
ABSTRACT
This article reports on teenage pregnancy and associated factors in Ethiopia. All studies available to the year 2020 conducted on teenage pregnancy in Ethiopia were included. The purpose of this systematic review and meta-analysis was to synthesize evidence on the prevalence and associated factors with teenage pregnancy in Ethiopia. The preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines to conduct this meta-analysis were followed by the reviewers. The pooled estimated prevalence of teenage pregnancy in Ethiopia was 23.59% (95% CI: 14.75, 32.43). Sexual practice before the age of 15 years (OR = 1.75(95%CI 1.06, 2.44), no history of contraceptive use OR =3.53 (95%CI 1.94, 5.12) and Marital status OR=2.35 (95%CI1.36, 3.34) were factors associated with teenage pregnancy. Sex education in schools and enhanced contraceptive utilization among adolescents are recommended. Future quantitative as well as qualitative researches should focus on personal as well as social determinants to teenage pregnancy.
Background
World Health Organization (WHO) defines the age group 13–19 years of teenagers. Pregnancy between this age group (teenage pregnancy) is a global reproductive health promotion problem that affects female teenagers, families, and communities, both in developed and developing countries, as children aged 10 to 19 years, unmarried and still at school, become pregnant. It is directly related to the high incidence of pregnancy-related complications that contribute to maternal morbidity and mortality, and social problems. Approximately 16 million adolescent girls aged 15–19 years and 2 million adolescents under the age of 15 years give birth annually in the world. Pregnancy and childbearing in adolescence contribute to increased risks of maternal mortality and morbidity, especially in very young adolescents(Mchunu et al., Citation2012; World Health Organization (WHO), Citation1999).
According to the UNFPA report, each year, an estimated 14 million adolescents between the ages of 15 and 19 give birth globally, and more than 90% of these live births occur in developing countries (Caffe et al., Citation2017). An estimated 70,000 teenaged girls die each year during pregnancy and childbirth, and more than one million infants born to adolescent girls die before their first birthday. Because of such grave health consequences, teenage pregnancies are termed a death sentence in the poorest countries. About 2 million or more of them suffered chronic illness or disabilities, shame, and abandonment. Moreover, each year 2.2 to 4 million adolescents resort to unsafe abortion(Caffe et al., Citation2017; Reynolds et al., Citation2006; United Nations Population Fund, Citation2007).
Adolescent pregnancy and childbearing have distinct and important deleterious consequences at global, societal, and personal levels. Globally, population growth is more rapid when women have their first child in their teenage as the early initiation of giving birth lengthens the reproductive period and subsequently increases fertility. At the societal level, the strong association observed between adolescent childbearing and low levels of educational achievement brings a negative impact on their position and potential contribution to society. Individually, adolescent fertility is associated with adverse maternal and child health outcomes including obstructed labour, low birth weight, foetal growth retardation, and high infant and maternal mortality rate(McDevitt et al., Citation1996; Rafalimanana, Citation2006).
Complications from pregnancy and childbirth are the leading cause of death for adolescent girls between the ages of 15 and 19 in poor countries. Girls in this age group are twice as likely to die from pregnancy and childbirth-related causes, compared with older women. Children born to teenage mothers are 50% more likely to die before the age of one than those born to women in their twenties. Furthermore, among teenagers who become pregnant only a few of them seek antenatal and delivery care from health professionals (Bearinger et al., Citation2007; United Nations Population Fund, Citation2007).
Approximately 16 million adolescent girls aged 15–19 years and 2 million adolescents under the age of 15 years give birth annually. These births constitute roughly 11% of all births worldwide; nearly 95% occur in developing countries. The proportion of adolescents giving birth ranged from 2% in China, to 18% in Latin America and the Caribbean, to more than 50% in sub-Saharan Africa (World Health Organization, Citation2008).
