
ABSTRACT
Social anxiety may disrupt the empathic process, and well-regulated empathy is critical for navigating the social world. Two studies aimed to further understand empathy in the context of social anxiety. Study 1 compared individuals with elevated or normative social anxiety on a measure assessing cognitive and affective empathy for positive and negative emotions conveyed by other people (“targets”), completed under social threat. Relative to individuals with normative social anxiety, individuals with elevated social anxiety had greater cognitive empathy and no differences in affective empathy, regardless of emotion type. As greater cognitive empathy can be maladaptive, Study 2 tested whether this could be down-regulated. Individuals with elevated social anxiety underwent emotional working memory training (eWMT) for negative emotional information, or control training (CT). Effects on an empathy measure completed under social threat were assessed. Cognitive empathy for negative emotions decreased following eWMT but not CT, and this was only evident for those with higher pre-training working memory capacity. Cognitive empathy for positive emotions and affective empathy were not affected. Overall, social anxiety is associated with aberrant elevated cognitive empathy for negative and positive emotions, and the deviation in cognitive empathy for negative emotions can be regulated with eWMT for certain individuals.
Trial registration: Australian New Zealand Clinical Trials Registry identifier: ACTRN12618001196235..
Social anxiety exists on a continuum and individuals with elevated social anxiety on the higher end of this continuum can experience significant individual burden (Fehm et al., Citation2008), with some meeting diagnostic criteria for social anxiety disorder (SAD; American Psychiatric Association, Citation2022). Individuals with elevated social anxiety are characterised by concerns about being evaluated by others and significant anxiety in relation to social-evaluative situations. According to psychological models of social anxiety (Clark & Wells, Citation1995; Heimberg et al., Citation2010; for a review, see Wong & Rapee, Citation2016), such anxiety can disrupt social abilities, leading to social performance deficits and actual negative evaluation from others. One important social ability is empathy, a process that has cognitive and emotional aspects which allows an individual to know another person’s emotional state (cognitive empathy) and share their emotional state (affective empathy). Empathy, when it is well-regulated, is considered fundamental to interpersonal functioning and navigating social interactions, while empathy at extreme levels can be maladaptive (Tone & Tully, Citation2014). A growing body of research has examined empathy in the context of social anxiety, although continued research is needed to further understand the relationship between these constructs, and how empathy might be optimised in individuals with elevated social anxiety.
From a theoretical perspective, psychological models of social anxiety (e.g. Clark & Wells, Citation1995) describe the cognitive and behavioural processes that maintain social anxiety. Based on these models, social anxiety that is experienced in social situations that are perceived to be threatening may interfere with empathic ability by disrupting normal empathic processes which then reduces one’s capacity to be empathic (interference hypothesis). However, an alternative to this can also be derived from models of social anxiety. With the perception of social threat, elevated social anxiety is associated with hypervigilance to evaluation from others (e.g. Heimberg et al., Citation2010). Although hypervigilance is considered a maintaining process of social anxiety, this process of increased attention to others may also lead to increased sensitivity to the thoughts and feelings of others, and enhance empathic ability (enhancement hypothesis; see also Tibi-Elhanany & Shamay-Tsoory, Citation2011).
From an empirical perspective, there are mixed findings with regard to social anxiety and its relationship with cognitive and affective empathy, with notable differences between studies for example in sample type (e.g. SAD versus undiagnosed socially anxious) and methodology (e.g. use of self-report trait empathy measures where participant completes a questionnaire on empathy, versus more dynamic measures of empathy where a participant watches a video of a target person and provides single ratings or continuous ratings of the perceived emotion of the target). Notably, a recent systematic review and meta-analysis attempted to integrate these findings, and found overall a positive association between social anxiety and affective empathy but no association between social anxiety and cognitive empathy (Pittelkow et al., Citation2021). There were also two points in Pittelkow et al. (Citation2021) that were particularly relevant to the present studies. First, only a very small number of studies have used more dynamic measures to assess cognitive and affective empathy (i.e. Auyeung & Alden, Citation2016, Citation2020; Morrison et al., Citation2016), and these studies have not consistently examined these empathy types for both positive and negative emotions. Second, only a very small number of studies have examined the presence of social threat (i.e. Auyeung & Alden, Citation2016, Citation2020), which is important for the activation of social anxiety according to psychological models (e.g. Clark & Wells, Citation1995). We will now focus on the identified studies given their relevance to the present studies.
In relation to cognitive empathy for negative emotions, there has been mixed findings amongst the identified studies. Auyeung and Alden (Citation2016) in a cross-sectional study of unselected undergraduates found elevated social anxiety was associated with better cognitive empathy for negative emotions related to exclusion experiences of targets but only in the presence of social threat (i.e. participants informed that they would be watched by experimenters). Auyeung and Alden (Citation2020) reported two other cross-sectional studies with similar methodology (one with an unselected undergraduate sample; one with a sample of individuals with SAD) and found the same positive relationship such that higher levels of social anxiety and SAD were both associated with better cognitive empathy for negative emotions related to exclusion experiences of targets, irrespective of the presence of a social exclusion manipulation. In contrast, Morrison et al. (Citation2016) in a cross-sectional study of SAD found no difference in cognitive empathy for negative emotions related to personal events of targets between individuals with SAD and healthy controls. In relation to cognitive empathy for positive emotions, there has been more consistent findings. The aforementioned study of undergraduates did not find an association between social anxiety and cognitive empathy for positive emotions related to inclusion experiences of targets (regardless of presence of social threat; Auyeung & Alden, Citation2016), and the aforementioned study of SAD found no difference in cognitive empathy for positive emotions related to personal events of targets between individuals with SAD and healthy controls (Morrison et al., Citation2016). Only one study has examined social anxiety and affective empathy separately for positive and negative emotions. In Morrison et al.’s (Citation2016) study of SAD, there was no difference in affective empathy for negative emotions related to personal events of targets between those with SAD and healthy controls, whereas individuals with SAD showed less affective empathy for positive emotions related to personal events of targets compared to healthy controls.
The reviewed studies on balance suggest that elevated social anxiety is associated with enhanced cognitive empathy for negative emotions (|Auyeung & Alden, Citation2016, Citation2020), consistent with an enhancement hypothesis. On the other hand, although based on limited evidence, elevated social anxiety is associated with deficits in affective empathy for positive emotions (Morrison et al., Citation2016), consistent with an interference hypothesis. Social anxiety does not appear to be associated with the other types of empathy. Given these findings, it is noteworthy that enhanced cognitive empathy may not be adaptive (e.g. Auyeung & Alden, Citation2016; Tone & Tully, Citation2014). For example, greater cognitive empathy can be a marker of excessive cognitive perspective-taking and may facilitate vulnerability to maladaptive emotional outcomes (Tone & Tully, Citation2014), and can also lead to adverse relationship outcomes when the other in the relationship has relationship-threatening thoughts and feelings (Simpson et al., Citation2003).
These considerations raise the question of how cognitive empathy for negative emotions and affective empathy for positive emotions may be regulated and optimised in individuals with elevated social anxiety. Interestingly, given a deficit in affective empathy for positive emotions in individuals with SAD (Morrison et al., Citation2016), Morrison et al. (Citation2019) found that group cognitive–behavioural therapy (CBT) improved affective empathy for positive emotions, but not other forms of empathy (i.e. affective empathy for negative emotions; cognitive empathy for negative or positive emotions), relative to waitlist as well as mindfulness-based stress reduction. This finding suggests that specific forms of empathy can be modified.
