
ABSTRACT
Electropalatography (EPG) has been used in the past 50 years for studying the patterns of contact between the tongue and the palate during speech production in typical speakers and those with speech disorders due to different causes. At the 7th EPG Symposium in Japan that was held online on 24 January 2021 (see: https://epg-research.sakura.ne.jp/), a panel of invited experts discussed their views regarding further developments and application of the technique. This paper provides a summary of this discussion. EPG offers information on articulation which cannot be replaced by other instrumental measures of speech. Identified areas for further hardware development are thinner EPG plates, better dental and palatal coverage, wireless connectivity, and sensors that provide additional articulatory information (e.g. tongue pressure, tongue-palate distance). EPG can serve as a resource for teaching speech disorders and phonetics. Furthermore, EPG therapy can be combined with telepractice in the speech therapy of clients with speech disorders.
Introduction
At the 7th Electropalatography (EPG) Symposium in Japan that was held online on 24 January 2021 (see: https://epg-research.sakura.ne.jp/), an international panel of experts was invited to discuss the impact of the COVID-19 pandemic on research and speech therapy using EPG and the protective measures adopted (reported in Lee et al., Citation2022), as well as their views regarding the future developments of EPG. This discussion was timely because the most recently published state-of-the-art reports date back over 15 years (e.g. Scobbie et al., Citation2004; Wrench, Citation2007). Moreover, the occurrence of the COVID-19 pandemic and the corresponding protective measures and restrictions prompted revisions of EPG procedures (Lee et al., Citation2022). This made us reflect on our current practice and think about how the recent changes might impact on our way in carrying out EPG research and therapy in the long run. The panel of experts agreed to document this discussion for sharing with colleagues in the research and clinical communities. Hence, this paper first gives an overview of how EPG works and summarises the state of the art. Then, the possibilities of further development and application of EPG in research, as a clinical tool in speech intervention, and for teaching speech disorders and phonetics are discussed.
Introduction to EPG
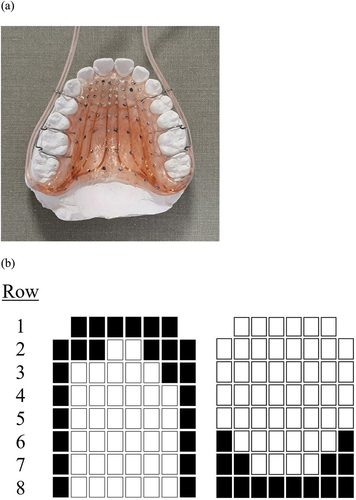
EPG is a computerised instrumental technique that allows users to detect, record, and display in real time where on the hard palate the tongue makes contact during speech production. The speaker wears a custom-made palatal EPG plate embedded with electrodes or sensors on the lingual surface (Hardcastle, Gibbon, Jones et al., Citation1991; see ). The contact between the tongue and the palate is detected by the electrodes. The signal is then transmitted through thin wires and processed by an external processing unit (a multiplexer) that is connected to an EPG machine and a computer. Hence, EPG only shows where on the palate the tongue makes contact, but it does not show which part of the tongue makes the contact (see for examples of tongue palate contact patterns). The speech signal is also audio-recorded and synchronised with the spatial and temporal information of tongue palate contact. This allows investigation of contact patterns of different speech sounds in an utterance.
Figure 1. (a) A custom-made palatal EPG plate of the Reading system displayed on a dental plaster cast and (b) two EPG frames that show the tongue palate contact pattern typically observed in alveolar plosives /t, d, n/ (left) and velar plosives /k, ɡ, ŋ/ (right). The 62 boxes represent the 62 electrodes embedded in eight horizontal rows on the plate, with the filled boxes indicating the presence of tongue palate contact at the corresponding electrodes.
There are three EPG systems that are currently available commercially: the LinguaGraph (icSpeech, Rose Medical Solutions Ltd., UK), the WinSTARS (Asahi Roentgen Ltd., Kyoto, Japan), and the SmartPalate system (CompleteSpeech, USA). Previous EPG systems included the Dynamic Palatograph (DP; Rion Ltd., Tokyo, Japan) that was used mainly in Japan in the 1970–80s, the WinEPGTM (Articulate Instruments Ltd., Edinburgh, UK) and the preceding Reading EPG systems that were used mainly in the UK, Europe, and Hong Kong, and the predecessors of the US system – the Kay Elemetrics Palatometer and the LogoMetrix palatometer system – that were used mainly in the US. The first Reading EPG system was developed in the late 1960s by Professor William Hardcastle in the UK, and the subsequent versions, EPG2 and EPG3, were developed and used up to the 90s before WinEPGTM came along. The US system was developed by Professor Samuel Fletcher in the late 1960s and produced by different manufacturers (for the history of EPG, see e.g. Articulate Instruments Ltd, Citation2013; Lee, Citation2021; Zin et al., Citation2021).
The different EPG systems mentioned above share similar general engineering design (see, e.g. Kochetov, Citation2020; Lee, Citation2019, Citation2021; Zin et al., Citation2021, for a recent account), but they differ in the hardware and software specifications. For example, the Reading-type EPG plate (developed for the Reading system, used with the succeeding WinEPGTM and compatible with the LinguaGraph and WinSTARS) has 62 electrodes embedded according to anatomical landmarks of the palate and upper teeth (Hardcastle et al., Citation1989; see, ). The electrodes are arranged in eight horizontal rows across the palate, with six electrodes in the most anterior row or Row 1, and eight in each of Row 2–8. Row 1 is placed along the palatal junctures of the upper front incisors and Row 8 at the juncture between the hard and soft palates. Moreover, Row 1–4 are placed closer to each other, occupying the anterior one-third of the plate (Hardcastle et al., Citation1989). The thin copper wires soldered to the electrodes are gathered behind the back of the last molar on both sides to form two bundles of wires that leave laterally at the corners of the mouth (Wrench, Citation2007). The EPG plate of the SmartPalate system uses up to 124 equidistant electrodes distributed in the anterior, lateral, and posterior part of the plate (see, e.g. in Fabus et al., Citation2015). The thin wires leave the mouth centrally. The WinSTARS employs Bluetooth technology for wireless transmission of the signal from the multiplexer to a laptop. In addition, the software of WinSTARS can display video input from a nasopharyngoscope, making simultaneous investigation of velopharyngeal function and lingual articulation possible.
To use EPG in research or speech intervention, the first step is to make a dental plaster cast of the palate and upper teeth of the research participants or the clients, which is done based on an alginate impression made by a dentist or an orthodontist. The dental model is then sent to a dental device company that makes EPG plates. When the EPG plate arrives, the speakers are advised to wear the device for at least 2 hours in order to get used to talking with the plate in the mouth before any articulation assessment (McLeod & Searl, Citation2006; see, which shows the key steps involved in using EPG and also Figure 8 in Zin et al., Citation2021). The input from different specialists – the dentists or orthodontists who make the dental models, the dental technicians who make the EPG plates, the technical support regarding hardware and software issues from the EPG manufacturers – are essential to continue the research and clinical viability of using EPG. The cost of using EPG may vary between research labs or clinics. For example, the cost of making the dental model and the EPG plates can be reduced if these can be manufactured ‘in house’. According to Cleland and Preston (Citation2021), the EPG plates cost ‘between about $200 [US Dollar, for the CompleteSpeech system] and $600 [for the Reading-type plate] in 2019’ (p. 586). The cost, time, and practical inconvenience of custom-making the EPG plate may be seen as a limitation of EPG. However, the technique is unique in a number of ways that cannot be replaced by any other current kinematic measures of speech.
Figure 2. The general key steps involved in using EPG in research and/or speech therapy.
