
ABSTRACT
Aims/Background
Studies on the association between perineal trauma (episiotomy and tear) and the risk of postpartum depression in Omani mothers are scarce. This study aimed to screen women for the risk of postpartum depression and associated maternal adverse outcomes (episiotomy and tear) in newly delivered Omani mothers.
Design/Methods
Mothers were screened for postpartum depression using only the Edinburgh Postnatal Depression Scale (EPDS), with cut-offs of 1–12 indicating low risk and 13–30 indicating high risk. Data on birth outcomes were collected retrospectively from the medical records. Descriptive analyses, group comparisons, and linear regression analyses were conducted.
Results
Of the 262 participating mothers (total sample, i.e. mothers with and without depression), 19.0% had an episiotomy, 29.0% had tears, and 52.0% had an intact perineum after their childbirth. The total EPDS score was significantly higher among mothers with episiotomy (10.4, SD = 5.4) compared to those with tears (8.1, SD = 4.8) and those with intact perineum (9.4, SD = 4.9) (p-value <0.05). Lower levels of depression (−2.23 points on average) were significantly (p-value <0.05) associated with higher levels of perineum status (coded as 1 = episiotomy, 2 = other). Mothers who had a tear or episiotomy had on average 1.24 points higher EPDS scores compared to mothers with an intact perineum, although not significant (p-value >0.05).
Conclusions
Policymakers and clinicians are recommended to consider following up mothers with adverse birth outcomes to outline the risk of developing postpartum depression, at the same time as they routinely screen all mothers for risk of postpartum depression during their postpartum visits.
Introduction
Pregnancy and delivery are significant events in the lives of a woman and her family’s lives (Unicef, Citation2017). Yet, several psychological and life circumstances might induce unpleasant emotions in mothers (Acheampong et al., Citation2021). While the majority of pregnancies go smoothly, all pregnancies have the possibility of facing or ending in different types of complications (Majella et al., Citation2019). According to WHO (Unicef, Citation2017), about 15% of all pregnant women may experience a potentially life-threatening condition. Such experiences might lead to mental adverse outcomes such as depression during the postpartum period. Depression appears to be a common mental manifestation in women during this critical period, as previous research has found that 12.8% of mothers are at risk of depression throughout the second trimester and the postpartum period (Takehara et al., Citation2018).
Both biological, hormonal, and childbirth-related factors such as caesarean section (Xu et al., Citation2017), intrapartum complications (Wu et al., Citation2018), and mode of delivery (Meky et al., Citation2020) have been reported to associate with increased risk of postpartum depression (Guintivano et al., Citation2018). Another important but less studied risk factor for postpartum depression is childbirth-related adverse outcomes, including episiotomy. A recent study found that symptoms of unexplained depression, anxiety, and/or feelings of loneliness that occur in mothers during the postpartum period, called ‘baby blues’, were linked to mothers whose vaginal deliveries were not spontaneous and/or large episiotomies were performed (Kurashina & Suzuki, Citation2021). Furthermore, Kohler et al (Kohler et al., Citation2018). showed that having had an episiotomy during vaginal birth was also associated with reduced quality of life during the postpartum period. Thus, there is an urgent need to investigate the relationship between birth-related outcomes with a focus on perineal status and risk of postpartum depression.
Episiotomy is one of the most common surgical incisions performed by midwives when assisting in the second stage of childbirth with the main objective of enlarging the pelvic floor outlet and avoiding advanced (3rd and 4th-degree) perineal injuries (Verghese et al., Citation2016). However, systematic reviews demonstrated no solid evidence for performing episiotomy even for such ‘classical’ indications as prevention of shoulder dystocia or vacuum extraction birth (Sagi-Dain et al., Citation2020). Sagi-Dain et al (Sagi-Dain et al., Citation2020). quote the American College of Obstetricians and Gynaecologists (ACOG) ‘Based on the existing evidence, there are no specific situations in which episiotomy is essential’. According to a report on NHS-funded maternity services, the episiotomy rate has been observed in 3% of women giving birth at home in Scandinavian countries, 7% in Iceland, 27% in Germany, 19–50% in Spain, 20% in France, 25% in England, 22% in Estonia, 30% in the Netherlands, 53% in the Czech Republic, 27% in Switzerland, 68% in Romania, and 51% in Saudi Arabia (Gebuza et al., Citation2018). Furthermore, it has been reported that the common practice of episiotomy has been reported to be performed in 67% of all vaginal deliveries in the Middle East (Ghiasvand et al., Citation2021) and 93.3% in Turkey (Kartal et al., Citation2017). The relationship between episiotomy and risk of postpartum depression has not been studied exhaustively and therefore needs to be examined from different perspectives and in different contexts. Some of the existing evidence has focused on the effect of depression on adverse outcomes and not the opposite relation. For example, in 2021, Acheampong and colleagues (Acheampong et al., Citation2021) followed 360 Ghanaian pregnant women with depression till birth to examine the risk of unfavourable maternal and perinatal outcomes in pregnant women with moderate-severe depression against those with mild depression. They concluded that moderate-to-severe depression was strongly associated with episiotomy and tear (Acheampong et al., Citation2021). Furthermore, there is currently no established routine for screening the psychological state of mothers attending antenatal care in Oman.