Although CBT like that used in Morrison et al. (Citation2019) is the gold standard treatment for SAD (e.g. Mayo-Wilson et al., Citation2014), research has highlighted that CBT does not work for all individuals with SAD, with a meta-analysis finding a mean remission rate of 40% at post-treatment (Springer et al., Citation2018). As such, alternative interventions have been investigated, including a novel intervention known as emotional working memory training (eWMT; Schweizer et al., Citation2011, Citation2013). eWMT aims to improve flexibility of mental control of emotional information during training so that individuals can apply this in their day-to-day lives to better mentally disengage or shift away from task-irrelevant emotional information (e.g. negative automatic thoughts and associated distress), enable focus on the task at hand, and achieve their goals. Although research on eWMT is not as extensive as that on CBT, and further research is needed to better understand different aspects of eWMT (e.g. adherence, dropout rate, remission rate), a number of studies have shown eWMT to improve mental control and/or emotional symptoms in various samples (unselected student and community samples, e.g. Schweizer et al., Citation2011, Citation2013; sample with elevated social anxiety, du Toit et al., Citation2020; sample with post-traumatic stress disorder, Schweizer et al., Citation2017). Interestingly, a related line of research has shown that individual differences in working memory capacity can influence the outcomes of working memory training programs, although there are mixed results in terms of the nature of this moderating effect. Some studies have shown that individuals with higher pre-training working memory capacity benefit more from training, while other studies have shown that individuals with lower pre-training working memory capacity benefit more from training (e.g. Foster et al., Citation2017; von Bastian & Oberauer, Citation2013). Based on this body of research, it may be the case that eWMT can help to regulate empathy, and this may be dependent on pre-training working memory capacity. Indeed, eWMT may have particular potential to regulate cognitive empathy for negative emotions and affective empathy for positive emotions in socially anxious individuals because of its ability to improve mental disengagement from task-irrelevant emotional information and processes (e.g. social anxiety symptoms, and hypervigilance to others; Heimberg et al., Citation2010). This in turn enables appropriate attentional processes as well as normal cognitive and affective empathic processes to occur in the social situation at hand.
In the present studies, we aimed to extend the literature on empathy in social anxiety to: (a) better understand the relationship between social anxiety and empathy (Study 1), and (b) examine whether improving mental control of emotional information can enable appropriate empathy in individuals with elevated social anxiety (Study 2).
Study 1
Study 1 was a cross-sectional study comparing individuals with elevated social anxiety and individuals with normative (i.e. non-elevated) social anxiety levels recruited from the community on a dynamic empathy measure covering four types of empathy (i.e. cognitive empathy for negative emotions and for positive emotions of targets; affective empathy for negative emotions and for positive emotions of targets) completed under conditions of social threat. Study 1 thus merges key methods from relevant existing studies (Auyeung & Alden, Citation2016, Citation2020; Morrison et al., Citation2016), including use of a dynamic empathy measure focusing on personal events of targets, and a social threat manipulation to activate social anxiety. This combination of methodological elements in Study 1, alongside the results of existing studies (Auyeung & Alden, Citation2016; Morrison et al., Citation2016), helps to better understand the factors that are potentially involved in the empathic processes of individuals with elevated social anxiety (i.e. role of social threat; role of stimuli highlighting exclusion experiences of targets versus personal events of targets).
Aims and hypotheses
Study 1 aimed to compare cognitive and affective empathy for negative and positive emotions in individuals with elevated social anxiety and individuals with normative social anxiety levels. Based on the weighting of evidence consistent with an enhancement hypothesis, we predicted that under conditions of social threat in our study, individuals with elevated social anxiety would have better cognitive empathy and affective empathy for negative emotions and positive emotions related to personal events of targets, compared to individuals with normative social anxiety.
Method
Participants
Participants were 15 adults with normative social anxiety levels and 15 adults with elevated social anxiety, matched on gender, education level, and ± 3 years of age. Empirically derived cut-off scores on social anxiety measures were used to determine participant social anxiety status (normative versus elevated; see Measures section). Data from the participants with elevated social anxiety have been reported in a previous publication which included research questions and measures not reported in the current study (see Holder et al., Citation2020). Participants were recruited from the Sydney community using social media advertising (e.g. Facebook), word-of-mouth, and a university-based research participant recruitment platform. Participants received a small monetary reimbursement or, where relevant, course credit for their participation. There were no exclusion criteria. Details of participants are shown in . Sample size calculations for Study 1 are described in Supplementary File 1.
Table 1. Descriptive statistics for Study 1 participants.
Measures
Short versions of the Social Interaction Anxiety Scale (SIAS-6) and the Social Phobia Scale (SPS-6; Peters et al., Citation2012)
The 6-item SIAS-6 and 6-item SPS-6 measure anxiety related to social interactions and performing various tasks (e.g. eating, writing), respectively. Items are rated on a 5-point Likert scale, ranging from 0 (“not at all characteristic or true of me”) to 4 (“extremely characteristic or true of me”). The SIAS-6 and SPS-6 both have demonstrated good internal consistency (in the current sample, Cronbach’s α = .89 and .94, respectively) and validity (Peters et al., Citation2012). The SIAS-6 and SPS-6 were used to determine participant social anxiety status. Based on Peters et al. (Citation2012), individuals who scored seven or higher on the SIAS-6 or two or higher on the SPS-6 were considered to have elevated social anxiety, whereas those who scored six or lower on the SIAS-6 and zero or one on the SPS-6 were considered to have a normative level of social anxiety.
Depression Anxiety Stress Scales (21-item version) – Depression subscale (DASS-D; Lovibond & Lovibond, Citation1995)
The 7-item DASS-D assesses levels of depression over the past week and was administered for the purpose of sample description. Items are rated on a 4-point Likert scale, ranging from 0 (“did not apply to me at all”) to 3 (“applied to me very much, or most of the time”). Following Lovibond and Lovibond (Citation1995), the DASS-D score was doubled to obtain the full DASS score equivalent. The DASS-D has demonstrated good internal consistency (in the current sample, Cronbach’s α = .86) and validity (Antony et al., Citation1998).
Modified State-Trait Anxiety Inventory – State subscale 3-item version (STAI-S3)
The original STAI-S (Spielberger et al., Citation1983) is composed of 20 items. A 3-item version of the STAI-S, henceforth referred to as the STAI-S3, was developed for the current study to enable an efficient assessment of state anxiety before and after the provision of social threat (see Procedure; for similar modifications of the STAI-S, see Reyes et al., Citation2020). Participants rated items referring to feeling nervous, worried, and tense in terms of “how you feel right now”. Each item was rated using a 4-point Likert scale from 1 to 4, with higher scores reflecting higher state anxiety. The 3 items were selected because they are the three positively worded items (i.e. worded in the same direction as the scale’s total score) with the highest factor loadings on the STAI-S factor (see Vigneau & Cormier, Citation2008). Preliminary evidence suggests that the STAI-S3 has good internal reliability (in the current sample, Cronbach’s α = .83).
