
ABSTRACT
The problem in language comprehension in people with right hemisphere damage (RHD) is more equivocal than people with left hemisphere damage. This study explores the reading and listening comprehension of Cantonese-speaking individuals with RHD, left hemisphere damage, and neurotypical healthy controls using the Cantonese Computerized Revised Token Test (CRTT-Cantonese) adapted from the English CRTT. Eighteen native Cantonese-speaking individuals with RHD, 32 individuals with left hemisphere damage and aphasia (PWA), and 42 healthy controls participated in this study. All the participants completed the Cantonese Aphasia Battery, Hong Kong Oxford Cognitive Screen, the listening comprehension version of CRTT-Cantonese (CRTT-L-Cantonese), and the reading comprehension version of CRTT-Cantonese (CRTT-R-WF-Cantonese) across different sessions. Linear mixed-effect analysis revealed significant differences among the groups in CRTT-Cantonese tests. However, there were no significant difference between CRTT-L-Cantonese and CRTT-R-WF-Cantonese within the PWA, RHD and healthy control groups. Tukey post-hoc pairwise comparisons showed that PWA scored significantly lower than RHD and healthy control groups (p < 0.0001) in both CRTT-L-Cantonese and CRTT-R-WF-Cantonese, and the RHD group scored significantly lower than healthy control group only on the CRTT-R-WF-Cantonese. The results demonstrate that the CRTT-L-Cantonese and CRTT-R-WF-Cantonese differentiate language comprehension abilities among PWA, RHD and healthy control groups. Although the current findings did not show any diversion between reading and listening comprehension in RHD group, this group showed poorer performance in reading comprehension when compared to healthy controls. The latter findings may support the view that the right hemisphere contributes to reading comprehension in Chinese.
Introduction
The left hemisphere is well-understood for its major role in language processing for majority of the right-handed people (Brownell et al., Citation1983; Buchweitz et al., Citation2009). However, the role of the right hemisphere in language processing and/or comprehension is less unequivocal. Some earlier studies reported that people with right hemisphere damage (RHD) have subtle deficits in comprehension of narrative stories and conversation (Jung-Beeman, Citation2005; Taylor & Regard, Citation2003). However, others reported that individuals with RHD had normal performance in comprehension of both stated information and implied intention of the stories when measured using a discourse comprehension test (Brady et al., Citation2006). Recent studies have reported language comprehension (i.e. auditory sentence to picture matching) deficits only among a subgroup of people with RHD (13%), especially when the lesion affects the right inferior frontal sulcus (Gajardo-Vidal et al., Citation2018). Furthermore, it has been shown that the activation of right hemisphere (i.e. right temporal lobe) contributes to the recovery of language comprehension in people with left hemisphere damage (Crinion & Price, Citation2005), suggesting that right hemisphere might have role in language processing following stroke. However, the most consistent findings across behavioural and neuroimaging studies of both neuropathological and neurotypical brain are that the right hemisphere is more engaged in coarser or higher-level language processing while the left hemisphere is more engaged with literal language processing (Blake, Citation2018; Brownell et al., Citation1983; Jung-Beeman, Citation2005; Weylman et al., Citation1989). Damage to the left hemisphere leads more commonly (than damage to the right hemisphere) to aphasia, which refers to difficulties using linguistic symbols across different modalities, i.e. listening, reading, speaking and writing, and across different linguistic domains, i.e. lexico-semantics, syntax and phonology (McNeil & Pratt, Citation2001). The diagnosis of aphasia encompasses the exclusion of any other sensory, motor, psychiatric and primary cognitive deficits, though they accompany aphasia frequently.
Neuroimaging studies that compared listening and reading comprehension of healthy participants have suggested reading comprehension is subserved with more left-lateralised neural network than listening comprehension, especially in western languages (Buchweitz et al., Citation2009). However, it has been suggested that individual differences might also play a role as readers with lower working memory capacities were shown to recruit more homologous right hemisphere area than people with higher working memory skills (Buchweitz et al., Citation2009; Prat et al., Citation2007). On the other hand, neuroimaging studies conducted on Chinese reading have suggested additional right lateralisation of visual systems including the lingual gyrus and fusiform gyrus (Tan et al., Citation2000; Tan, Feng, et al., Citation2001; Tan, Liu, et al., Citation2001). It has been argued that the right hemisphere seems to be functionally dominant in certain language processing such as pictographic reading, as in reading Japanese Kanji and Chinese characters (Taylor & Regard, Citation2003). The left visual field-right hemisphere was found to perform better in reading pictographic stimuli such as logos or kanji characters than the right visual field-left hemisphere in split visual field experiments (Taylor & Regard, Citation2003; Tzeng et al., Citation1979). Unlike most of the alphabetic languages that have a linear arrangement of letters, Chinese characters belong to a logographic system, in which a character is formed by a number of strokes that are packed into a square shape. Some studies have suggested strong activation in the right occipital cortex that contributes to spatial recognition of visual symbols was also observed during processing of Chinese characters (Clark et al., Citation1996; Shen et al., Citation1999). Therefore, it seems that more right hemisphere cortical regions were involved in Chinese reading relative to that of English reading, attributed to its square-shaped logograph which requires more extensive analysis of spatial information and various strokes forming the characters (Tan et al., Citation2000; Tan, Feng, et al., Citation2001; Tan, Liu, et al., Citation2001).