Aim
The purpose of the study was to screen women for risk of postpartum depression and to determine maternal adverse birth outcomes (episiotomy and tear) associated with increased risk of postpartum depression in an Omani population of newly delivered mothers.
Materials and methods
Study design
To investigate maternal outcomes associated with increased risk of postpartum depression, a retrospective cohort study design was used. The researchers screened mothers for risk of postpartum depression (the outcome variable) during their postpartum visit (2–6 weeks after childbirth) and collected information about the childbirth outcomes (the exposure) with a special focus on the maternal outcomes (episiotomy, tear, instrumental delivery) from the medical records, after getting permission from the participating mother.
Setting
Data collection was conducted at two health centres in Wilayat Ibri, which is located in the Al Dhahirah governorate. The Wilayat of Ibri is one of the largest states with a large population located in the northeastern part of the Sultanate of Oman. The average number of registered pregnant women attending the selected health centres annually was 4725 women in 2020 (Local Authorities Statistical Office, oral communication).
Sample
Using an online sample size calculator (ClinCalc) and based on one study group, a continuous outcome variable, a mean EPDS score of 10 (SD = 5) from previous literature, power of 80% and alpha of 0.05 resulted in a sample size of 196 women.
The study targeted Omani women who gave birth during the three months before the data collection period (June to August 2021), were 18 years or older, were able to communicate in Arabic or English, and were not diagnosed with depression or any psychiatric disorder before their pregnancy. Furthermore, the mothers were expected to be living in Ibri Wilayat and attending one of the included health centres during the data collection period. Mothers with mental disorders were excluded from the study.
A non-probability sampling technique was used to classify participants. All available women fulfiling the inclusion criteria were invited to participate. The recruitment process and the self-administered data were initiated in the waiting room of the included health centres and completed during the same day of the postpartum visit. Mothers were screened for postpartum depression signs and symptoms in face-to-face interviews while information about childbirth outcomes was collected with a special focus on maternal outcomes (episiotomy, tear, instrumental delivery) from the medical records.
Study instrument
The screening tool used in this research was Edinburgh Postnatal Depression Scale [EPDS] (Cox et al., Citation1987; Wisner et al., Citation2002) which is widely used as the primary tool for assessing risk of depression across the perinatal period and has demonstrated reliability and validity in various countries (Palfreyman, Citation2021; Shrestha et al., Citation2016). Its utility lies in detecting symptoms of depression and anxiety, rather than serving as a definitive diagnostic tool for postpartum depression. When increased risk of depression is identified, individuals are typically referred to appropriate channels for a thorough evaluation and diagnosis. The instrument consists of ten items with responses graded from 3 to 0 reflecting (as much as always, not quite so much, definitely not so much, not at all) (Naja et al., Citation2021). Some of the items, namely 1, 2, and 4 are reversed (0–3). The total score ranges from 0 to 30. A rating of ≥ 13 is predictive of increased risk of postpartum depression. The instrument is available in the public domain and can be found at (EPDS).
We used the validated and psychometrically tested Arabic version of EPDS (Naja et al., Citation2021). The internal consistency of the EPDS was α = 0.865 and the convergent construct validity was demonstrated through a rotated component matrix of 0.75, which is acceptable and significant (p = 0.01) (Naja et al., Citation2021).
Variables
In addition to the outcome variable (EPDS total score, continuous normally distributed variable), background data was collected as:
Exposure: perineal status (intact, episiotomy, tear).
Predictors: the onset of labour (spontaneous, induction), intrapartum complications (yes, no), and initiation of breastfeeding (immediate, delayed).
Confounding factors: the age of the mother (continuous variable), pre-pregnancy BMI (continuous variable), current BMI (continuous variable), parity status (primipara, multipara), mode of childbirth (vaginal delivery, instrumental delivery, caesarean section), physical activity (yes, no).
Data collection procedure
Two assistants (registered nurses) assisted in data collection after receiving a one-day training at an individual level on the use of EPDS as well as data collection methods and procedures for conducting informed consent. All participants in the study received written information and an oral explanation of the study’s purpose before written informed consent was obtained. An isolated place was used during the screening procedure.