Empathic accuracy task (Zaki et al., Citation2008)
We used a modified version of the empathic accuracy task (Zaki et al., Citation2008) used in Morrison et al. (Citation2016) to measure cognitive empathy and affective empathy for both positive and negative emotions (for a schematic of the empathic accuracy task procedure, see Morrison et al., Citation2016). The dynamic and performance-based nature of this task provides a more ecologically valid assessment of empathy compared to other measures of empathy (e.g. self-report measures). The task consists of 10 brief video clips (i.e. each < 180 s; M = 125 s) of individuals (“targets”) discussing emotional and personally-relevant life events. There were four male targets and six female targets, with five targets conveying an overall positive story and five targets conveying an overall negative story. During the creation of the task by Zaki et al. (Citation2008), after targets were filmed, they watched their own videos and provided continuous (i.e. moment-to-moment) ratings of the level of positive or negative valence they had experienced at each moment in the video clip using a 9-point Likert scale (1 = very negative to 9 = very positive). As participants complete the empathic accuracy task, their moment-to-moment perceptions of the target’s emotions are typically correlated with the targets’ self-ratings to provide an index of cognitive empathy (Ripoll et al., Citation2013; Zaki et al., Citation2008).
In the current study, participants watched each of the 10 video clips on a laptop screen and were instructed to either provide continuous ratings for how the person in the video was feeling or provide continuous ratings of how they themselves were feeling while watching the video clip. In total, there were: three videos with targets conveying negative emotions where participants were asked to rate how the person in the video was feeling (i.e. cognitive empathy for negative emotions), two videos with targets conveying positive emotions where participants were asked to rate how the person in the video was feeling (i.e. cognitive empathy for positive emotions), two videos with targets conveying negative emotions where participants were asked to rate their own emotions while watching the video clip (i.e. affective empathy for negative emotions), and three videos with targets conveying positive emotions where participants were asked to rate their own emotions while watching the video clip (i.e. affective empathy for positive emotions). Videos were presented in the same pseudo-random order to all participants. To make their ratings, participants used a 101-point slider scale (0 = very negative to 100 = very positive) presented at the bottom of the laptop screen under each video. In general, cognitive empathic accuracy for relevant videos was determined by the correlation between the target ratings and the participant ratings for how the person in the video was feeling. Affective empathic accuracy for relevant videos was determined by the correlation between the target ratings and the participant ratings of their own emotions while watching the video clip.
More specifically, to calculate indices of empathic accuracy, participant ratings were first rescaled to be consistent with the 9-point scale used by Morrison et al. (Citation2016) (i.e. using Y = 0.08*X + 1). Participant ratings were sampled every 500 milliseconds, and consecutive blocks of four ratings were averaged, with each two-second averaged rating then forming one datapoint in the time-series data for analysis (see Morrison et al., Citation2016). The same data-reduction approach was applied to target ratings. Pearson correlations were computed for target and participant time-series data for each video and then transformed using the Fisher r-to-z transformation to normalise the distribution of correlations. Transformed Pearson correlations for relevant videos were then averaged to obtain an overall empathic accuracy score for the four domains (cognitive empathy for negative emotions, cognitive empathy for positive emotions, affective empathy for negative emotions, affective empathy for positive emotions), with higher scores reflecting greater empathic accuracy. Previous studies have provided evidence of the construct validity of the empathic accuracy task (e.g. cognitive empathic accuracy for negative emotions derived from the empathic accuracy task was positively correlated with participant self-reported trait empathy; Ripoll et al., Citation2013).
Procedure
Ethics approval was obtained from the Western Sydney University Human Research Ethics Committee. The study was preregistered as part of a larger study with the Australian New Zealand Clinical Trials Registry (ACTRN12618001196235). Interested individuals contacted the researchers and were emailed a link to online versions of the SIAS-6, SPS-6, and DASS-D. Participants were then invited to an individual in-person research session, where they provided informed consent, completed a demographics questionnaire, the STAI-S3, and were then administered the social threat. Specifically, they were informed that later in the session, they would be asked to complete an impromptu speech task. They were informed that their speech would be video-recorded using a camera embedded in the researcher’s laptop, and that their speech performance would be evaluated by the research team. Participants then completed another STAI-S3. Following this, participants completed the empathic accuracy task and other assessment measures not analysed in the current study (i.e. an anxiety-related questionnaire together with an executive function task). The order of presentation of the empathic accuracy task and the other assessment measures was randomised. Participants then completed a 2-minute speech task; they were given a speech topic, 1 min to prepare, and then 2 min to deliver the speech in front of the camera embedded in the researcher’s laptop. Recorded speech task performances were not analysed for the current study.
Statistical analyses
A one-way analysis of variance (ANOVA) or chi-square tests were used to determine whether there were differences between the two social anxiety groups. As a manipulation check, linear mixed models were used to examine change in state anxiety from before to after the provision of social threat (i.e. explanation of speech task). For the main analyses, following Morrison et al. (Citation2016), analyses were conducted separately for cognitive empathy and affective empathy. Linear mixed models were used for analysis with Group (elevated versus normative social anxiety), the repeated-measures variable Valence (target conveys negative emotions versus target conveys positive emotions), and a Group x Valence interaction specified as fixed effects, and an intercept term for subjects specified as a random effect.
Results
Preliminary analyses
Data screening
Data screening results are described in Supplementary File 2.
Group differences
Participants with elevated social anxiety and normative social anxiety did not significantly differ on demographic variables, all ps > .114, and as expected, the elevated social anxiety group had higher scores on the SIAS-6, SPS-6, and DASS-D, all ps < .001 (see ).
Manipulation check for the social threat induction
Relative to reported state anxiety at baseline, M = 4.77 (SD = 1.83), there was significantly higher reported state anxiety following the information given by the experimenter about the impending speech task, M = 5.77 (SD = 2.45), t(30) = 2.22, p = .034, d = 0.40. This indicates that the impending speech task was anxiety-provoking for participants and successful as a social threat. Further analyses also showed that there was no significant interaction between Group (elevated versus normative social anxiety) and Time (baseline versus after provision of information about speech task), t(30) = 0.30, p = .769, indicating the two groups had similar increases in anxiety.
Primary analyses
In the mixed model predicting cognitive empathic accuracy, the Valence main effect and the Valence x Group interaction were not significant, both ts < |1.43|, both ps > .164. However, the Group main effect was significant, reflecting higher cognitive empathic accuracy on average across the two valence conditions for the elevated social anxiety group compared to the normative social anxiety group, B = 0.32, 95% CI [0.13, 0.51], t(30) = 3.45, p = .002, Cohen’s d = 0.92. Notably, exploratory analyses confirmed similar effects when each of the valence conditions were specifically examined (negative emotions: B = 0.35, 95% CI [0.10, 0.60], t(58.73) = 2.84, p = .006, Cohen’s d = 1.04; positive emotions: B = 0.29, 95% CI [0.05, 0.54], t(58.73) = 2.38, p = .020, Cohen’s d = 0.81).
In the mixed model predicting affective empathic accuracy, the Group main effect and the Valence x Group interaction were not significant, both ts < |0.93|, both ps > .358. The Valence main effect was significant, reflecting higher affective empathic accuracy on average across the two participant groups for when targets conveyed positive emotions compared to when targets conveyed negative emotions, B = −0.27, 95% CI [−0.45, −0.10], t(60) = −3.08, p = .003, Cohen’s d = 0.53.
