
Abstract
Objective: This study is an open clinical trial. The aim of this study was to show the changes that occur in the viscoelastic properties of the plantar fascia (twenty healthy volunteers) measured by SEL and the changes in the plantar fascia temperature measured by thermography after the application of a 448 kHz capacitive resistive monopolar radiofrequency (CRMR) in active healthy subjects immediately after treatment and at the 1-week follow-up.
Methods: Furthermore, to analyze if an intervention with 448 kHz CRMR in the plantar fascia of the dominant lower limb produces a thermal response in the plantar fascia of the non-dominant lower limb. The final objective was to analyze the level of association between the viscoelastic properties of the PF and the temperature before and after the intervention with 448 kHz CRMR.
Results: Our results showed that a temperature change, which was measured by thermography, occurred in the plantar fascia after a single intervention (T0-T1) and at the 1-week follow up (T1-T2).
Conclusion: However, no changes were found in the viscoelastic properties of the plantar fascia after the intervention or at the 1-week follow up. This is the first study to investigate changes in both plantar fascia viscoelastic properties and in plantar fascia temperature after a radiofrequency intervention.
Introduction
Radiofrequency treatment is a therapeutic approach used in the treatment of most musculoskeletal and sports injuries. The use of a 448 kHz current flowing through the body due to the voltage difference created between two diversely placed electrodes is one of the most studied radiofrequency treatments. The current is commonly referred to as capacitive resistive monopolar radiofrequency (CRMR). The stimulating electrical voltage is created by an active circular electrode that can be repositioned during the treatment while the return electrode, which is of a rectangular design, stays in the same place for the duration of the treatment [Citation1–5].
In the clinical setting, 448 kHz has been associated with pain reduction and improved functionality in patients with musculoskeletal disorders. Its application is often used as a way to relieve pain and inflammation and potentially enhance tissue healing [Citation1,Citation6,Citation7]. In addition, hyperthermia can also change the nature of connective tissues and alter the properties of tendons, ligaments, and muscles, which results in an increase in their extensibility and reduces their tone and spasm [Citation8]. The extent of physiological effects may vary depending on the level of exposure. Furthermore, hyperthermia CRMR can lead to a considerable increase in cell metabolism and accelerated recovery. These hyperthermal adaptations to radiofrequency treatment are based on vasodilatation, which causes a targeted local increase in blood perfusion and a decrease in muscle tension and spasm, an increase in oxygen and nutrient supply, and an acceleration of healing [Citation6].
The term ‘radiofrequency’ makes reference to electromagnetic signals whose frequencies range from 30 KHz to 1 GHz in the electromagnetic spectrum [Citation9]. Wavelengths of 300 kHz to 1 MHz are commonly used among physiotherapists for pain management and to reduce the recovery time of musculoskeletal disorders [Citation10]. As redard technical aspects, two types of energy transmission devices exist: capacitive–resistive, and dielectric [Citation10]. Nowadays, there are three types of application modalities: (i) monopolar modalities: a single pole acts as an aerial which means that a receptor is not needed to emit the signal since the receptor pole will be the tissue on which the signal is applied; (ii) bipolar modalities: there is an emitting pole and a receptor pole and (iii) multipolar modalities: a type of bipolar modality where one of the poles has more than one output (three outputs in the case of tripolar, five in case of pentapolar…). As a consequence, the contact surface between both poles may be further reduced while at the same time producing an increase in the energy density [Citation9,Citation10]. There are different diathermy devices. One form is shortwave diathermy (SWD), which at short wave frequency (27.12 MHz) produces both, an electrical and magnetic field in tissues. SWD may be delivered through either the inductive technique that the greatest amount of heating occurs on deep tissues, or through the capacitive technique where the greatest amount of heating occurs on superficial tissues [Citation11,Citation12]. In addition, microwave diathermies (MWDs) (2456/915 MHz) are electromagnetic (EM) radiation emitting systems that are used by for thermotherapy treatment in different tissues. Hyperthermia induced by microwave diathermy raises the temperature of deep tissues from 41 degrees C to 45 degrees C using electromagnetic power [Citation12,Citation13]. Currently, most clinicians use another form of diathermy namely continuous diathermy. The ReBound (ReGear Life Sciences, Inc, Pittsburgh PA) is a continuous diathermy device, which uses an induction helical-coil sleeve to deeply heat the muscle at 35 W and 13.56 MHz [Citation14]. However, Indiba, a 488 kHz radiofrequency device was used in this study due to the number of clinical trials reporting its use.