The questionnaire was administered when the mothers visited the clinics for the postpartum follow-up visit. The socioeconomic and medical characteristics of the women were first reported and followed by the EPDS questionnaire. All parts of the instrument were self-administered while adverse outcomes were extracted from medical records. The procedures for recruitment, monitoring, and execution of data collection were concurrently carried out over a six-month duration, spanning from June to November 2021.
Data analysis
For data entry, the survey items were coded, entered, cleansed, and re-categorised where needed. First, a descriptive analysis (including means, SD, frequencies, and percentages) was performed and followed by group comparisons (Chi-square and ANOVA with Bonferroni correction). In the group comparison, both the outcome variable (risk of postpartum depression, measured by EPDS) and the background variables were assessed across categories of the exposure variable, specifically perineal status (episiotomy, tear, and intact).
Multiple linear regression analysis (Stepwise method) was conducted to investigate the association between the dependent variable (total score of EPDS) and the independent variables (exposure, predictor, and confounding variables; either as continuous or dichotomous/dummy variables). The linear regression aimed also to clarify the level to which the included independent variables could explain the variation in the dependent variable. Both odds ratios (OR) and the 95% confidence interval (CI) for odds ratios were reported. Furthermore, the p-value <0.05 was the lowest limit of statistical significance in all analyses.
Ethical considerations
Ethical approval was obtained from the College of Nursing, the Medical Ethics Committee at Sultan Qaboos University (REF. NO. SQU-EC/029/2022 – MREC #2725), and the Ministry of Health of Oman (MH/DGHS/DG/22). After a detailed description of the study (both oral and written), the respondents who agreed to participate were asked to sign an informed consent. They also had their queries answered and were assured that they could withdraw from the study at any time without explanation. Participants were informed of the confidentiality and privacy of their study-related information.
A possible risk of this study could be that mothers who receive feedback on their risk of postpartum depression status based on the screening tool (EDPS) may develop an increased level of stress and anxiety. The researchers mitigated this risk through a follow-up call to all participating mothers to offer counselling and effective psychological support via the related health centres if needed. Upon the follow-up call, no mother communicated a need for consultation or psychological support.
Results
Of the total of 262 participating mothers, 49 (19.0%) had episiotomy, 77 (29.0%) had tears, and 136 (52.0%) had an intact perineum after their birth. The mean age of mothers with episiotomy was 26.2 years (SD = 3.7), which was significantly (p-value <0.001) lower than those with spontaneous tears (31.7, SD = 5.0) and those with intact perineum (32.2, SD = 5.4). While the current BMI did not differ significantly between the groups, the prepregnancy BMI was significantly (p-value = 0.028) lower in mothers with episiotomy (24.1, SD = 5.4) compared to those with tears (25.9, SD = 5.4) and those with intact perineum (27.0, SD = 7.9). Furthermore, the total postpartum depression score, according to the EPDS scale, was significantly (p-value = 0.044) higher among mothers with episiotomy (10.4, SD = 5.4) compared to those with tears (8.1, SD = 4.8) and those with intact perineum (9.4, SD = 4.9) ().
Table 1. Characteristics of mothers about perineum status.
Significant differences in parity status were also found. Of all mothers who gave birth for the first time (primiparous, n = 68), the vast majority (n = 42, 61.8%) had an episiotomy performed, 8 (11.8%) had tears, and 18 (26.5%) had intact perineum. Contrary to that, among mothers with intrapartum complications (n = 61), the majority had intact perineum (n = 43, 70.5%), while those with no complications (n = 201) had an episiotomy (n = 38, 18.9%), tears (n = 70, 34.8%), and intact perineum (n = 93, 46.3%) with significant differences (p-value <0.001) ().
Expectedly, mothers who had a caesarean section (n = 33) had all intact perineum (100%). However, the majority of mothers with vaginal childbirth had either episiotomy or tears (n = 44, 19.6% and n = 77, 34.4% respectively). Furthermore, 27 (14.8%) of the mothers who came with spontaneous onset of labour had an episiotomy while 59 (32.4%) had a tear. Lastly, 49 (21.4%) of mothers with immediate initiation of breastfeeding had an episiotomy, and 76 (33.2%) had a tear. See for more details.
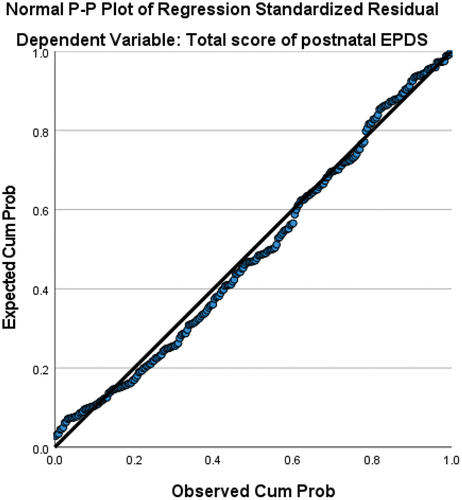
The multiple linear regression analysis was conducted after testing for the assumptions. The collinearity statistics showed no (VIF)-values above 10 which were considered as the absence of multicollinearity. The normality assumption was tested using a residual probability plot that showed a roughly normal distribution (). Similarly, homoskedasticity, independence of residuals, and linear relationship between predictor variables and the response variable showed normal findings.