Application of EPG
Many speech sounds in the world’s languages are produced within the oral cavity via lingual articulatory gestures (see, e.g. Ladefoged & Maddieson, Citation1996). As EPG is the only instrumental technique designed to capture the details of tongue palate contact dynamics during speech, the information is important for the way we describe speech sounds in terms of place and manner of articulation. EPG has been used extensively for research and clinical purposes (see, e.g. Fletcher, Citation1992; Gibbon & Wood, Citation2010; Ladefoged, Citation2003; Stone, Citation1997). Moreover, it is being constantly developed to date (Gibbon & Lee, Citation2011; Gibbon & Nicolaidis, Citation1999; Lee, Citation2021; Wrench, Citation2007). Other kinematic techniques such as ultrasound tongue imaging (UTI) and electromagnetic articulography (EMA) are quite useful for quantifying tongue shapes and positions during speech, but they are not designed to capture the details of tongue placement on the palate. This makes EPG not only unique but also suitable for use in combination with techniques such as EMA and UTI.
Another advantage of EPG over some other kinematic techniques (e.g. UTI) is that it offers relatively straightforward data reduction indices such as percent contact and centre of gravity (COG) index (see, e.g. Gibbon & Nicolaidis, Citation1999; Hardcastle, Gibbon, Nicolaidis et al., Citation1991; Lee, Citation2021). Percent contact is the ratio of the number of electrodes contacted to the total number of electrodes embedded on the EPG plate, expressed as a fraction of 100. The COG index is ‘a single numerical value representing the position of the greatest concentration of activated electrodes across the palate in the front/back dimension’ (Gibbon & Crampin, Citation2001, p. 99). For the visual display of tongue palate contact, it is intuitive which makes EPG user- and client-friendly (Gibbon & Wood, Citation2010). However, there are specific areas of hardware and software design, where further developments would be welcomed by researchers and clinicians.
Desirable further developments in hardware and software design of EPG
Although hardware improvements are generally more expensive than software updates and cost-effectiveness might be an issue, there are several areas where EPG hardware might improve further. Thinner plates with better dental and palatal coverage, wireless connectivity, and new sensors for obtaining additional articulatory information (e.g. tongue pressure and tongue-palate distance) are some of the areas where advances might be expected.
Thickness and coverage of EPG plate
The thickness of the EPG plate and the coverage of the palate are perennial concerns. The thickness of the most widely used Reading-type acrylic EPG plate is around 2 to even 3 mm at the alveolar ridge, which is potentially problematic for articulatory precision and comfort (McAuliffe et al., Citation2008; Wrench, Citation2007). In contrast to the acrylic plates, the thermoformed plates (e.g. the Articulate and the Kay plates) are thinner and have a uniform thickness throughout the surface of the plate (see, for an example of a thermoformed EPG plate). This results in shorter adaptation period to the presence of the plate in the mouth (Searl et al., Citation2006). Another advantage of the thermoformed plates is reduced manufacturing time, when compared with acrylic resin design, because of the faster plate-shaping process (Wrench, Citation2007). The manufacturing time of an EPG plate can be reduced further by using pre-tested flexible circuits (see, ), instead of the conventional method of embedding individual electrodes on the plate, as soldering and wiring of each electrode is no longer needed (e.g. Lee et al., Citation2022). The use of pre-tested flexible circuits is compatible with thermoformed plates (see the left half of the EPG plate in ). An alternative EPG plate design combining the acrylic-type plate and pre-tested flexible circuits is the Mcyam plate (Yamamoto Dental Clinic, Nishinomiya, Japan) (see, ).
Figure 3. (a) A thermoformed EPG plate (displayed on a dental plaster cast) that shows the comparison of two types of electrode placement, i.e., the use of pre-tested flexible circuits (left) and the conventional method of individual electrode placement (right); (b) a pre-tested flexible circuit (right) comprised of electrodes (left) embedded on an electrode sheet (middle); and (c) a Mcyam EPG plate.
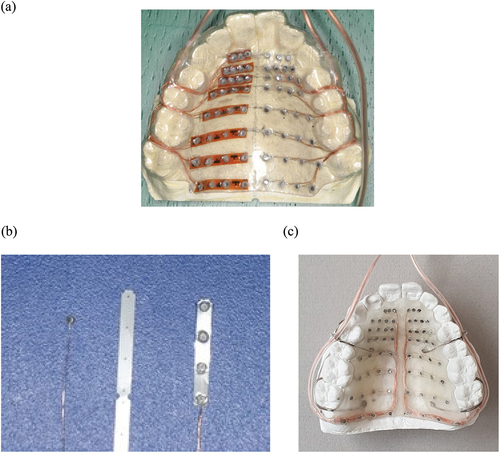
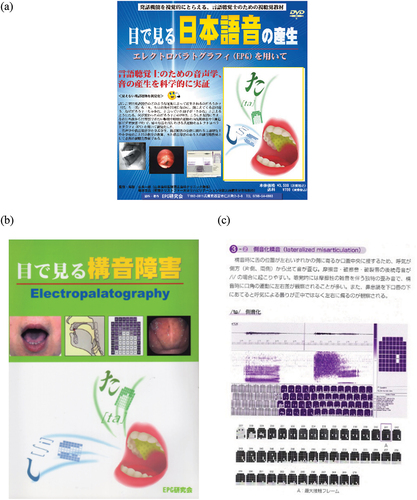
Figure 4. (a) Cover of ‘Visualizing Japanese speech sounds production – Using electropalatography’ (DVD; Yamamoto & Fujiwara, Citation2009); (b) cover of ‘Visualizing atypical speech sound production – Using electropalatography’ (book with DVD; Yamamoto & Fujiwara, Citation2014); and (c) a sample page from the book.
Acrylic resin EPG plates usually cover the hard palate and the anterior section of the soft palate, but they do not extend over the teeth as metal clasps are used to hold them in place (see, ). Thermoformed plates are thin enough to extend over the teeth so metal clasps are not needed (see, ). Since the EPG plate is extended over the teeth, EPG electrodes can be positioned in the dental area to increase the coverage of the plate. This would address the criticism about the absence of dental articulatory zone in acrylic plates that has often been made (e.g. Fougeron et al., Citation2000; McLeod, Citation2006). However, increased EPG coverage of the plate is a controversial issue. Covering the upper incisors with thermoformed plate prevents air from passing through gaps between the teeth, which can influence linguo-dental and dental consonant productions (Wrench, Citation2007). An ideal solution for this problem is yet to be found. One possible solution would be to use an EPG plate with metal clasps and extend the front portion of the plate to cover the inner surface of the upper incisors, while also keeping the plate thin enough to avoid interference with anterior sibilant productions.
Wireless connectivity
As stated above, the wires connecting the electrodes and the multiplexer exit the mouth either at the sides or centrally. Both designs of wire positioning have their advantages and drawbacks. While ‘central position may not restrict lip rounding to the same degree as cables that exit from the sides of the mouth … the central leads may impede airflow if they are allowed to hang in front of the mouth’ (Wrench, Citation2007, p. 7). Replacing the leads with a wireless transmitter would address these issues, but the designers of the wireless EPG plate would have to deal with the problem of the power-source and transmitter placement within the plate or in the oral cavity. There are no such designs in use today for the conventional EPG systems, but the pressure-sensing EPG plate reported in Sardini et al. (Citation2014) and the Tongue Position Tracking Device (TPTD) developed by Pastore (Citation2018) (both described below) are wireless plates that use Bluetooth technology for signal transmission. There is also a new, wireless EPG system under development (see research project Smart Electropalatography for Linguistic and Medical Applications (SELMA) led by Yong-Kyu Yoon; Yoon, Citation2020–2023). The system is not commercially available yet and the exact specifications are still unavailable. But current patent descriptions suggest that the system should offer significantly thinner plate with wireless charging and connectivity.