Evidence has shown that factors associated with teenage pregnancy include the age of mother at pregnancy, mother’s educational status, place of residence, employment, contraceptive use, contraceptive non-use, educational status, poverty, breakdown of parental homes, inequality, and poor participation in decision-making, housemaid, monthly income, absence of communication on reproductive health issues with parents, having parental teenage pregnancy, religion ethnicity, being sexually active before the age of 15, and being married before the age of 18 (Ayele, W. M, Citation2013; Beyene et al., Citation2015; Tewodros and et al., Citation2010).
Objectives
This systematic review and meta-analysis was conducted with the objectives of determining the magnitude of teenage pregnancy and identifying factors associated with teenage pregnancy in Ethiopia. The result from this systematic review and meta-analysis may benefit policy makers and stakeholders to improve the prevention as well as management strategies for teenage pregnancy.
Materials and methods
Study design and search strategy
A systematic review and meta-analysis of published and unpublished studies were conducted to assess the pooled prevalence and associated factors of adolescent pregnancy in Ethiopia. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines(AKERS, Citation2009) were strictly followed in doing this review. The databases used to search for studies were; PubMed, Directory of Open Access Journals search, Google Scholar, and African Journals Online (AJOL). All search terms for ‘Prevalence OR Incidence OR Epidemiology AND Adolescent pregnancy OR teen pregnancy OR teenage pregnancy OR young maternal age AND Africa’ were used separately and in combination using the Boolean operators like ‘OR’ or ‘AND’. Also, terms like ‘determinant factors’ OR ‘determinant factors’ OR ‘associated factors’ were used in combination with the above search terms.
Eligibility criteria study selection
All available studies conducted until the year 2020 were included in this review. All cross-sectional studies, case-control studies, and Demographic and Health Survey (DHS) analyses on teenage pregnancy were included in this review. Reviews, commentaries, editorial, case series/reports, and patient stories and studies conducted among the non-adolescent populations were excluded from the analysis. Articles, where their full texts were inaccessible, were excluded. The references of the selected articles were also screened to retrieve any additional articles which could be incorporated in this review.
Quality assessment and data extraction
Articles were screened using their titles, abstracts, and full paper reviews prior to including in the meta-analysis. The Joanna Briggs Institute (JBI) critical appraisal checklistThe Joanna Briggs Institute Reviewer’s Manual, Citation2008) was used to assess the quality of included studies. The tool contains information on sample representativeness of the target population, participant recruitment, adequacy of the sample size, detailed description of the study subjects and study setting, sufficient coverage of the data analysis, objective criteria in the measurement of the outcome variable and identification of subpopulation, reliability, appropriate statistical analysis, and identification of confounding variables. The quality scores of the included studies were assessed and presented using the mean scores to designate as high or low-quality. The JBI tool for prevalence studies (Institute, Citation2017) was used as a guideline for data extraction from the finally selected articles. The data extraction tool contains information on the author and year of the study, title, year study was conducted and year of publication, study area and country, sub-region, study design and type, study population, age range of adolescent participants, sample size, response rate, the outcome measured, and prevalence rate of adolescent pregnancy. Information regarding the publication status was also collected. Additionally, for the factors, a separate data extraction tool was prepared. The tool contains information on author’s name, year of publication, number of pregnant adolescents and total adolescents by residence, marital status, adolescent’s and their family educational status, and parent to adolescent communication on SRH issues was collected.
Data synthesis
Meta-analysis was conducted using STATA 11 Software to compute the pooled prevalence of teenage pregnancy in Ethiopia. A random-effect meta-analysis model was used to pool the overall prevalence of teenage pregnancy in Ethiopia. The heterogeneity test of included studies was assessed by using the I2 statistics. The p-value for I2 statistics less than 0.05 was used to determine the presence of heterogeneity. Low, moderate and high heterogeneity was assigned to I2 test statistics results of 25, 50, and 75% respectively(Higgins et al., Citation2003). The publication bias was assessed using the Egger regression asymmetry test(Begg & Mazumdar, Citation1994)(Egger et al., Citation1997). For meta-analysis results which showed the presence of publication bias (Egger test = p < 0.05), and fill analysis using the random effect analysis was conducted to account for publication bias(Duval, Citation2000).