Study 1 Discussion
When under social threat, relative to individuals with normative social anxiety, individuals with elevated social anxiety demonstrated higher cognitive empathic accuracy when a target conveyed negative emotions, as well as when a target conveyed positive emotions, consistent with predictions. Inconsistent with predictions, we found individuals with elevated versus normative social anxiety did not differ in terms of affective empathic accuracy for targets conveying negative or positive emotions, although on average across the two groups, there was greater affective empathic accuracy for targets conveying positive emotions compared to negative emotions.
The interesting finding is that elevated social anxiety was associated with greater accuracy in terms of cognitive empathy in general, regardless of emotion conveyed by targets. This finding aligns with previous research showing elevated social anxiety was associated with greater cognitive empathy for negative emotions related to exclusion experiences of targets but only in the presence of social threat (Auyeung & Alden, Citation2016). Our study extends this previous research beyond situations where targets are discussing exclusion experiences, by showing that under social threat, elevated social anxiety is also associated with excessive cognitive empathy when targets are discussing personal events of a negative or positive nature.
One potential explanation for the cognitive empathy results is that the hypervigilance to evaluation from others that characterises individuals with elevated social anxiety, particularly when faced with social threat, may allow greater sensitivity at a cognitive level to the emotions that others are feeling (Tibi-Elhanany & Shamay-Tsoory, Citation2011), consistent with the enhancement hypothesis. Interestingly, the enhancement hypothesis, as well as the interference hypothesis, did not appear to apply to affective empathy in that individuals with elevated social anxiety were comparable to their counterparts with normative levels of social anxiety in sharing the negative or positive emotions of targets. The affective empathy results are difficult to directly compare with the only other study that has examined affective empathy using a dynamic empathy task in individuals with SAD and healthy controls (Morrison et al., Citation2016) because the previous study did not administer a social threat. The current study’s findings in relation to affective empathy nonetheless suggest that in the presence of social threat, there is no interference to nor enhancement of the sharing of emotions for individuals with elevated social anxiety relative to those with normative social anxiety levels. Overall, these results, and their relationships with the enhancement and interference hypotheses, collectively suggest that cognitive and affective empathy are distinct processes, consistent with previous work (e.g. Zaki & Ochsner, Citation2012). Given this, it may be that hypervigilance, a cognitive process that can help enhance cognitive awareness of others’ negative and positive emotions, is functionally independent of processes related to the felt sense of others’ emotions.
Study 2
Given Study 1 has shown that under social threat, individuals with elevated social anxiety exhibit greater cognitive empathy than their counterparts with normative social anxiety, it is possible then that this increased cognitive empathy might contribute to maladaptive emotional and relational outcomes (Simpson et al., Citation2003; Tone & Tully, Citation2014). Interventions such as eWMT that can improve mental control over emotional information and allow better disengagement from potential processes contributing to elevated cognitive empathy (e.g. hypervigilance to others) should then enable appropriate empathic processes to occur. Hence, Study 2 examined whether eWMT can help to regulate elevated levels of cognitive empathic accuracy in individuals with elevated social anxiety.
Aims and hypotheses
Study 2 had two main aims: (a) to examine the effect of an eWMT task, designed to train mental control over negative emotional information, versus a control training (CT) procedure, on cognitive and affective empathy for negative emotions and positive emotions in individuals with elevated social anxiety, and (b) to test whether pre-training working memory capacity influenced the effect of eWMT versus CT. The latter aim was based on previous evidence showing the moderating effect of pre-training working memory capacity on the outcomes of working memory training programs, although as mentioned previously, there are mixed results as to the nature of this moderation (e.g. von Bastian & Oberauer, Citation2013).
Based on previous eWMT studies (e.g. Schweizer et al., Citation2011), the finding that aberrations in empathy can be ameliorated (Morrison et al., Citation2019), and the nature of the eWMT task in this study (i.e. trains mental control over negative emotional information which may help to disengage hypervigilance to negative emotional information), we predicted individuals with elevated social anxiety would have a decrease in their cognitive empathy for negative emotions (i.e. down-regulation of enhanced cognitive empathic accuracy so it is no longer elevated) following eWMT, but not following CT. Although previous research also suggests that this proposed training effect might be moderated by individual pre-training working memory capacity (e.g. von Bastian & Oberauer, Citation2013), the mixed results in previous work meant that we did not have a specific prediction regarding pre-training working memory capacity as a moderator. Rather, our test of pre-training working memory capacity as a moderator was exploratory. Considering the nature of the eWMT task focused on negative emotional information, we also did not expect an effect of eWMT (relative to CT) on cognitive empathy for positive emotions. Finally, given in Study 1 there was no difference in affective empathic accuracy (regardless of emotion conveyed by target) between individuals with elevated versus normative social anxiety (i.e. affective empathy was not aberrant in the elevated social anxiety group), we did not expect an effect of eWMT (relative to CT) on affective empathy for negative or positive emotions in Study 2.
Method
Participants
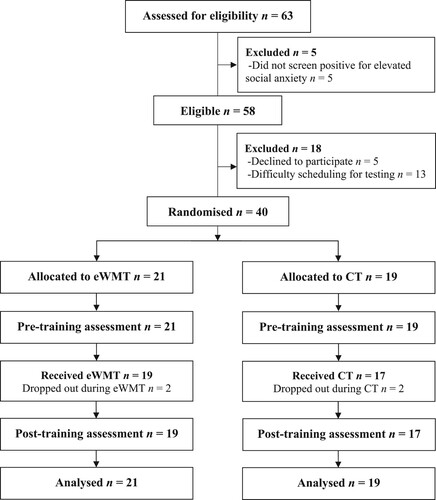
Participants were 40 adults with elevated social anxiety recruited from the Sydney community (35 females; mean age in years = 22.95; SD = 7.17; SIAS-6 and SPS-6 cut-off scores were used to determine elevated social anxiety status, as in Study 1). Data from these participants have been reported in a previous publication which included research questions and measures not reported in the current study (see du Toit et al., Citation2020). Recruitment methods and reimbursements for participation were the same as those used in Study 1. There were no exclusion criteria. There was no overlap in participants for Study 1 and Study 2. Participants of Study 2 were randomly allocated to either the eWMT condition (n = 21) or the CT condition (n = 19). Descriptive characteristics of participants are shown in . Sample size calculations for Study 2 are described in Supplementary File 1.
Table 2. Descriptive statistics for Study 2 participants in the eWMT and CT conditions.
Design
The study had a single-blind randomised design. Randomisation occurred at the start of the study using a random number generator. Researchers conducting the study were informed of participant training condition allocation (eWMT or CT) after participants had been recruited into the study, and researchers were therefore not blinded to training condition allocation. Participants were informed that they would be undertaking working memory training. They were not informed that there were actually two training conditions, one of which was a CT condition, and they were not informed of the condition to which they were allocated. Outcomes were assessed at pre-training and post-training. A CONSORT flow diagram is shown in .
Figure 1. CONSORT flow diagram. eWMT = Emotional working memory training; CT = Control training.