Wireless connectivity of the EPG plate with the multiplexer unit would improve plate-wearing comfort and enhance the use of EPG in more natural communicative situations and in multimodal speech investigations. Advanced kinematic techniques have mostly been restricted to laboratories, where communicative situations often differ from those in everyday speech, which might result in differences in speech production (Koch, Citation2008; Liker, Citation2018). Therefore, researchers are often faced with a dilemma – to study speech in natural everyday communication where advanced instruments are often unavailable or to use advanced techniques to investigate speech processes in highly controlled but unnatural communicative situations provided by research laboratories. By removing the wired connection between the plate and the multiplexer/computer, clients would be less restricted by the equipment and would experience more communicative freedom, which in turn would result in more natural communicative situations. This might also enable researchers to find ways to include EPG in multimodal investigations of speech and language (e.g. Danner et al., Citation2018).
Sensing tongue pressure on the palate
The conventional EPG technique provides information of tongue palate contact patterns based on the presence/absence of contact at each electrode, whereas an EPG plate with pressure-sensing function gives information about the level of tongue pressure exerted to create those contact patterns. This technological feature would be particularly useful for studying articulation difficulties related to impaired speech motor control such as dysarthrias (Mirchandani et al., Citation2020; Murdoch et al., Citation2004). Another atypical articulatory feature that could be further investigated using a pressure-sensing EPG plate is the undifferentiated lingual gestures that have been reported in some children with speech sound disorders (Gibbon, Citation1999). The undifferentiated lingual gestures were inferred from the indistinctive tongue palate contact patterns for contrasting speech sounds. For example, the typical contact pattern of alveolar plosives is characterised by the presence of contact in the alveolar region (Row 1–2) across the palate and the sides of the palate, whereas the typical pattern of velar plosives is contact in the velar region (Row 6–8) (see, ). In undifferentiated lingual gestures, the speakers showed similar contact pattern for both alveolar and velar plosives (/t, d/ and /k, ɡ/), where the tongue contacted nearly the entire hard palate (Gibbon, Citation1999). In these cases, it would be useful to measure the amount of pressure exerted by the tongue on the different regions of the palate where presence of contact was detected. This is because the use of differential tongue pressure on different regions of the palate might indicate the speakers’ attempt to control the tongue in order to produce the appropriate tongue configuration for producing the target speech sound. This could be a positive prognostic factor for speech intervention.
There have already been some developments of a tongue pressure-sensing EPG plate by different research teams using different types of sensors (e.g. Baldoli et al., Citation2017; Hori et al., Citation2009; Matsumura et al., Citation2002; Mirchandani et al., Citation2020; Murdoch et al., Citation2004; Sardini et al., Citation2014; Tiede et al., Citation2003; Wakumoto et al., Citation1998; Woo et al., Citation2021; see, also for a summary). The most recent studies were by Baldoli et al. (Citation2017), Mirchandani et al. (Citation2020), and Woo et al. (Citation2021). Among the nine studies summarised in , the EPG plate reported in Baldoli et al. (Citation2017) had the highest number of pressure sensors which allowed detailed investigation of tongue pressure. It has 62 sensors made using piezoresistive fabrics that can be arranged in the same way as the Reading EPG plate described above. The EPG plate developed by Woo et al. (Citation2021) also used a relatively high number of pressure sensors: 36 electrodes, with six in the alveolar region, 22 in the palatal region (in five horizontal rows) and eight in the velar region (in three rows).
Table 1. Studies (the latest publications from the relevant research teams) on tongue pressure-sensing EPG plates.
In terms of how the tongue pressure data is displayed, most of the studies reported line graphs of tongue pressure level over time (see, also ). The most user-friendly format is probably the one shown in Woo et al. (Citation2021), where the contact patterns were shown in a similar way to the display of the CompleteSpeech system and the tongue pressure level at each electrode was indicated using four different colours: red for strong, yellow for medium, blue for weak, and white for no contact. For Baldoli et al. (Citation2017) and Matsumura et al. (Citation2002), the tongue pressure data were displayed in the format of a heat map, with red representing the highest level of pressure and blue representing the lowest level.
All the pressure-sensing EPG plates are still at the testing stage and have only been tested on small groups of typical speakers. In general, the findings were that the voiceless alveolar plosive /t/ had a higher tongue pressure level than the voiced cognate /d/ (Baldoli et al., Citation2017; Mirchandani et al., Citation2020; Tiede et al., Citation2003; Wakumoto et al., Citation1998), with maximum pressure exerted against the alveolar region of the palate (Baldoli et al., Citation2017; Matsumura et al., Citation2002). However, the pressure difference was not apparent between the voiceless and voiced velar plosives /k, ɡ/ (Mirchandani et al., Citation2020). In addition, the nasal alveolar plosive /n/ showed a lower tongue pressure than the voiceless and voiced oral alveolar plosives /t, d/ (Tiede et al., Citation2003). Further investigation of tongue pressure level during the production of consonants and vowels is warranted to advance our understanding of typical articulation.
Sensing tongue-palate distance
The principle of optical distance sensing has been applied in the development of an EPG plate that measures the distance between the tongue and the palate during speech (Chuang & Wang, Citation1978; Fletcher et al., Citation1989; Wagner et al., Citation2022; Wrench et al., Citation1996), hence the equipment is known as optopalatograph (OPG; or glossometer in Fletcher et al., Citation1989). The technique involves sensors that each consists of a light emitting diode (LED) and a photodiode. The LED radiates a light beam towards the surface of the tongue and the photodiode detects the proportion of light reflected back, inferring the distance between the tongue and the palate (Wagner et al., Citation2022; Wrench et al., Citation1996). Hence, the higher the level of sensor activation, the shorter the distance between the tongue and the plate. The prototype OPG reported in Wrench et al. (Citation1998) had 16 sensors arranged in a T-shape on the plate, with six along the midsagittal line and five on each side in the anterolateral region. In their paper, the authors showed the midsagittal and coronal tongue surface contours of an adult speaker during the production of a few phonemes (/t, k, i/) using nine of the sensors. The latest OPG device developed by the research team led by Birkholz was described in Wagner et al. (Citation2022). It had nine digital optical proximity sensors: five along the midsagittal line and two on each side around the postalveolar and palatal region. The sensors were embedded and connected on a flexible circuit board and this double cross-shaped device was placed on the hard palate using a biocompatible adhesive. The device is not personalised because a custom-made dental retainer is not required to fit it to the palate (Wagner et al., Citation2022). The device was used with 13 typical adults to measure their tongue movement trajectories during a number of non-speech and speech tasks. The speech tasks were production of the word ‘hawk’ and the palatal fricative /ç/. The results of the tongue movement trajectories over time were displayed in the form of a line graph and heatmap for each sensor. Distinctive patterns of data were observed for the different phonemes tested. For example, for /ç/, the activation level was the highest in the sensors in the palatal region, followed by those in the alveolar region, and it was the lowest in the sensor in the velar region. Whereas for /k/, the activation level was high in the four sensors at the back but low in the five sensors at the front (Wagner et al., Citation2022).