Ethical consideration
Articles included in the analysis of this review were all available in the public domain; as a result no special ethical considerations were required.
Results
Identification of studies
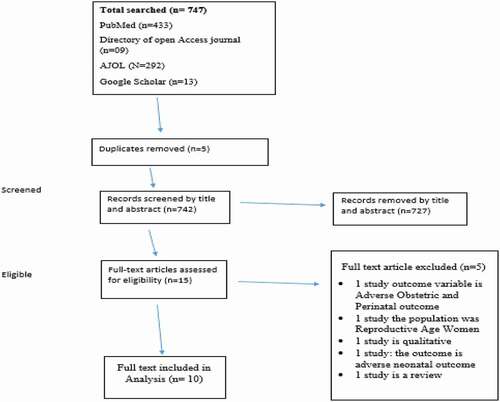
A total of 747 articles were identified through searching both electronic data base and back references. Among these, 725 research articles were excluded as they did not fulfill the eligibility criteria. 22 full-text articles were retrieved of which 12 articles were excluded and finally 10 articles were included in the systematic review and meta-analysis ().
Figure 1. PRISMA flow chart of review researches
Characteristics of included studies
Among the 10 studies included in the systematic review, three studies were cross-sectional (Beyene et al., Citation2015; Habitu et al., Citation2018; Mathewos & Mekuria, Citation2018), three studies were case-control studies (Geda, Citation2019; Kawo & Abate Tadesse, Citation2019; Kidan Ayele et al., Citation2018) and the rest 4 studies were analyses of EDHS data(Alemayehu et al., Citation2010; Ayele, W. M, Citation2013; Birhanu et al., Citation2019; Kassa et al., Citation2019). One study is from each of the regions Tigray (Kidan Ayele et al., Citation2018), Amhara(Habitu et al., Citation2018) and SPPNR(Mathewos & Mekuria, Citation2018). The sample sizes of the studies included ranged from 414 to 14,366; making the total population participated in the studies 36,052 ().
Table 1. Characteristics of included studies
Quality of included studies
The Joanna Briggs Institute (JBI)(Institute, Citation2017) Checklist for Analytical Cross Sectional Studies was used to check the methodological quality of studies included in the review. Accordingly, seven studies were of high methodological quality (>80%) and three studies were moderate methodological quality (60–80%). (Supplementary file)
Pooled prevalence teenage pregnancy in Ethiopia
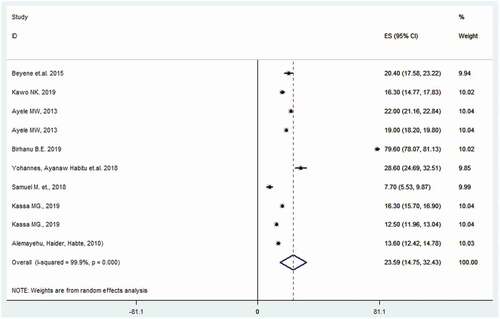
The pooled estimated prevalence of teenage pregnancy in Ethiopia was 23.59% (95% CI: 14.75, 32.43) and the observed heterogeneity was significant (I2 = 99.9%, P < 0.001), the prevalence ranged 7.7% to 79.6% ().
Figure 2. Pooled prevalence of teenage pregnancy in Ethiopia
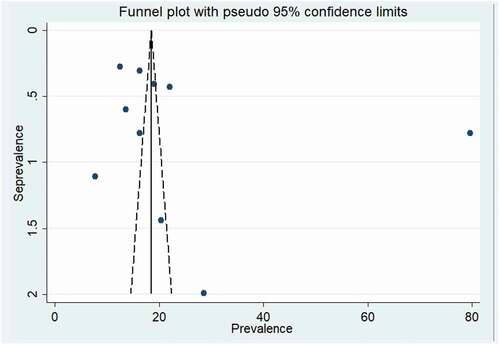
Publication bias
In this systematic review and meta-analysis, both visual inspection of funnel plot and Egger’s test shows no evidence of publication bias (B = 18.66, SE = 17.71.26, p = 0. 323) ().