Interventions
Emotional working memory training (eWMT) task
The eWMT task was a dual n-back task from Schweizer et al. (Citation2011) designed to train mental control over negative emotional information. Participants in the task simultaneously monitored: (a) visual stimuli (70% negative emotional faces, e.g. angry, sad, fearful, and 30% neutral faces) presented for 500 milliseconds in one of 16 locations on a 4 × 4 grid on a laptop screen, and (b) auditory stimuli (70% negative emotional words, e.g. rape, evil, and 30% neutral words, e.g. tree, book) presented for 350–900 milliseconds through a speaker. Any time from the onset of each face-word presentation to the onset of the next trial after 2500 milliseconds, participants needed to indicate whether the just-displayed visual stimulus was in the same location as that presented n presentations prior by pressing the left arrow key, and whether the previously presented auditory stimulus was the same as that presented n presentations prior by pressing the right arrow key. If both the visual stimulus location and auditory stimulus was the same as that presented n presentations prior, participants needed to press both the left and right arrow keys. If the visual stimulus location or the auditory stimulus was not the same as that presented n presentations prior, participants were instructed to press neither of the keys. Auditory feedback was given for correct responses (single long high-pitch tone) and incorrect or missed responses (two short low-pitch tones). Individual training sessions consisted of multiple blocks (number of blocks differed depending on how many blocks an individual participant could complete in 10 min) and each block had 20 + n picture-word pair trials. Six trials in each block were “target trials” where each presented a stimulus that matched the stimulus n positions back (two for visual modality, two for auditory modality, two for visual and auditory modalities simultaneously). Training started with n-back = 1, and when three or more consecutive trials were completed accurately, the n-back level increased by 1 for the next block. However, when five or more consecutive trials were completed inaccurately, the n-back level decreased by 1 for the next block (to a minimum of n = 1). In this way, the task monitors and adjusts so participants are always working at their peak performance level. Performance level on the eWMT for each training session was indicated by the mean level of n-back achieved. The training schedule was such that participants completed six 10-minute individual training sessions, with one session per day over six consecutive days (with the exception of weekends). Notably, this eWMT schedule was different to that used in Schweizer et al. (Citation2011), which involved 20 sessions in total each about 20 min in duration spread over a month.
Control training (CT) task
The CT task was a feature match task that had minimal demands on participants’ working memory, similar to the CT task used in Schweizer et al. (Citation2011). However, unlike the Schweizer et al. (Citation2011) CT task which used geometrical shapes as the visual stimuli, the current study’s CT task used the same visual stimuli as the eWMT task (i.e. 70% negative emotional faces and 30% neutral faces). Participants were presented with a series of trials on a laptop screen, with each trial consisting of two panels presented on the left and right of the screen. Each panel contained a minimum of eight faces, and participants were required to indicate whether the panels were identical. Participants were provided with auditory feedback on whether a response was correct or incorrect. The number of faces presented in subsequent trials increased with improved performance to a maximum of 12 faces per panel. Performance level on the CT task was indicated by a composite score which accounted for: the number of correct trials, number of trials attempted, and reaction time. The training schedule was such that participants completed six 10-minute individual training sessions, with one session per day over six consecutive days (with the exception of weekends). Notably, this CT schedule was different to that used in Schweizer et al. (Citation2011), which involved 20 sessions in total each of 20 min in duration spread over a month.
Measures
The SIAS-6, SPS-6, DASS-D, and empathic accuracy task as described in Study 1 were used again in Study 2. Empathic accuracy task data in Study 2 were processed in the same way as described in Study 1.
Digit span backwards task (DSBT; Wechsler, Citation2008)
This task assessed working memory capacity for neutral stimuli (i.e. numbers). Participants were verbally provided with a series of numbers, increasing from two digits to eight digits, which they then repeated verbally but in reverse order. The task had 14 trials (2 trials for each digit span) and was stopped when participants had both trials incorrect for a specific digit span. Following Schweizer et al. (Citation2011), the maximum number of digits repeated in reverse order correctly was used as the outcome for this task.
Procedure
Ethics approval was obtained from the Western Sydney University Human Research Ethics Committee. The study was part of a larger study pre-registered with the Australian New Zealand Clinical Trials Registry (ACTRN12618001196235). Interested individuals contacted the researchers and were emailed a link to online versions of the SIAS-6, SPS-6, and DASS-D. Individuals who had elevated social anxiety (as per SIAS-6 and SPS-6 cut-off scores) were invited to an individual in-person pre-training session, where they provided informed consent. Participants then completed a demographics questionnaire, the DSBT, and were then administered the social threat. Specifically, they were informed that later in the session, they would be asked to complete an impromptu speech task. They were informed that their speech would be video-recorded using a camera embedded in the researcher’s laptop, and that their speech performance would be evaluated by the research team. Following this, participants completed the empathic accuracy task and other assessment measures not analysed in the current study (i.e. a task assessing attention, which was randomised in terms of order with the empathic accuracy task, followed by an anxiety-related questionnaire). Participants then completed a 2-minute speech task; they were given a speech topic, 1 min to prepare, and then 2 min to deliver the speech in front of the camera embedded in the researcher’s laptop. Recorded speech task performances were not analysed for the current study.
Participants subsequently completed either the training schedule for the eWMT task or the training schedule for the CT task, depending on their allocated condition. Following the training sessions, participants attended an individual post-training session, which involved repeated administration of components from the pre-training session (i.e. administration of a social threat, the empathic accuracy task and assessment measures not analysed in the current study, speech task).
Statistical analyses
A one-way ANOVA or chi-square tests were used to determine whether there were pre-training differences between the two conditions. Linear mixed models analyses with time specified as a fixed effect and an intercept term for subjects specified as a random effect were conducted to examine training performance changes over the six training sessions for each training condition separately (as the training performance variable for each training condition was different). For the empathic accuracy task, consistent with Study 1 and Morrison et al. (Citation2016), analyses were conducted separately for cognitive empathy and for affective empathy. Furthermore, we opted to further separate these analyses by the emotions of targets to examine cognitive empathy for negative and positive emotions separately, and affective empathy for negative and positive emotions separately. This was done considering the number of factors in Study 2 (see below) and to prevent an underpowered analysis of a model involving a four-way interaction (cf. sample size calculation focused on Time x Condition interaction). Hence, for each of the empathy variables, linear mixed models analyses were used to examine the effect of training on change in empathy such that: Time (Pre- versus Post-training), Condition (eWMT versus CT), and an interaction involving these factors were specified as fixed effects, and an intercept term for subjects was specified as a random effect. These analyses were then replicated but with pre-training social anxiety and depression levels added as covariates to allow modelling of symptom levels, consistent with du Toit et al. (Citation2020). For each of the empathy variables, linear mixed models analyses were also used to examine pre-training working memory capacity (DSBT) as a moderator of the effect of training on change in empathy such that: Time (Pre- versus Post-training), Condition (eWMT versus CT), pre-training working memory capacity (DSBT), and interactions involving these factors were specified as fixed effects, and an intercept term for subjects was specified as a random effect. These analyses were again repeated with pre-training social anxiety and depression levels added as covariates. For all analyses, interpretation focused on the Time x Condition interaction. The linear mixed models analyses incorporated all available data, including participants with at least one data point on outcome variables under the missing-at-random assumption. Thus, our analyses followed the intention-to-treat principle.
Results
Preliminary analyses
Data screening
Data screening results are described in Supplementary File 2. Two participants who did not adhere to the study protocol and four participants who dropped out were retained for analyses following the intention-to-treat principle.
