
ABSTRACT
Background
All common variants of primary progressive aphasia (PPA) exhibit naming deficits. Variants are distinguished by relative deficits in repetition (logopenic; lvPPA), object knowledge (semantic; svPPA), and agrammatism or articulation (non-fluent/agrammatic; nfavPPA; Gorno-Tempini et al., 2011). The Hopkins Action Naming Assessment (HANA) is a 30-item verb naming task that can distinguish between variants (Stockbridge et al., 2021). Item-level accuracy is driven by target verb frequency, semantic information density, and conceptual concreteness of the target word (Stockbridge, Venezia, et al., 2022).
Aims
In this investigation, we examined whether word frequency, semantic density, concreteness, and age of acquisition (AoA) also shaped the incorrect responses patients provided. We hypothesised that error responses would vary in these dimensions as a function of PPA variant.
Methods & Procedures
The HANA was administered to 271 participants with PPA, resulting in 443 total administrations and 4,529 analysable error responses. Standardised differences between error and target responses for frequency, density, concreteness, and AoA were calculated and averaged for each patient. Analysis of variance (ANOVA) for correlated samples was used to compare variants and planned post-hoc analyses examined the effect of variant on each response quality.
Outcomes & Results
Participants were similar in age, sex, handedness, and education. There was a significant interaction between PPA variant and the standardised mean differences in lexical qualities (Pillai’s Trace = 0.11, F(9, 747) = 3.19, p < 0.001). Univariate ANOVAs revealed significant differences in the semantic density of error responses relative to the target (F(3) = 7.91, p < 0.001, ηP2= 0.09), as individuals with lvPPA tended to produce error responses with greater semantic density than the target when compared to the words produced by individuals with nfavPPA (mean difference = 1.45, 95%CI = [0.60,2.29], p < 0.001; Figure 1). PPA variants also differed in the concreteness of their error responses relative to the target (F(3) = 5.99, p<0.001, ηP2 = 0.07), as error responses produced by individuals with nfavPPA were significantly more concrete than those with lvPPA (mean difference = 0.08, 95%CI = [0.02,0.13], p = 0.003) or svPPA (mean difference=0.08, 95%CI = [0.02,0.14], p = 0.007). Variants did not differ significantly in AoA or frequency of responses relative to their targets. All variants tended to produce more frequent words with a lower AoA than the target verb.
Conclusions
Error responses tended to be more semantically dense, more concrete, higher frequency, and younger AoA than the target verb. However, PPA variants differed significantly in the extent to which these broader trends held true. These distinct patterns may be included as part of a larger diagnostic picture that to distinguish among PPA variants.
Introduction
Progressive neurodegenerative impairment with central language features, called primary progressive aphasia (PPA), can be further distinguished for most patients into one of three common variants (Gorno-Tempini et al., Citation2011): non-fluent/agrammatic (nfavPPA), semantic (svPPA), or logopenic (lvPPA). NfavPPA and svPPA are associated primarily with underlying frontotemporal lobar degeneration. Degeneration of the left posterior fronto-insular regions is associated with nfavPPA, while degeneration to the anterior temporal regions is associated with svPPA. In contrast, lvPPA is associated primarily with Alzheimer’s disease affecting the left posterior perisylvian or parietal regions (Harris et al., Citation2013). Variants also are distinguishable behaviorally by relative language deficits. All variants experience naming deficits (Hillis et al., Citation2004), but individuals with nfavPPA have relatively spared single-word comprehension and object knowledge. Individuals with nfavPPA often experience agrammatism (Montembeault et al., Citation2018) and impaired comprehension of complex sentences (Thompson & Mack, Citation2014). Some have found evidence that people with agrammatism have unique difficulty with verbs (Silveri & Ciccarelli, Citation2007; Thompson et al., Citation2012). Apraxia of speech also is common (Ash et al., Citation2010). Individuals with svPPA have impaired word retrieval and object knowledge but often spared repetition and grammar. Individuals with lvPPA experience impaired word retrieval and sentence repetition (often attributed to phonological working memory deficits) usually with spared grammar, object knowledge, and comprehension at the word level (Montembeault et al., Citation2018).