Figure 1. The first assumption of the linear relationship between the predictor variables (age, pre-pregnancy BMI, perineal status, parity, physical activity, onset of labour, mode of delivery, intrapartum complications, and initiation of breastfeeding) and the dependent variable (EPDS total score).
The regression analysis showed that no variables were significantly associated with the EPDS total score, except for perineal status where episiotomy was compared with other conditions (tear and intact perineum); namely, lower levels of depression (−2.23 points on average) were significantly (p-value = 0.015) associated with higher levels of perineum status (coded as 1 = episiotomy, 2 = other). On the other hand, mothers who had a tear or episiotomy had on average 1.24 points higher EPDS score compared to mothers with an intact perineum, although not significant (p-value = 0.082) ().
Table 2. Multiple linear regression of variables associated with postpartum depression in Omani mothers.
Discussion
This study aimed to screen women for risk of postpartum depression and to determine maternal adverse birth outcomes (episiotomy, tear, instrumental delivery) associated with increased risk of postpartum depression in newly delivered Omani mothers. The highest EPDS scores were found among mothers who had episiotomy. These mothers were characterised by being significantly younger than those with a tear or intact perineum, were mostly primipara, had fewer intrapartum complications, and their birth was more often induced than spontaneous.
In the present study, it was observed that women with an intact perineum manifested a significantly higher mean postpartum depression score compared to those with perineal tears (p-value = 0.044). However, divergent findings have been reported in other studies regarding the association between perineal tears and postpartum depression or depressed mood (Dunn et al., Citation2015; Wolf et al., Citation2021). One plausible explanation for our observation is that mothers with an intact perineum may possess other characteristics that contribute to an elevated risk of postpartum depression. Notably, maternal age, pre-pregnancy BMI, and intrapartum complications were marginally but significantly higher in the group of mothers with an intact perineum compared to those with tears. These factors and their documented associations with postpartum depression have been corroborated in other studies as well (Alshikh Ahmad et al., Citation2021; Bradshaw et al., Citation2022; Fraga & Theme-Filha, Citation2020), thereby supporting and validating our study’s findings. Furthermore, our results showed that episiotomy is significantly contributing to higher scores of EPDS compared with mothers with an intact perineum, i.e. they had an increased risk of developing postpartum depression. Episiotomy is a common practice used as a preventive measure to decrease the occurrence of perineal trauma, among other reasons (Verghese et al., Citation2016). However, there is evidence of numerous other practices to protect the perineum from spontaneous tears. For example, perineal support during vaginal delivery was shown to reduce the risk of major obstetric anal sphincter injuries (Naidu et al., Citation2017). Another practice that could replace the practice of performing an episiotomy is the presence of two midwives during the second stage of labour, which could reduce severe perineal trauma in women who give birth for the first time (Porcar et al., Citation2021). Additionally, there is strong evidence to support the slow speed at the time of birth to prevent severe perineal tears (Maimburg & De Vries, Citation2019). Furthermore, paying special attention to and managing the pre-pregnancy and during-pregnancy risk factors (e.g. high BMI), may help reduce the risk of perineal trauma during delivery (Ye et al., Citation2022) and thus affect adverse psychological effects such as increased risk of postpartum depression. The current study findings may provide a basis for policymakers to apply new rules and recommendations to improve the care of mothers during pregnancy by implementing screening tools for mental health status and regulating episiotomy practices in childbirth units. In addition, the responsibility of the health care providers is to act as facilitators. They help individuals recognise their problems and develop the resources and abilities they need to implement necessary improvements. The self-empowerment of perinatal mothers is crucial. Therefore, the results of the current study may shed light on the need for educating newly delivered mothers who had experienced an episiotomy to be aware of the increased risk of postpartum depression.