One way to behaviourally examine involvement of the right hemisphere in Chinese reading versus listening comprehension is to compare the performance of people with RHD to people with left hemisphere damage (LHD) and neurologically healthy participants using assessment tests that have identical linguistic stimuli, scoring and response requirements across the reading and listening modalities. However, existing studies that examined Chinese reading comprehension at the lexical-semantic and syntactic levels are mainly limited to normal participants (Kuo et al., Citation2004; Tan et al., Citation2000; Tan, Feng, et al., Citation2001; Tan, Liu, et al., Citation2001) and people with aphasia (PWA) (Law & Leung, Citation1998, Citation2000). Furthermore, the widely used existing language assessment tool in Cantonese, i.e. the Cantonese Aphasia Battery (CAB, Yiu, Citation1992) is not suitable for examination of modality differences between reading and listening comprehension because the linguistic stimuli used across its reading and listening comprehension subtests are not adequately matched, which may result in an invalid comparison of language comprehension across different modalities. Although the CAB has been reported as a valid assessment for Chinese-speaking PWA with high test-retest reliability (.95–1.00), high inter-rater (.88–1.00) and intra-rater (.82–1.00) reliability for most of its subtests (Yiu, Citation1992), normative data have not been developed for its reading subtest and its validity in differentiating reading performance of brain damaged people and healthy individuals is unknown.
Conversely, the Cantonese version of the Computerized Revised Token Test (CRTT-Cantonese) developed by Bakhtiar et al. (Citation2020) is a suitable behavioural assessment tool for examination of modality differences in reading and listening comprehension. The CRTT-Cantonese used matched stimuli across the reading and listening comprehension versions for examination of sentence comprehension in PWA. The CRTT-Cantonese was developed based on the Computerised Revised Token Test (CRTT) (McNeil et al., Citation2015), which is a computerised version of the Revised Token Test (RTT) developed by McNeil and Prescott (Citation1978). The reading version of the CRTT-Cantonese (CRTT-R-WF-Cantonese) uses standard Chinese in traditional scripts while the listening version of the CRTT-Cantonese (CRTT-L-Cantonese) uses formal Cantonese to ensure the stimuli are culturally appropriate and linguistically natural (Bakhtiar et al., Citation2020). The presentation of stimuli in the CRTT-R-WF-Cantonese is self-paced word-by-word sentence assembly, with each previous word disappearing with the onset of the next word. This presentation has similar effects as the serial word presentation in the CRTT-L-Cantonese, with both requiring comparable cognitive-motor demands, equivalent response demands, and identical multidimensional scoring conventions, and hence allowing a more direct comparison across modalities than other standardised aphasia and general language tests (Bakhtiar et al., Citation2020; McNeil et al., Citation2015). Each CRTT-Cantonese test consists of 10 subtests, in which each subtest contains 10 homogeneous commands to allow for the well-documented moment-to-moment variability in people with aphasia, and to reliably capture their average performance. The test stimuli are identical across the reading and listening subtests and well controlled in terms of syntactic structures and linguistics units. The target lexical items are limited to five colours, two shapes and two sizes to avoid or minimise the potential linguistic biases that may be influenced by age, gender, intellectual, and cultural issues (Bakhtiar et al., Citation2020; McNeil et al., Citation2015). It has been reported that the CRTT-Cantonese tests significantly differentiate reading and listening comprehension of PWAs from healthy individuals and has high test-retest reliability (ranging from .82–.96) (Bakhtiar et al., Citation2020).
To date, there is insufficient evidence to profile the fundamental listening and reading language abilities of Cantonese speakers with RHD. It is the purpose of this study to shed light to the existing limited and controversial research findings related to language comprehension capabilities of people with RHD. Furthermore, the examination of listening and reading comprehension of the Cantonese speakers with RHD versus LHD will shed light on the role of the right hemisphere in Chinese reading. Therefore, this study aims to profile the reading and listening comprehension of people with RHD as compared to the LHD people with aphasia (PWA), and neurotypical healthy controls (HC) using the CRTT-Cantonese tests. Our hypotheses are that (a) there will be significant differences among the RHD, PWA and HC groups on the overall scores in both CRTT-R-WF-Cantonese and CRTT-L-Cantonese. Consistent with the findings of the original non-computerised English Revised Token Test, we predict that the PWA would have poorest performance followed by the RHD and HC (McNeil & Prescott, Citation1978), and (b) the RHD participants will have poorer performance in reading comprehension than listening comprehension, since reading in Chinese characters would be more depending on the recruitment of neural resources of the right hemisphere.