The TPTD is another tongue-palate distancing-sensing device (Pastore, Citation2018). It uses capacitive proximity sensing, where the distance between the sensor and the tongue is inferred from the capacitance in the electric field generated by the sensor. Capacitance is the measure of the capacity of an object (or a capacitor) in storing energy in the form of electric charge (Silman & Emmer, Citation2012). In the parallel plate capacitor formed by the sensor and the tongue, the capacitance is inversely proportional to the distance between the sensor and the tongue (Pastore, Citation2018). Hence, the capacitance increases when the distance between the sensor and the tongue decreases. A total of 12 sensors were used in TPTD, with two along the midsagittal line in the alveolar region and five on each side along the lateral dental arch, forming an inverted V-shape in the visual display of data. The technique was tested on six typical adults who produced 22 English phonemes (18 consonants and four vowels) in isolation 10 times. The tongue-palate distance information could be displayed using a mobile phone app, in the form of contact pattern with the capacitance value of each sensor shown according to a greyscale: black indicates contact and shades close to white indicate increased distance between the tongue and the palate. Characteristic patterns were reported for the different classes of phonemes. For example, there was an increased tongue-palate distance in all sensors for open vowels /ɑː, ɒ/, but a reduced distance or the presence of contact in all sensors for alveolar plosives /t, d, n/, affricate /tʃ/, and approximant /j/. A pattern of increased tongue-palate distance in the front sensors but presence of contact in the back sensors was observed in the velar plosives /k, ɡ/, labiodental fricative /f/, and approximant /ɹ/. For fricatives /s, ʃ, θ/, all sensors showed the presence of contact except the anterior medial sensor. The contact patterns reported generally agree with those reported in the EPG literature. However, perhaps due to the relatively lower number of sensors used, particularly in the alveolar region, some of the fine details of lingual articulation (e.g. the absence of contact in the anterior medial electrodes or the presence of a medial groove for alveolar and post-alveolar fricatives) that can be captured using the conventional EPG plates were not shown using the TPTD. Hence, one of the author’s suggestions for further improvement was to include more electrodes to ‘increase the spatial resolution’ (Pastore, Citation2018, p. 67).
Software packages
Software packages for EPG data collection and data analyses are sophisticated because they offer various options for data organisation and highly customisable data quantification procedures. Users can set up numerical indices for the quantification of various articulatory variables, such as amount of contact, amount of closure, and tongue palate contact asymmetry. Despite being sophisticated, EPG software packages have been optimised for a long time, so they are intuitive to use. Many of the well-documented data reduction indices are pre-configured and visualisations are provided in order to improve data interpretation. Although existing software packages are comprehensive and relatively easy to use, there are some areas of possible improvement. For example, three-dimensional (3D) plate mapping and the development of numerical indices which take into account differences in shapes and sizes of the individual palate could be useful tools for speech analysis. The artificial EPG plate closely follows the shape of the hard palate of each client, but during data processing, visualisation and analysis, the tongue palate contact is represented as a two-dimensional (2D) pattern, and individual differences in the palate shape are disregarded and normalised. Although there are many practical reasons for this normalisation, some research papers have shown that some individual differences in lingual articulation might be due to differences in the palate shapes and sizes (e.g. Hiki & Itoh, Citation1986). Therefore, 3D EPG plate mapping with numerical indices that take palate shapes into account could address these issues. There were several attempts to develop a 3D EPG software package (Chiu et al., Citation1995; Saw, Citation1993; Wakumoto & Masaki, Citation1999), but those software solutions were not widely used. Apart from phonetic research, 3D EPG could also prove useful in the field of articulatory synthesis for the development of advanced feedback systems, such as virtual speech and language teachers (e.g. Artur – The Articulation Tutor, Engwall, Citation2006) and for machine learning with the aim of automatic identification of atypical speech patterns. It remains to be seen whether these software advancements will generate enough demand so they can be implemented into mainstream EPG software packages.
Related tongue-palate devices
Although the primary application of EPG is within the fields of speech and phonetic sciences, the technique has been successfully used for other purposes as well. Advances in the area of human machine input (HMI) provide evidence that the human tongue can be used as an input device for personal computers (e.g. Andreasen Struijk et al., Citation2017; Draghici, Citation2014; Große & Birkholz, Citation2020; Huo et al., Citation2008). Using the tongue instead of hands to control computers is potentially useful for individuals with impaired limb control (e.g. tetraplegia) and in entertainment industry since the accuracy of such device can reach up to 88% of the regular computer joystick (Draghici, Citation2014). Horne and Kelly (Citation2015) modified a Reading-type EPG plate by reducing the number of tongue contact areas from 62 to 16 and the location of the tongue palate contact was then converted into a specific computer command. They showed that EPG can be a useful tool for controlling computers in patients with spinal cord injury. The authors measured the speed with which a user could hit a particular contact area on the EPG plate and showed that users could touch the target area within one second. They concluded that EPG provided a good foundation for the development of a completely new class of devices for aiding particular groups of users. These and other possible applications in the area of HMI might encourage further investments in the development of EPG technology. The integration of visual feedback, pressure-sensing, optical tongue distance sensing and wireless technology could enable such tongue-input systems to utilise different tongue-palate pressures to, for example, toggle between upper and lower case when selecting letters or to simulate single and double-click with a mouse by differences in tongue pressure or shape. Also, if a person can successfully control a computer via tongue-input, this feature can be utilised to control other computer-operated devices, such as wheelchairs.
EPG as a clinical tool
EPG has been used as a clinical tool for assessing and treating speech disorders. In terms of speech intervention, EPG provide clients with real-time visual information about their tongue palate contact patterns during speech (Michi et al., Citation1993). The external biofeedback and the clinician’s live demonstration of target contact pattern help the clients alter their lingual articulation in order to achieve correct production of the speech sounds (Gibbon & Wood, Citation2010). The concrete information about tongue placement also gives the clients an idea about their progress, which can motivate them to keep working on the treatment targets (Michi et al., Citation1993). In speech assessment, EPG allows an objective record as well as qualitative and quantitative measurements of articulatory behaviours (Michi et al., Citation1993). The assessment can also be carried out mid-way and post therapy to monitor the treatment progress and evaluate the final outcome as well as the maintenance of intervention effects (Gibbon & Wood, Citation2010; Michi et al., Citation1993; see also e.g. Darelid et al., Citation2016, for an example of assessment schedule in a single case study of EPG therapy for an adult with cochlear implant).
When using EPG in speech evaluation, the results from both auditory-perceptual judgment and EPG assessment are considered together to identify the speech sounds affected and the speech errors demonstrated. The extra information about contact patterns can supplement auditory-perceptual judgements to help clinicians gain a better insight into the nature of the articulation difficulties of the clients. This is crucial for establishing the prognosis of the clients and planning the intervention. For example, the demonstration of covert contrast has been reported in previous EPG studies (see, Gibbon & Lee, Citation2017, for a review). Covert contrast refers to phonological contrasts that a speaker attempts to make but which are not readily perceived by the listeners. The presence of covert contrast is considered as a positive sign because it indicates that the speakers have underlying knowledge about the sound contrast (Tyler et al., Citation1993). It has also been reported that children with covert contrast required fewer treatment sessions to achieve the treatment target than those without (Tyler et al., Citation1993). Hence, added information from EPG about subtle articulatory gestures (such as covert contrast) can help clinicians to make a better estimation of their clients’ prognosis for speech therapy.