Figure 3. Forest plot indicating publication bias
Factors associated with teenage pregnancy
As summarized in Sexual experience before the age of 15 years (OR = 1.75 (95%CI 1.06, 2.44), history of no contraceptive use OR = 3.53 (95%CI 1.94, 5.12) and Marital status OR = 2.35 (95%CI1.36, 3.34) were statistically significant factors associated with teenage pregnancy ().
Table 2. Factors associated with teenage pregnancy in Ethiopia
Discussion
Teenage pregnancy is a major public health concern with diverse health consequences on adolescents globally with a higher magnitude in developing countries including Ethiopia. The study reviewed available evidence on the prevalence of teenage pregnancy and associated factors in Ethiopia. A total of 10 studies were included in the analysis, cautiously selected based on specific inclusion criteria. The findings of the review provide insights into the overall magnitude of teenage pregnancy in Ethiopia. This systematic review and meta-analysis was aimed to estimate the prevalence of teenage pregnancy and associated factors in Ethiopia. The pooled prevalence of teenage pregnancy in Ethiopia in this meta-analysis was 23.59% (95% CI: 14.75, 32.43). The estimate showed that it is higher than studies conducted in African countries. A retrospective study conducted in southern Nigeria has reported that the prevalence of teenage pregnancy to be 1.5% (Onwubuariri & Kasso, Citation2019). Cameroonian studies conducted in 2015 and 2017 showed that the prevalence was 13.3% and 8.7%, respectively (Egbe et al., Citation2015; Njim & Agbor, Citation2017). While similar findings have been reported from rural western Kenya teenage pregnancy is 23.3%(Omoroa et al., Citation2018), Nigeria 22.9%. (Amoran, Citation2012) and South Africa 19.2% (Mchunu et al., Citation2012) a study from Cameroon show a high prevalence (60.75%) of teenage pregnancy (Donatus et al., Citation2018).
The review also identifies factors associated with teenage pregnancy. Sexual experience before the age of 15 years, no history of contraceptive use and marital status were factors significantly associated with teenage pregnancy. Adolescents who initiated sexual intercourse before the age of 15 years were more than 1.7 times more likely to get pregnant compared to their counterparts (OR = 1.75(95%CI 1.06, 2.44). Teenagers who started sexual intercourse before the age of 15 years were more than 1.7 times more likely to get pregnant compared to their counterparts (OR = 1.75 (95%CI 1.06, 2.44). Adolescence represents a vulnerable phase in human development as it is a transition from childhood to physical and psychological maturity. During this period, adolescents learn and develop knowledge and skills to deal with critical aspects of their health and development while their bodies mature (UNICEF, Citation2019). As they started to grow physically, emotionally and psychologically they will start to explore. And there are different factors which motivates them to engage in sexual activities like poor economic conditions, peer pressure to be sexually active to prove one’s gender identity, the centrality of sexual activity to definitions and practices of adult masculinity, and gendered inequalities of power. Adolescent girls identified money, fun, and pleasure as important factors. The mass media stimulated adolescents through erotic visual images, music, soap operas and pornographic movies (Kempadoo & Dunn, Citation2001). Furthermore girls at their early ages are more likely to get coerced to sexual intercourse. The younger the teen at the time of coitarche, the more likely it is that the sexual episode was not voluntary(Anderson Moore et al., Citation1989). In many societies, the communal recognition of sexual maturation in girls brings expectations of increased household responsibilities, restricts movement around boys and men, and increases pressures for sexual initiation early in their age which may lead them to get pregnant during their adolescence age (World Bank, Citation2007).