Real-time sonoelastography (SEL) is a recently developed, noninvasive ultrasound (US) technique that allows for the in vivo assessment of the mechanical properties of tissues and assesses tissue stiffness [Citation15,Citation16]. The principle underlying elastography is that tissue compression produces a strain (displacement) within the tissue, which provides a color-coded image superimposed over the B-mode image. The color scale indicates the relative elasticity of tissues within the region of interest. Two SEL methods are commonly used in musculoskeletal clinical practice and research: shear wave elastography (SWE), in which compressive acoustic waves dynamically provide local stress in the soft tissues [Citation17] (ROI)[Citation18], and strain elastography, in which a mechanical force compresses the tissues axially [Citation17,Citation18]. Despite, strain elastography, was used in this study. The validity of SEL use in the plantar fascia (PF), as well as its ability to detect changes in the elastic properties of fascia, has been studied [Citation16,Citation19], thus allowing plantar fascia disorders or plantar fasciitis to be detected. Nevertheless, there are no conclusive studies in this regard. In addition, according to published studies on plantar fasciitis, SWE seems to be able to identify degenerative changes involving the PF, which include collagen breakdown and disorientation, matrix degradation, increased mucoid content, and angio-fibroblastic hyperplasia; the result is a softer appearance of the PF in SWE [Citation17,Citation20]. The use of ultrasound elastography to assess how CRMR affects tendon elasticity has been evaluated in different structures but not in the plantar fascia. Currently, studies have shown elastic changes in different structures after a 448 kHz CRMR intervention, however knowledge about how this affects other structures in general, such as loading tendons and particularly the plantar fascia, are needed. In this regard, a CRMR intervention appears to show great potential in modulating the elastic properties of soft tissue. Hence, increased knowledge about the physiological responses that are produced in healthy subjects will help develop how injury conditions are understood and may serve as a potential improvement marker after receiving treatment.
The infrared thermography measurement of human skin temperature (TSK) in healthy and unhealthy populations is growing in importance and has been highlighted by the increase in the number of publications using this technique [Citation21–24]. Medical infrared thermography (MIT) provides a noninvasive and non-radiating analysis tool for analyzing physiological functions related to skin-temperature control. This rapidly developing technology is used to detect and locate thermal abnormalities characterized by an increase or decrease found at the skin surface. The technique involves the detection of infrared radiation that can be directly correlated with the temperature distribution of a defined body region [Citation24]. This technology, through the capture of higher resolution photographs [Citation21,Citation25], allows skin temperature data to be obtained from different regions of interest (ROI). After exercise, such information can be very helpful in quantifying the physiological responses which indicates the training load and recovery of the athlete [Citation21]. Nowadays, there are not many studies which deal with thermography and plantar fascia [Citation24,Citation26]. In this regard, the objective was to determine if patients with plantar fasciitis showed a specific temperature on the sole of the foot that could be detected by infrared thermography [Citation26].
Our hypothesis is that this application of a 448 kHz CRMR can produce changes in the elastic properties and temperature of the plantar fascia, which can be measured by SEL and thermography, and could produce a thermal response in both the plantar fascia of the dominant lower limb and in the non-dominant lower limb. This will help in the understanding of which response is expected to occur under physiological and healthy circumstances after the use of a CRMR intervention, as well as strengthening the use of SEL as a tissue quality measurement tool.
The aim of this study was to show the changes that occur in the viscoelastic properties of the plantar fascia measured by SEL and the changes in the plantar fascia temperature measured by thermography after the application of a 448 kHz CRMR in active healthy subjects immediately after treatment and at the 1-week follow-up. Furthermore, to analyze if an intervention with 448 kHz CRMR in the plantar fascia of the dominant lower limb produces a thermal response in the plantar fascia of the non-dominant lower limb. The final objective was to analyze the level of association between the viscoelastic properties of the PF and the temperature before and after the intervention with 448 kHz CRMR.
Material and methods
Design
This is an open clinical trial. This study was registered in a clinical trial database with ID NCT05460117.