Since mothers with episiotomy showed significantly higher levels of EPDS scores in the current study, we checked the characteristics of the mothers with episiotomy. Similarly to our findings, both younger age (Bączek et al., Citation2022; Mousavi et al., Citation2020; Urmee & Vwalika, Citation2022; Woretaw et al., Citation2021) and parity status (primiparous) (Mousavi et al., Citation2020; Urmee & Vwalika, Citation2022) were found to be associated with increased risks of having an episiotomy performed. Episiotomy was also reported in 66.0% of Omani primiparous mothers (Al-Ghammari et al., Citation2016), 50.5% in Lebanese primipara mothers (Kaddoura et al., Citation2019), and 90% of all episiotomies in a study conducted in Iran were primiparas (Mousavi et al., Citation2020). The prevalence of episiotomy in the current study (19.0%) is notably lower compared to rates reported in other countries. It is important to note that the 19.0% represents the overall prevalence among all participants. However, when specifically considering primiparous mothers in our study, the prevalence (61.8%) was lower than the figures documented in Al-Ghammari et al. (Citation2016) and higher than those reported in Kaddoura et al. (Citation2019). It should be noted, however, that the prevalence of episiotomy is comparably low in certain populations such as Swedish mothers, between 1.5 and 13.4% (Petersson et al., Citation2022). Taking into account the outcome of risk of postpartum depression and its association with episiotomy, it is highly recommended that healthcare professionals follow the WHO recommendation of a maximum of 10% performed episiotomies (Organization, Citation2018) to reduce the morbidity associated with the procedure.
Furthermore, in the current study, mothers with high scores of EDPS were those who had an episiotomy and were characterised by having fewer intrapartum complications, and their childbirth was more often induced than spontaneous. In line with our findings, recent studies have shown a positive relationship between oxytocin (used as an induction method to stimulate labour) use and episiotomy (Bączek et al., Citation2022). However, it is more difficult to explain the episiotomy procedure in mothers with no intrapartum complications, as no evidence could be found. Nevertheless, taking all the characteristics of these mothers into account, one can argue that the age of the mother (younger than those with tears or intact perineum) and the parity status (being primipara) could explain the conduction of the episiotomy procedure (Mousavi et al., Citation2020; Urmee & Vwalika, Citation2022) even though no complications were observed. According to several studies, at least 90% of women in certain Asian countries such as India who have their first child endure this unpleasant procedure (Kropp et al., Citation2005). These statistics were claimed to be even higher in some sections of North America and Asia (100%) (Ho et al., Citation2010). Research has proposed that one of the most commonly assumed advantages of performing an episiotomy is the avoidance of advanced (3rd and 4th degree) perineal injuries (Verghese et al., Citation2016). However, a meta-analysis of 22 observational studies involving 651,934 births indicated that women with severe perineal tears were more likely to have had an episiotomy performed with an odds ratio (OR) of 3.82 [95% (CI) 1.96–7] (Pergialiotis et al., Citation2014). Similarly, a 2017 Cochrane Collaboration meta-analysis found that routine episiotomy usage is linked to a higher risk of advanced tears in women having an unassisted vaginal birth (Jiang et al., Citation2017). Therefore, episiotomy should be performed selectively rather than frequently (Gebuza et al., Citation2018) to minimise its correlated adverse effects, including risk of developing postpartum depression. Furthermore, since both mental and physical adverse outcomes are related to episiotomy and tear during childbirth, this study aimed to provide evidence to guide healthcare providers and policymakers in actively working to plan and implementing preventive strategies to reduce the number of episiotomies and tears associated with childbirth and therefore prevent future health hazards and consequences associated with this procedure. The study’s findings could also facilitate referring postpartum women with high scores of depressive symptoms to psychiatric care facilities for appropriate diagnosis and treatment.
Limitations
While this study contributes beneficial insights into a significant maternal health issue, its findings must be interpreted in light of certain limitations. A major constraint lies in the exclusive reliance on a single instrument, namely the EPDS, for assessing the outcome (risk of postpartum depression). Although researchers contend that the validity of any psychological assessment should be established through multiple methods (Meyer et al., Citation2001), the primary objective of the current study was not to diagnose the state of depression but rather to assess signs and symptoms of depression among the participating mothers. Nevertheless, employing a gold standard could have facilitated a comparison of the EPDS outcomes, a practice we recommend for any future follow-up studies.
An additional constraint may arise from the study’s design, wherein the variables were measured concurrently. Despite the childbirth-related outcomes occurring before scale assessment and the exclusion of women self-reporting no depression diagnosis before pregnancy, the design precludes establishing a causal relationship between the outcome and exposure variables (Mann, Citation2012). Instead, we propose causal hypotheses for subsequent validation in analytical studies or longitudinal inquiries, as detailed in both the discussion and conclusions sections. Moreover, this study investigated the variation of the EPDS value as a dependent variable contingent on various factors, rather than providing the accurate diagnosis of postpartum depression.
