
Abstract
Objectives
To develop effective nomograms for predicting pneumothorax and delayed pneumothorax after microwave ablation (MWA) in lung malignancy (LM) patients.
Methods
LM patients treated with MWA were randomly allocated to a training or validation cohort at a ratio of 7:3. The predictors of pneumothorax identified by univariate and multivariate analyses in the training cohort were used to develop a predictive nomogram. The C-statistic was used to evaluate predictive accuracy in both cohorts. A second nomogram for predicting delayed pneumothorax was developed and validated using identical methods.
Results
A total of 552 patients (training cohort: n = 402; validation cohort: n = 150) were included; of these patients, 27.9% (154/552) developed pneumothorax, with immediate and delayed pneumothorax occurring in 18.8% (104/552) and 9.1% (50/552), respectively. The predictors selected for the nomogram of pneumothorax were emphysema (hazard ratio [HR], 6.543; p < .001), history of lung ablation (HR, 7.841; p= .025), number of pleural punctures (HR, 1.416; p < .050), ablation zone encompassing pleura (HR, 10.225; p < .001) and pulmonary fissure traversed by needle (HR, 10.776; p < .001). The C-statistics showed good predictive performance in the training and validation cohorts (0.792 and 0.832, respectively). Another nomogram for delayed pneumothorax was developed based on emphysema (HR, 2.952; p= .005), ablation zone encompassing pleura (HR, 4.915; p < .001) and pulmonary fissure traversed by needle (HR, 4.348; p = .015). The C-statistics showed good predictive performance in the training cohort, and it had efficacy for prediction in the validation cohort (0.719 and 0.689, respectively).
Conclusions
The nomograms could effectively predict the risk of pneumothorax and delayed pneumothorax after MWA.
Introduction
Lung malignancy (LM) is one of the most fatal cancer globally, and consists of primary lung cancer (PLC) and lung metastases; of these, PLC is the leading cause of cancer incidence and mortality worldwide [Citation1]. In terms of treatment, surgery is a curative therapy to improve survival and remains the first-line therapy. However, only 20–40% of LM patients are surgical candidates at the time of diagnosis [Citation2,Citation3]. In recent decades, thermal ablation has been reported as a primary therapeutic strategy or/and an adjuvant to other treatments for LM patients, or for the patients with limited pulmonary reserve who cannot tolerate the surgery, including those with single lung post pneumonectomy [Citation4–8]. Of these, radiofrequency ablation (RFA) was first applied in 2000, while microwave ablation (MWA) was first applied in 2002 [Citation9,Citation10]. Compared to RFA, MWA is theoretically superior as it has a higher intra-tumoral temperature, larger ablation scope, decreased ablation duration, and deeper penetration [Citation2].
Pneumothorax is a common complication that can occur during or after thermal ablation, and consists of immediate intraprocedural pneumothorax and delayed pneumothorax, which occurs after the MWA procedures. A systemic review reported that the incidence rate of pneumothorax after RFA ranged between 1.3% and 60% [Citation11]. Although MWA requires fewer ablation needles and has a lesser ablation duration, the occurrence of pneumothorax after MWA appears to be unchanged, with a reported incidence rate of 21.1–63% [Citation2,Citation12]. In addition, Yoshimatsu et al. [Citation13] reported an incidence rate of 10.3% for delayed pneumothorax after RFA. Some patients with delayed pneumothorax are asymptomatic, which may deteriorate over time and influence the resilience and recoil of the lung, leading to depressed ventilation and even respiratory failure. Previous studies have explored the predictors for pneumothorax after thermal ablation [Citation14–20], including emphysema, age, sex, number of ablated tumors, tumor location, tumor diameter, and traversal of pulmonary fissure. However, many studies have focused on RFA, rather than MWA, and have not separately evaluated immediate and delayed pneumothorax. Further, the combined effects of pneumothorax are complex, and verification of the importance of each predictor is difficult. A pragmatic and reliable predictive model based on objective measurements is necessary for predicting the occurrence of pneumothorax. Nomograms are statistical models specifically designed to maximize the predictive accuracy, which can provide predictive information based on a combination of variables that allow for an individualized prediction of outcomes [Citation21]. However, no such tool is yet available for predicting the occurrence of pneumothorax after MWA.