Accuracy in verb naming on the Hopkins Action Naming Assessment (HANA; https://score.jhmi.edu/downloads.html; Breining et al., Citation2021) appears to be a useful basis for distinguishing among PPA variants (Stockbridge et al., Citation2021). The HANA is a 30-item verb picture naming task frequency-matched (Van der Wouden, Citation1990) with Boston Naming Test (Williams et al., Citation1989) 30-item short-form. High scores on the HANA are predictive of nfavPPA while low scores are predictive of svPPA, and lvPPA is predicted best by mid-to-high scores but is not readily distinguishable from nfavPPA (Stockbridge et al., Citation2021). Beyond accuracy, prior work has demonstrated that certain lexical qualities drive the difficulty of naming a given target verb. Words that are more frequently used in a language are more likely to be named correctly by healthy individuals and people with language deficits, including PPA (Bastiaanse et al., Citation2016; DeDe, Citation2012; Diesfeldt, Citation2011; Kremin et al., Citation2001; Patterson et al., Citation2006; Ralph et al., Citation2011; Wilson et al., Citation2014). More accurate verb naming by individuals with PPA is also impacted by greater semantic density and concreteness (versus abstractness; Stockbridge, Venezia, et al., Citation2022). Words conveying more specific information tend to be lower in frequency and higher in concreteness. Semantic density captures the quality that some words convey richer semantic information (e.g., shear, shred, shave) while others are more general and widely applied (e.g., cut). In order to compare semantic density across a large set of words in a replicable, scalable, and objective way, one can count the total number of distinct meanings a word has, called the word’s synset (van Ewijk & Avrutin, Citation2016). Larger synsets typically are associated with more general words. Prior work has demonstrated that lower numbers of synsets contribute to greater difficulty in svPPA and lvPPA, but not nfavPPA or unclassifiable PPA, even when accounting for the overlapping influences of each factor and participant-level random effects (Stockbridge, Venezia, et al., Citation2022).
However, it is not yet known whether the same factors that influence which verbs are more likely to be named correctly also drive the responses patients produce when answering incorrectly. While accuracy is a frequent means of examining differences among PPA variants, it is rarer to examine incorrect responses. This perhaps is because the latter is far more labour-intensive and introduces challenges when distilling divergent responses into comparable units of analysis. Rather than classifying each response by the dominant perceived relationship with the target (e.g., semantic versus phonological errors), this work sought to avoid the potential subjectivity in judging overlapping influences introduced by this method and expand upon the findings from Stockbridge et al. (Citation2022) by examining the relative influence of four aspects of error responses: frequency, semantic density, concreteness, and age of acquisition. We examined the hypothesis that error responses would vary in these four dimensions as a function of their variant of PPA. Our specific hypothesis was that substituted words provided in error would be driven by the same factors that drove accuracy. While not all of the same aspects of words were considered as in Stockbridge et al. (Citation2022), we expected semantic density might be higher among error responses provided by those with svPPA and lvPPA than those with nfavPPA, since lower semantic density contributed to decreased accuracy specifically for individuals with those variants.
Materials and methods
Records reviewed
This study involved a retrospective analysis of prospectively collected outpatient clinical data from March 2011 to February 2022 previously described with regard to accuracy (Stockbridge, Venezia, et al., Citation2022). Participants were selected on the basis of having received the HANA during their evaluation. Participants had follow-up visits every 6 to 12 months, and their performance from all visits during which the HANA was administered was analysed, so long as the administration resulted in at least one erroneous response.
Clinical PPA diagnosis and variant classification were determined based on extensive cognitive-linguistic evaluation, neurological evaluation, review of medical history, and consultation with family, if present. Diagnosis was affirmed with magnetic resonance imaging for all patients to differentially diagnose variant via location and severity of atrophy. Asymmetric frontal atrophy was required for a diagnosis of nfavPPA. Left temporo-parietal atrophy was required for a diagnosis of lvPPA, and primarily left anterior and inferior temporal atrophy was required for a diagnosis of svPPA. Some patients were unclassifiable because they either did not meet any of the core criteria (e.g., were only anomic and dysgraphic) or met core criteria for more than one variant. Although known genetic mutations are associated with svPPA, nfavPPA, and unclassifiable PPA, genetic data was not available for individuals in the present sample. Over the course of follow-up visits, some participants’ profiles changed to be best described by a different variant than first identified or to shift from being unclassifiable to fitting criteria of a given variant. HANA performance associated with a given administration was labelled according to the variant best capturing their performance at that given visit. This affected 19/271 (7%) patients whose data were considered. It is not rare for the variant to change over time, as the variant is just a collection of symptoms that reflect the location of neurodegeneration. As the disease spreads, new symptoms are seen. The variant (behavioural syndrome) is loosely correlated with the underlying disease but is not a “diagnosis” itself. Just as the symptoms of a common cold often change over the course of the disease, the diagnosis remains a common cold.