Methods
Participant
A total of 92 participants have been included in this study: 42 HCs (14 females and 28 males, mean age: 58.59 years, range: 43–76 years old, SD = 7.97), 32 PWAs (10 females and 22 males, mean age: 58.78 years, range: 46–72 years, SD = 6.31), and 18 RHDs (6 females and 12 males, mean age: 60.39 years, range: 40–76 years old, SD = 8.48).Footnote1 The proportion of gender distribution across the three groups were nearly identical (~1/3 females and 2/3 males). Furthermore, there were no significant group differences in terms of the age (F(2, 89) = .38, p = 0.68), or education level (F(2, 89) = .63, p = 0.54). The demographic information of the participants is displayed in . All the participants were native Cantonese speakers with at least 6 years of formal education and had no premorbid history of speech, language, hearing, cognitive and/or psychiatric disorders. The participants were recruited through promotions at different community groups, support groups, as well as social media.
Table 1. Demographic details and clinical information of the healthy controls (HC), participants with right hemisphere brain damage (RHD) and participants with left hemisphere brain damage with aphasia (PWA) based on the Cantonese Aphasia Battery (CAB).
The participants with a history of left hemisphere stroke and aphasia quotient (AQ) score below 96.4 based on the CAB were assigned to the PWA group. Whereas the participants with a history of right hemisphere stroke and did not fit the profile of aphasia based on the CAB were assigned to the RHD group (see ). If left or right hemiparesis was present, it was a sign consistent with right or left hemisphere unilateral stroke. Participants were excluded from the study who demonstrated (1) a visual acuity lower than 20/40 for either eye [based on the Snellen chart (Azzam & Ronquillo, Citation2022) or Near Vision Test]; (2) a pure tone hearing threshold at any single frequency that was higher than 50 dB at 500 Hz, 1000 Hz, 2000 Hz and 4000 Hz in either ear; (3) a major cognitive impairment (except for aphasia in the PWA group) as indicated using the Hong Kong version of the Oxford Cognitive Screen (HK-OCS, Kong et al., Citation2016), a valid tool for cognitive assessment of Cantonese-speaking adults post-stroke with excellent intra-rater, inter-rater reliability and fair test-retest reliability for most of its subtests (ranging from .90–1.00, .59–1.00, and .31–.99, respectively); (4) insufficient knowledge and perceptual skills on the target lexical items (i.e. colour, shape, size); and (5) insufficient hand motor abilities to perform the CRTT tasks as determined by the CRTT pre-tests. Additionally, any PWAs and RHDs with a poststroke onset time of less than 4 months were excluded from the study. The Mann – Whitney U test showed that the PWA and RHD groups had nonsignificantly different poststroke onset time (U = 258, p = 0.54). Furthermore, any PWAs with a diagnosis of global aphasia were also excluded from the study. The study was approved by the Human Subject Ethics Committee of the Hong Kong Polytechnic University (Reference number: HSEARS20171228002). All the participants gave their written consent before their participation in the study.
Procedure
All participants completed the screening tests (i.e. visual and auditory screenings, HK-OCS, CAB and CRTT-Cantonese pre-tests) to determine their eligibility before implementation of the CRTT-L-Cantonese and CRTT-R-WF-Cantonese for examination of their sentence comprehension. Participants were randomly assigned to start with either the CRTT-L-Cantonese, followed by the CRTT-R-WF-Cantonese in the next session or the reverse order, with a time interval of approximately one week. The screening tests and CRTT-Cantonese tests were conducted by two final-year master students of speech therapy under supervision of two experience qualified speech therapists in a sound-proof room at the Hong Kong Polytechnic University. Since the CRTT-Cantonese tests are a fully computerised and self-administered program, a minimal training is sufficient for successful operation and data collection. The screening tests and one of the CRTT-Cantonese tests (i.e. CRTT-L-Cantonese, or CRTT-R-WF-Cantonese) were conducted on the first session, which took between 90 and 120 mins. The other CRTT-Cantonese test (i.e. CRTT-R-WF-Cantonese, or CRTT-L-Cantonese) was conducted on the second session, which took between 30 and 60 mins.
A laptop computer with a 14-inch diagonal screen (Lenovo, Think-Pad TP470) connected to a standard mouse was used to administer the CRTT-Cantonese tests. The height of the laptop was adjusted using a computer stand to ensure the monitor was located at the eye level with a 16-inch distance from the participant. The auditory stimuli were presented through the laptop speaker at a comfortable intensity level. The PWA and RHD participants used their intact hand (i.e. left hand for the PWA and right hand for the RHD) to respond to the stimuli while the HC participants were asked to use their nondominant hand (i.e. left hand) to perform the tests. The participants’ performance was recorded by the CRTT-Cantonese tests and the overall and efficiency scores were automatically computed. The overall CRTT score is derived from the average of the 580, 15-point multidimensionally assigned scores that are automatically produced for each part of speech (with exception the definite articles which are unscored) in each of the 100 sentences in the test. illustrates the scoring convention for part of a single subtest taken from simulated performance from an English CRTT-L test. The details on computation of the overall scores can be found in Bakhtiar et al. (Citation2020) and McNeil et al. (Citation2015). For the purpose of this study, only the overall scores of the CRTT-Cantonese tests will be used for further analyses.