Participants
Volunteers were recruited from a private clinic in Malaga (Spain). A total of 20 plantar fascia from healthy volunteers were analyzed. The inclusion criteria were: (i) being physically active, (ii) having no injuries in the lower limb in the last 2 years, (iii) having no pain or discomfort at the moment of evaluation and (iv) being aged between 24 and 42 years of age. The exclusion criteria were as follows: (i) diagnosis of a systemic inflammatory disease, (ii) diagnosis of connective tissue disease, (iii) previous local trauma, (iv) presence of plantar fibroma, and (v) treatment with plantar fascia corticosteroids, hyaluronic acid, or injections of plasma rich in platelets within the 3 months prior to screening [Citation4,Citation5]. The participants were fully informed of the characteristics of the study before providing signed consent. Informed written and verbal consent were obtained from all participants before enrollment and baseline demographic and clinical data were collected. The study was approved by a Medical Research Ethics Committee (100-2022-H) and conducted in accordance with the Declaration of Helsinki and ethical approval have been obtained for all protocols from the local institutional review board (IRB). This study is reported in line with the standard protocol items of the CONSORT Statemen [Citation27,Citation28].
Allocation
The dominant lower limb is considered as the intervention group and the non-dominant lower limb as the control group ().
Intervention description
Experimental group
Patients received one intervention in the plantar fascia of the dominant lower limb using 448 kHz CRMR. The whole plantar fascia was stimulated. The patients were positioned in ventral decubitus on an examination table, and the central band of the subject’s plantar fasciás was traced by hand from the arch to the heel to discern the borders [Citation29]. Capacitive resistive monopolar radiofrequency at 448 kHz was delivered using ‘INDIBA Activ 8’ equipment (INDIBA S.A. Spain), with a peak power of 200 W and 450 VA. Capacitive (CAP) and resistive (RES) waves were applied using metallic electrodes via a coupling medium. The applicator consists 30 mm Capacitive (CAP) and 30 mm resistive (RES) head. Firstly, Firstly, the CAP was administered as a 5-min thermal dose (based on patient feedback on his/her perception of heat, with the patient’s perception expected to be 8 out of 10). According to patient feedback on his/her perception of heat. Perception number 10 is burn. Subsequently, the RES mode was delivered as a thermal dose (hyperthermia) in a continuous wave for 5 min [Citation2].
SEL measurements
The US imaging was conducted by means of a GE Logiq-S7 and a 3.0-10.0 MHz linear-array transducer (GE Healthcare) with a frequency of 8 MHz and ‘Coded Harmonic Imaging’ was used for the study period. Nevertheless, the US operator could change the focus, gain, or depth, as necessary. The patients were positioned in ventral decubitus on an examination table, and the central band of the plantar fasciás subject was traced by hand from the arch to the heel to discern the borders [Citation30]. Four ultrasound elastography measurements were taken from the calcaneal insertion of the subject’s plantar fascia (). The stiffness color scheme was blue (soft), green (medium), and red (hard) () [Citation4,Citation5,Citation15]. The color histogram was analyzed and subsequently, the mean intensity of each color component of the pixels within a standardized area, was computed.
Figure 2. Region of interest (ROI) and SEL measurements. Note: Left to right: Point 1: PF insertion to the calcaneus; Point 2 body of the FP in mid-proximal portion; Point 3: body of the FP in middle portion; Point 4: body of the PF in mid-distal portion.
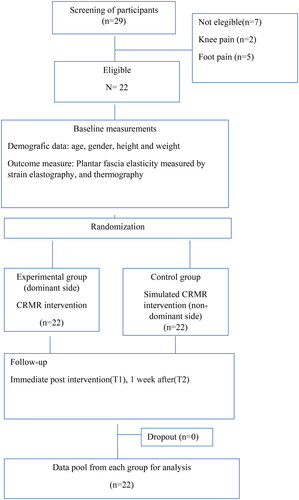
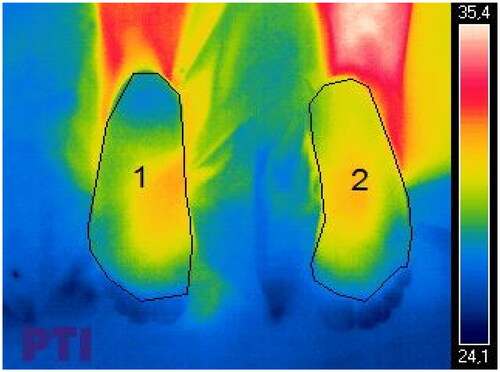
Figure 3. Region of interest (ROI) and thermography measurements.