Assessment & data extraction
The HANA consists of 30 illustrations of common actions and requires the participant to produce the verb (single word) that the image represents. Patients are informed that the test stimuli are intended to elicit action words only. The HANA was designed to be frequency-matched to the 30-item short form (Mack et al., Citation1992) of the Boston Naming Test (Kaplan et al., Citation2001). Each illustration is presented to the patient, and their response is recorded for later scoring. A single verb response of any conjugation is counted as correct, but nominalizations are errors (i.e., “prescribe” or “prescribing” is correct, but “prescription” is not). As the test is not designed to diagnose difficulties in articulation, scrutable dysarthric or apraxic errors were ignored. Inscrutable responses were removed from further analysis.
As expected, patients’ errant responses took many forms. To arrive at a consistent basis for examining errors’ characteristics, a single word was extracted from each response based on the following rules. 1) If a response contained one or more response attempts, the last verb included in the response was used (e.g., “eat, no swallow cookies” => “swallow”). 2) If a response contained a verb phrase, the first verb was used (e.g., “try to eat” => “try”). 3) Linking verbs were ignored, and their complements were coded (e.g., “he seems to be eating” => “eat”). 4) Negative responses were treated as responses if there was no alternative provided (e.g., “it’s not swallowing” => “swallowing”). All verbs were analysed in their lemma form.
If a response contained no verbs, the last content word was used, and the singular or plural usage of nouns was preserved. Responses were assumed to be verbs in accordance with the task demands, even if they could be a noun (e.g., “run” was always assumed to be used as a verb). Non-word responses and responses with no content words were excluded.
Error response characterization
Four lexical qualities were identified a priori based on the findings from examining HANA item accuracy (Stockbridge, Venezia, et al., Citation2022). Word frequency, semantic density, and concreteness were examined in the previous investigation by Stockbridge et al. (Citation2022) and were measured using the same methods in the present work. Briefly, word frequency was measured using SUBTLEX log10 values for each word (Brysbaert et al., Citation2012). Individuals with all variants of PPA demonstrated increased difficulty with low-frequency words (Diesfeldt, Citation2011; Patterson et al., Citation2006; Ralph et al., Citation2011; Wilson et al., Citation2014). Semantic density was examined in WordNet (Miller, Citation1995). This is a measure of the number of distinct meanings a given word has (“synset”), and it is interpreted as the breadth of the single underlying lexical concept. For example, “vacuum” has a synset of five. Four meanings are nouns (e.g., “the absence of matter,” and “the electrical home appliance that cleans by suction”) and one verb (“to clean with a vacuum”). Prior authors have demonstrated that higher numbers of synsets for a given verb appear to facilitate processing among those with agrammatism secondary to stroke (van Ewijk & Avrutin, Citation2016). Given that several items had unusually high numbers of synsets relative to the remaining items, a log10 transform was applied prior to analysis. Concreteness, the degree to which a concept refers to a perceptible entity, was assessed using mean ratings on a 5-point scale. Higher ratings reflect “something that exists in reality; you can have immediate experience of it through your senses (smelling, tasting, touching, hearing, seeing) and the actions you do” (Brysbaert et al., Citation2014). The fourth previously analysed trait, valency, was dropped from this investigation due to its lack of influence on target verb accuracy and because it is a unique quality of verbs (thus, could not be analysed in any responses that did not include a verb). Age of acquisition (AoA) was included in the present analysis instead, reflecting upon the previously reported effect of AoA on word finding in dementia (Cuetos et al., Citation2010; Hirsh & Funnell, Citation1995; Ralph et al., Citation1998; Taylor, Citation1998). AoA norms were extracted from Kuperman et al. (Citation2012). See for examples.
Table 1. Example Target Word and Response Pairs.
Error response words that did not exist in one or more of the corpora used were excluded from that analysis. Seventeen participants of the 271 exclusively made errors that could not be analysed for semantic density and concreteness (their few errors were not present in these smaller corpora) and were dropped from these analyses. Thus, the number of patients contributing error data to the analysis was 271 for the frequency and AoA analysis and 254 for the semantic density and concreteness analysis.
Once the frequency, AoA, concreteness, and semantic density of each error response was determined, a standardised difference between the value for the error response and the value for the target response was calculated (e.g., (word frequency of error response – word frequency of target response)/word frequency of target response). This was done to account for differences in lexical characteristics of the different target verbs when considering the erroneous label produced when responding to that item. Next, standardised differences were averaged for each patient. As the investigative question was about the nature of distinct errors as a function of variant, this both stabilized profiles within individuals and addressed the possibility of a single patient with a high number of errors having an outsized effect on the analysis of the variant generally. Patients whose identified variant had evolved between visits had their responses averaged separately by variant with each variant included as a unique participant in the sample. Thus, a high error rate did not result in the individual contributing disproportionately to the overall dataset. Average standardised differences for each of the four lexical qualities for each participant constituted the four dependent variables that were entered into analysis.