EPG has probably been used most frequently with individuals with speech disorders associated with cleft palate (Gibbon & Paterson, Citation2006), followed by speech sound disorders of unknown origin, and those associated with (acquired and developmental) neurological impairments, hearing problems, and intellectual disabilities (e.g. Down syndrome; see e.g. the EPG bibliography by Gibbon, Citation2013). Hence, more progress in EPG assessment and treatment (and the investigation of EPG treatment efficacy) has been made in the area of cleft palate speech management (see, e.g. Gibbon et al., Citation2001; Lee et al., Citation2009; Lohmander et al., Citation2010). One innovation is the clinician-researcher collaboration in the provision of EPG treatment in the CLEFTNET projects (CLEFTNET Scotland in Gibbon et al., Citation1998; and CLEFTNET UK in Lee et al., Citation2007). In these initiatives, the clinicians identified clients who might benefit from EPG therapy, and they carried out speech assessment and treatment using EPG. The researchers provided initial training on using the equipment to the clinicians and supported their work with offline detailed analysis of their clients’ EPG data and treatment recommendations. There are also similar clinician-researcher collaborations in Japan where EPG data collected by clinicians or video-recordings of tongue-palate contact patterns made by caregivers of the clients were sent to researchers for analysis and feedback. There are advantages of this model of collaboration to both clinicians and researchers. The detailed data analysis and recommendations support the clinicians’ work, and the client data allows the researchers to further their investigations of atypical articulations. If this kind of collaboration model is to be used in future projects, careful planning of data transfer and storage would be necessary because of the increasing awareness and regulations regarding privacy and confidentiality of personal data.
Another relatively recent idea in speech therapy using EPG is the use of telepractice to deliver the service. Telepractice is the ‘application of telecommunications technology to the delivery of speech language pathology and audiology professional services at a distance by linking clinician to client or clinician to clinician for assessment, intervention, and/or consultation’ (CitationAmerican Speech-Language-Hearing Association [ASHA], n.d.). Clients who have mobility issues or live far away from the service provider can access speech and language therapy (SLT) services more easily and frequently using this service delivery method. Telepractice has been gradually expanding in the field of cleft palate speech management in recent years. For example, Shprintzen and Golding-Kushner (Citation2012) reported a Distance Care programme for international clients with velo-cardio-facial syndrome who required specialist care that was not readily available near them. Sweeney et al. (Citation2016) and Sweeney, Hegarty et al. (Citation2020) reported a feasibility study and a randomised controlled trial of a programme that trained parents of children with speech disorders associated with cleft palate to carry out speech training with their children at home with support from specialist SLTs through regular online meetings. The authors concluded that their programme ‘can be as effective as routine care in changing speech, activity and participation outcomes for children with cleft palate’ (Sweeney et al., Citation2020, p. 639).
For EPG therapy, Fujiwara (Citation2007) reported an intervention programme that used EPG portable training units (PTU; Articulate Instruments Ltd, Edinburgh, UK) with a group of clients with residual articulation errors associated with cleft palate. The PTU is a light-weight device that provides real-time visual display of tongue palate contact only using arrays of light-emitting diodes (Jones & Hardcastle, Citation1995). A PTU was lent to each client, and they were instructed to do home practice for 30 minutes each day using the device. The progress of each individual was monitored by the clinician through a monthly therapy session at the clinic, except for one client who had additional online therapy sessions once every week. Because the client had a PTU at home, the clinician could easily monitor the client’s tongue placement by viewing the PTU display, even during online sessions. For speech intervention programmes, such as those reviewed above (Fujiwara, Citation2007; Shprintzen & Golding-Kushner, Citation2012; Sweeney et al., Citation2020, Citation2016), at least one initial face-to-face evaluation was needed in order to get a clear picture of the speech difficulties and related issues of the clients. Recently, because of the COVID-19 pandemic and the corresponding measures on movement restrictions (particularly in 2020–2021), there was a reduction in the offer of face-to-face therapy sessions globally. In order to maintain SLT service to clients, there was a further increased implementation of telepractice (e.g. Fong et al., Citation2021; Kraljević et al., Citation2020). This was also the case for EPG therapy in Japan (Lee et al., Citation2022). It is possible that in the future, speech therapy via telepractice (or a blended face-to-face and online therapy model) may remain an option for clients because of its advantages and convenience over face-to-face therapy sessions.
EPG for teaching speech disorders and phonetics
Speech disorders and phonetics are two key components of SLT training, and phonetics is also a core element in the degree programmes of phonetics and linguistics. Conventionally, 2D mid-sagittal line-drawing diagrams of the vocal tract are the main materials for teaching articulatory phonetics (i.e. the ‘mechanics of speech production’, Knight & Whitworth, Citation2014, p. 3). The knowledge about articulatory gestures forms the basis for teaching topics such as phonological processes and atypical articulation errors associated with organic causes. Altogether, the knowledge is applied in the clinics in speech assessment, the results of which informs the choice of the treatment approach and the setting of treatment targets. However, the vocal tract is three-dimensional and the use of 2D diagrams for teaching speech sound production and errors could miss some important information about tongue configurations and placement in the transverse plane. McLeod (Citation2011, p. 1010) reported that the SLTs who took part in their study showed ‘good knowledge of tongue/palate contact along the midline (sagittal plane), but poor knowledge of contact along lateral margins of the palate’. Particularly, they showed ‘limited awareness of the extent (breadth) of contact for alveolar consonants /t, d, n, l/ and velar consonants /k, ɡ, ŋ/; lateral bracing for alveolar consonants /t, d, n, s, z/; the groove for sibilants /s, z, ʃ, ʒ/; and posterior lateral contact for many other consonants /b, v, θ, ð, w/’ (McLeod, Citation2011, p. 1010). Hence, the author pointed out the need of including information of lingual articulation from different views in SLT education. This can be achieved using live EPG demonstration (if the educators already have their own EPG plate and have access to an EPG system) or recorded video clips of dynamic EPG frames. The educators can use EPG (or the PTU) to show the tongue palate contact pattern of different speech sounds in typical articulation. They can also simulate speech errors to show students how the errors occur as a result of atypical lingual gestures.
There is a substantial body of written resources on typical and atypical lingual articulation in the literature that educators can draw on. An EPG bibliography managed by Gibbon (Citation2013) is available on the website of Articulate instruments Ltd. The bibliography lists EPG articles related to the description of different EPG systems, EPG studies in English published between 1957 and 2012, and clinical applications of EPG. EPG studies of typical lingual articulation of various languages are available (see the bibliography). The resource book by McLeod and Singh (Citation2009) provides tongue palate contact patterns for all English consonants and monophthongs of a typical English-speaking adult. For atypical articulation, a good start is to consult review articles on atypical tongue palate contact patterns, which are available for the following clinical groups or articulatory phenomena: speech sound disorders of unknown origin (Gibbon, Citation1999) and cleft palate (Gibbon, Citation2004; Gibbon & Lee, Citation2010; Lee et al., Citation2019); and covert contrast (Gibbon & Lee, Citation2017) and residual speech errors (Gibbon & Lee, Citation2015). For teaching the use of EPG in treatment, a number of recent papers and book chapters might be of use: Lee et al. (Citation2007), Gibbon and Wood (Citation2010), Gibbon and Lee (Citation2011), and Lee et al. (Citation2019), and Cleland and Preston (Citation2021). The chapter by Lee et al. (Citation2019) comes with a video clip of EPG therapy.
There are also published video resources on tongue palate contact patterns that can be used for teaching. Yamamoto and Fujiwara (Citation2009) produced a DVD entitled ‘Visualizing Japanese speech sounds production – Using electropalatography’ (see ). The contents include (1) an explanation of the processes of speech production: respiration, phonation, resonation, and articulation, (2) an introduction to EPG, and (3) dynamic EPG patterns of Japanese consonants in consonant-vowel syllabic structure and special segments: the mora nasal, gemination, and vowel length. Aside from EPG data, it also contains nasoendoscopic and videofluoroscopic recordings of speech production. The DVD has been widely used by educators of SLT programmes in Japan to help students understand the speech production mechanism. The same authors also published a book entitled ‘Visualizing atypical speech sound production – Using electropalatography’ (Yamamoto & Fujiwara, Citation2014; see ). The book contains illustrations of data analysis (including waveform display, spectrogram, and dynamic tongue palate contact patterns) using the Articulate Assistant software of WinEPGTM (Articulate Instruments Ltd., Edinburgh, UK) for each target speech sound. It comes with video clips of tongue palate contact patterns, lip movement, mirror test, and nasopharyngoscopic exams of speakers with speech errors including palatalisation, retracted alveolar sounds, lateralisation, and nasopharyngeal articulation. Whether it is typical or atypical, speech production involves movement of internal anatomical structures. By integrating the different information from combined evaluation methods using EPG, nasoendoscopy, and videofluoroscopy, students can gain a more comprehensive understanding of atypical speech sound production.