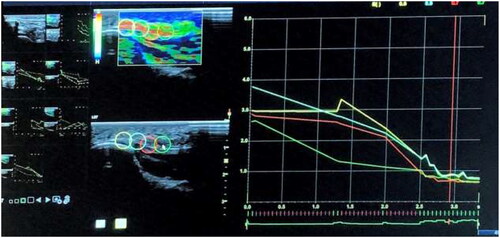
Figure 1. Flow diagram of participants.
Data analysis
SPSS® Statistics version 21.0 (IBM, Chicago, IL, USA) was used for all analyses. The Shapiro–Wilk test was used to verify data distribution normality. To compare the two groups, in regards to clinical characteristics, at baseline (T0), after the intervention (T1) and at the one-week follow-up (T2), a three-way repeated measurement ANOVA was conducted, with three levels corresponding to each time of assessment (T0, T1 and T2). A p-value < 0.05 was considered statistically significant. The following calculations were included: (i) Bonferroni adjustments for multiple comparisons, (ii) a Pearson correlation coefficient for a normal data distribution or (iii) a Spearman’s coefficient in the case of absence of normality. A weak correlation was defined as values between 0.3 and 0.5, with the correlation being considered moderate if the value was between 0.5 and 0.7 and strong if the value was greater than 0.7.
Results
Our results showed that a temperature change, which was measured by thermography, occurred in the plantar fascia after a single intervention (T0-T1) and at the 1-week follow up (T1-T2) (). However, no changes were found in the viscoelastic properties of the plantar fascia after the intervention or at the 1-week follow up (). Our results suggested that there was a vascular response that increases skin temperature although not enough to alter the viscoelastic properties of the plantar fascia. This is the first study to show changes in both plantar fascia viscoelastic properties and in plantar fascia temperature after a radiofrequency intervention (hyperthermia), therefore comparisons with other studies are difficult.
Table 1. Between group differences on plantar fascia elasticity and temperature at baseline (T0); after the intervention (T1); and at one-week (T2) follow-up (95%CI).
Table 2. Levels of association between plantar fascia strain elastography and thermography at baseline (T0); after the intervention (T1); and at one-week (T2) follow-up in both groups.
Discussion
The aim of this study was to show the changes that occur in the viscoelastic properties of the plantar facia measured by SEL and the changes in the plantar fascia temperature measured by thermography after the application of a 448 kHz CRMR in active healthy subjects immediately after treatment and at the1-week follow-up. Furthermore, to analyze if an intervention with 448 kHz CRMR in the plantar fascia of the dominant lower limb produces a thermal response in the plantar fascia of the non-dominant lower limb. The final objective was to analyze the level of association between the viscoelastic properties of the PF and the temperature before and after the 448 kHz CRMR intervention. Our results showed that a temperature change, which was measured by thermography, occurred in the plantar fascia after a single intervention (T0-T1) and at the 1-week follow up (T1-T2). However, no changes were found in the viscoelastic properties of the plantar fascia after the intervention or at the 1-week follow up. Our results suggested that there was a vascular response that increases skin temperature although not enough to alter the viscoelastic properties of the plantar fascia. In this regard, the deep muscle tissue warming can be generated by the current which in turn improve hemoglobin saturation, increase deep and superficial blood flow, cause vasodilation and an increase in temperature. The resulting responses such as an increase in blood perfusion and a resulting temperature increase can explain the visco-elastic changes in a tendon when measured by SEL [Citation7,Citation31].
This is the first study to show changes in both plantar fascia viscoelastic properties and in plantar fascia temperature after a radiofrequency intervention (hyperthermia), therefore comparisons with other studies are difficult.