Statistical analysis
We hypothesized that profiles of relative strengths and weaknesses in individuals with different PPA variants would lead them to produce erroneous responses that differed systematically in their frequency, age of acquisition, concreteness, or semantic density. An analysis of variance (ANOVA) for correlated samples (also called a repeated measures ANOVA when examining change over time) was chosen as the analytical approach, as dependent variables were expected to be significantly correlated (actual Pearson correlations among targets ranged from 0.65-0.06, while correlations among standardized differences ranged from 0.68-.001). This ANOVA was considered using a significance level of α = 0.05. Post-hoc analyses of a significant interaction effect were planned using univariate analyses of variance to examine the effect of variant on each of the four response qualities (α = 0.05/4 = 0.01), followed by an examination of Scheffe-corrected pairwise contrasts to explore significant univariate ANOVAs.
Results
The demographics of the patients whose error data were included in the analysis are summarised in . The entire set of 271 patients diagnosed with PPA contributed a total of 443 HANA administrations (each individual contributed 1.6 HANA administrations), resulting in 4,529 error responses able to be analysed (). Groups varied significantly in the part of speech included in their response (; p < 0.001 for all contrasts) and standardized differences varied significantly as a function of whether the word included in error was a verb versus a noun or adjective (Pillai’s Trace = 0.14, F(3, 4459) = 234.84, p < 0.001). The standardized differences in frequency between error verbs and the target was significantly greater than for nouns (Mean Difference = 0.36, p < 0.001), and standardized differences in age of acquisition were significantly lower than that for nouns (Mean Difference = -0.07, p < 0.001). Standardized differences in semantic density were significantly greater in verbs than nouns (Mean Difference = 4.21, p < 0.001) or adjectives (Mean Difference = 3.23, p < 0.001). Standardized differences in concreteness were significantly smaller in verbs versus nouns (Mean Difference = -0.21, p < 0.001) and significantly larger in verbs versus adjectives (Mean Difference = 0.21, p < 0.001). Although closed class responses did occur, there were too few to analyse. Patients with each of the four variants were similar in age at first visit F(3) = 0.37, p = 0.77, sex distribution, χ2 = 6.4, p = 0.09, handedness, χ2 = 1.5, p = 0.71, and education, F(3) = 1.86, p = 0.14.
Figure 1. Standardized mean differences between targets and responses in four dimensions.
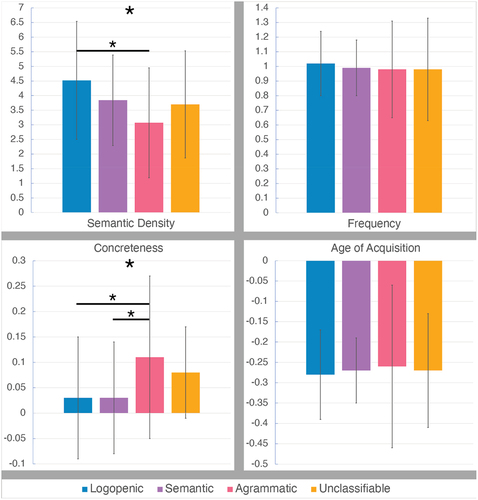
Table 2. Summary of sample characteristics.
Table 3. Summary of error responses by part of speech.
The majority of error responses maintained consistency with the task demands of eliciting a verb. The next most common error responses were nouns. Anecdotally, many error verbs were general, all-purpose verbs substituted for more specific verbs (e.g., “put” the pencil in the sharpener for “sharpen,” “put out” the fire for “extinguish”). Noun responses often were tools or descriptions of the subject doing the action (e.g., “razor” for “shave” or “baby” for “suck”). Modifiers and other parts of speech were far less common. Few to no responses examined were suggestive that the patient may have misidentified the picture; however, apparent self-cuing attempts were common.
The analysis of variance for correlated samples demonstrated a significant interaction between PPA variant and the standardised mean differences in lexical qualities, Pillai’s Trace = 0.11, F(9, 747) = 3.19, p < 0.001. Univariate analyses of variance used to characterise this significant interaction effect are summarised in .
Table 4. Standardised differences in lexical qualities by subtype.
PPA variants differed in the semantic density of their error responses relative to the target, F(3) = 7.91, p < 0.001, ηP2 = 0.09. While all PPA variants’ error responses tended to be more semantically dense than the target verb, this difference was driven by the fact that individuals with lvPPA tended to produce error responses with greater semantic density than the target (e.g., “clean” is more semantically dense than the target “vacuum”). The difference in semantic density between response and target was higher for lvPPA than for individuals with the agrammatic variant, mean difference = 1.45, 95%CI = [0.60,2.29], p < 0.001. Other pairwise differences were not significant.