Therefore, a retrospective study was conducted to develop effective nomograms for predicting pneumothorax and delayed pneumothorax after MWA in LM patients.
Methods
Patient criteria
This single-center retrospective study included all consecutive LM patients who received thermal ablation in this institution. The institutional ethics review board approved this study. The study protocol was conducted in accordance with the Declaration of Helsinki. The informed consent was waived owing to the retrospective nature of this study. Confirmed or suspected LM patients treated with thermal ablation between September 2016 and July 2020 at this institution were screened for this study, and were randomly allocated to either the training cohort or the validation cohort at a ratio of 7:3. Randomization allocation was created using the Stata version 9.0 (StataCorp., College Station, TX) statistical software. The inclusion criteria for this study were as follows: (a) age older than 18 years; (b) confirmed or suspected LM treated with MWA; and (c) previous or current histopathological examinations confirming the diagnosis of the malignancy. The exclusion criteria were as follows: (a) LM treated with RFA; (b) without previous and current histopathological examinations; (c) benign lesions according to histopathological examinations; (d) other concomitant therapies, such as the radioactive seeds implantation, performed during the MWA procedure; (e) the presence of pneumothorax before MWA; and (f) incomplete data.
Definitions and pre-MWA management
The detection of pneumothorax was based on axial computed tomography (CT) scanning, with the CT classification according to the largest distance from the pleura to the retraction of lung surface [Citation22]. Pneumothorax was classified as mild if it presented with the retraction of lung surface less than 2 cm from the pleura, moderate if it presented with retraction of 2–4 cm, and severe if it presented with retraction of more than 4 cm. Delayed pneumothorax was defined as a pneumothorax that was not detected by CT scan obtained immediately after MWA but was found on follow-up CT reexamination, which is underwent at least 24 h after MWA. The diagnosis of emphysema was according to the Goddard Visual Score [Citation23], and was made by two radiologists with >5 years of experience in diagnostic radiology. The PLC tumor stage was identified via the clinical TNM staging system of the Union for International Cancer Control (8th edition) [Citation24]. The tumor stage was regarded as IV for lung metastases patients. All patients with LM underwent chest CT and/or contrasted-enhanced CT (GE Healthcare) before the MWA procedure to evaluate the location, quantity and size of tumors. PET/CT was performed on demand to evaluate the lymph node and distant metastases. All laboratory examinations were conducted 1–4 d before MWA. For patients with multiple MWA procedures but without pneumothorax, data from the first MWA treatment was collected. For patients with multiple MWA procedures and pneumothorax, data from the MWA with subsequent pneumothorax were collected.
MWA procedure and follow-up
The MWA indications and procedures followed the guidelines of the Cardiovascular and Interventional Radiology Society of Europe [Citation25]. An MTC-3C MWA system (Vison Medicine) or an ECO-100A1 MWA system (ECO Medical Instrument) were used, with a microwave emission frequency of 2450 ± 50 MHz and an adjustable continuous-wave output power of 20–80 W. A thermocouple was applied to monitor the temperature to prevent damage to adjacent organs. The MWA needles (Vison Medicine or ECO Medical Instrument) were 10–18 cm in effective length and 15–17 G in outside diameter according to the tumor location and distance to the pleura, with a 15 mm active tip. Pre-procedural CT was performed to inform the treatment plan to clarify the suitable position, puncture sites location, optimal puncture trajectory and number of MWA needles. Local anesthesia was the general option for most of the patients, while intravenous anesthesia was administrated to the patients who cannot tolerate the intraprocedural pain. Needles were introduced into the planned site, and MWA was performed as per the planned power and duration, with adjustments of suitable power and duration being conducted according to the intraprocedural location of MWA needles as needed. The procedure was terminated when the ablation zone presented a 5–10 mm rim of ground-glass opacification (GGO) beyond the lesion boundary, which was measured on the intraprocedural CT scan. Finally, a repeat chest CT scan was performed to evaluate the ablation zone and detect possible complications. For patients without a histopathological examination, a synchronous coaxial-cannula biopsy was performed if necessary. A 15 G coaxial introducer needle (Argon Medical Devices) was first advanced into the tumor, and then the stylet was replaced by a 16 G full-core biopsy needle (Argon Medical Devices) through the cannula. A 17 G MWA needle (Vison Medicine or ECO Medical Instrument) was introduced into the tumor through the cannula [Citation26]. Short-term follow-up with CT reexamination was conducted 1–5 d after MWA during hospitalization, while the long-term follow-up with CT reexamination was performed 3–4 weeks after MWA in an outpatient visit. The patients who presented with symptoms were received the CT reexamination on demand. Ablation zone encompassing pleura was determined when the rim of GGO encompassed pleura on the intraprocedural CT scan. Intercostal tube placement was performed for patients with moderate and severe pneumothorax and was terminated when the retraction of lung surface disappeared.
