.1519/JSC.0b013e31822dfb8b
- Rechichi, C., Dawson, B., & Goodman, C. (2008). Oral contraceptive phase has no effect on endurance test. International Journal of Sports Medicine, 29(4), 277–281. https://doi.org/10.1055/s-2007-965334
- Redman, L. M., & Weatherby, R. P. (2004). Measuring performance during the menstrual cycle: A model using oral contraceptives. Medicine and Science in Sports and Exercise, 36(1), 130–136. https://doi.org/10.1249/01.MSS.0000106181.52102.99
- Rickenlund, A., Carlström, K., Ekblom, B., Brismar, T. B., Von Schoultz, B., & Hirschberg, A. L. (2004). Effects of oral contraceptives on body composition and physical performance in female athletes. Journal of Clinical Endocrinology and Metabolism, 89(9), 4364–4370. https://doi.org/10.1210/jc.2003-031334
- Riechman, S. E., & Lee, C. W. (2022). Oral contraceptive use impairs muscle gains in young women. Journal of Strength and Conditioning Research, 36(11), 3074–3080. https://doi.org/10.1519/JSC.0000000000004059
- Rivera, R., Yacobson, I., & Grimes, D. (1999). The mechanism of action of hormonal contraceptives and intrauterine contraceptive devices. American Journal of Obstetrics and Gynecology, 181(5), 1263–1269. https://doi.org/10.1016/S0002-9378(99)70120-1
- Romance, R., Vargas, S., Espinar, S., Petro, J. L., Bonilla, D. A., Schöenfeld, B. J., Kreider, R. B., & Benítez-Porres, J. (2019). Oral contraceptive use does not negatively affect body composition and strength adaptations in trained women. International Journal of Sports Medicine, 40(13), 842–849. https://doi.org/10.1055/a-0985-4373
- Sarwar, R., Niclos, B. B., & Rutherford, O. M. (1996). Changes in muscle strength, relaxation rate and fatiguability during the human menstrual cycle. Journal of Physiology, Paris, 493(1), 267–272. https://doi.org/10.1113/jphysiol.1996.sp021381
- Savage, K. J., & Clarkson, P. M. (2002). Oral contraceptive use and exercise-induced muscle damage and recovery. Contraception, 66(1), 67–71. https://doi.org/10.1016/S0010-7824(02)00320-7
- Schaumberg, M. A., Jenkins, D. G., Janse de Jonge, X. A. K., Emmerton, L. M., & Skinner, T. L. (2017). Oral contraceptive use dampens physiological adaptations to sprint interval training. Medicine and Science in Sports and Exercise, 49(4), 717–727. https://doi.org/10.1249/MSS.0000000000001171
- Simpson, C. L., Flatman, M. M., Kim, B. D. H., Bouwmeester, N. M., & Jakobi, J. M. (2018). Increase in post activation potentiation in females following a cycling warmup. Human Movement Science, 57(November), 171–177. https://doi.org/10.1016/j.humov.2017.12.003
- Sims, S. T., Rehrer, N. J., Bell, M. L., & Cotter, J. D. (2007). Preexercise sodium loading aids fluid balance and endurance for women exercising in the heat. Journal of Applied Physiology, 103(2), 534–541. https://doi.org/10.1152/japplphysiol.01203.2006
- Smith, E. S., McKay, A. K. A., Ackerman, K. E., Harris, R., Elliott-Sale, K. J., Stellingwerff, T., & Burke, L. M. (2022). Methodology review: A protocol to audit the representation of female athletes in sports science and sports medicine research. International Journal of Sport Nutrition and Exercise Metabolism, 32(2), 114–127. https://doi.org/10.1123/ijsnem.2021-0257
- Sousa, M., Dellagrana, R., Lunardi, M., Rossato, M., Hoinaski, L., Bento, C., & Freitas, C. (2020). Menstrual cycle and use of different doses of oral contraceptive do not affect torque parameters in strength training programs. Motricidade, 16(2), 176–183. https://doi.org/10.6063/motricidade.18181
- Sunderland, C., & Nevill, M. (2003). Effect of the menstrual cycle on performance of intermittent, high intensity. European Journal of Applied Physiology, 88(4), 345–352. https://doi.org/10.1007/s00421-002-0722-1
- Sunderland, C., Tunaley, V., Horner, F., Harmer, D., & Stokes, K. A. (2011). Menstrual cycle and oral contraceptives’ effects on growth hormone response to sprinting. Applied Physiology, Nutrition and Metabolism, 36(4), 495–502. https://doi.org/10.1139/h11-039
- Sung, E. S., Han, A., Hinrichs, T., Vorgerd, M., & Platen, P. (2022). Effects of oral contraceptive use on muscle strength, muscle thickness, and fiber size and composition in young women undergoing 12 weeks of strength training: A cohort study. BMC Women’s Health, 22(1), 1–10. https://doi.org/10.1186/s12905-022-01740-y
- Taipale-Mikkonen, R. S., Raitanen, A., Hackney, A. C., Solli, G. S., Valtonen, M., Peltonen, H., McGawley, K., Kyröläinen, H., & Ihalainen, J. K. (2021). Influence of menstrual cycle or hormonal contraceptive phase on physiological variables monitored during treadmill testing. Frontiers in Physiology, 12(December), 1–10. https://doi.org/10.3389/fphys.2021.761760
- Thompson, B. M., Drover, K. B., Stellmaker, R. J., Sculley, D. V., & Janse de Jonge, X. A. K. (2021). The effect of the menstrual cycle and oral contraceptive cycle on muscle performance and perceptual measures. International Journal of Environmental Research and Public Health, 18(20), 10565. https://doi.org/10.3390/ijerph182010565
- Vaiksaar, S., Jurimae, J., Maestu, J., Purge, P., Kalytka, S., Shakhlina, L., & Jurimae, T. (2011). No effect of menstrual cycle phase and oral contraceptive use on endurance performance in rowers. Journal of Strength and Conditioning Research, 25(6), 1571–1578. https://doi.org/10.1519/JSC.0b013e3181df7fd2
- Weidauer, L., Zwart, M. B., Clapper, J., Albert, J., Vukovich, M., & Specker, B. (2020). Neuromuscular performance changes throughout the menstrual cycle in physically active females. Journal of Musculoskeletal & Neuronal Interactions, 20(3), 314–324. https://doi.org/10.1249/01.mss.0000486533.03765.e3
- Wickham, K. A., McCarthy, D. G., Pereira, J. M., Cervone, D. T., Verdijk, L. B., van Loon, L. J. C., Power, G. A., & Spriet, L. L. (2019). No effect of beetroot juice supplementation on exercise economy and performance in recreationally active females despite increased torque production. Physiological Reports, 7(2), 1–14. https://doi.org/10.14814/phy2.13982
- Wirth, J., & Lohman, T. (1982). The relationship of static muscle function to use oral contraceptives. Medicine & Science in Sport and Exercise, 14(1), 16–20. https://doi.org/10.1249/00005768-198201000-00003
- Yanovich, R., Ketko, I., Muginshtein-Simkovitch, J., Yanovich, E., Eliyahu, U., Fleischmann, C., Atias-Varon, D., Waissengrin, B., Makranz, C., & Heled, Y. (2019). Physiological differences between heat tolerant and heat intolerant young healthy women. Research Quarterly for Exercise and Sport, 90(3), 307–317. https://doi.org/10.1080/02701367.2019.1599799