Conclusions
This study aimed to screen women for postpartum depression and determine the maternal adverse outcomes (episiotomy and tear) associated with increased risk of postpartum depression in an Omani population of newly delivered mothers. We found that almost half of the participants had either episiotomy or tears and that mothers with episiotomy had significantly higher scores of depression, most of whom were younger first-time mothers. Policymakers and clinicians should consider including regular screening to detect risk of postpartum depression and follow-up of mothers with adverse birth outcomes to outline the risk of developing postpartum depression. Future studies, on the other hand, might answer the research questions related to effective interventions to support first-time mothers and decrease the prevalence of episiotomy, especially in the absence of complications and/or clinical indications.
Ethics approval
Ethical approval was obtained from the College of Nursing, the Medical Ethics Committee at Sultan Qaboos University (REF. NO. SQU-EC/029/2022 – MREC #2725), and the Ministry of Health of Oman (MH/DGHS/DG/22).
Informed consent
All participants signed an informed consent form and the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki.
Authors’ contribution
All authors contributed to the study’s conception and design. Data collection and entry were led by NAA while the data analysis and interpretation were performed by AK and MAQ. AK and NAA prepared the first draft of the manuscript and MAQ read the manuscript critically and provided suggestions along the way. All authors read and approved the final manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets generated and/or analysed during the current study are available from the corresponding author (AK) on reasonable request.
Additional information
Funding
References
- Acheampong, K., Pan, X., Kaminga, A. C., Wen, S. W., & Liu, A. (2021). Risk of adverse maternal outcomes associated with prenatal exposure to moderate-severe depression compared with mild depression: A fellow-up study. Journal of Psychiatric Research, 136, 32–38. https://doi.org/10.1016/j.jpsychires.2021.01.036
- Al-Ghammari, K., Al-Riyami, Z., Al-Moqbali, M., Al-Marjabi, F., Al-Mahrouqi, B., Al-Khatri, A., & Al-Khasawneh, E. M. (2016). Predictors of routine episiotomy in primigravida women in Oman. Applied Nursing Research, 29, 131–135. https://doi.org/10.1016/j.apnr.2015.05.002
- Alshikh Ahmad, H., Alkhatib, A., & Luo, J. (2021). Prevalence and risk factors of postpartum depression in the Middle East: A systematic review and meta–analysis. BMC Pregnancy and Childbirth, 21(1), 1–12. https://doi.org/10.1186/s12884-021-04016-9
- Bączek, G., Rychlewicz, S., Sys, D., Rzońca, P., & Teliga-Czajkowska, J. (2022). Episiotomy for medical indications during vaginal birth—retrospective analysis of risk factors determining the performance of this procedure. Journal of Clinical Medicine, 11(15), 4334. https://doi.org/10.3390/jcm11154334
- Bradshaw, H., Riddle, J. N., Salimgaraev, R., Zhaunova, L., & Payne, J. L. (2022). Risk factors associated with postpartum depressive symptoms: A multinational study. Journal of Affective Disorders, 301, 345–351. https://doi.org/10.1016/j.jad.2021.12.121
- Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of postnatal depression: Development of the 10-item Edinburgh postnatal depression scale. British Journal of Psychiatry, 150(6), 782–786. https://doi.org/10.1192/bjp.150.6.782
- Dunn, A. B., Paul, S., Ware, L. Z., & Corwin, E. J. (2015). Perineal injury during childbirth increases risk of postpartum depressive symptoms and inflammatory markers. Journal of Midwifery & Women’s Health, 60(4), 428–436. https://doi.org/10.1111/jmwh.12294
- Fraga, A. C. S. A., & Theme-Filha, M. M. (2020). Pregestational overweight and obesity and symptoms of postpartum depression: Data from the birth in Brazil study. Journal of Affective Disorders, 277, 463–469. https://doi.org/10.1016/j.jad.2020.08.054
- Gebuza, G., Kaźmierczak, M., Gdaniec, A., Mieczkowska, E., Gierszewska, M., Dombrowska-Pali, A., Banaszkiewicz, M., & Maleńczyk, M. (2018). Episiotomy and perineal tear risk factors in a group of 4493 women. Health Care for Women International, 39(6), 663–683. https://doi.org/10.1080/07399332.2018.1464004
- Ghiasvand, M., Nahidi, F., Sedigh Mobarakabadi, S., Broumandnia, N., & Sharifnia, H. (2021). Prevalence and meta-analysis of episiotomy in the Middle East. The Iranian Journal of Obstetrics, Gynecology & Infertility, 24(4), 90–99.