PPA variants also differed in the concreteness of their error responses relative to the target, F(3) = 5.99, p <0.001, ηP2 = 0.07. All variants produced responses marginally more concrete than the target, but error responses produced by individuals with nfavPPA were significantly more concrete than those with lvPPA, mean difference = 0.08, 95%CI = [0.02,0.13], p = 0.003). or svPPA, mean difference = 0.08, 95%CI = [0.02,0.14], p = 0.007. Variants did not differ significantly in the age of acquisition, F(3) = 0.16, p = 0.92, or frequency, F(3) = 0.42, p = 0.74, of their responses relative to their targets. All variants produced words that were more frequent with a lower age of acquisition than the target verb.
Discussion
In this investigation, we examined whether there were variant-specific patterns in the standardised differences between target verb frequency, semantic density, concreteness, and age of acquisition and the erroneous responses patients provided. We were particularly interested in examining whether variant-specific patterns of lexical qualities were consistent with those observed to influence item accuracy. That is, if a lexical quality had been shown to make certain target verbs more difficult to name for one variant of PPA, were the words they produced in their erroneous responses easier in this dimension?
Overall, individuals with PPA trended toward making errors that differed from the target in similar ways. Error responses were more concrete, more semantically dense, higher frequency words with lower age of acquisition than the targeted verb. This was consistent with our prior finding that HANA accuracy was predicted best by a model in which word frequency received the highest weight (0.62), followed by concreteness (0.21), and semantic density (0.17) (Stockbridge, Venezia, et al., Citation2022).
Standardised differences in age of acquisition and frequency between erroneous responses and target verbs were similar across PPA variants. However, semantic density and concreteness drove unique effects for certain variants. Those with lvPPA provided incorrect responses that were significantly more semantically dense (had more distinct usages) when compared to the target than other variants. This is consistent with our prior finding that low semantic density contributed to increased difficulty for individuals with lvPPA and svPPA but not nfavPPA or unclassifiable variants (Stockbridge, Venezia, et al., Citation2022). Those with svPPA had the second highest standardised differences in semantic density, which did not achieve significant difference from the other variants in pair-wise contrasts. Prior authors also have found modest evidence that individuals with svPPA have difficulty producing verbs rated as being sufficiently specific and related, instead erring toward more general, all-purpose verbs (Lukic et al., Citation2022). However, the same was not observed in lvPPA. Within the dual-stream model of language (Hickok & Poeppel, Citation2000, Citation2004, Citation2007), atrophy in dorsal pathways (longitudinal fasciculus and SLF) is consistent with behavioral patterns seen in lvPPA and nfavPPA. In contrast, ventral changes (uncinate and inferior longitudinal fasciculus) are associated with svPPA (Keator et al., Citation2022). Semantic knowledge deficits are thought to be under-recognised in lvPPA (Sikora et al., Citation2021).
Those with nfavPPA demonstrated a unique effect of concreteness compared to the other variants. Consistent with our prior analysis of HANA accuracy, which found no evidence that low concreteness affected accuracy in individuals with svPPA or lvPPA (Stockbridge, Venezia, et al., Citation2022), incorrect responses provided by those with lvPPA and svPPA demonstrated negligible standardised differences in concreteness. In contrast, those with nfavPPA demonstrated standardised differences in concreteness 3-4 times that seen in svPPA or lvPPA. Their unique tendency to provide incorrect responses that were more concrete than their targets is an unexpected finding that must be interpreted cautiously given the nature of this task. HANA verbs skew toward high concreteness to achieve consistent elicitation of the target verb using a single static illustration. This, in turn, influences standardised differences between target verbs and the errors produced. A future investigation examining spontaneous discourse may provide additional information on the relationship between lexical access in nfavPPA and the concreteness of concepts. These distinct patterns may be included as part of a larger diagnostic picture that to distinguish among PPA variants.
A dimension of response we were able to describe secondary to the investigative hypothesis was the rate of substitution of verbs for other parts of speech when responding in error. While groups did include nouns, verbs, and adjectives in differing distributions and parts of speech do have differing tendencies in frequency, age of acquisition, semantic density, and concreteness, the interpretation of this observation was not straightforward. It seemed equally plausible that individuals could have made errors that substituted different parts of speech because those words had lexical qualities that made them more easily produced (word qualities drove word choice outside of the intended response parameters). However, it seemed equally likely that patients could have included other parts of speech for other reasons (e.g., momentarily forgetting the task demands). When patients provided non-verb responses, they were provided with additional cues to provide verb responses. Therefore, we did not have a design that permitted us to distinguish between these interpretations (e.g., by looking at runs of similar error responses within the task to infer strategy). A future direction of this work would be to examine whether patients forced to provide a constrained verb response show similar effects of semantic density and concreteness to those observed in the present trial. However, this ambiguity remains a potential limitation to the interpretation of these findings.