Statistical analysis
Categorical variables are described as frequencies and percentages, and continuous variables are described as the mean ± SDs. Statistical analyses were performed using SPSS version 25.0 for Windows (IBM, Somers, NY). The data of the two cohorts were compared by Student’s t-test for continuous variables and by Pearson’s chi-square test or Fisher’s exact test for categorical variables. The possible predictors for pneumothorax were analyzed by univariate logistic regression analyses in the training cohort, including 24 parameters on demographics, treatment history, ablation factors and radiological features. Variables with p< .05 in the univariate analyses were entered as candidate variables into the multivariate logistic regression analyses. Model discrimination was assessed using C-statistic. A p< .05 was considered to indicate statistical significance in the multivariate analyses.
The establishment of the nomograms was based on the results of multivariate analyses of the training cohort. The nomograms were constructed with the regression modeling strategies package in R version 3.0.2 (R Project for Statistical Computing; www.r-project.org). After establishing the predictive nomogram for pneumothorax, C-statistic and the receiver operating characteristic (ROC) curve were used to validate the accuracy and discriminative capacity of the nomogram both internally (training cohort) and externally (validation cohort). The C-statistic was calculated as the area under the ROC curve and used to evaluate the predictive ability of the risk model [Citation27]. The optimum cutoff value for clinical use was determined by maximizing the Youden index (sensitivity + specificity-1). Then, the predictors for delayed pneumothorax were selected, and another nomogram was developed and validated via identical methods. An artificial neural network (ANN) model was established using SPSS version 25.0 statistical software to compare the importance of variables for predicting pneumothorax. For the establishment of the ANN, two-thirds of the patients in training cohort were randomly selected to build the model, and the remaining one-third was used for cross validation. This cross validation helps to maintain the stability and practicality of the ANN model and to prevent overtraining, which might lead to good performance on a training set. In this study, a three-layer feedforward ANN was developed, including input nodes, a hidden layer and output nodes. The back propagation of error was used for learning. The ANN model learned to associate each input with the corresponding output by modifying the weight of the connections. A decrease in the minimum error between the ANN output and the desired output was reached as learning proceeds.
Results
Patient characteristics and management of pneumothorax
A total of 552 LM patients (402 in the training cohort and 150 in the validation cohort; ) with 614 MWA procedures (494 patients with one procedure, 54 patients with two procedures and four patients with three procedures) in the mean follow-up of 3.6 ± 2.8 months were enrolled in this study, comprising 338 males (61.2%) and 214 females (38.8%). Detailed demographic characteristics are presented in . A total of 154 patients (27.9%) developed pneumothorax after MWA. Of these, 104 patients (18.8%) had immediate pneumothorax and 50 (9.1%) had delayed pneumothorax, with a mean time to delayed pneumothorax of 4.2 ± 6.3 d. For the management of pneumothorax, 72/154 (46.8%) patients received intercostal tube placement (56 in training cohort and 16 in validation cohort) and 23/154 (14.9%) patients received manual evacuation (14 in training cohort and 9 in validation cohort). All patients recovered from the pneumothorax.
Figure 1. Patients selection flowchart. RFA: Radiofrequency ablation; MWA: microwave ablation.