Teenagers who do not use contraceptives were more likely have an early teenage pregnancy OR = 3.53 (95%CI 1.94, 5.12). Contraception is the most effective way to prevent teenage pregnancy among adolescents however due to different reasons like accessibility and lack of awareness contraceptive prevalence in the SSA countries is 38.6% (Chandra-Mouli et al., Citation2014; Greene & Merrick, Citation2015; Sánchez-Páez & Ortega, Citation2018). Effective counselling regarding contraceptive options and provision of resources to increase access are key components of adolescent health care however contraception utilization is still low and different reasons have been reported for adolescents not to use contraceptives, occurrence of an unintended pregnancy, reports of side effects, behaviour issues and desire for pregnancy (Borovac-Pinheiro et al., Citation2016) (Care, Citation2017). During adolescence, young people navigate numerous physical, cognitive, emotional, and behavioural changes as they acquire increasing autonomy and experiment in many areas. Experimentation may include alcohol or drug use, smoking, and sexual activity, all of which may be associated with sexual and reproductive health risks such as unintended teenage pregnancy and sexually transmitted infections (STIs) (Todd & Black, Citation2020)
The review also indicated married adolescents were prone to get pregnant early. Compared to single adolescents married adolescents were more than two times more likely to get pregnant OR = 2.35 (95%CI1.36, 3.34). Consistently a systematic reviews in Africa and a qualitative study from Lao have shown that adolescents who were married are more likely to be pregnant(Gm et al., Citation2018; Sychareun et al., Citation2018). In many societies, adolescents are under pressure to marry and bear children early (World Health Organization (WHO), Citation2020).
Limitations of the study
This meta-analysis has some limitations. The first limitation of this study was only English articles were considered to estimate the pooled prevalence of teenage pregnancy and associated factors in Ethiopia. Six out of 10 included studies were analysis of EDHS the result of this meta-analysis may be affected with social desirability bias. Except for the analysis of EDHS articles the rest are conducted in four regions of the country which may not fully representative of the complete picture of the status of teenage pregnancy in the country.
Implications for practice
For teenagers to have a smooth transition to healthy and effective adulthood they need to be observed and cared starting from early adolescence, since this could be an important opportunity for public health intervention. All responsible bodies including Ministry of health, health care facilities and others should work to reduce teenage pregnancy. A comprehensive approach to prevent teenage pregnancy should implemented including school-based sex educations, contraceptive accessibility and prevention of early marriage. School-based sex education programmes can reduce early age sexual initiations and promote contraceptive use among adolescents in school. Contraceptive accessibility and uptake should be guaranteed by the health facilities.
Conclusion
The analysis showed that teenage pregnancy is still high in Ethiopia. Sexual experience before the age of 15 years, not using contraceptive and marital status were factors associated with teenage pregnancy. Prevention of early marriage and creating awareness about contraceptive and ensuring its accessibility is recommended to prevent teenage pregnancy. Further investigations should be carried out to observe for the reproductive health, and sexual practice among adolescents and psychological and physiological explanations and cultural assumptions needs to be explored to establish the causes that lead adolescents to early sexual debut and subsequent complications.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data sharing is not applicable to this article since there is no new data created or analyzed in this study.
Additional information
Funding
Notes on contributors
Kassa Mamo
Kassa Mamo is a University lecturer of Midwifery at Ambo University, Ethiopia. His research focuses on Midwifery, women and child health, and reproductive health. He has been engaged in different research activities as well as community services and extracurricular activities at the university.
Melese Siyoum
Melese Siyoum is an assistant professor and a Ph.D. fellow at Hawassa University, Ethiopia. He is a university lecturer and researcher. His research interests focus on maternal and child health, family planning, and reproductive health. He has been involved in a number of research activities and community services at the University.
Adamu Birhanu
Adamu Birhanu is an assistant professor of psychiatry nursing at Ambo University, Ethiopia. He has authored and co-authored a number of articles on different disciplines. His research mainly focuses on adult Psychiatry and addiction. He has been working on various studies in mental health and public health issues.