Previous studies have reported the benefits and the viscoelastic changes in tendons, ligaments and fascia of using 448 kHz CRMR in musculoskeletal disorders [Citation3,Citation8,Citation32]. It is very important for studies using CRMR to be carried out in healthy subjects to better understand which physiological responses normally occur. In this regard, the current used can generate warming of deep muscle tissues which in turn improves hemoglobin saturation, can increase deep and superficial blood flow, cause vasodilation and increase temperature [Citation33,Citation34]. Plantar fasciitis intervention has been reported in many studies [Citation35–37], however, the viscoelastic changes that occur in plantar fascia after the application of a 448 kHz CRMR in active healthy subjects remains unreported in the literature. Nowadays, several studies have reported changes in the viscoelastic properties of plantar fasciitis when using different interventions such as, extracorporeal shockwave [Citation37], ultrasound therapy [Citation36], laser therapy [Citation35] and many types of injections [Citation38]. Alviti et al. [Citation39] reported on an extracorporeal shockwave (ESWT) treatment in plantar fasciopathy measured with SEL. The findings at the 1-month follow up showed an increase in plantar fascia thickness and a softening of the areas on the elastogram color map, which can be attributed to the effects of ESWT on tissues; activating a neovascularization process, amplifying growth factor and protein synthesis to stimulate collagen synthesis and tissue remodelling [Citation39]. In their study, there was an improvement in pain and the number of blue areas in the elastography color map, three months after the treatment had ended. These findings can be correlated with the synthesis of new collagen and therefore, with the restoration of plantar fascia characteristics after the ESWT treatment. In addition, Kim et al. [Citation40] reported SEL values in the evaluation of plantar fasciitis treatment at the follow-up, three months after a collagen injection. After treatment, a mild and statistically insignificant decrease was detected in the mean plantar fascial thickness using grey-scale sonography. No statistically significant difference was seen in either the plantar fascial hypoechogenicity or in the strain ratio. In the plantar fascia, the strain ratio was significantly lower before having the injection, or at the follow-up, which indicates that the fascia elasticity increased after the collagen injection [Citation21,Citation40]. Lastly, Gatz et al. [Citation41] evaluated the clinical effects of a 3-month physical therapy-based treatment and its influence on B-mode and SWE ultrasound findings in patients suffering from plantar fasciitis, reporting that it relieves the associated symptoms. In line with symptom reduction, the stiffness (Young’s-moduli) of the plantar fascia increased significantly, while B-mode ultrasound revealed no measurable changes during the healing process.
In addition, Fernández-Cuevas, I. et al. analyze the use of infrared thermography can be an efficient, effective, and noninvasive method to control internal loads, for example, during strength training. Therefore, a good metabolic indicator could be the skin temperature that might help to quantify the internal workload after strength training. Important information on the recovery status of athletes and thereby their ability to continue training at the highest level may provide analysis of the local thermal response [Citation21]. It is very important to carry out research to see if similar changes could occur when we use an intervention such as shockwave, ultrasound therapy, laser therapy, different types of injections or 448 kHz CRMR. In this regard, the importance of extrapolating the use of infrared thermography to a population with injuries is necessary because the analysis of intratendinous or intrafascial vascular resistance (IVR) can be more useful to understand the physiological state of the tissue [Citation42].
Clinical significance of the results
The results of the present study show clinical relevance. This study is the first that investigates changes in plantar fascia viscoelastic properties measured by SEL, and shows changes in the temperature of plantar fascia after a radiofrequency intervention (hyperthermia). Our results show that while no changes were found in the viscoelastic properties of the plantar fascia after a 448 kHz CRMR intervention program there were changes in plantar fascia temperature measured by thermography. Our results suggested that there was a vascular response although not enough to alter the viscoelastic properties of the plantar fascia.
Strengths and weaknesses of the study
The present study shows several strengths since it is a first step toward better understanding the effects of a single CRMR treatment application on plantar fascia SEL in a healthy population with a 1-week follow-up. Demographic characteristics were similar in both groups (). Furthermore, all SEL measurements were carried out by an experienced professional in musculoskeletal ultrasound imaging, which ensures the high quality of the values obtained. In addition, four ultrasound elastography measurements were taken from the calcaneal insertion of the plantar fascia ().
Table 3. Baseline demographic characteristics.
However, several weaknesses have to be acknowledged. The participants were healthy subjects, thus the presented results must be interpreted with caution, as must any extrapolation to other populations. The whole foot was measured for temperature changes, but only the heel areas (4 ROIs) were measured for the elasticity changes. Further research is suggested to improve knowledge in this field which could include increasing the number of participants and/or including a population with injuries. Furthermore, assessing changes in the elasticity of the tissue over time may help clinicians detect possible injuries as well as serve as an indicator of recovery, which may elicit new treatment lines for those suffering from plantar fasciitis. However, more studies are needed to confirm our results in plantar fascia and other structures and additionally, an analysis after a complete treatment program with healthy and injured subjects, and not only after an intervention, needs to be carried out.