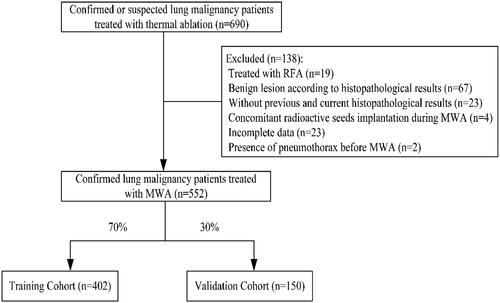
Table 1. Clinical characteristics of LM patients treated with MWA.
Predictors of pneumothorax and delayed pneumothorax in the training cohort
The results of univariate analyses and multivariate analyses for pneumothorax are presented in . The predictors were emphysema (hazard ratio [HR], 6.543; 95% confidence interval [CI], 3.726–11.489; p < .001), history of lung ablation (HR, 7.841; 95% CI, 1.292–47.599; p= .025), number of pleural punctures (HR, 1.416; 95% CI, 0.999–2.008; p < .050), ablation zone encompassing pleura (HR, 10.225; 95% CI, 3.736–27.984; p < .001) and pulmonary fissure traversed by needle (HR, 10.776; 95% CI, 3.078–37.721; p < .001). The results of univariate analyses and multivariate analyses for delayed pneumothorax are presented in . The predictors were emphysema (HR, 2.952; 95% CI, 1.393–6.255; p= .005), ablation zone encompassing pleura (HR, 4.915; 95% CI, 2.023–11.942; p < .001) and pulmonary fissure traversed by needle (HR, 4.348; 95% CI, 1.326–14.252; p= .015).
Table 2. Univariate analyses and multivariate logistic regression analyses for pneumothorax after MWA in the training cohort.
Table 3. Univariate analyses and multivariate logistic regression analyses for delayed pneumothorax after MWA in the training cohort.
Development and validation of the nomograms
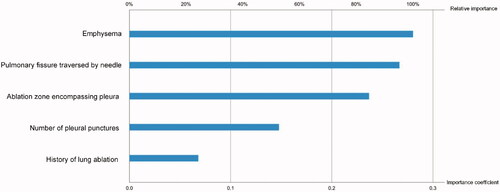
Two nomograms were developed based on the predictors, one to predict pneumothorax and one to predict delayed pneumothorax (). In the nomograms, each patient received a point total according to the characteristics before and/or during MWA to predict the occurrence of pneumothorax or delayed pneumothorax with risk percentages. According to the internal validation for pneumothorax in the training cohort, the C-statistic of this nomogram was 0.792 (95% CI, 0.738–0.847; ), and the external validation index in the validation cohort was 0.832 (95% CI, 0.750–0.914; ). Similarly, according to the internal validation for delayed pneumothorax, the C-statistic of this nomogram was 0.719 (95% CI, 0.619–0.818; ) and the external validation index was 0.689 (95% CI, 0.542–0.837; ). An ANN model was established based on the univariate analyses and multivariate analyses. The importance of each predictor for pneumothorax is shown in . According to the ANN model, emphysema was the predominant predictor of pneumothorax. According to the maximized Youden index, the optimal cutoff values for pneumothorax and delayed pneumothorax risk were 0.46 and 0.38, respectively.
Figure 2. (a) Nomogram for predicting pneumothorax after MWA. (b) Nomogram for predicting delayed pneumothorax after MWA. To use the nomogram, an individual patient’s value is located on each variable axis, and a line is drawn upward to determine the number of points received for each variable. The sum of these points is located on the Total Point axis, and a line is drawn downward to the risk axes to determine the likelihood of developing pneumothorax or delayed pneumothorax.