References
- Akers, J. (2009). Systematic reviews: CRD’s guidance for undertaking reviews in health care, University of York: Centre for Reviews and Dissemination. http://www.amazon.co.uk/Systematic-Reviews-Guidance-Undertaking-Healthcare/dp/1900640473/ref=sr_1_6?ie=UTF8&s=books&qid=1228830560&sr=1-6
- Alemayehu, T., Haider, J., & Habte, D. (2010). Determinants of adolescent fertility in Ethiopia. Ethiop. Journal of Health Development, 24(1), 30–38. https://doi.org/https://doi.org/10.4314/ejhd.v24i1.62942
- Alemayehu, T., Haider, J., & Habte, D. (2010). Determinants of adolescent fertility in Ethiopia. Ethiopian Journal of Health Development, 24(1), 30–38. https://doi.org/https://doi.org/10.4314/ejhd.v24i1.62942
- Amoran, O. E. (2012). A comparative analysis of predictors of teenage pregnancy and its prevention in a rural town in Western Nigeria. International Journal for Equity in Health, 11(1), 37. https://doi.org/https://doi.org/10.1186/1475-9276-11-37
- Anderson Moore, K., Winquist Nord, C., & Peterson, J. L. (1989). Nonvoluntary sexual activity among adolescents. Family Planning Perspectives, 21(3), 110–114. https://doi.org/https://doi.org/10.2307/2135660
- Ayele, W. M. (2013). Differentials of early teenage pregnancy in Ethiopia, 2000, and 2005. DHS Working Papers No. 90, (February). http://dhsprogram.com/pubs/pdf/WP90/WP90.pdf
- Bearinger, L. H., Sieving, R. E., Ferguson, J., & Sharma, V. (2007). Global perspectives on the sexual and reproductive health of adolescents: Patterns, prevention, and potential. Lancet, 369(9568), 1220–1231. https://doi.org/https://doi.org/10.1016/S0140-6736(07)60367-5
- Begg, C. B., & Mazumdar, M. (1994). Operating characteristics of a rank correlation test for publication bias. Biometrics, 50(4), 1088. https://doi.org/https://doi.org/10.2307/2533446
- Beyene, A., Muhiye, A., Getachew, Y., Hiruye, A., Mariam, D. H. A., Derbew, M., Mammo, D., & Enquselassie, F. (2015). Assessment of the magnitude of teenage pregnancy and its associated factors among teenage females visiting assosa general hospital. Ethiopian Medical Journal, Suppl 2, 25–37. www.emjema.org
- Birhanu, B. E., Kebede, D. L., Kahsay, A. B., & Belachew, A. B. (2019). Predictors of teenage pregnancy in Ethiopia: A multilevel analysis. BMC Public Health, 19(1), 1. https://doi.org/https://doi.org/10.1186/s12889-019-6845-7
- Borovac-Pinheiro, A., Surita, F., D’Annibale, A., Pacagnella, R., & Pinto E Silva, J. (2016). Adolescent contraception before and after pregnancy—choices and challenges for the future. Revista Brasileira de Ginecologia E Obstetrícia/RBGO Gynecology and Obstetrics, 38(11), 545–551. https://doi.org/https://doi.org/10.1055/s-0036-1593971
- Caffe, S., Plesons, M., Camacho, A. V., Brumana, L., Abdool, S. N., Huaynoca, S., Mayall, K., Menard-Freeman, L., de Francisco Serpa, L. A., Gomez Ponce de Leon, R., & Chandra-Mouli, V. (2017). Looking back and moving forward: Can we accelerate progress on adolescent pregnancy in the Americas? Reproductive Health, 14(1), 1. https://doi.org/https://doi.org/10.1186/s12978-017-0345-y
- Care, C. O. A. H. (2017). Counseling adolescents about contraception. Obstetrics and Gynecology, 131 (728), 35–42. https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Adolescent-Health-Care/Counseling-Adolescents-About-Contraception
- Chandra-Mouli, V., McCarraher, D. R., Phillips, S. J., Williamson, N. E., & Hainsworth, G. (2014). Contraception for adolescents in low and middle income countries: Needs, barriers, and access. Reproductive Health, 11(1), 1–8. https://doi.org/https://doi.org/10.1186/1742-4755-11-1
- Donatus, L., Sama, D. J., Tsoka-Gwegweni, J. M., & Cumber, S. N. (2018). Factors associated with adolescent school girl’s pregnancy in kumbo east health district north west region Cameroon. Pan African Medical Journal, 31(138) . https://doi.org/https://doi.org/10.11604/pamj.2018.31.138.16888