Throughout the investigation, individuals with unclassifiable PPA behaved in ways inconsistently associated with any one other common variant, often falling between the trends in performance seen in svPPA and nfavPPA. This was not unexpected. Unclassifiable PPA often represents a hodgepodge of underlying profiles, which may at any one time include those very early in their PPA course, who later do fall under the classification criteria of a common variant (Stockbridge, Tippett, et al., Citation2022), those very late in their PPA course who have such severe deficits across domains that their differential strengths are no longer easily measured, or those whose presentation is a result of mixed pathology or may reflect the potential for additional, uncommon PPA variants. Unfortunately, teasing apart the relative contribution of these explanations is extremely challenging, often simply because analyses are underpowered to examine them. In over a decade of outpatient clinical evaluations, 29 such individuals completed the HANA out of 34 total identified as having uvPPA in that time (Stockbridge, Tippett, et al., Citation2022). PPA as a whole is a rare syndrome, affecting 20-40% of those with frontotemporal lobar degeneration, who themselves have a prevalence of 2.7-15.0 per 100,000 (Grossman, Citation2010). Even with the highest prevalence estimates, based on the inclusion of individuals with uvPPA in our sample (34/271), if 6 per 100,000 have PPA, only 75 individuals per 10,000,000 would be unclassifiable. Our deliberate decision not to exclude uvPPA from our analyses reflects a concerted effort to continue building upon what is known about these individuals, even if our sample is necessarily modest in size.
While this investigation is based upon a large sample size and substantial total number of errors, there are limitations to the methods utilized. For example, when data are averaged (as was the case with participant visits), the resulting value can obfuscate true multimodal distributions. Moreover, including all manner of word classes included in erroneous responses, rather than just verbs, may introduce systematic differences in the factors examined across word types. However, there was no a priori reason to suspect that these would vary asymmetrically as a function of PPA variant.
Taken together, these results highlight the value of uncommonly examined lexical qualities – namely, semantic density and concreteness, which do not often receive the attention in the literature that word frequency and age of acquisition do. We hope that these findings will inspire future work to better understand the effect of these lexical qualities, particularly utilizing the relatively objective operationalization of semantic density using synsets. As has occurred for post-stroke aphasia, we also hope a better understanding of the relationship between semantic density and concreteness and PPA variant will continue to inspire the development of new clinical interventions for patients with PPA (Bailey et al., Citation2020).
Disclosure statement
Dr. Hillis receives compensation from the American Heart Association as Editor-in-Chief of Stroke and from Elsevier as Associate Editor of PracticeUpdate Neurology. All authors receive salary support from NIH (NIDCD) through grants.
Data availability statement
Deidentified participant data will be made available from the Inter-university Consortium for Political and Social Research (ICPSR) upon publication.
Additional information
Funding
References
- Ash, S., McMillan, C., Gunawardena, D., Avants, B., Morgan, B., Khan, A., Moore, P., Gee, J., & Grossman, M. (2010). Speech errors in progressive non-fluent aphasia. Brain and Language, 113(1), 13–20. https://doi.org/10.1016/j.bandl.2009.12.001
- Bailey, D. J., Nessler, C., Berggren, K. N., & Wambaugh, J. L. (2020). An aphasia treatment for verbs with low concreteness: A pilot study. American Journal of Speech-Language Pathology, 29(1), 299–318. https://doi.org/10.1044/2019_AJSLP-18-0257
- Bastiaanse, R., Wieling, M., & Wolthuis, N. (2016). The role of frequency in the retrieval of nouns and verbs in aphasia. Aphasiology, 30(11), 1221–1239. https://doi.org/10.1080/02687038.2015.1100709
- Breining, B. L., Faria, A. V., Caffo, B., Meier, E. L., Sheppard, S. M., Sebastian, R., Tippett, D. C., & Hillis, A. E. (2021). Neural regions underlying object and action naming: Complementary evidence from acute stroke and primary progressive aphasia. Aphasiology. http://dx.doi.org/10.1080/02687038.2021.1907291
- Brysbaert, M., New, B., & Keuleers, E. (2012). Adding part-of-speech information to the SUBTLEX-US word frequencies. Behavior Research Methods, 44(4), 991–997. https://doi.org/10.3758/s13428-012-0190-4
- Brysbaert, M., Warriner, A. B., & Kuperman, V. (2014). Concreteness ratings for 40 thousand generally known English word lemmas. Behavior Research Methods, 46(3), 904–911. https://doi.org/10.3758/s13428-013-0403-5
- Cuetos, F., Herrera, E., & Ellis, A. W. (2010). Impaired word recognition in Alzheimer’s disease: The role of age of acquisition. Neuropsychologia, 48(11), 3329–3334.