Pre-training differences
The eWMT and CT conditions did not significantly differ on the pre-training variables shown in , all ps > .052. Notably the Study 2 sample had significantly higher pre-training cognitive empathic accuracy for negative and positive emotions, and similar affective empathic accuracy for negative and positive emotions, when compared to the Study 1 sample with normative social anxiety (see Supplementary File 3).
Training performance
Dual N-back task for eWMT
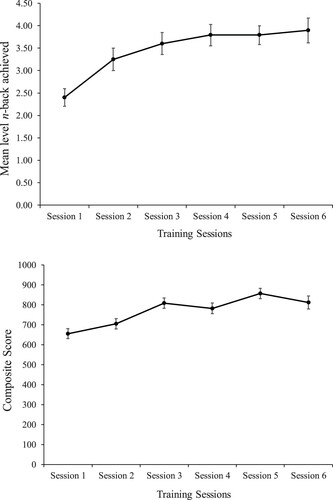
(Panel A) shows the training performance changes during eWMT. There was a significant effect of Time, B = 0.28, 95% CI [0.20, 0.35], t(97.66) = 7.34, p < .001, indicating the mean level of n-back achieved increased over the training, reflecting performance improvements. Based on the modelled mean difference between Session 1 and Session 6, and the SD at Session 1, Cohen’s d = 1.57 for the Time effect.
Figure 2. Panel A (top panel): Training performance changes for the dual n-back task during emotional working memory training (eWMT). Panel B (bottom panel): Training performance changes for the feature match task during control training (CT). Error bars represent standard errors.
Feature match task for CT
(Panel B) shows the training performance changes during CT. There was a significant effect of Time, B = 34.73, 95% CI [24.96, 44.49], t(89.57) = 7.06, p < .001, indicating the composite score of the feature match task increased over the training, reflecting performance improvements. Based on the modelled mean difference between Session 1 and Session 6, and the SD at Session 1, Cohen’s d = 1.57 for the Time effect.
The effect of training on empathic accuracyFootnote1
Cognitive empathic accuracy for negative emotions
Results are shown in . In the first analysis examining the training effect, and in the replication of this analysis with pre-training social anxiety and depression levels added as covariates, the Time x Condition interactions were non-significant (both ps > .211). In the analysis examining pre-training working memory capacity (DSBT) as a moderator of the training effect, there was a significant Time x Condition interaction (p = .038), but this was secondary to a significant Time x Condition x DSBT interaction (p = .014). In the replication of this analysis with pre-training social anxiety and depression levels added as covariates, the Time x Condition interaction, and the Time x Condition x DSBT interaction, remained significant (ps = .036 and .013, respectively).
Table 3. Effects of eWMT and CT on cognitive empathic accuracy for negative and positive emotions of targets in Study 2.
To probe the structure of the significant three-way interaction in the model with working memory capacity as a moderator of the training effect and covariates, simple slopes analyses were conducted to examine the eWMT versus CT training effect at low and high levels of pre-training working memory capacity (i.e. 1 SD below and 1 SD above the mean on the DSBT variable, respectively). At low levels of pre-training working memory capacity, there was no significant pre- to post-training change in cognitive empathic accuracy for negative emotions for the eWMT condition, B = 0.04, 95% CI [−0.14, 0.22], z = 0.45, p = .655, or the CT condition, B = −0.10, 95% CI [−0.32, 0.19], z = −0.90, p = .367. At high levels of pre-training working memory capacity, there was no significant pre- to post-training change in cognitive empathic accuracy for negative emotions for the CT condition, B = 0.19, 95% CI [−0.03, 0.42], z = 1.69, p = .091, but there was a significant pre- to post-training decrease in cognitive empathic accuracy for negative emotions for the eWMT condition, B = −0.22, 95% CI [−0.40, −0.04], z = −2.45, p = .014. Based on the modelled mean difference between pre- and post-training, and the SD at pre-training, the decrease in cognitive empathic accuracy for negative emotions for the eWMT condition in terms of Cohen’s d was 0.72.
Cognitive empathic accuracy for positive emotions
Results are shown in . There were no significant Time x Condition interactions or Time x Condition x DSBT interactions in any of the models (all ps > .103).
Affective empathic accuracy for negative emotions
Results are shown in . There were no significant Time x Condition interactions or Time x Condition x DSBT interactions in any of the models (all ps > .608).
Table 4. Effects of eWMT and CT on affective empathic accuracy for negative and positive emotions of targets in Study 2.
Affective empathic accuracy for positive emotions
Results are shown in . There were no significant Time x Condition interactions or Time x Condition x DSBT interactions in any of the models (all ps > .556).
Study 2 Discussion
Against predictions, there was no differential effect of eWMT versus CT on cognitive empathy for negative emotions in individuals with elevated social anxiety. However, when pre-training working memory capacity was examined as a moderator of the training effect, a differential training effect was found for those with higher pre-training working memory capacity such that cognitive empathic accuracy for negative emotions decreased following eWMT and did not significantly change following CT. For those with lower pre-training working memory capacity, there was no significant change in cognitive empathic accuracy for negative emotions following eWMT or CT. Consistent with predictions, there was no effect of eWMT versus CT on cognitive empathy for positive emotions, or affective empathy for negative or positive emotions, even when pre-training working memory capacity was examined as a moderator.
General discussion
Two studies were conducted to further the literature on social anxiety and empathy. Using a dynamic empathy measure, in Study 1 we examined the differences in cognitive and affective empathy for positive and negative emotions under conditions of social threat between individuals with elevated social anxiety and individuals with normative social anxiety. Inconsistent with both the enhancement and interference hypotheses, the elevated social anxiety group were comparable in affective empathy for positive and negative emotions relative to the normative social anxiety group in the presence of social threat. Consistent with the enhancement hypothesis and previous research (Auyeung & Alden, Citation2016), the elevated social anxiety group showed better cognitive empathy for positive and negative emotions than the normative social anxiety group. This latter finding suggests that individuals with elevated social anxiety under conditions of social threat may have a generalised enhancement of cognitive empathy, regardless of emotion conveyed by targets when discussing personal events. This is consistent with models of social anxiety (e.g. Heimberg et al., Citation2010), which highlight the tendency of individuals with elevated social anxiety under conditions of social threat to be hypervigilant to evaluation from others. Such increased attention to others may facilitate enhanced cognitive empathy. However, if this is the case then this process appears to be independent of affective empathy.
Study 2 used an eWMT program designed to train mental control over negative emotional information to examine its effect on cognitive and affective empathy for negative and positive emotions in individuals with elevated social anxiety. Although there was no overall treatment effect as anticipated whereby cognitive empathy for negative emotions would decrease following eWMT but not CT, this differential treatment effect was found specifically for those with higher pre-training working memory capacity. Furthermore, as expected, there was no effect of eWMT versus CT on cognitive empathy for positive emotions, or affective empathy for negative or positive emotions, even when pre-training working memory capacity was examined as a moderator. Considering both Study 1 and Study 2 results, it is noteworthy that there was alignment in the findings. Specifically, cognitive empathy for negative emotions, shown to be higher in individuals with elevated social anxiety from Studies 1 and 2 relative to individuals with normative social anxiety from Study 1, was also shown in Study 2 to decrease following eWMT in individuals with elevated social anxiety with higher pre-training working memory capacity.