- Duval, S. T. R. A. (2000). nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. JASA, 95(449), 89–98. https://doi.org/https://doi.org/10.1111/j.0006-341X.2000.00455.x
- Egbe, T. O., Omeichu, A., Halle-Ekane, G. E., Tchente, C. N., Egbe, E. N., & Oury, J. F. (2015). Prevalence and outcome of teenage hospital births at the buea health district, South West Region, Cameroon. Reproductive Health, 12(1), 1. https://doi.org/https://doi.org/10.1186/s12978-015-0109-5
- Egger, M., Smith, G. D., Schneider, M. M. C., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ, 315(7109), 629–634. https://doi.org/https://doi.org/10.1136/bmj.315.7109.629
- Geda, Y. (2019). Determinants of teenage pregnancy in Ethiopia: A Case–control study, 2019. Current Medical Issues, 17(4), 112. https://doi.org/https://doi.org/10.4103/cmi.cmi_12_19
- Gm, K., Ao, A., Aa, O., & Aw, Y. (2018). Prevalence and determinants of adolescent pregnancy in Africa: A systematic review and Meta-analysis. Reproductive Health, 15 (1), 195. http://www.epistemonikos.org/documents/7799f1f0fd9d13cc576cf6ea7a893c3ff3f387f5.
- Greene, M., & Merrick, T. (2015). The case for investing in research to increase access to and use of contraception among adolescents. Washington: Alliance for Reproductive, Maternal, and Newborn Health.
- Habitu, Y. A., Yalew, A., & Bisetegn, T. A. (2018). Prevalence and factors associated with teenage pregnancy, northeast Ethiopia, 2017: A cross-sectional study. Journal of Pregnancy, 2018(5). https://doi.org/https://doi.org/10.1155/2018/1714527
- Higgins, J. P. T., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses. British Medical Journal, 327(7414), 557–560. https://doi.org/https://doi.org/10.1136/bmj.327.7414.557
- Institute, J. B. (2017). The Joanna Briggs institute critical appraisal tools for use in JBI systematic reviews: Checklist for prevalence studies. Crit Apprais Checkl Preval Stud, 7. http://joannabriggs.org/research/critical-appraisal-tools.html
- Institute, T. J. B. (2017). The joanna briggs institute critical appraisal tools for use in JBI systematic reviews, checklist for analytical cross sectional studies. http://joannabriggs.org/research/critical-appraisal-tools.html
- Joanna Briggs Institute. (2008). Joanna Briggs Institute reviewers' manual: 2008 edition. Adelaide: Joanna Briggs Institute.
- Kassa, G. M., Arowojolu, A. O., Odukogbe, A. T. A., & Yalew, A. W. (2019). Trends and determinants of teenage childbearing in Ethiopia: Evidence from the 2000 to 2016 demographic and health surveys. Italian Journal of Pediatrics, 45(1), 1. https://doi.org/https://doi.org/10.1186/s13052-019-0745-4
- Kawo, K. N., & Abate Tadesse, Z. D. B. D. (2019). Determinants of teenage pregnancy in Rural Ethiopia. Journal of Health, Medicine and Nursing, 68, 8–16. https://doi.org/https://doi.org/10.7176/JHMN/68-02
- Kempadoo, K., & Dunn, L. (2001). Factors that shape the initiation of early sexual activiy among adolescent boys and girls: A study in three communities in Jamaica. Kingston: UNICEF and UNFPA. http://www.unicef.org/evaldatabase/files/JAM_2001_804.pdf
- Kidan Ayele, B. G., Gebregzabher, T. G., Hailu, T. T., & Assefa, B. A. (2018). Determinants of teenage pregnancy in degua tembien district, Tigray, Northern Ethiopia: A community-based case-control study. PLoS ONE, 13(7). https://doi.org/https://doi.org/10.1371/journal.pone.0200898
- Mathewos, S., & Mekuria, A. (2018). teenage pregnancy and its associated factors among school adolescents of Arba Minch Town, Southern Ethiopia. Ethiopian Journal of Health Sciences, 28(3), 287–298. https://doi.org/https://doi.org/10.4314/ejhs.v28i3.6
- McDevitt, T. M., Adlakha, A., Fowler, T. B., & Harris-Bourne, V. (1996). Trends in adolescent fertility and contraceptive use in the developing world, US bureau of the census.