Future longitudinal studies that analyze short, medium, and long-term changes in the elastic properties of tissue and temperature following CRMR treatments, are necessary. It would be interesting for future research to study any temperature increase in the control group after treatment T1. In addition, studies on other load-bearing tendons, such as the patellar tendon or the Achilles tendon, need to be carried out in both healthy and injured populations.
Conclusion
There are changes in PF temperature after a single 448 kHz CRMR intervention but not in the elastic properties of the plantar fascia in healthy subjects. Furthermore, the changes in PF temperature are not associated with the elastic properties of the tissue. In addition to longitudinal designs and standardized intervention programs, more studies are needed to corroborate our findings and better understand the presented results.
Author contributions
Conceptualization, D.A-N and S.N-L; methodology, D.A-N and, A.G-M; validation, M.A-G; formal analysis, P.C-G and, S.N-L.; investigation, M-A-G; resources, M.C-C; writing—original draft preparation, D.A-N, P.C-G and, S.N-L supervision, S.N-L, M.C-C, M.A-G and, A.G-M. All authors have read and agreed to the published version of the manuscript.
Acknowledgement
The authors show their gratitude to the original coauthors who helped in the initial research process. The authors thank all the subjects who have participated in this study.
Disclosure statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data availability statement
The data is available to consult.
Additional information
Funding
References
- Kumaran B, Watson T. Treatment using 448kHz capacitive resistive monopolar radiofrequency improves pain and function in patients with osteoarthritis of the knee joint: a randomised controlled trial. Physiotherapy. 2019;105(1):98–107. doi:10.1016/j.physio.2018.07.004.
- Spottorno J, Gonzalez de Vega C, Buenaventura M, et al. Influence of electrodes on the 448 kHz electric currents created by radiofrequency: a finite element study. Electromagn Biol Med. 2017;36(3):306–314. doi:10.1080/15368378.2017.1354015.
- Takahashi K, Suyama T, Onodera M, et al. Clinical Effects of Capacitive Electric Transfer Hyperthermia Therapy for Lumbago. J Phys Ther Sci. 1999;11(1):45–51. doi:10.1589/jpts.11.45.
- Navarro-Ledesma S, Gonzalez-Muñoz A. Short-term effects of 448 kilohertz radiofrequency stimulation on supraspinatus tendon elasticity measured by quantitative ultrasound elastography in professional badminton players: a double-blinded randomized clinical trial. Int J Hyperthermia. 2021;38(1):421–427. doi:10.1080/02656736.2021.1896790.
- Aguilar-Nuñez D, Cervera-Garvi P, Aguilar-Garcia M, et al. Ultrasound strain elastography reliability in the assessment of the plantar fascia and its relationship with the plantar thickness in healthy adults: an intra and interobserver reliability study in novice evaluators. Biomedicines. 2023;11(7):2040. https://pubmed.ncbi.nlm.nih.gov/37509678/. doi:10.3390/biomedicines11072040.
- Yokota Y, Tashiro Y, Suzuki Y, et al. Effect of capacitive and resistive electric transfer on tissue temperatura, muscle flexibility, and blood circulation. J Nov Physiother. 2017;7:1.
- Fousekis K, Chrysanthopoulos G, Tsekoura M, et al. Posterior thigh thermal skin adaptations to radiofrequency treatment at 448 kHz applied with or without Indiba ® fascia treatment tools. J Phys Ther Sci. 2020;32(4):292–296. doi:10.1589/jpts.32.292.
- Kumaran B, Watson T. Thermal build-up, decay and retention responses to local therapeutic application of 448 kHz capacitive resistive monopolar radiofrequency: a prospective randomised crossover study in healthy adults. Int J Hyperthermia. 2015;31(8):883–895. doi:10.3109/02656736.2015.1092172.
- Aj I-V. Radiofrequency in aesthetics skin treatment: classification and modalities. Dermatol Res Skin Care. 2017;1(1):1–3.
- González-Gutiérrez MD, López-Garrido Á, Cortés-Pérez I, et al. Effects of non-invasive radiofrequency diathermy in pelvic floor disorders: a systematic review. Medicina. 2022;58(3):437. https://pubmed.ncbi.nlm.nih.gov/35334613/. doi:10.3390/medicina58030437.
- Benincá IL, de Estéfani D, Pereira de Souza S, et al. Tissue heating in different short wave diathermy methods: a systematic review and narrative synthesis. J Bodyw Mov Ther.]. 2021;28:298–310. https://pubmed.ncbi.nlm.nih.gov/34776156/. doi:10.1016/j.jbmt.2021.07.031.