The Study 2 results are consistent with research showing that pre-training individual differences need to be considered when examining working memory training effects (von Bastian & Oberauer, Citation2013). The Study 2 results are also broadly consistent with the only other interventional study in the area of empathy and social anxiety showing that non-normative empathic accuracy at baseline can be normalised following intervention (Morrison et al., Citation2019). While the intervention study by Morrison et al. (Citation2019) showed that group CBT improved affective empathy for positive emotions better than a waitlist condition or mindfulness-based stress reduction, we found that eWMT focused on negative emotional information was able to down-regulate elevated cognitive empathy for negative emotions relative to CT for those with higher pre-training working memory capacity. We have thus extended the literature to show that aberrations in empathy may be addressed through interventions which target mental control of emotional information.
One potential interpretation of the overall Study 2 findings is that those socially anxious individuals with higher pre-training working memory capacity were able to benefit the most from the eWMT task, meaning that they were more able to improve their mental control over negative emotional information and disengage from the hypervigilance to negativity from others that is typically associated with social anxiety, especially under conditions of social threat (Heimberg et al., Citation2010). We speculate that disengaging such hypervigilance may have helped to: (a) regulate attentional focus to negative emotional information during the empathic accuracy task, which in turn enabled (b) the regulation of cognitive empathy for negative emotions. Future studies could further evaluate this possibility by examining hypervigilance to others in relation to empathic accuracy task performance both before and after eWMT. Future studies may also test whether eWMT tasks which include the training of mental control over positive emotional information impacts cognitive empathy for positive emotions.
Several limitations of the studies should be considered. First, individuals with elevated social anxiety were recruited for both studies and clinical interviews were not conducted to determine whether participants met criteria for SAD. An important next step would therefore be to examine how social threat conditions influence performance on a dynamic empathy measure in a sample of individuals with SAD, before potential evaluation of the effect of eWMT on empathy in such a clinical sample. Second, we inferred the aberrant nature of enhanced cognitive empathy in individuals with elevated social anxiety in Study 1 from a comparison with the cognitive empathy of individuals with normative social anxiety. An important direction for future research will be to further characterise the ways in which enhanced cognitive empathy in individuals with elevated social anxiety may be maladaptive (e.g. whether elevated cognitive empathy about others’ negative emotional states may contribute to one’s own personal distress about others; see also Tone & Tully, Citation2014). Third, eWMT used in Study 2 focused on training mental control over negative emotional information. As mentioned, future studies could use eWMT which includes both negative and positive emotional information to allow training of mental control over both types of information. Fourth, we did not have in our studies a condition where there was no social threat induction. Future studies should consider including such a condition to examine the role of social threat in the results. Fifth, the dose of eWMT in Study 2 (six 10-minute sessions spread over about a week) was relatively small compared to other studies (e.g. Schweizer et al., Citation2011). Future research could investigate whether a greater number of eWMT sessions might allow individuals with elevated social anxiety and low pre-training working memory capacity to show down-regulation of their cognitive empathic accuracy. Sixth, we used a dynamic empathy measure in both studies which involved pre-recorded videos of targets describing emotional personal events. Future studies could consider using actual dyadic conversation tasks and use reported thoughts and feelings in an empathic accuracy assessment (see Simpson et al., Citation2003). Finally, although sample sizes for both studies were based on sample size calculations that enabled sufficient power to detect effects of interest, the sample sizes can be considered relatively small, which can affect the precision of estimates, and may also result in inflated effects (Button et al., Citation2013). Future research should replicate the studies with large sample sizes for more definitive conclusions.
In sum, we provided evidence that the empathic abilities of individuals with elevated social anxiety deviate from those with normative social anxiety levels in terms of cognitive empathy for positive and negative emotions that is enhanced. This may be explained by hypervigilance to others (e.g. Heimberg et al., Citation2010). We also provided evidence that the deviation in cognitive empathy for negative emotions can be ameliorated with eWMT focused on negative emotional information, although this effect requires individuals with higher working memory capacity to undertake the training. Future research that further evaluates the nature of such deviations in empathic processes and the potential of interventions like eWMT will improve our understanding of social anxiety and empathy.
Supplemental Material
Download MS Word (36.6 KB)Acknowledgements
We would like to thank Sarah Certoma for helpful discussions and comments on this paper. All authors read and approved the final manuscript. SK (Conceptualization; Formal analysis; Methodology; Project administration; Writing – original draft; Writing – review and editing); SdT (Conceptualization; Methodology; Project administration; Writing – review and editing); CD (Conceptualization; Methodology; Project administration; Writing – review and editing); SS (Conceptualization; Methodology; Writing – review and editing); AM (Methodology; Writing – review and editing); DO (Methodology; Writing – review and editing); AP (Conceptualization; Methodology; Project administration; Writing – review and editing); LH (Conceptualization; Methodology; Project administration; Writing – review and editing); JH (Methodology; Writing – review and editing); MT (Methodology; Writing – review and editing); QJJW (Conceptualization; Data curation; Formal analysis; Methodology; Supervision; Writing – original draft; Writing – review & editing)
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets generated and analysed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
Notes
1 For completeness, all analyses in this section were also repeated with the participants who did not follow protocol or who dropped out (n = 6) removed from the dataset. The results of these analyses were virtually identical to the results presented from the intention-to-treat analyses based on N = 40, and led to the same conclusions.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev).
- Antony, M. M., Bieling, P. J., Cox, B. J., Enns, M. W., & Swinson, R. P. (1998). Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176–181. https://doi.org/10.1037/1040-3590.10.2.176
- Auyeung, K., & Alden, L. E. (2020). Accurate empathy, social rejection, and social anxiety disorder. Clinical Psychological Science, 8(2), 266–279. https://doi.org/10.1177/2167702619885410
- Auyeung, K. W., & Alden, L. E. (2016). Social anxiety and empathy for social pain. Cognitive Therapy and Research, 40(1), 38–45. https://doi.org/10.1007/s10608-015-9718-0
- Button, K. S., Ioannidis, J. P. A., Mokrysz, C., Nosek, B. A., Flint, J., Robinson, E. S. J., & Munafò, M. R. (2013). Power failure: why small sample size undermines the reliability of neuroscience. Nature Reviews Neuroscience, 14(5), 365–376. https://doi.org/10.1038/nrn3475
- Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In R. G. Heimberg, M. R. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social phobia: Diagnosis, assessment, and treatment (pp. 69–93). The Guilford Press.
- du Toit, S. A., Kade, S. A., Danielson, C. T., Schweizer, S., Han, J., Torok, M., & Wong, Q. J. J. (2020). The effect of emotional working memory training on emotional and cognitive outcomes in individuals with elevated social anxiety. Journal of Affective Disorders, 261, 76–83. https://doi.org/10.1016/j.jad.2019.09.085
- Fehm, L., Beesdo, K., Jacobi, F., & Fiedler, A. (2008). Social anxiety disorder above and below the diagnostic threshold: Prevalence, comorbidity and impairment in the general population. Social Psychiatry and Psychiatric Epidemiology, 43(4), 257–265. https://doi.org/10.1007/s00127-007-0299-4
- Foster, J. L., Harrison, T. L., Hicks, K. L., Draheim, C., Redick, T. S., & Engle, R. W. (2017). Do the effects of working memory training depend on baseline ability level? Journal of Experimental Psychology: Learning, Memory, and Cognition, 43(11), 1677–1689. https://doi.org/10.1037/xlm0000426
- Heimberg, R. G., Brozovich, F. A., & Rapee, R. M. (2010). A cognitive-behavioral model of social anxiety disorder: Update and extension. In S. G. Hofmann, & P. M. DiBartolo (Eds.), Social anxiety: Clinical, developmental, and social perspectives (pp. 395–422). Academic Press. https://doi.org/10.1016/B978-0-12-375096-9.00015-8.