- Mchunu, G., Peltzer, K., Tutshana, B., & Seutlwadi, L. (2012). Adolescent pregnancy and associated factors in South African youth. African Health Sciences, 12 (4), 426–434. http://www.ajol.info/index.php/ahs/article/view/85072/75042%5Cnhttp://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed11&NEWS=N&AN=2013081281.
- Njim, T., & Agbor, V. N. (2017). Adolescent deliveries in semi-urban Cameroon: Prevalence and adverse neonatal outcomes. BMC Research Notes, 10(1), 1. https://doi.org/https://doi.org/10.1186/s13104-017-2555-3
- Omoroa, T., Grayb, S. C., George Otienoa, C. M., Phillips-Howardc, P. A., Tameka Hayesd, F. O., & Gust, D. A. (2018). Teen pregnancy in rural western Kenya: A public health issue. InternatIonal Journal of Adolescence and Youth, 23(4), 399–408. https://doi.org/https://doi.org/10.1080/02673843.2017.1402794
- Onwubuariri,M.I.,&Kasso,T. (2019). Teenage pregnancy: Prevalence, pattern and predisposing factors in a tertiary Hospital, Southern Nigeria. Asian Journal of Medicine and Health, 17(3), 1–5.https://doi.org/https://doi.org/10.9734/ajmah/2019/v17i330165
- Rafalimanana, H. (2006). Adolescent Fertility in the developing world: Levels and Trends in the 1990s and early 2000s. Population Association of America (United Nations). http://paa2006.princeton.edu/papers/60711
- Reynolds, H. W., Wong, E. L., & Tucker, H. (2006). Adolescents’ use of maternal and child health services in developing countries. International Family Planning Perspectives, 32(1), 6–16. https://doi.org/https://doi.org/10.1363/3200606
- Sánchez-Páez, D. A., & Ortega, J. A. (2018). Adolescent contraceptive use and its effects on fertility. Demographic Research, 38(1), 1359–1388. https://doi.org/https://doi.org/10.4054/DemRes.2018.38.45
- Sychareun, V., Vongxay, V., Houaboun, S., Thammavongsa, V., Phummavongsa, P., Chaleunvong, K., & Durham, J. (2018). Determinants of adolescent pregnancy and access to reproductive and sexual health services for married and unmarried adolescents in rural Lao PDR: A qualitative study. BMC Pregnancy and Childbirth, 18(1), 1. https://doi.org/https://doi.org/10.1186/s12884-018-1859-1
- Todd, N., & Black, A. (2020). Contraception for adolescents. Journal of Clinical Research in Pediatric Endocrinology, 12(Suppl 1), 28–40. https://doi.org/https://doi.org/10.4274/jcrpe.galenos.2019.2019.S0003
- UNICEF. (2019). UNICEF: For all children. https://www.unicef.org/reports
- United Nations Population Fund. (2007). Giving girls today and tomorrow: Breaking the cycle of teenage pregnancy.
- World Bank. (2007). World development report: Development and the next generation.
- World Health Organization (WHO). (1999). Programming for adolescent health and development. Report of a WHO/UNFPA/UNICEF study group on programming for adolescent health. World Health Organization technical report series (Vol. 886).
- World Health Organization (WHO). (2020). Adolescent pregnancy. https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy
- World Health Organization. (2008). Why is giving special attention to adolescents important for achieving MD Goal 5? <https://www.Who.Int/Making_Pregnancy_Safer/Events/2008/Mdg5/Adolescent_Preg.Pdf>