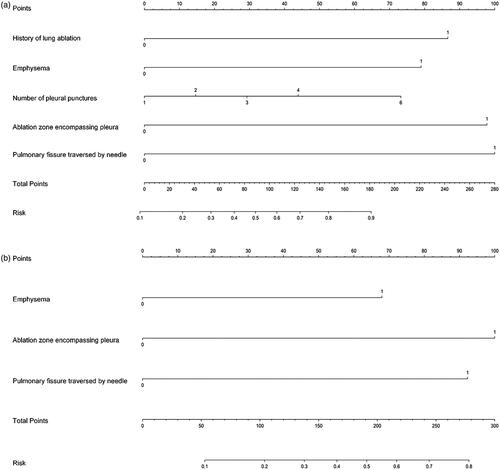
Figure 3. Receiver operating characteristic curve analyses for the nomograms in internal and external validation. The diagonal red line indicates that the index of AUC was 0.5, which was a reference value. Harrell’s C statistic was calculated as the area between the ROC curve (blue curve) and horizontal axis. (a) The area under the curve (C-statistic) was 0.792 (95% CI, 0.738–0.847) in the training cohort for predicting pneumothorax. (b) The area under the curve (C-statistic) was 0.832 (95% CI, 0.750–0.914) in the validation cohort for predicting pneumothorax. (c) The area under the curve (C-statistic) was 0.719 (95% CI, 0.619–0.818) in the training cohort for predicting delayed pneumothorax. (d) The area under the curve (C-statistic) was 0.689 (95% CI, 0.542–0.837) in the validation cohort for predicting delayed pneumothorax.
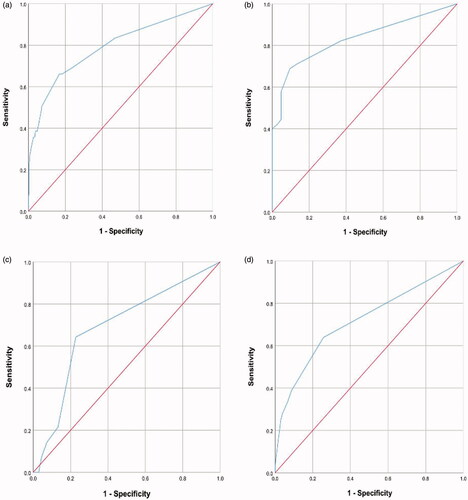
Figure 4. Schematic representation and the importance of each variable in the artificial neural network model. The relative importance was calculated with reference to the predictor that was of the highest importance to the target event. MWA: microwave ablation; TKI: tyrosine kinase inhibitor.
Discussion
Thermal ablation is an effective therapeutic strategy for LM patients, with 3- and 5-year survival rates of 36–88% and 25–61%, respectively, after RFA in non-small cell lung cancer patients [Citation28,Citation29]. Previous studies have identified that multiple predictors are significantly correlated with pneumothorax [Citation14–20]. Although the combined effects of pneumothorax are complex and nonlinear, it is possible to use factors related to MWA to predict the risk of pneumothorax. In addition, Yoshimatsu et al. [Citation13] defined delayed pneumothorax as pneumothorax that was not detected by the CT scan obtained immediately after RFA; however, was detected on follow-up chest radiographs, which were taken 3 h after RFA procedures. In this study, delayed pneumothorax had a similar definition and occurred at least 24 h after MWA, owing to the short-term follow-up with CT reexaminations that were performed at least 1 d after MWA procedure.
Emphysema is the permanent enlargement of airspaces distal to the terminal bronchiole with destruction of the alveolar walls [Citation30] and is a significant predictor for pneumothorax after thermal ablation [Citation14–19]. Emphysema is usually classified according to the predominant involved region of the acinus (proximal, distal or whole acinus). Yamagami et al. [Citation16] reported an incidence rate of 29.5% (38/129) for pneumothorax after RFA; 23.7% (9/38) of patients presented with pneumothorax and 6.6% (6/91) of non-pneumothorax patients were accompanied by emphysema. In 2011, Kashima et al. [Citation14] analyzed 1000 RFA sessions in 420 patients and reported an incidence rate of 44.5% for pneumothorax; emphysema was a significant risk factor for pneumothorax requiring pleural sclerosis. In this study, 77/119 (64.7%) patients with emphysema had pneumothorax after MWA, and 25/119 (21.0%) patients with emphysema had delayed pneumothorax. The multivariate analyses revealed that emphysema was significantly associated with both pneumothorax and delayed pneumothorax. A potential mechanism for this is that the anatomic distribution of emphysema affects the development of pneumothorax, which may occur more likely when emphysematous bullae are traversed by needles.