- Holder, L. J., Prasad, A., Han, J., Torok, M., & Wong, Q. J. J. (2020). Shifting as a key executive function underlying cognitive restructuring for individuals with elevated social anxiety. Psychology and Psychotherapy: Theory, Research and Practice, 94(2), 217–230. https://doi.org/10.1111/papt.12301
- Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). Guilford Press.
- Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the depression anxiety stress scales (2nd ed.). Psychology Foundation.
- Mayo-Wilson, E., Dias, S., Mavranezouli, I., Kew, K., Clark, D. M., Ades, A. E., & Pilling, S. (2014). Psychological and pharmacological interventions for social anxiety disorder in adults: A systematic review and network meta-analysis. The Lancet Psychiatry, 1(5), 368–376. https://doi.org/10.1016/S2215-0366(14)70329-3
- Melchers, M., Montag, C., Reuter, M., Spinath, F. M., & Hahn, E. (2016). How heritable is empathy? Differential effects of measurement and subcomponents. Motivation and Emotion, 40(5), 720–730. https://doi.org/10.1007/s11031-016-9573-7
- Mikolajewski, A. J., Chavarria, J., Moltisanti, A., Hart, S. A., & Taylor, J. (2014). Examining the factor structure and etiology of prosociality. Psychological Assessment, 26(4), 1259–1267. https://doi.org/10.1037/a0037132
- Morrison, A. S., Mateen, M. A., Brozovich, F. A., Zaki, J., Goldin, P. R., Heimberg, R. G., & Gross, J. J. (2016). Empathy for positive and negative emotions in social anxiety disorder. Behaviour Research and Therapy, 87, 232–242. https://doi.org/10.1016/j.brat.2016.10.005
- Morrison, A. S., Mateen, M. A., Brozovich, F. A., Zaki, J., Goldin, P. R., Heimberg, R. G., & Gross, J. J. (2019). Changes in empathy mediate the effects of cognitive-behavioral group therapy but not mindfulness-based stress reduction for social anxiety disorder. Behavior Therapy, 50(6), 1098–1111. https://doi.org/10.1016/j.beth.2019.05.005
- Peters, L., Sunderland, M., Andrews, G., Rapee, R. M., & Mattick, R. P. (2012). Development of a short form social interaction anxiety (SIAS) and social phobia scale (SPS) using nonparametric item response theory: The SIAS-6 and the SPS-6. Psychological Assessment, 24(1), 66–76. https://doi.org/10.1037/a0024544
- Pittelkow, M. M., Aan Het Rot, M., Seidel, L. J., Feyel, N., & Roest, A. M. (2021). Social anxiety and empathy: A systematic review and meta-analysis. Journal of Anxiety Disorders, 78, 102357. https://doi.org/10.1016/j.janxdis.2021.102357
- Reyes, N., Boulton, K. A., Han, J., Torok, M., & Wong, Q. J. J. (2020). Cognitive bias modification for the induction of negative versus benign interpretations of the self in individuals with elevated social anxiety: Effects on self-related and anxiety outcomes. Cognitive Therapy and Research, 44(3), 567–580. https://doi.org/10.1007/s10608-019-10074-3
- Ripoll, L. H., Zaki, J., Perez-Rodriguez, M. M., Snyder, R., Strike, K. S., Boussi, A., Bartz, J. A., Ochsner, K. N., Siever, L. J., & New, A. S. (2013). Empathic accuracy and cognition in schizotypal personality disorder. Psychiatry Research, 210(1), 232–241. https://doi.org/10.1016/j.psychres.2013.05.025
- Schweizer, S., Grahn, J., Hampshire, A., Mobbs, D., & Dalgleish, T. (2013). Training the emotional brain: Improving affective control through emotional working memory training. The Journal of Neuroscience, 33(12), 5301–5311. https://doi.org/10.1523/JNEUROSCI.2593-12.2013
- Schweizer, S., Hampshire, A., & Dalgleish, T. (2011). Extending brain-training to the affective domain: Increasing cognitive and affective executive control through emotional working memory training. PLoS One, 6(9), e24372. https://doi.org/10.1371/journal.pone.0024372
- Schweizer, S., Samimi, Z., Hasani, J., Moradi, A., Mirdoraghi, F., & Khaleghi, M. (2017). Improving cognitive control in adolescents with post-traumatic stress disorder (PTSD). Behaviour Research and Therapy, 93, 88–94. https://doi.org/10.1016/j.brat.2017.03.017
- Simpson, J. A., Oriña, M. M., & Ickes, W. (2003). When Accuracy hurts, and when it helps: A test of the empathic accuracy model in marital interactions. Journal of Personality and Social Psychology, 85(5), 881–893. https://doi.org/10.1037/0022-3514.85.5.881
- Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., & Jacobs, G. A. (1983). Manual for the state-trait anxiety inventory. Consulting Psychologists Press.
- Springer, K. S., Levy, H. C., & Tolin, D. F. (2018). Remission in CBT for adult anxiety disorders: A meta-analysis. Clinical Psychology Review, 61, 1–8. https://doi.org/10.1016/j.cpr.2018.03.002
- Tibi-Elhanany, Y., & Shamay-Tsoory, S. G. (2011). Social cognition in social anxiety: First evidence for increased empathic abilities. Israel Journal of Psychiatry and Related Sciences, 48, 98–106.
- Tone, E. B., & Tully, E. C. (2014). Empathy as a “risky strength”: A multilevel examination of empathy and risk for internalizing disorders. Development and Psychopathology, 26(4pt2), 1547–1565. https://doi.org/10.1017/S0954579414001199
- Vigneau, F., & Cormier, S. (2008). The factor structure of the state-trait anxiety inventory: An alternative view. Journal of Personality Assessment, 90(3), 280–285. https://doi.org/10.1080/00223890701885027
- von Bastian, C. C., & Oberauer, K. (2013). Effects and mechanisms of working memory training: A review. Psychological Research, 78(6), 803–820. https://doi.org/10.1007/s00426-013-0524-6
- Wechsler, D. (2008). Wechsler adult intelligence scale-fourth edition (WAIS-IV). Pearson.
- Wong, Q. J. J., & Rapee, R. M. (2016). The aetiology and maintenance of social anxiety disorder: A synthesis of complementary theoretical models and formulation of a new integrated model. Journal of Affective Disorders, 203, 84–100. https://doi.org/10.1016/j.jad.2016.05.069
- Zaki, J., Bolger, N., & Ochsner, K. (2008). It takes two: The interpersonal nature of empathic accuracy. Psychological Science, 19(4), 399–404. https://doi.org/10.1111/j.1467-9280.2008.02099.x
- Zaki, J., & Ochsner, K. (2012). The neuroscience of empathy: Progress, pitfalls and promise. Nature Neuroscience, 15(5), 675–680. https://doi.org/10.1038/nn.3085