Figure 1. The scoring convention for part of a single subtest taken from simulated performance from an English CRTT-L test.
Data analysis
One-way ANOVAs were used to compare the demographic information of the participants including the age and education level, and also their performance on the screening tests including the CAB and subtest scores of HK-OCS across different groups. Linear mixed-effect (LME) modelling was used to analyse the overall scores of the CRTT-Cantonese tests. LME is a robust statistical analysis that has become increasingly popular in psycholinguistics and allows modelling of the fixed effects as well as random effects, which increase the generalisability and allow population-level inferences (Baayen et al., Citation2008). For the analysis of the CRTT-Cantonese scores, LME analysis was constructed to compare the language comprehension of the three groups (PWA, RHD and HC) across two different modalities (reading, listening). It has been suggested to include all random effects justified by the design in the LME model (Barr, Citation2013). Therefore, a maximal model was fitted including the above variables and their interactions (i.e. groups × modalities) as the fixed factors, and the random factors including the random intercepts of the participants and subtests, and also the random effects of modalities for participants. The inclusion of the random effect of groups for subtests resulted in convergence errors. Furthermore, the random effects of groups for participants and modalities for subtests are meaningless, as each participant belongs to one group only and each subtest belongs to each modality. Thus, the final random effects model, expressed in {lme4}. syntax, was (Modality | Participants) + (1 | Subtests).
A Pearson correlation coefficient was computed between CRTT-L-Cantonese and CRTT-R-WF-Cantonese for each of the three groups in order to determine the degree of association of language comprehension between the listening and reading modalities.
Results
Screening tests
A one-way ANOVA revealed significant differences in CAB-AQ scores across the groups (F(2, 89) = 81.4, p < 0.001). The post hoc analysis using Tukey multiple pairwise-comparisons revealed lower CAB-AQ scores in the PWA (M = 82.60, SD = 10.11) compared to the HC (M = 99.50, SD = .63) and RHD (M = 99.10, SD = 1.18) groups (ps < .001). No significant difference was found between the HC and RHD groups (p = 0.97). The performance of the HC, PWA, and RHD groups on the HK-OCS and their group differences are displayed in . For the HK-OCS scores, the three groups showed non-significantly different performance across HK-OCS subtests except for the sentence reading (F(2, 89) = 8.01, p < 0.001), number writing (F(2, 89) = 11.94, p < 0.001), episodic memory (F(2, 89) = 3.83, p < 0.05), and broken hearts (F(2, 89) = 4.62, p < 0.05). For the sentence reading subtest, the PWA group (M = 19.25, SD = 3.81) scored significantly lower than the HC (M = 21.24, SD = .98) and RHD (M = 21.50, SD = .79) groups. Similarly, for the number writing subtest, the PWA group (M = 2.06, SD = 1.10) scored significantly lower than the HC (M = 2.83, SD = .37) and RHD (M = 2.83, SD = .38) groups. However, for the episodic memory subtest, the RHD group (M = 3.56, SD = .51) scored significantly lower than the HC (M = 3.88, SD = .33) and PWA (M = 3.69, SD = .53) groups. Furthermore, the RHD group (M = 45.11, SD = 6.50) scored significantly lower on the broken hearts subtest compared to the HC (M = 48.38, SD = 1.87) and PWA (M = 48.09, SD = 2.01) groups.
Table 2. The performance of the HC, PWA and RHD groups on the Hong Kong version of the Oxford Cognitive Screen (HK-OCS).
CRTT-Cantonese tests
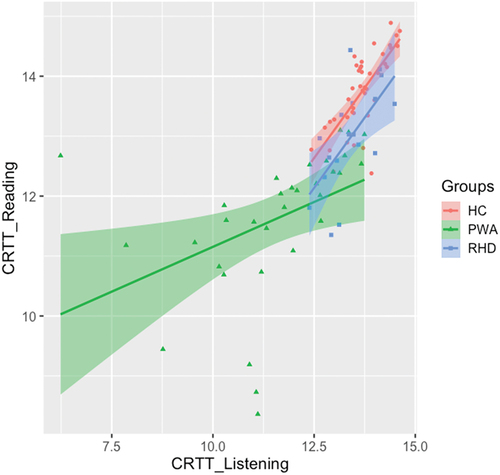
The results of the CRTT-L-Cantonese and CRTT-R-WF-Cantonese across the participant groups are displayed in . In order to compare the listening and reading comprehension abilities/deficits across the three groups, LME analysis was conducted across the participant groups (HC, PWA and RHD) and CRTT modalities (reading, listening). The findings revealed a significant effect of groups (χ2 = 79.95, p < 0.0001), but no significant effect of modalities (χ2 = .02, p = 0.88) or overall interaction between group and modality (χ2 = 3.40, p = 0.18). Post hoc pairwise comparison (using lsmeans package) with Tukey adjustment found that the PWA group showed significantly lower performance than both the HC and RHD groups in both reading and listening modalities (ps < .001). However, the RHD group, when compared with the HC group, showed significantly lower performance only in the reading modality (p < 0.01) while no between group differences were found in the listening modality (p = 0.57). Furthermore, significant positive correlations were found in the overall scores between modalities for each group: HC (r = .73, p < 0.0001), PWA (r = .42, p < 0.05) and RHD (r = .64, p < 0.05) (see ).