Conclusion
This paper presents the state of the art of EPG and discusses possible directions for further development of the technique and application of EPG in research, clinical management of speech disorders, and teaching of speech disorders and phonetics. While applying innovative technologies to advance the EPG hardware and software is important, broadening the manufacturing network and shortening the EPG production time are also crucial for ensuring the research and clinical viability of using EPG. EPG is an invaluable tool for studying articulation and despite the recent increase of popularity of other instrumental techniques, there is still a place for EPG in speech research and therapy.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- American Speech-Language-Hearing Association. (n.d.). Telepractice. https://www.asha.org/practice-portal/professional-issues/telepractice/
- Andreasen Struijk, L. N. S., Lontis, E. R., Gaihede, M., Caltenco, H. A., Lund, M. E., Schioeler, H., & Bentsen, B. (2017). Development and functional demonstration of a wireless intraoral inductive tongue computer interface for severely disabled persons. Disability and Rehabilitation: Assistive Technology, 12(6), 631–640. http://dx.doi.org/10.1080/17483107.2016.1217084
- Articulate Instruments Ltd. (2013). A history of EPG. http://www.articulateinstruments.com/a-history-of-epg/
- Baldoli, I., Maselli, M., Manti, M., Surace, E., Cianchetti, M., & Laschi, C. (2017). A pressure-sensitive palatograph for speech analysis. Proceedings of the 39th annual international conference of the IEEE engineering in medicine and biology society (pp. 4431–4434). https://doi.org/10.1109/EMBC.2017.8037839
- Chiu, W. S., Shadle, C. H., & Carter, J. N. (1995). Quantitative measures of the palate using enhanced electropalatography. European Journal of Disorders of Communication, 30(2), 149–160. https://doi.org/10.3109/13682829509082526
- Chuang, C.-K., & Wang, W. S.-Y. (1978). Use of optical distance sensing to track tongue motion. Journal of Speech & Hearing Research, 21(3), 482–496. https://doi.org/10.1044/jshr.2103.482
- Cleland, J., & Preston, J. L. (2021). Biofeedback interventions. In A. L. Williams, S. McLeod, & R. J. McCauley (Eds.), Interventions for speech sound disorders in children (2nd ed., pp. 573–600). Paul H. Brookes Publishing Co.
- Danner, S. G., Barbosa, A. V., & Goldstein, L. (2018). Quantitative analysis of multimodal speech data. Journal of Phonetics, 71, 268–283. https://doi.org/10.1016/j.wocn.2018.09.007
- Darelid, M. Ö., Hartelius, L., & Lohmander, A. (2016). Generalised EPG treatment effect in a cochlear implant user maintained after 2 years. International Journal of Speech-Language Pathology, 18(1), 65–76. https://doi.org/10.3109/17549507.2015.1048827
- Draghici, O. I. (2014). The MouthPad – A tongue interface for hands-free computer control [Doctoral dissertation]. University of Ottawa. https://ruor.uottawa.ca/bitstream/10393/31855/3/Draghici_Ovidiu_2014_thesis.pdf
- Engwall, O. (2006). Feedback strategies of human and virtual tutors in pronunciation training. TMH-QPSR, 48(1), 11–34. https://www.speech.kth.se/prod/publications/files/qpsr/2006/2006_48_1_011-034.pdf
- Fabus, R., Raphael, L., Gatzonis, S., Dondorf, K., Giardina, K., Cron, S., & Badke, B. (2015). Preliminary case studies investigating the use of electropalatography (EPG) manufactured by CompleteSpeech® as a biofeedback tool in intervention. International Journal of Linguistics and Communication, 3(1), 11–23. https://doi.org/10.15640/ijlc.v3n1a3
- Fletcher, S. G., McCutcheon, M. J., Smith, S. C., & Smith, W. H. (1989). Glossometric measurements in vowel production and modification. Clinical Linguistics & Phonetics, 3(4), 359–375. https://doi.org/10.3109/02699208908985296
- Fletcher, S. G. (1992). Articulation: A physiological approach. Singular Publishing Group Inc.
- Fong, R., Tsai, C. F., & Yiu, O. Y. (2021). The implementation of telepractice in speech language pathology in Hong Kong during the COVID-19 pandemic. Telemedicine Journal and E-Health, 27(1), 30–38. https://doi.org/10.1089/tmj.2020.0223
- Fougeron, C., Menadier, Y., & Demoulin, D. (2000). 62 vs. 96 electrodes: A comparative analysis of reading and kay elemetrics EPG pseudo-palates. Seminar on speech production: Models and data – CREST workshop on models on speech production: Motor planning and articulatory modelling (pp. 1–4). https://hal.archives-ouvertes.fr/hal-00244496/document
- Fujiwara, Y. (2007). Electropalatography home training using a portable training unit for Japanese children with cleft palate. Advances in Speech-Language Pathology, 9(1), 65–72. https://doi.org/10.1080/14417040601120904
- Gibbon, F. E., Crampin, L., Hardcastle, B., Nairn, M., Razzell, R., Harvey, L., & Reynolds, B. (1998). CleftNet (Scotland): A network for the treatment of cleft palate speech using EPG. International Journal of Language & Communication Disorders, 33(Suppl. 1), 44–49. https://doi.org/10.3109/13682829809179393
- Gibbon, F. E., & Nicolaidis, K. (1999). Palatography. In W. J. Hardcastle & N. Hewlet (Eds.), Coarticulation: Theory, data and techniques (pp. 229–245). Cambridge University Press.
- Gibbon, F. E. (1999). Undifferentiated lingual gestures in children with articulation/phonological disorders. Journal of Speech, Language, and Hearing Research, 42(2), 382–397. https://doi.org/10.1044/jslhr.4202.382
- Gibbon, F. E., & Crampin, L. (2001). An electropalatographic investigation of middorsum palatal stops in an adult with repaired cleft palate. The Cleft Palate-Craniofacial Journal, 38(2), 96–105. https://doi.org/10.1597/1545-1569_2001_038_0096_aeiomp_2.0.co_2
- Gibbon, F. E., Hardcastle, W. J., Crampin, L., Reynolds, B., Razzell, R., & Wilson, J. (2001). Visual feedback therapy using electropalatography (EPG) for articulation disorders associated with cleft palate. Asia Pacific Journal of Speech, Language and Hearing, 6(1), 53–58. https://doi.org/10.1179/136132801805576798
- Gibbon, F. E. (2004). Abnormal patterns of tongue-palate contact in the speech of individuals with cleft palate. Clinical Linguistics & Phonetics, 18(4–5), 285–311. https://doi.org/10.1080/02699200410001663362
- Gibbon, F. E., & Paterson, L. (2006). A survey of speech and language therapists’ views on electropalatography therapy outcomes in Scotland. Child Language Teaching and Therapy, 22(3), 275–292. https://doi.org/10.1191/0265659006ct308xx
- Gibbon, F. E., & Lee, A. (2010). Producing turbulent speech sounds in the context of cleft palate. In S. Fuchs, M. Toda, & M. Żygis (Eds.), Turbulent sounds: An interdisciplinary guide (pp. 303–341). de Gruyter.