- Guintivano, J., Sullivan, P., Stuebe, A., Penders, T., Thorp, J., Rubinow, D., & Meltzer-Brody, S. (2018). Adverse life events, psychiatric history, and biological predictors of postpartum depression in an ethnically diverse sample of postpartum women. Psychological Medicine, 48(7), 1190–1200. https://doi.org/10.1017/S0033291717002641
- Ho, J. J., Pattanittum, P., Japaraj, R. P., Turner, T., Swadpanich, U., Crowther, C. A., & Group, S. O. S. (2010). Influence of training in the use and generation of evidence on episiotomy practice and perineal trauma. International Journal of Gynecology & Obstetrics, 111(1), 13–18. https://doi.org/10.1016/j.ijgo.2010.04.035
- Jiang, H., Qian, X., Carroli, G., & Garner, P. (2017). Selective versus routine use of episiotomy for vaginal birth. Cochrane Database of Systematic Reviews, 2017(2). https://doi.org/10.1002/14651858.CD000081.pub3
- Kaddoura, R., DeJong, J., Zurayk, H., Kabakian, T., Abbyad, C., & Mirza, F. G. (2019). Episiotomy practice in the Middle East: A Lebanese teaching tertiary care centre experience. Women & Birth, 32(2), e223–e228. https://doi.org/10.1016/j.wombi.2018.07.005
- Kartal, B., Kızılırmak, A., Calpbinici, P., & Demir, G. (2017). Retrospective analysis of episiotomy prevalence. Journal of the Turkish German Gynecological Association, 18(4), 190. https://doi.org/10.4274/jtgga.2016.0238
- Kohler, S., Sidney Annerstedt, K., Diwan, V., Lindholm, L., Randive, B., Vora, K., & De Costa, A. (2018). Postpartum quality of life in Indian women after vaginal birth and cesarean section: A pilot study using the EQ-5D-5L descriptive system. BMC Pregnancy and Childbirth, 18(1), 1–13. https://doi.org/10.1186/s12884-018-2038-0
- Kropp, N., Hartwell, T., & Althabe, F. (2005). Episiotomy rates from eleven developing countries. International Journal of Gynecology & Obstetrics, 91(2), 157–159. https://doi.org/10.1016/j.ijgo.2005.07.013
- Kurashina, R., & Suzuki, S. (2021). Postpartum depression without antenatal depression in primiparous women. Journal of Clinical Medicine Research, 13(10–11), 517. https://doi.org/10.14740/jocmr4624
- Maimburg, R. D., & De Vries, R. (2019). Coaching a slow birth with the woman in an empowered position may be less harmful than routine hands-on practice to protect against severe tears in birth–A discussion paper. Sexual & Reproductive Healthcare, 20, 38–41. https://doi.org/10.1016/j.srhc.2019.02.007
- Majella, M. G., Sarveswaran, G., Krishnamoorthy, Y., Sivaranjini, K., Arikrishnan, K., & Kumar, S. G. (2019). A longitudinal study on high risk pregnancy and its outcome among antenatal women attending rural primary health centre in Puducherry, South India. Journal of Education and Health Promotion, 8, 1–6. https://doi.org/10.4103/jehp.jehp_144_18
- Mann, C. (2012). Observational research methods—cohort studies, cross sectional studies, and case–control studies. African Journal of Emergency Medicine, 2(1), 38–46. https://doi.org/10.1016/j.afjem.2011.12.004
- Meky, H. K., Shaaban, M. M., Ahmed, M. R., & Mohammed, T. Y. (2020). Prevalence of postpartum depression regarding mode of delivery: A cross-sectional study. The Journal of Maternal-Fetal & Neonatal Medicine, 33(19), 3300–3307. https://doi.org/10.1080/14767058.2019.1571572
- Meyer, G. J., Finn, S. E., Eyde, L. D., Kay, G. G., Moreland, K. L., Dies, R. R., Eisman, E. J., Kubiszyn, T. W., & Reed, G. M. (2001). Psychological testing and psychological assessment: A review of evidence and issues. American Psychologist, 56(2), 128. https://doi.org/10.1037/0003-066X.56.2.128
- Mousavi, S. H. S., Miri, M., & Farzaneh, F. (2020). Episiotomy and its complications. Zahedan Journal of Research in Medical Sciences, 23(2). https://doi.org/10.5812/zjrms.104127
- Naidu, M., Sultan, A. H., & Thakar, R. (2017). Reducing obstetric anal sphincter injuries using perineal support: Our preliminary experience. International Urogynecology Journal, 28(3), 381–389. https://doi.org/10.1007/s00192-016-3176-4
- Naja, S., Al Kubaisi, N., Singh, R., Abdalla, H., & Bougmiza, I. (2021). Screening for antenatal depression and its determinants among pregnant women in Qatar: Revisiting the biopsychosocial model. BMC Pregnancy and Childbirth, 21(1), 1–12. https://doi.org/10.1186/s12884-021-03793-7
- Organization, W. H. (2018). WHO recommendations on intrapartum care for a positive childbirth experience. World Health Organization.