Figure 2. CRTT-Cantonese scores for the HC, PWA and RHD groups across listening (L) and reading (R) modalities.
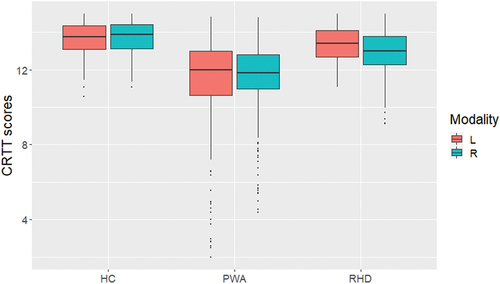
Figure 3. Relationships between CRTT-L-Cantonese and CRTT-R-WF-Cantonese scores for the HC, PWA and RHD groups.
Discussion
Results of the CRTT-Cantonese tests found that the RHD group had significantly better performance in listening and reading comprehension than the PWA group. However, when compared to the HC group, the RHD group showed comparable listening comprehension and poorer reading comprehension. The results of this study is consistent with those of McNeil and Prescott (Citation1978) when they examined the HC, PWA and RHD groups using the non-computerised listening Revised Token Test and found significant differences among the three groups of participants. Their HC group had the best performance, followed by the RHD group, then the PWA group. On the contrary, we did not find significant difference in CRTT-listening between RHD and HC, which also does not support some of the earlier studies reporting impaired auditory comprehension in people with RHD (Jung-Beeman, Citation2005; Taylor & Regard, Citation2003). It is notable that in this study we used LME modelling for analysis of the data, which account for random variations imposed by the natural heterogeneity of the research participants, often ignored when analysing the averaged data (Baayen, Citation2008). We believe our analysis, which is based on LME modelling, offers more robust and reliable results as compared to the previous studies using more traditional analyses (Baayen et al., Citation2008).
The overall performance of the RHD group is found to be significantly better than the PWA group when examined using the CRTT-Cantonese tests. Different behavioural studies showed that RHD individuals have more problems in comprehension of nonliteral than literal language such as understanding jokes, indirect requests and metaphors (Blake, Citation2018; Brownell et al., Citation1983; Weylman et al., Citation1989). This has been supported by multiple neuroimaging studies reporting higher activation of the right hemisphere compared to the left hemisphere when the healthy participants are engaged in higher-level language processing tasks such as comprehension of the metaphors, inferred meanings, humours or jokes (Diaz & Eppes, Citation2018; Jung-Beeman, Citation2005; Yang, Citation2014) and information that involves distant semantic relations (Bookheimer, Citation2002; Démonet et al., Citation2005; Humphries et al., Citation2001; Xu et al., Citation2005). However, the commands included in the CRTT-Cantonese tests involve simple and compound imperative, prepositional and adverbial clause sentences with adjectival padding. They were designed and are more challenging for the PWA than for the RHD group. Additionally, a closer look at shows that individual differences among participants in the RHD group is smaller than those observed in the PWA group. The comparison of overall performance and individual differences between the PWA and RHD groups suggests that language comprehension deficit in the RHD group is more subtle or less severe, with less between subject variability. This leads to the question of whether the difference is one of severity or underlying impairment (Rivers & Love, Citation1980). We speculate that the nature of the impairments between PWA and RHD individuals is different. It is yet unclear whether the demands of the CRTT tasks reveal a shared impairment of the cognitive underpinnings for their language impairments, relative to HC performance. The linguistic stimuli used are the same for both CRTT-Cantonese tests, and the two tests differed primarily in their input modality, in which the stimuli in the CRTT-R-WF-Cantonese were presented visually in orthographic forms while the stimuli in the CRTT-L-Cantonese were presented auditorily in phonological forms. As the RHD participants in this study were not different from the healthy controls on the CRTT-L-Cantonese listening task but did perform significantly more poorly on the CRTT-R-WF-Cantonese reading task, it argues that the difference between the two pathological groups is not due to the nature of the linguistic demands per se or due to the nature of the language processing attributed to the damaged hemispheres between the two groups (e.g. figurative vs literal). That is, the CRTT tasks do not make demands on figurative language, although it does require the differential perception and comprehension of colours, shapes and sizes of the response stimuli. The lack of listening impairment for the RHD group also argues against a linguistic deficit as a source of their reading impairment. This leads to the speculation that higher-level visual-spatial processing needed in logographic reading in Chinese characters is the source of impairment for the RHD reading deficit which has been suggested to involve the right hemisphere (Tan et al., Citation2000; Tan, Feng, et al., Citation2001; Tan, Liu, et al., Citation2001).