Previous studies have found that ablation zones, which include the pleural puncture site, are associated with pneumothorax [Citation31]. Therefore, an indirect approach that leaves at least 2 cm of normal aerated lung between the lesion and pleura is recommended [Citation32]. The presence of a minimum 5 mm rim of GGO around tumors is regarded as technical success for thermal ablation [Citation33]. Yoshimatsu et al. [Citation13] found that the presence of a GGO, which emerged around ablation zones that encompass the pleura, was significantly associated with delayed or recurrent pneumothorax. In addition, Clasen et al. [Citation34] hypothesized that the coagulation of the pleura and adjacent lung parenchyma may induce dehydration and reduce the elastic properties of the lung parenchyma. However, another study claimed that a higher pleural temperature was correlated with pleural effusion rather than with pneumothorax [Citation35]. In an animal study evaluating the pleural puncture site in relation to the risk of pneumothorax, 13 cases of pneumothorax occurred among 62 lung MWA sessions; if the pleural puncture site was not within the ablation zone, the risk of pneumothorax was decreased [Citation31]. In general, the energy applied in the MWA procedure usually ranges between 20 and 80 W in LM patients. Vogl et al.[Citation36] compared the high-frequency MWA and conventional low-frequency MWA, and found no significant difference in the occurrence of pneumothorax. In this study, the mean minimum distance to the pleura was 0.9 ± 1.1 cm, and 41 patients had an ablation zone that encompassed the pleura; according to the multivariable analyses, this was significantly associated with pneumothorax and delayed pneumothorax. A potential mechanism for this association is that the heated pleura may lose resilience and recoil or wrap the pleural ablation zone. In addition, the delivery power was up to 80 W in this study, which was not associated with the occurrence of pneumothorax.
This study included 42 (7.6%) patients with lesions adjacent to or invading the pulmonary fissure; in 30 (5.4%) patients, the pulmonary fissure was traversed by the MWA needles. Nour-Eldin et al. [Citation18] reported that the pulmonary fissure traversed by needle was correlated with the occurrence of pneumothorax. Additionally, the traversal of pulmonary fissure could increase the number of pleural punctures, which was also a predictor of pneumothorax in accordance with previous findings [Citation15]. In the MWA procedure, the needles created a large pleural hole than the biopsy needles; these pleural holes can be further enlarged by respiratory-induced lung motion. An increased incidence of pulmonary fissure traversed by needle and increased number of pleural punctures can lead to an increased number of pleural holes and their enlargement; thereby, increasing the risk of pneumothorax. Wang et al. [Citation26] attempted synchronous coaxial-cannula biopsy and MWA to reduce the number of pleural punctures and found that the risk of pneumothorax was significantly reduced compared to patients who underwent sequential procedures. Similarly, 175 patients received synchronous coaxial-cannula biopsy and MWA in this study, and this coaxial-cannula procedure revealed the consistent results toward pneumothorax when compared to the sequential procedures.
Two nomograms were established to predict pneumothorax and delayed pneumothorax after MWA. We used the data from the training cohort as an internal validation and the data from the validation cohort as an external validation to evaluate the accuracy of the nomograms. The C-statistic values indicate the high accuracy of the nomograms. According to the maximized Youden index, the cutoff values for pneumothorax and delayed pneumothorax risks were 0.46 and 0.38, respectively, which signify sufficient predictive accuracy. The nomograms can be applied to identify LM patients who may develop pneumothorax or delayed pneumothorax after MWA, and they may be helpful for stratifying the risk of pneumothorax or delayed pneumothorax and decision-making regarding further surveillance and/or interventions. Patients at high risk (>0.38) should be monitored for delayed pneumothorax by timely radiological reexaminations, especially at a mean time of 4.2 d after MWA. In addition, the relative importance of predictors associated with pneumothorax remains controversial [Citation14–18]. As a computer technology that structurally and functionally models biological neural systems, ANN has been found to outperform conventional discrimination analyses. Additionally, ANN can learn from observing datasets and complicated nonlinear relationships between input and output parameters and can determine the importance of each variable for target events [Citation37,Citation38]. Here, the ANN model revealed emphysema to be the most significant predictor of pneumothorax after MWA.
This study has several limitations that should be noted. First, this was a retrospective study; thus, patient selection bias may exist. Second, although a validation cohort was established and showed a high accuracy for predictive performance, external validation from other datasets is warranted. Third, the study did not explore the needle angulation owing to the multiple adjustments required during the MWA procedure, and needle angulation may be potentially correlated with pneumothorax. Finally, a longer follow-up duration should be included to evaluate rare recurrent pneumothorax after MWA in future studies.