- Shah SGS, Farrow A. Assessment of physiotherapists’ occupational exposure to radiofrequency electromagnetic fields from shortwave and microwave diathermy devices: a literature review. J Occup Environ Hyg. 2013;10(6):312–327. https://pubmed.ncbi.nlm.nih.gov/23570423/. doi:10.1080/15459624.2013.782203.
- Koutsojannis C, Andrikopoulos A, Adamopoulos A, et al. Microwave diathermy in physiotherapy: introduction and evaluation of a quality control procedurE. Radiat Prot Dosimetry. 2018;181(3):229–239. https://pubmed.ncbi.nlm.nih.gov/29438554/. doi:10.1093/rpd/ncy018.
- Draper DO, Hawkes AR, Johnson AW, et al. Muscle heating with Megapulse II shortwave diathermy and ReBound diathermy. J Athl Train. 2013;48(4):477–482. https://pubmed.ncbi.nlm.nih.gov/23725462/. doi:10.4085/1062-6050-48.3.01.
- Cuevas-Cervera M, Aguilar-Nuñez D, Aguilar-García M, et al. Patellar tendon elasticity and temperature following after a 448 kilohertz radiofrequency intervention on active healthy subjects: an open controlled clinical trial. Diagnostics. 2023;13(18):2976. https://pubmed.ncbi.nlm.nih.gov/37761343/. doi:10.3390/diagnostics13182976.
- Sconfienza LM, Silvestri E, Orlandi D, et al. Real-time sonoelastography of the plantar fascia: comparison between patients with plantar fasciitis and healthy control subjects. Radiology. 2013;267(1):195–200. doi:10.1148/radiol.12120969.
- Albano D, Messina C, Gitto S, et al. Shear-wave elastography of the plantar fascia: a systematic review and meta-analysis. J Ultrasound. 2023;26(1):59–64. https://pubmed.ncbi.nlm.nih.gov/36662404/. doi:10.1007/s40477-022-00770-4.
- Gatz M, Bejder L, Quack V, et al. Shear Wave Elastography (SWE) for the evaluation of patients with plantar fasciitis. Acad Radiol. 2020;27(3):363–370. doi:10.1016/j.acra.2019.04.009.
- Wu CH, Chiu YH, Chang KV, et al. Ultrasound elastography for the evaluation of plantar fasciitis: a systematic review and meta-analysis. Eur J Radiol. 2022;155:110495. doi:10.1016/j.ejrad.2022.110495.
- Wearing SC, Smeathers JE, Urry SR, et al. The pathomechanics of plantar fasciitis. Sports Med. 2006;36(7):585–611. https://pubmed.ncbi.nlm.nih.gov/16796396/.
- Fernández-Cuevas I, Torres G, Sillero-Quintana M, et al. Thermographic assessment of skin response to strength training in young participants. J Therm Anal Calorim. 2023;148(9):3407–3415. doi:10.1007/s10973-023-11978-9.
- Hillen B, Pfirrmann D, Nägele M, et al. Infrared Thermography in Exercise Physiology: the Dawning of Exercise Radiomics. Sports Med. 2020;50(2):263–282. https://pubmed.ncbi.nlm.nih.gov/31734882/. doi:10.1007/s40279-019-01210-w.
- Dias de Lacerda AP, Rodrigues de Andrade P, Kamonseki DH, et al. Accuracy of infrared thermography in detecting tendinopathy: a systematic review with meta-analysis. Phys Ther Sport. 2022;58:117–125. https://pubmed.ncbi.nlm.nih.gov/36274313/. doi:10.1016/j.ptsp.2022.10.005.
- Hildebrandt C, Raschner C, Ammer K. An overview of recent application of medical infrared thermography in sports medicine in Austria. Sensors. 2010;10(5):4700–4715. https://pubmed.ncbi.nlm.nih.gov/22399901/. doi:10.3390/s100504700.