- DeDe, G. (2012). Effects of word frequency and modality on sentence comprehension impairments in people with aphasia. American Journal of Speech-Language Pathology, 21(2). https://doi.org/10.1044/1058-0360(2012/11-0082)
- Diesfeldt, H. (2011). The phonological variant of primary progressive aphasia, a single case study. Tijdschrift voor Gerontologie en Geriatrie, 42(2), 79–90. https://doi.org/10.1007/s12439-011-0013-6
- Gorno-Tempini, M. L., Hillis, A. E., Weintraub, S., Kertesz, A., Mendez, M., Cappa, S. F., Ogar, J. M., Rohrer, J., Black, S., & Boeve, B. F. (2011). Classification of primary progressive aphasia and its variants. Neurology, 76(11), 1006–1014. https://doi.org/10.1212/WNL.0b013e31821103e6
- Grossman, M. (2010). Primary progressive aphasia: clinicopathological correlations. Nature Reviews Neurology, 6(2), 88–97. https://doi.org/10.1038/nrneurol.2009.216
- Harris, J. M., Gall, C., Thompson, J. C., Richardson, A. M., Neary, D., du Plessis, D., Pal, P., Mann, D. M., Snowden, J. S., & Jones, M. (2013). Classification and pathology of primary progressive aphasia. Neurology, 81(21), 1832–1839. https://doi.org/10.1212/01.wnl.0000436070.28137.7b
- Hickok, G., & Poeppel, D. (2000). Towards a functional neuroanatomy of speech perception. Trends in Cognitive Sciences, 4(4), 131–138. https://doi.org/10.1016/S1364-6613(00)01463-7
- Hickok, G., & Poeppel, D. (2004). Dorsal and ventral streams: A framework for understanding aspects of the functional anatomy of language. Cognition, 92(1–2), 67–99. https://doi.org/10.1016/j.cognition.2003.10.011
- Hickok, G., & Poeppel, D. (2007). The cortical organization of speech processing. Nature Reviews Neuroscience, 8(5), 393–402. https://doi.org/10.1038/nrn2113
- Hillis, A. E., Oh, S., & Ken, L. (2004). Deterioration of naming nouns versus verbs in primary progressive aphasia. Annals of Neurology: Official Journal of the American Neurological Association and the Child Neurology Society, 55(2), 268–275. https://doi.org/10.1002/ana.10812
- Hirsh, K. W., & Funnell, E. (1995). Those old, familiar things: Age of acquisition, familiarity and lexical access in progressive aphasia. Journal of Neurolinguistics, 9(1), 23–32.
- Kaplan, E., Goodglass, H., & Weintraub, S. (2001). Boston Naming Test-2 (BNT-2) (2nd ed.). Pro-Ed.
- Keator, L. M., Yourganov, G., Faria, A. V., Hillis, A. E., & Tippett, D. C. (2022). Application of the dual stream model to neurodegenerative disease: Evidence from a multivariate classification tool in primary progressive aphasia. Aphasiology, 36(5), 618–647. https://doi.org/10.1080/02687038.2021.1897079
- Kremin, H., Perrier, D., De Wilde, M., Dordain, M., Le Bayon, A., Gatignol, P., Rabine, C., Corbineau, M., Lehoux, E., & Arabia, C. (2001). Factors predicting success in picture naming in Alzheimer’s disease and primary progressive aphasia. Brain and Cognition, 46(1–2), 180–183. https://doi.org/10.1006/brcg.2000.1270
- Kuperman, V., Stadthagen-Gonzalez, H., & Brysbaert, M. (2012). Age-of-acquisition ratings for 30,000 English words. Behavior Research Methods, 44, 978–990. https://doi.org/10.3758/s13428-012-0210-4
- Lukic, S., Licata, A. E., Weis, E., Bogley, R., Ratnasiri, B., Welch, A., Hinkley, L., Miller, Z., García, A., & Houde, J. (2022). Auditory verb generation performance patterns dissociate variants of Primary Progressive Aphasia. https://doi.org/10.31234/osf.io/ajy7m
- Mack, W. J., Freed, D. M., Williams, B. W., & Henderson, V. W. (1992). Boston Naming Test: shortened versions for use in Alzheimer’s disease. Journal of Gerontology, 47(3), P154–P158. https://doi.org/10.1093/geronj/47.3.P154
- Miller, G. A. (1995). WordNet: a lexical database for English. Communications of the ACM, 38(11), 39–41. https://doi.org/10.1145/219717.219748
- Montembeault, M., Brambati, S. M., Gorno-Tempini, M. L., & Migliaccio, R. (2018). Clinical, anatomical, and pathological features in the three variants of primary progressive aphasia: a review. Frontiers in Neurology, 9, 692. https://doi.org/10.3389/fneur.2018.00692
- Patterson, K., Ralph, M. A. L., Jefferies, E., Woollams, A., Jones, R., Hodges, J. R., & Rogers, T. T. (2006). “Presemantic” cognition in semantic dementia: Six deficits in search of an explanation. Journal of cognitive neuroscience, 18(2), 169–183. https://doi.org/10.1162/jocn.2006.18.2.169
- Ralph, M. A. L., Graham, K. S., Ellis, A. W., & Hodges, J. R. (1998). Naming in semantic dementia—what matters? Neuropsychologia, 36(8), 775–784.