- Gibbon, F. E., & Wood, S. E. (2010). Visual feedback therapy with electropalatography. In A. L. Williams, S. McLeod, & R. J. McCauley (Eds.), Interventions for speech sound disorders in children (pp. 509–536). Paul H. Brookes Publishing Co.
- Gibbon, F. E., & Lee, A. (2011). Articulation – Instruments for research and clinical practice. In S. Howard & A. Lohmander (Eds.), Cleft palate speech: Assessment and intervention (pp. 221–238). Wiley-Blackwell.
- Gibbon, F. E. (2013). Bibliography of electropalatographic (EPG) studies in English (1957-2013). Articulate Instruments Ltd. http://www.articulateinstruments.com/EPGrefs.pdf
- Gibbon, F. E., & Lee, A. (2015). Electropalatography (EPG) for older children and adults with residual speech errors. Seminars in Speech and Language, 36(4), 271–282. https://doi.org/10.1055/s-0035-1562910
- Gibbon, F. E., & Lee, A. (2017). Electropalatographic (EPG) evidence of covert contrasts in disordered speech. Clinical Linguistics & Phonetics, 31(1), 4–20. https://doi.org/10.1080/02699206.2016.1174739
- Große, K., & Birkholz, P. (2020). Tongue mouse – Comparison of physical measurement principles. In A. Wendemuth, R. Böck, & I. Siegert (Eds.), Studientexte zur Sprachkommunikation: Elektronische Sprachsignalverarbeitung 2020 (pp. 34–43). TUDpress.
- Hardcastle, W. J., Jones, W., Knight, C., Trudgeon, A., & Calder, G. (1989). New developments in electropalatography: A state-of-the-art report. Clinical Linguistics & Phonetics, 3(1), 1–38. https://doi.org/10.3109/02699208908985268
- Hardcastle, W. J., Gibbon, F., & Nicolaidis, K. (1991). EPG data reduction methods and their implications for studies of lingual coarticulation. Journal of Phonetics, 19(3–4), 251–266. https://doi.org/10.1016/S0095-4470(19)30343-2
- Hardcastle, W. J., Gibbon, F. E., & Jones, W. (1991). Visual display of tongue-palate contact: Electropalatography in the assessment and remediation of speech disorders. British Journal of Disorders of Communication, 26(1), 41–74. https://doi.org/10.3109/13682829109011992
- Hiki, S., & Itoh, H. (1986). Influence of palate shape on lingual articulation. Speech Communication, 5(2), 141–158. https://doi.org/10.1016/0167-6393(86)90004-X
- Hori, K., Ono, T., Tamine, K.-I., Kondo, J., Hamanaka, S., Maeda, Y., Dong, J., & Hatsuda, M. (2009). Newly developed sensor sheet for measuring tongue pressure during swallowing. Journal of Prosthodontic Research, 53(1), 28–32. https://doi.org/10.1016/j.jpor.2008.08.008
- Horne, R. J., & Kelly, S. W. (2015). Electropalatography as a human input device for patients suffering from spinal cord injuries. Proceedings of the IET international conference on Technologies for Active and Assisted Living (TechAAL) (pp. 1–4). https://doi.org/10.1049/ic.2015.0141
- Huo, X., Wang, J., & Ghovanloo, M. (2008). A magneto-inductive sensor based wireless tongue-computer interface. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 16(5), 497–504. doi: 10.1109/TNSRE.2008.2003375
- Jones, W., & Hardcastle, W. J. (1995). New developments in EPG3 software. European Journal of Disorders of Communication, 30(2), 183–192. https://doi.org/10.3109/13682829509082529
- Knight, R.-A., & Whitworth, N. (2014). Introduction. In N. Whitworth & R.-A. Knight (Eds.), Methods in teaching clinical phonetics and linguistics (pp. 1–22). J&R Press.
- Koch, K. A. (2008). Spontaneous speech, lab speech, and effects on intonation: Some useful findings for fieldworkers (and laboratory phonologists). Proceedings of the 2008 annual conference of the Canadian linguistic association (pp. 1–14). http://homes.chass.utoronto.ca/~cla-acl/actes2008/CLA2008_Koch.pdf
- Kochetov, A. (2020). Research methods in articulatory phonetics I: Introduction and studying oral gestures. Language and Linguistics Compass, 14(4), e12368. https://doi.org/10.1111/lnc3.12368
- Kraljević, J. K., Matić, A., & Dokoza, K. P. (2020). Telepractice as a reaction to the COVID-19 crisis: Insights from Croatian SLP settings. International Journal of Telerehabilitation, 12(2), 93–104. https://doi.org/10.5195/ijt.2020.6325
- Ladefoged, P., & Maddieson, I. (1996). The sounds of the world’s languages. Wiley-Blackwell.
- Ladefoged, P. (2003). Phonetic data analysis: An introduction to fieldwork and instrumental techniques. Blackwell Publishing.
- Lee, A., Gibbon, F. E., Crampin, L., Yuen, I., & McLennan, G. (2007). The national CLEFTNET project for individuals with speech disorders associated with cleft palate. Advances in Speech-Language Pathology, 9(1), 57–64. https://doi.org/10.1080/14417040601001997
- Lee, A., Law, J., & Gibbon, F. E. (2009). Electropalatography for articulation disorders associated with cleft palate. Cochrane Database of Systematic Reviews, 2009( Issue 3), Art. No.: CD006854. https://doi.org/10.1002/14651858.CD006854.pub2
- Lee, A., Harding-Bell, A., & Gibbon, F. E. (2019). Diagnosis and intervention for cleft palate speech using electropalatography (EPG). In A. Harding-Bell (Ed.), Case studies in cleft palate speech: Data analysis and principled intervention (pp. 299–325). J&R Press Ltd.
- Lee, A. (2019). Electropalatography. In J. S. Damico & M. J. Ball (Eds.), The SAGE encyclopedia of human communication sciences and disorders (pp. 679–680). SAGE Publications, Inc.
- Lee, A. (2021). Electropalatography. In M. J. Ball (Ed.), Manual of clinical phonetics (pp. 339–353). Routledge.
- Lee, A., Fujiwara, Y., Liker, M., Yamamoto, I., Takei, Y., & Gibbon, F. (2022). EPG activities in Japan and the impact of COVID-19 pandemic on EPG research and therapy: A report of presentations at the 7th EPG Symposium. International Journal of Language & Communication Disorders. Advance online publication. https://doi.org/10.1111/1460-6984.12720
- Liker, M. (2018). Electropalatographic analysis of vowels in quasi-spontaneous speech: A preliminary investigation. The Phonetician, 115, 5–22. http://isphs.org/Phonetician/ThePhonetician115_2018.pdf
- Lohmander, A., Henriksson, C., & Havstam, C. (2010). Electropalatography in home training of retracted articulation in a Swedish child with cleft palate: Effect on articulation pattern and speech. International Journal of Speech-Language Pathology, 12(6), 483–496. https://doi.org/10.3109/17549501003782397
- Matsumura, M., Yamasaki, H., Tsuji, R., Niikawa, T., Hara, H., Tachimura, T., & Wada, T. (2002). Measurement of palatolingual contact pressure and tongue force using a force-sensor mounted on a palatal plate. Biomechanisms, 16(1), 75–85. https://doi.org/10.3951/biomechanisms.16.75
- McAuliffe, M. J., Lin, E., Robb, M. P., & Murdoch, B. E. (2008). Influence of a standard electropalatography artificial palate upon articulation. Folia Phoniatrica Et Logopaedica, 60(1), 45–53. https://doi.org/10.1159/000112216
- McLeod, S., & Searl, J. (2006). Adaptation to an electropalatograph palate: Acoustic, impressionistic, and perceptual data. American Journal of Speech-Language Pathology, 15(2), 192–206. https://doi.org/10.1044/1058-0360(2006/018)
- McLeod, S. (2006). Australian adults’ production of /n/: An EPG investigation. Clinical Linguistics & Phonetics, 20(2–3), 99–107. https://doi.org/10.1080/02699200400026496
- McLeod, S., & Singh, S. (2009). Speech sounds: A pictorial guide to typical and atypical speech. Plural Publishing Inc.