- Physiology of Thermal Signals. In: Medical devices and systems. CRC Press; 2006. p. 447–466. https://www.taylorfrancis.com/chapters/edit/10.1201/9781420003864-28/physiology-thermal-signals-david-pascoe-james-mercer-lois-de-weerd-21-1
- Gómez Bernal A, Fernández Cuevas I, Alfaro Santafé JJ, et al. Termografía infrarroja para la determinación del perfil térmico en fascitis plantar: estudio descriptivo. Revista Española de Podología. 2020; 31:1. https://dialnet.unirioja.es/servlet/articulo?codigo=7351518&info=resumen&idioma=SPA
- Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. 2016;2(1):64. doi:10.1186/s40814-016-0105-8.
- Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol. 2010;63(8):e1–37. doi:10.1016/j.jclinepi.2010.03.004.
- Heinen EH, Lima K e, Correia R, et al. Reliability in ultrasound measurements of plantar aponeurosis thickness. Foot. 2021;46:101749. doi:10.1016/j.foot.2020.101749.
- Heinen EH, Lima K e, Correia R, et al. Reliability in ultrasound measurements of plantar aponeurosis thickness. Foot (Edinb). 2021;46:21–24.
- Ramirez-GarciaLuna JL, Bartlett R, Arriaga-Caballero JE, et al. Infrared thermography in wound care, surgery, and sports medicine: a review. Front Physiol. 2022;13:838528. doi:10.3389/fphys.2022.838528.
- Takahashi K, Suyama T, Takakura Y, et al. Clinical effects of capacitive electric transfer hyperthermia therapy for cervico-omo-brachial pain. undefined. 2000;12:43–48.
- Rodríguez-Sanz J, López-de-Celis C, Hidalgo-García C, et al. Temperature and current flow effects of different electrode placement in shoulder capacitive-resistive electric transfer applications: a cadaveric study. BMC Musculoskelet Disord. 2021;22(1):139. https://pubmed.ncbi.nlm.nih.gov/33541324/. doi:10.1186/s12891-020-03918-7.
- López-De-Celis C, Hidalgo-García C, Pérez-Bellmunt A, et al. Thermal and non-thermal effects off capacitive-resistive electric transfer application on the Achilles tendon and musculotendinous junction of the gastrocnemius muscle: a cadaveric study. BMC Musculoskelet Disord. 2020;21(1):46. doi:10.1186/s12891-020-3072-4.
- Ulusoy A, Cerrahoglu L, Orguc S. Magnetic resonance imaging and clinical outcomes of laser therapy, ultrasound therapy, and extracorporeal shock wave therapy for treatment of plantar fasciitis: a randomized controlled trial. J Foot Ankle Surg. 2017;56(4):762–767. doi:10.1053/j.jfas.2017.02.013.
- Ultrasonography and clinical outcome comparison of extracorporeal shock wave therapy and corticosteroid injections for chronic plantar fasciitis: A randomized controlled trial. J Musculoskelet Neuronal Interact. 2018;18(1):47– 54. https://pubmed.ncbi.nlm.nih.gov/29504578/
- Al-Siyabi Z, Karam M, Al-Hajri E, et al. Extracorporeal shockwave therapy versus ultrasound therapy for plantar fasciitis: a systematic review and meta-analysis. Cureus. 2022;14(1):e20871. doi:10.7759/cureus.20871.
- Ferreira GF, Sevilla D, Oliveira CN, et al. Comparison of the effect of hyaluronic acid injection versus extracorporeal shockwave therapy on chronic plantar fasciitis: protocol for a randomized controlled trial. PLoS One. 2021;16(6):e0250768. doi:10.1371/journal.pone.0250768.
- Alviti F, D’Ercole C, Schillizzi G, et al. Elastosonographic evaluation after extracorporeal shockwave treatment in plantar fasciopathy. Med Ultrason. 2019;21(4):399–404.
- Kim M, Choi YS, You MW, et al. Sonoelastography in the evaluation of plantar fasciitis treatment: 3-month follow-up after collagen injection. Ultrasound Q. 2016;32(4):327–332. doi:10.1097/RUQ.0000000000000233.
- Gatz M, Betsch M, Quack V, et al. Shear wave elastography for treatment monitoring of plantar fasciitis. J Sports Med Phys Fitness. 2020;60(8):1137–1147. doi:10.23736/S0022-4707.20.10702-3.
- Molina-Payá FJ, Ríos-Díaz J, Carrasco-Martínez F, et al. Infrared thermography, intratendon vascular resistance, and echotexture in athletes with patellar tendinopathy: a cross-sectional study. Ultrason Imaging. 2023;45(2):47–61. doi:10.1177/01617346231153581.