- Ralph, M. A. L., Sage, K., Heredia, C. G., Berthier, M. L., Martínez-Cuitiño, M., Torralva, T., Manes, F., & Patterson, K. (2011). El-La: The impact of degraded semantic representations on knowledge of grammatical gender in semantic dementia. Acta Neuropsychologica. https://doi.org/10.0000/01.3001.0001.0774
- Sikora, J., Stein, C., Ubellacker, D., Walker, A., & Tippett, D. C. (2021). Longitudinal decline in spoken word recognition and object knowledge in primary progressive aphasia. Medicine, 100(22). https://doi.org/10.1097/MD.0000000000026163
- Silveri, M. C., & Ciccarelli, N. (2007). Naming of grammatical classes in frontotemporal dementias: linguistic and non linguistic factors contribute to noun-verb dissociation. Behavioural Neurology, 18(4), 197–206. https://doi.org/10.1155/2007/428191
- Stockbridge, M. D., Tippett, D. C., Breining, B. L., & Hillis, A. E. (2022). When words first fail: Predicting the emergence of primary progressive aphasia variants from unclassifiable anomic performance in early disease. Aphasiology, 1–13. https://doi.org/10.1080/02687038.2022.2084706
- Stockbridge, M. D., Tippett, D. C., Breining, B. L., Vitti, E., & Hillis, A. E. (2021). Task performance to discriminate among variants of primary progressive aphasia. Cortex, 145, 201–211. https://doi.org/10.1016/j.cortex.2021.09.015
- Stockbridge, M. D., Venezia, J. H., Vitti, E., Tippett, D. C., & Hillis, A. E. (2022). Verb frequency and density drive naming performance in primary progressive aphasia. Aphasiology, 1–17. https://doi.org/10.1080/02687038.2022.2142036
- Taylor, R. (1998). Effects of age of acquisition, word frequency, and familiarity on object recognition and naming in dementia. Perceptual and Motor skills, 87(2), 573–574.
- Thompson, C. K., Lukic, S., King, M. C., Mesulam, M. M., & Weintraub, S. (2012). Verb and noun deficits in stroke-induced and primary progressive aphasia: The Northwestern Naming Battery. Aphasiology, 26(5), 632–655. https://doi.org/10.1080/02687038.2012.676852
- Thompson, C. K., & Mack, J. E. (2014). Grammatical impairments in PPA. Aphasiology, 28(8–9), 1018–1037. https://doi.org/10.1080/02687038.2014.912744
- Van der Wouden, T. (1990). Celex: Building a multifunctional polytheoretical lexical data base. Proceedings of BudaLex, 88, 363–373.
- van Ewijk, L., & Avrutin, S. (2016). Lexical access in non-fluent aphasia: A bit more on reduced processing. Aphasiology, 30(11), 1264–1282. https://doi.org/10.1080/02687038.2015.1135867
- Williams, B. W., Mack, W., & Henderson, V. W. (1989). Boston naming test in Alzheimer’s disease. Neuropsychologia, 27(8), 1073–1079. https://doi.org/10.1016/0028-3932(89)90186-3
- Wilson, S. M., Brandt, T. H., Henry, M. L., Babiak, M., Ogar, J. M., Salli, C., Wilson, L., Peralta, K., Miller, B. L., & Gorno-Tempini, M. L. (2014). Inflectional morphology in primary progressive aphasia: An elicited production study. Brain and Language, 136, 58–68. https://doi.org/10.1016/j.bandl.2014.07.001