One may argue that comparisons with people with RHD and a diagnosis of aphasia are needed for drawing conclusions regarding the nature of the language impairment in the RHD group as compared to LHD group as well as about language processing in general. However, all the participants with RHD recruited in the current study had a stroke in the right hemisphere and were diagnosed to be non-aphasic according to the CAB. All were self-reported to be right-handed. Research also showed that crossed aphasia (i.e. aphasia following a right hemisphere damage in right-handed individuals) is rare with an estimated prevalence below 3% (Coppens et al., Citation2002).
The findings on language performance documented with the CRTT-Cantonese tests are somewhat different from the CAB results in which nonsignificant different language performance was reported between the HC and RHD groups while the PWA group performed significantly more poorly than the HC and RHD groups. It is notable that CAB does not incorporate the reading scores in the calculation of the overall AQ scores (Yiu, Citation1992). This finding suggests that the CRTT-Cantonese tests are more sensitive than the CAB, an aphasia test, in differentiating the subtle language differences across the modalities between the PWA and RHD groups.
While data on the exact lesion site of the RHD participants were not available to this study, overall, the behavioural findings suggest that right hemisphere damage may compromise Chinese reading comprehension ability in people with RHD to a certain extent, but it is insufficient to differentiate the RHD performance in reading and listening modalities. While these participants did not demonstrate a significant differential impairment between the CRTT modality tests, their performance was poorer on the reading test than the listening test, the lack of significance of which may be accounted for by a reduced statistical power attributed to the small sample size. Although the RHD group in this study showed the largest effect size (.39) in terms of the modality differences compared to other groups (HC = −.08, PWA = −.05), the rather smaller sample size (n = 18), may explain the lack of significant difference between the reading and listening comprehension among this group. A post hoc power analysis, using an alpha level of .05, revealed an achieved power of .48, which is below the traditionally acceptable level of .80, with the current sample size and with an effect size of .39. Further study with a larger sample size of approximately 42 RHD participants is recommended to further examine the language comprehension abilities of the RHD participants with the CRTT tests.
This study has several limitations and issues remain to be further investigated. The inclusion of people with RHD and aphasia will further elucidate the nature of language processing in the left versus right hemispheres. Heterogeneity in the RHD population has been reported (Blake, Citation2018); thus, a closer look at the individual data may provide more insights into the language deficits of different individuals with RHD. Additionally, the interpretation of behavioural findings will benefit from data on the exact lesion sites of the participants, especially for the RHD group, which was not available in this study. Future studies are recommended to include brain imaging for examination of brain network connectivity during reading and listening comprehension to shed lights on the role of the right hemisphere in Chinese language reading comprehension. While the significant difference in CRTT-R-WF-Cantonese performance between the HC and RHD groups is not explained by the RHD group small sample, a larger sample size is clearly needed to achieve the power to detect a difference between the modalities for the RHD group.
Conclusion
This study documented significant differences in reading and listening comprehension abilities among the PWA, RHD and HC groups using the CRTT-Cantonese tests. As expected by theory and experimental precedence, the PWA group had significantly poorer performance in listening and reading comprehension than the HC and RHD groups. Although the current study did not find a significant difference between reading and listening comprehension in the RHD group, nor between the HC and RHD groups for listening, the RHD group did demonstrate poorer performance in reading comprehension when compared to the HC group. The role of the right hemisphere in Chinese reading comprehension remains a candidate for explaining this finding; however, it is still unclear if other factors can better explain these findings. Additional research is needed to unravel the various cognitive and neurological factors that will eventually shed light on this important theoretical and clinical issue. Overall the findings confirm that the language comprehension measured by the CRTT is more impaired in the LHD group with aphasia than RHD and HC groups. This study also confirms that the CRTT-Cantonese tests showed sufficient sensitivity to differentiate levels of performance across different modalities among HC, PWA and RHD.
Acknowledgments
The authors would like to thank all the participants for their involvement in this study and acknowledge Emily Ka Yin Tsui and Winni Hoi Wai Wong for their help in data collection. The contents of this article do not represent the views of the Department of Veterans Affairs or the U.S. Government.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes
1 The HC and PWA groups’ data have been published previously in Bakhtiar et al. (Citation2020) and are included as comparison groups to assess the performance of RHD group in listening and reading comprehension.