In conclusion, the nomograms can effectively predict the risk of pneumothorax and delayed pneumothorax after MWA, and emphysema is the predominant predictor for pneumothorax after MWA. Patients at high risk (>0.38) should be monitored for delayed pneumothorax by timely radiological reexaminations. However, further prospective randomized controlled trials are warranted to validate these findings.
Acknowledgments
The authors thank Xin Huang, MS, for his assistance in protocol review and statistical analyses.
Disclosure statement
The authors declare that they have no conflict of interest.
Additional information
Funding
References
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
- Liu H, Steinke K. High-powered percutaneous microwave ablation of stage I medically inoperable non-small cell lung cancer: a preliminary study. J Med Imaging Radiat Oncol. 2013;57(4):466–474.
- Mazzone P. Preoperative evaluation of the lung resection candidate. Cleve Clin J Med. 2012;79(5):S17–S22.
- Postmus PE, Kerr KM, Oudkerk M, et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(4):v1–21.
- Donington J, Ferguson M, Mazzone P, et al. American College of Chest Physicians and Society of Thoracic Surgeons consensus statement for evaluation and management for high-risk patients with stage I non-small cell lung cancer. Chest. 2012;142(6):1620–1635.
- Kurilova I, Gonzalez-Aguirre A, Beets-Tan RG, et al. Microwave ablation in the management of colorectal cancer pulmonary metastases. Cardiovasc Intervent Radiol. 2018;41(10):1530–1544.
- Sofocleous CT, May B, Petre EN, et al. Pulmonary thermal ablation in patients with prior pneumonectomy. AJR Am J Roentgenol. 2011;196(5):W606–12.
- Hess A, Palussiere J, Goyers JF, et al. Pulmonary radiofrequency ablation in patients with a single lung: feasibility, efficacy, and tolerance. Radiology. 2011;258(2):635–642.
- Dupuy DE, Zagoria RJ, Akerley W, et al. Percutaneous radiofrequency ablation of malignancies in the lung. AJR Am J Roentgenol. 2000;174(1):57–59.
- Feng W, Liu W, Li C, et al. Percutaneous microwave coagulation therapy for lung cancer. Zhonghua Zhong Liu Za Zhi. 2002;24(4):388–390.
- Zhu JC, Yan TD, Morris DL. A systematic review of radiofrequency ablation for lung tumors. Ann Surg Oncol. 2008;15(6):1765–1774.
- Cheng G, Shi L, Qiang W, et al. The safety and efficacy of microwave ablation for the treatment of CRC pulmonary metastases. Int J Hyperthermia. 2018;34(4):486–491.
- Yoshimatsu R, Yamagami T, Terayama K, et al. Delayed and recurrent pneumothorax after radiofrequency ablation of lung tumors. Chest. 2009;135(4):1002–1009.
- Kashima M, Yamakado K, Takaki H, et al. Complications after 1000 lung radiofrequency ablation sessions in 420 patients: a single center's experiences. AJR Am J Roentgenol. 2011;197(4):W576–80.
- Hiraki T, Tajiri N, Mimura H, et al. Pneumothorax, pleural effusion, and chest tube placement after radiofrequency ablation of lung tumors: incidence and risk factors. Radiology. 2006;241(1):275–283.
- Yamagami T, Kato T, Hirota T, et al. Pneumothorax as a complication of percutaneous radiofrequency ablation for lung neoplasms. J Vasc Interv Radiol. 2006;17(10):1625–1629.
- Okuma T, Matsuoka T, Yamamoto A, et al. Frequency and risk factors of various complications after computed tomography-guided radiofrequency ablation of lung tumors. Cardiovasc Intervent Radiol. 2008;31(1):122–130.
- Nour-Eldin NE, Naguib NN, Saeed AS, et al. Risk factors involved in the development of pneumothorax during radiofrequency ablation of lung neoplasms. AJR Am J Roentgenol. 2009;193(1):W43–W48.