- McLeod, S. (2011). Speech-language pathologists’ knowledge of tongue/palate contact for consonants. Clinical Linguistics & Phonetics, 25(11–12), 1004–1013. https://doi.org/10.3109/02699206.2011.620678
- Michi, K., Yamashita, Y., Imai, S., Suzuki, N., & Yoshida, H. (1993). Role of visual feedback treatment for defective /s/ sounds in patients with cleft palate. Journal of Speech, Language, and Hearing Research, 36(2), 277–285. https://doi.org/10.1044/jshr.3602.277
- Mirchandani, B., Perrier, P., Grosgogeat, B., & Jeannin, C. (2020). Study of tongue-palate pressure patterns during the hold phase in the production of French dentialveolar and velar stops. Clinical Linguistics & Phonetics, 34(1–2), 54–71. https://doi.org/10.1080/02699206.2019.1610978
- Murdoch, B. E., Goozée, J. V., Veidt, M., Scott, D. H., & Meyers, I. A. (2004). Introducing the pressure-sensing palatograph – The next frontier in electropalatography. Clinical Linguistics & Phonetics, 18(6–8), 433–445. https://doi.org/10.1080/02699200410001703628
- Pastore, G. (2018). Tongue Position Tracking Device (TPTD): A discreet wireless electropalatography and glossometry device [Doctoral dissertation]. University of Illinois at Chicago.
- Sardini, E., Serpelloni, M., & Pandini, S. (2014). Analysis of tongue pressure sensor for biomedical applications. Proceedings of the 2014 IEEE international symposium on Medical Measurements and Applications (MeMeA) (pp. 1–5). https://doi.org/10.1109/MeMeA.2014.6860031
- Saw, C. C. (1993). Customized 3-D electropalatography display. UCLA Working Papers in Phonetics, 85, 71–96. https://escholarship.org/content/qt5jn7b0m3/qt5jn7b0m3.pdf?t=krno1m
- Scobbie, J. M., Wood, S. E., & Wrench, A. A. (2004). Advances in EPG for treatment and research: An illustrative case study. Clinical Linguistics & Phonetics, 18(6–8), 373–389. https://doi.org/10.1080/02699200410001703682
- Searl, J., Evitts, P., & Davis, W. J. (2006). Perceptual and acoustic evidence of speaker adaptation to a thin pseudopalate. Logopedics Phoniatrics Vocology, 31(3), 107–116. https://doi.org/10.1080/14015430500390961
- Shprintzen, R. J., & Golding-Kushner, K. J. (2012). The international use of telepractice. Perspectives on Telepractice, 2(1), 16–25. https://doi.org/10.1044/tele2.1.16
- Silman, S., & Emmer, M. B. (2012). Instrumentation for audiology and hearing science: Theory and practice. Plural Publishing Inc.
- Stone, M. (1997). Laboratory techniques for investigating speech articulation. In W. J. Hardcastle & J. Laver (Eds.), Handbook of phonetic sciences (pp. 28–31). Wiley-Blackwell.
- Sweeney, T., Sell, D., & Hegarty, F. (2016). Parent-led articulation therapy in cleft palate speech: A feasibility study. Journal of Clinical Speech and Language Studies, 23(1), 21–41. https://doi.org/10.3233/ACS-2017-23105
- Sweeney, T., Hegarty, F., Powell, K., Deasy, L., O’Regan, M., & Sell, D. (2020). Randomized controlled trial comparing Parent Led Therapist Supervised Articulation Therapy (PLAT) with routine intervention for children with speech disorders associated with cleft palate. International Journal of Language & Communication Disorders, 55(5), 639–660. https://doi.org/10.1111/1460-6984.12542
- Tiede, M., Perkell, J., Zandipour, M., Matthies, M., & Stockmann, E. (2003). A new approach to pressure-sensitive palatography using a capacitive sensing device. In M. J. Solé, D. Recasens, & J. Romero (Eds.), Proceedings of the 15th International Congress of Phonetic Sciences (ICPhS) (pp. 3149–3152). Causal Productions.
- Tyler, A. A., Figurski, G. R., & Langsdale, T. (1993). Relationships between acoustically determined knowledge of stop place and voicing contrasts and phonological treatment progress. Journal of Speech & Hearing Research, 36(4), 746–759. https://doi.org/10.1044/jshr.3604.746
- Wagner, C., Stappenbeck, L., Wenzel, H., Steiner, P., Lehnert, B., & Birkholz, P. (2022). Evaluation of a non-personalized optopalatographic device for prospective use in functional post-stroke dysphagia therapy. Journal of IEEE Transactions on Biomedical Engineering, 69(1), 356–365. https://doi.org/10.1109/TBME.2021.3094415
- Wakumoto, M., Masaki, S., Honda, K., & Ohue, T. (1998). A pressure sensitive palatography: Application of new pressure sensitive sheet for measuring tongue-palatal contact pressure. Proceedings of the 5th International Conference on Spoken Language Processing (ICSLP98). https://www.isca-speech.org/archive/pdfs/icslp_1998/wakumoto98_icslp.pdf
- Wakumoto, M., & Masaki, S. (1999). Three-Dimensional visualisation of electropalatographic data. The Journal of the Acoustical Society of Japan, 20(2), 137–141. https://doi.org/10.1250/ast.20.137
- Woo, S.-T., Ha, J.-W., Na, S., Choi, H., & Pyun, S.-B. (2021). Design and evaluation of Korean Electropalatography (K-EPG). Sensors, 21(11), 3802. https://doi.org/10.3390/s21113802
- Wrench, A. A., McIntosh, A. D., & Hardcastle, W. J. (1996). Optopalatograph: A new apparatus for speech production analysis. Proceedings of the 4th International Conference on Spoken Language Processing (ICSLP96). https://www.isca-speech.org/archive/icslp_1996/wrench96_icslp.html
- Wrench, A. A., McIntosh, A. D., Watson, C., & Hardcastle, W. J. (1998). Optopalatograph: Real-time feedback of tongue movement in 3D. Proceedings of the 5th International Conference on Spoken Language Processing (ICSLP98). https://www.isca-speech.org/archive/pdfs/icslp_1998/wrench98_icslp.pdf
- Wrench, A. A. (2007). Advances in EPG palate design. Advances in Speech-Language Pathology, 9(1), 3–12. https://doi.org/10.1080/14417040601123676
- Yamamoto, I., & Fujiwara, Y. (2009). Visualizing Japanese speech sounds production – Using electropalatography [DVD]. EPG Study Group. https://epg-research.sakura.ne.jp/category/item
- Yamamoto, I., & Fujiwara, Y. (2014). Visualizing atypical speech sound production – Using electropalatography. EPG Study Group. https://epg-research.sakura.ne.jp/category/item
- Yoon, Y.-K., (Principal Investigator). (2020-2023). SenSE: Smart Electropalatography for Linguistic and Medical Applications (SELMA) [Grant]. National Science Foundation. https://www.nsf.gov/awardsearch/showAward?AWD_ID=2037266
- Zin, S. M., Md Rasib, S. Z., Suhaimi, F. M., & Mariatti, M. (2021). The technology of tongue and hard palate contact detection: A review. BioMedical Engineering Online, 20(1), 17. https://doi.org/10.1186/s12938-021-00854-y