References
- Azzam, D., & Ronquillo, Y. (2022). Snellen chart. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK558961/
- Baayen, R. H. (2008). Analyzing linguistic data: A practical introduction to statistics using R. Cambridge University Press. https://doi.org/10.1017/CBO9780511801686
- Baayen, R. H., Davidson, D. J., & Bates, D. M. (2008). Mixed-effects modeling with crossed random effects for subjects and items. Journal of Memory and Language, 59(4), 390–412. https://doi.org/10.1016/j.jml.2007.12.005
- Bakhtiar, M., Wong, M. N., Tsui, E. K. Y., & McNeil, M. R. (2020). Development of the English listening and reading computerized revised token test into Cantonese: Validity, reliability, and sensitivity/specificity in people with aphasia and healthy controls. Journal of Speech, Language, and Hearing Research, 63(11), 3743–3759. https://doi.org/10.1044/2020_JSLHR-20-00103
- Barr, D. (2013). Random effects structure for testing interactions in linear mixed-effects models. Frontiers in Psychology, 4, 328. https://doi.org/10.3389/fpsyg.2013.00328
- Blake, M. L. (2018). The right hemisphere and disorders of cognition and communication: Theory and clinical practice. Plural Publishing Inc.
- Bookheimer, S. (2002). Functional MRI of language: New approaches to understanding the cortical organization of semantic processing. Annual Review of Neuroscience, 25(1), 151–188. https://doi.org/10.1146/annurev.neuro.25.112701.142946
- Brady, M., Armstrong, L., & Mackenzie, C. (2006). An examination over time of language and discourse production abilities following right hemisphere brain damage. Journal of Neurolinguistics, 19(4), 291–310. https://doi.org/10.1016/j.jneuroling.2005.12.001
- Brownell, H. H., Michel, D., Powelson, J., & Gardner, H. (1983). Surprise but not coherence: Sensitivity to verbal humor in right-hemisphere patients. Brain and Language, 18(1), 20–27. https://doi.org/10.1016/0093-934X(83)90002-0
- Buchweitz, A., Mason, R. A., Tomitch, L. M., & Just, M. A. (2009). Brain activation for reading and listening comprehension: An fMRI study of modality effects and individual differences in language comprehension. Psychology & Neuroscience, 2(2), 111–123. https://doi.org/10.3922/j.psns.2009.2.003
- Clark, V. P., Keil, K., Maisog, J. M., Courtney, S., Ungerleider, L. G., & Haxby, J. V. (1996). Functional magnetic resonance imaging of human visual cortex during face matching: A comparison with positron emission tomography. Neuroimage, 4(1), 1–15. https://doi.org/10.1006/nimg.1996.0025
- Coppens, P., Hungerford, S., Yamaguchi, S., & Yamadori, A. (2002). Crossed aphasia: An analysis of the symptoms, their frequency, and a comparison with left-hemisphere aphasia symptomatology. Brain and Language, 83(3), 425–463. https://doi.org/10.1016/S0093-934X(02)00510-2
- Crinion, J., & Price, C. J. (2005). Right anterior superior temporal activation predicts auditory sentence comprehension following aphasic stroke. Brain, 128(12), 2858–2871. https://doi.org/10.1093/brain/awh659
- Démonet, J. F., Thierry, G., & Cardebat, D. (2005). Renewal of the neurophysiology of language: Functional neuroimaging. Physiology Reviews, 85(1), 49–95. https://doi.org/10.1152/physrev.00049.2003
- Diaz, M. T., & Eppes, A. (2018). Factors influencing right hemisphere engagement during metaphor comprehension. Frontiers in Psychology, 9. https://doi.org/10.3389/fpsyg.2018.00414
- Gajardo-Vidal, A., Lorca-Puls, D. L., Hope, T. M. H., Parker Jones, O., Seghier, M. L., Prejawa, S., Crinion, J. T., Leff, A. P., Green, D. W., & Price, C. J. (2018). How right hemisphere damage after stroke can impair speech comprehension. Brain, 141(12), 3389–3404. https://doi.org/10.1093/brain/awy270
- Humphries, C., Willard, K., Buchsbaum, B., & Hickok, G. (2001). Role of anterior temporal cortex in auditory sentence comprehension: An fMRI study. Neuroreport, 12(8), 1749–1752. https://doi.org/10.1097/00001756-200106130-00046
- Jung-Beeman, M. (2005). Bilateral brain processes for comprehending natural language. Trends in Cognitive Sciences, 9(11), 512–518. https://doi.org/10.1016/j.tics.2005.09.009