- Zheng A, Wang X, Yang X, et al. Major complications after lung microwave ablation: a single-center experience on 204 sessions. Ann Thorac Surg. 2014;98(1):243–248.
- Kim MS, Hong HP, Ham SY, et al. Complications after 100 sessions of cone-beam computed tomography-guided lung radiofrequency ablation: a single-center, retrospective experience. Int J Hyperthermia. 2020;37(1):763–771.
- Bochner BH, Kattan MW, Vora KC. Postoperative nomogram predicting risk of recurrence after radical cystectomy for bladder cancer. J Clin Oncol. 2006;24(24):3967–3972.
- Nour-Eldin NE, Naguib NN, Tawfik AM, et al. Outcomes of an algorithmic approach to management of pneumothorax complicating thermal ablation of pulmonary neoplasms. J Vasc Interv Radiol. 2011;22(9):1279–1286.
- Goddard PR, Nicholson EM, Laszlo G, et al. Computed tomography in pulmonary emphysema. Clin Radiol. 1982;33(4):379–387.
- Lim W, Ridge CA, Nicholson AG, et al. The 8th lung cancer TNM classification and clinical staging system: review of the changes and clinical implications. Quant Imaging Med Surg. 2018;8(7):709–718.
- Venturini M, Cariati M, Marra P, et al. CIRSE standards of practice on thermal ablation of primary and secondary lung tumours. Cardiovasc Intervent Radiol. 2020;43(5):667–683.
- Wang D, Li B, Bie Z, et al. Synchronous core-needle biopsy and microwave ablation for highly suspicious malignant pulmonary nodule via a coaxial cannula. J Cancer Res Ther. 2019;15(7):1484–1489.
- Xu S, Guan LJ, Shi BQ, et al. Recurrent hemoptysis after bronchial artery embolization: prediction using a nomogram and artificial neural network model. AJR Am J Roentgenol. 2020;215:1490–1498.
- Hiraki T, Gobara H, Iguchi T, et al. Radiofrequency ablation for early-stage nonsmall cell lung cancer. Biomed Res Int. 2014;2014:152087.
- Palussiere J, Lagarde P, Aupérin A, et al. Percutaneous lung thermal ablation of non-surgical clinical N0 non-small cell lung cancer: results of eight years’ experience in 87 patients from two centers. Cardiovasc Intervent Radiol. 2015;38(1):160–166.
- The Definition of Emphysema. Report of a national heart, lung, and blood institute, division of lung diseases workshop. Am Rev Respir Dis. 1985;132(1):182–185.
- Lee KS, Takaki H, Yarmohammadi H, et al. Pleural puncture that excludes the ablation zone decreases the risk of pneumothorax after percutaneous microwave ablation in porcine lung. J Vasc Interv Radiol. 2015;26(7):1052–1058.
- Hinshaw JL, Lubner MG, Ziemlewicz TJ, et al. Percutaneous tumor ablation tools: microwave, radiofrequency, or cryoablation-what should you use and why? Radiographics. 2014;34(5):1344–1362.
- Anderson EM, Lees WR, Gillams AR. Early indicators of treatment success after percutaneous radiofrequency of pulmonary tumors. Cardiovasc Intervent Radiol. 2009;32(3):478–483.
- Clasen S, Kettenbach J, Kosan B, et al. Delayed development of pneumothorax after pulmonary radiofrequency ablation. Cardiovasc Intervent Radiol. 2009;32(3):484–490.
- Tajiri N, Hiraki T, Mimura H, et al. Measurement of pleural temperature during radiofrequency ablation of lung tumors to investigate its relationship to occurrence of pneumothorax or pleural effusion. Cardiovasc Intervent Radiol. 2008;31(3):581–586.
- Vogl TJ, Basten LM, Nour-Eldin NA, et al. Microwave ablation (MWA) of pulmonary neoplasms: clinical performance of high-frequency MWA with spatial energy control versus conventional low-frequency MWA. AJR Am J Roentgenol. 2019;213(6):1388–1396.
- Cross SS, Harrison RF, Kennedy RL. Introduction to neural networks. Lancet. 1995;346(8982):1075–1079.
- Baxt WG. Application of artificial neural networks to clinical medicine. Lancet. 1995;346(8983):1135–1138.