- Palfreyman, A. (2021). Addressing psychosocial vulnerabilities through antenatal care—depression, suicidal ideation, and Behavior: A study among urban Sri Lankan women. Frontiers in Psychiatry, 12, 554808. https://doi.org/10.3389/fpsyt.2021.554808
- Pergialiotis, V., Vlachos, D., Protopapas, A., Pappa, K., & Vlachos, G. (2014). Risk factors for severe perineal lacerations during childbirth. International Journal of Gynecology & Obstetrics, 125(1), 6–14. https://doi.org/10.1016/j.ijgo.2013.09.034
- Petersson, K. S. Y., Conner, P., Sengpiel, V., Storck Lindholm, E., Kloow, M., Elvander, L., & Granfors, M. (2022). Graviditetsregistrets annual report 2021. Retrieved July 11, from chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.medscinet.com/GR/uploads/hemsida/dokumentarkiv/Graviditetsregistrets%20%C3%85rsrapport%202021_1.0.pdf
- Porcar, I., Garzon, S., Loreti, S., Bosco, M., Paola, R., Pomini, P., Raffaelli, R., Leopardi, F., Uccella, S., Franchi, M., & Zorzato, P. (2021). Risk factors for obstetric anal sphincter injuries during vaginal delivery: Can we reduce the burden? Clinical and Experimental Obstetrics & Gynecology, 48(6), 1267. https://doi.org/10.31083/j.ceog4806201
- Sagi-Dain, L., Kreinin-Bleicher, I., Bahous, R., Gur Arye, N., Shema, T., Eshel, A., Caspin, O., Gonen, R., & Sagi, S. (2020). Is it time to abandon episiotomy use? A randomized controlled trial (EPITRIAL). International Urogynecology Journal, 31(11), 2377–2385. https://doi.org/10.1007/s00192-020-04332-2
- Shrestha, S. D., Pradhan, R., Tran, T. D., Gualano, R. C., & Fisher, J. R. (2016). Reliability and validity of the Edinburgh Postnatal Depression Scale (EPDS) for detecting perinatal common mental disorders (PCMDs) among women in low-and lower-middle-income countries: A systematic review. BMC Pregnancy and Childbirth, 16(1), 1–19. https://doi.org/10.1186/s12884-016-0859-2
- Takehara, K., Tachibana, Y., Yoshida, K., Mori, R., Kakee, N., & Kubo, T. (2018). Prevalence trends of pre-and postnatal depression in Japanese women: A population-based longitudinal study. Journal of Affective Disorders, 225, 389–394. https://doi.org/10.1016/j.jad.2017.08.008
- Unicef. (2017). Managing complications in pregnancy and childbirth: A guide for midwives and doctors. WHO, UNFPA, and Unicef.
- Urmee, R. J., & Vwalika, B. (2022). The maternal factors and short term outcomes associated with episiotomy during vaginal delivery at women and Newborn Hospital, Lusaka, Zambia. Medical Journal of Zambia, 49(2), 163–169. https://doi.org/10.55320/mjz.49.2.10
- Verghese, T. S., Champaneria, R., Kapoor, D. S., & Latthe, P. M. (2016). Obstetric anal sphincter injuries after episiotomy: Systematic review and meta-analysis. International Urogynecology Journal, 27(10), 1459–1467. https://doi.org/10.1007/s00192-016-2956-1
- Wisner, K. L., Parry, B. L., & Piontek, C. M. (2002). Postpartum depression. New England Journal of Medicine, 347(3), 194–199. https://doi.org/10.1056/NEJMcp011542
- Wolf, A., Ruiz, C., & Anderson, T.-L. (2021). Perineal tearing: Home vs. Hospital.
- Woretaw, E., Teshome, M., & Alene, M. (2021). Episiotomy practice and associated factors among mothers who gave birth at public health facilities in Metema district, northwest Ethiopia. Reproductive Health, 18(1), 1–11. https://doi.org/10.1186/s12978-021-01194-9
- Wu, Y. M., McArthur, E., Dixon, S., Dirk, J., & Welk, B. (2018). Association between intrapartum epidural use and maternal postpartum depression presenting for medical care: A population-based, matched cohort study. International Journal of Obstetric Anesthesia, 35, 10–16. https://doi.org/10.1016/j.ijoa.2018.04.005
- Xu, H., Ding, Y., Ma, Y., Xin, X., & Zhang, D. (2017). Cesarean section and risk of postpartum depression: A meta-analysis. Journal of Psychosomatic Research, 97, 118–126. https://doi.org/10.1016/j.jpsychores.2017.04.016
- Ye, J., Chen, Y., Yang, H., Chen, Q., Huang, Y., Zhao, J., Tu, L., Liu, M., & Zhang, J. (2022). A nationwide cross-sectional survey of episiotomy practice in China. The Lancet Regional Health–Western Pacific, 19, 19. https://doi.org/10.1016/j.lanwpc.2021.100345