- Kong, A.P. -H., Lam, P.H. -P., Ho, D.W. -L., Lau, J. K., Humphreys, G. W., Riddoch, J., & Weekes, B. (2016). The Hong Kong version of the Oxford Cognitive Screen (HK-OCS): Validation study for Cantonese-speaking chronic stroke survivors. Aging, Neuropsychology, and Cognition, 23(5), 530–548. https://doi.org/10.1080/13825585.2015.1127321
- Kuo, W. -J., Yeh, T. -C., Lee, J. -R., Chen, L. -F., Lee, P. -L., Chen, S. -S., Ho, L. -T., Hung, D. L., Tzeng, O. J. L., & Hsieh, J. -C. (2004). Orthographic and phonological processing of Chinese characters: An fMRI study. Neuroimage, 21(4), 1721–1731. https://doi.org/10.1016/j.neuroimage.2003.12.007
- Law, S. -P., & Leung, M. -T. (1998). Sentence comprehension in Cantonese Chinese aphasic patients. Aphasiology, 12(1), 49–63. https://doi.org/10.1080/02687039808249443
- Law, S. -P., & Leung, M. -T. (2000). Sentence processing deficits in two Cantonese aphasic patients. Brain and Language, 72(3), 310–342. https://doi.org/10.1006/brln.2000.2298
- McNeil, M. R., & Pratt, S. R. (2001). Defining aphasia: Some theoretical and clinical implications of operating from a formal definition. Aphasiology, 15(10–11), 901–911. https://doi.org/10.1080/02687040143000276
- McNeil, M. R., Pratt, S. R., Szuminsky, N., Sung, J. E., Fossett, T. R. D., Fassbinder, W., & Lim, K. Y. (2015). Reliability and validity of the computerized revised token test: Comparison of reading and listening versions in persons with and without aphasia. Journal of Speech, Language, and Hearing Research, 58(2), 311–324. https://doi.org/10.1044/2015_JSLHR-L-13-0030
- McNeil, M. R., & Prescott, T. (1978). Revised token test. PRO-ED.
- Prat, C. S., Keller, T. A., & Just, M. A. (2007). Individual differences in sentence comprehension: A functional magnetic resonance imaging investigation of syntactic and lexical processing demands. Journal of cognitive neuroscience, 19(12), 1950–1963. https://doi.org/10.1162/jocn.2007.19.12.1950
- Rivers, D. L., & Love, R. J. (1980). Language performance on visual processing tasks in right hemisphere lesion cases. Brain and Language, 10(2), 348–366. https://doi.org/10.1016/0093-934x(80)90061-9
- Shen, L., Hu, X., Yacoub, E., & Ugurbil, K. (1999). Neural correlates of visual form and visual spatial processing. Human brain mapping, 8(1), 60–71. doi:https://doi.org/10.1002/(SICI)1097-0193(1999)8:1<60:AID-HBM5>3.0.CO;2-6
- Tan, L. H., Feng, C. M., Fox, P. T., & Gao, J. H. (2001). An fMRI study with written Chinese. Neuroreport, 12(1), 83–88. https://doi.org/10.1097/00001756-200101220-00024
- Tan, L. H., Liu, H. L., Perfetti, C. A., Spinks, J. A., Fox, P. T., & Gao, J. H. (2001). The neural system underlying Chinese logograph reading. Neuroimage, 13(5), 836–846. https://doi.org/10.1006/nimg.2001.0749
- Tan, L. H., Spinks, J. A., Gao, J. H., Liu, H. L., Perfetti, C. A., Xiong, J., Stofer, K. A., Pu, Y., Liu, Y., & Fox, P. T. (2000, May). Brain activation in the processing of Chinese characters and words: A functional MRI study. Human brain mapping, 10(1), 16–27. doi:https://doi.org/10.1002/(SICI)1097-0193(200005)10:1<16:AID-HBM30>3.0.CO;2-M
- Taylor, K. I., & Regard, M. (2003). Language in the right cerebral hemisphere: Contributions from reading studies. Physiology, 18(6), 257–261. https://doi.org/10.1152/nips.01454.2003
- Tzeng, O. J., Hung, D. L., Cotton, B., & Wang, W. S. Y. (1979). Visual interalisation effect in reading Chinese characters. Nature, 282(5738), 499–501. https://doi.org/10.1038/282499a0
- Weylman, S. T., Brownell, H. H., Roman, M., & Gardner, H. (1989). Appreciation of indirect requests by left- and right-brain-damaged patients: The effects of verbal context and conventionality of wording. Brain and Language, 36(4), 580–591. https://doi.org/10.1016/0093-934X(89)90087-4
- Xu, J., Kemeny, S., Park, G., Frattali, C., & Braun, A. (2005). Language in context: Emergent features of word, sentence, and narrative comprehension. Neuroimage, 25(3), 1002–1015. https://doi.org/10.1016/j.neuroimage.2004.12.013
- Yang, J. (2014). The role of the right hemisphere in metaphor comprehension: A meta-analysis of functional magnetic resonance imaging studies. Human brain mapping, 35(1), 107–122. https://doi.org/10.1002/hbm.22160
- Yiu, E. M. L. (1992). Linguistic assessment of Chinese-speaking aphasics: Development of a Cantonese aphasia battery. Journal of Neurolinguistics, 7(4), 379–424. https://doi.org/10.1016/0911-6044(92)90025-R