
Letter to the editor for the article “The vascular cooling effect in hepatic multipolar radiofrequency ablation leads to incomplete ablation ex vivo”.
We read with great interest the well-written and very informative article of Franz G. M. Poch and co-worker assessing the vascular cooling effect in hepatic multibipolar radiofrequency ablation (RFA) [Citation1] and concluded that multibipolar RFA is significantly impacted by heat-sink effect. As recalled by the authors, heat-sink effect is a major cause of local tumour progression and multibipolar RFA has been developed to overcome this problem by delivering higher energy than monopolar RFA.
In our recent study, we found that multibipolar RFA provides improved sustained tumour control compared with monopolar RFA for hepatocellular carcinoma near vessels >3 mm diameter [Citation2]. The local progression rates for multipolar vs. monopolar RFA were 12.5 and 40%, respectively. We wish to discuss several points on the RFA procedure that could explain the discordance between our clinical results vs. the ex vivo results of Poch et al.:
The choice of RF probe does not match with our clinical practise. Franz G. M. Poch and co-worker chose to use bipolar applicators with an active length of 20 mm (T-20) while in clinical practise for multibipolar RFA on liver, we do not recommend to use T-20 applicator; we strongly recommend to use at least T-30 applicator and T-40 at best because the active lengths are 30 and 40 mm, respectively. The larger active length leads to higher energy delivery because the power used for ablation is 1 W for 1 mm of active length, so using three T-40 will require a total power of 120 W.
The “endpoint” of ablation is different from the one we use in clinical practise [Citation3]. In this study, the authors stop the ablation after an energy input of 40 KJ while in clinical practise, the increase in impedance leading to shutdown between each electrode combination is the end-point of energy cycle deposition. Therefore, if after energy input of 40 KJ, the increase of impedance between each electrode is not reached, the ablation is incomplete and that leads to overestimate the heat-sink effect. Using the increase in impedance as endpoint should decrease the rate of incomplete ablation near the vessel because the electrode will work until complete tissue necrosis is achieved (i.e. increase of impedance) [Citation4]. However, time to reach this endpoint will be longer because of vessel proximity and heat-sink effect.
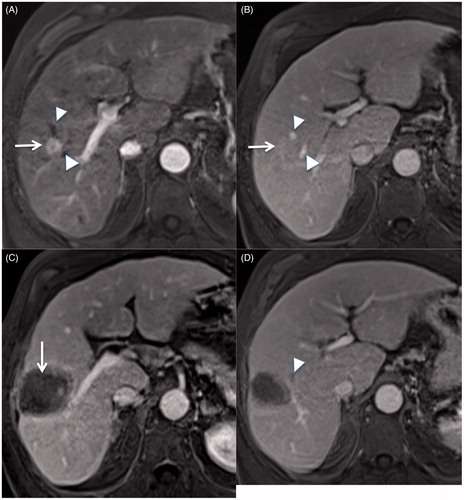
Applicator placing is very important. The most common presentation is a vessel >2–3 mm adjacent to the tumour (and not inside the tumour). In this case, in order to maximise the energy deposition near the vessel, one applicator should be placed parallel to the vessel and directly adjacent to it when possible. Furthermore, for sub-segmental vessels (hepatic artery, portal vein or hepatic vein), the aim of the RFA should be the occlusion of the vessel adjacent to the tumour () that leads to a significant decrease of local tumour progression by avoiding heat-sink effect [Citation5].
Figure 1. Contrast enhanced T1W at arterial (A) and portal (B) phase showing a hepatocellular carcinoma (white arrow) near two small hepatic veins (white arrowhead). An MRI performed one month after multibipolar radiofrequency ablation using 3 T-40 electrodes shows a large and homogeneous ablative volume (C, white arrow) with thrombosis of small hepatic vein adjacent to the tumour (D, white arrowhead).
Using temporary surgical blood flow, occlusion is not necessary because it is easy to perform a percutaneous puncture of the portal or hepatic vein under ultrasound guidance and to temporary occlude them using a balloon.
In conclusion, this ex vivo study showed that multibipolar is also impacted by heat-sink effect but we think that using optimal parameter for multibipolar RFA should drastically reduce the incomplete ablation rate of tumour near vessels and so local tumour progression [Citation2,Citation6,Citation7].
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
References
- Poch FGM, Rieder C, Ballhausen H, et al. (2016). The vascular cooling effect in hepatic multipolar radiofrequency ablation leads to incomplete ablation ex vivo. Int J Hyperthermia. [Epub ahead of print]. doi: 10.1080/02656736.2016.1196395.
- Hocquelet A, Aubé C, Rode A, et al. (2016). Comparison of no touch multibipolar vs. monopolar radiofrequency ablation for small HCC. J Hepatol. [Epub ahead of print]. doi: 10.1016/j.jhep.2016.07.010.
- Seror O, N’Kontchou G, Nault J-C, et al. (2016). Hepatocellular carcinoma within Milan criteria: no-touch multibipolar radiofrequency ablation for treatment-long-term results. Radiology 280:611–21.
- Seror O, N’Kontchou G, Van Nhieu JT, et al. (2014). Histopathologic comparison of monopolar versus no-touch multipolar radiofrequency ablation to treat hepatocellular carcinoma within Milan criteria. J Vasc Interv Radiol JVIR 25:599–607.
- Chiang J, Cristescu M, Lee MH, et al. (2016). Effects of microwave ablation on arterial and venous vasculature after treatment of hepatocellular carcinoma. Radiology. [Epub ahead of print]. doi: 10.1148/radiol.2016152508.
- Hocquelet A, Balageas P, Laurent C, et al. (2015). Radiofrequency ablation versus surgical resection for hepatocellular carcinoma within the Milan criteria: a study of 281 western patients. Int J Hyperthermia 31:749–57.
- Cartier V, Boursier J, Lebigot J, et al. (2015). Radiofrequency ablation of hepatocellular carcinoma: mono or multipolar? J Gastroenterol Hepatol 31:654–60.