
ABSTRACT
Dry eye disease (DED), a multifactorial condition of the tear film and ocular surface, is one of the leading reasons for patients seeking eye care. Despite the multiple toxic ingredients of eye make-up products and their long-term application close to the ocular surface, few studies have analyzed their role in initiating and worsening DED. Females and the elderly experience the highest prevalence of DED and may be particularly vulnerable to the effects of eye make-up. The multifactorial nature of DED and common mechanisms behind several ocular surface diseases make it difficult to link a particular ingredient-driven mechanism to DED. Therefore, here, we list potential responses to eye cosmetics that may be involved in DED development. The first part of this review introduces the anatomy of the eye and DED, the second section explains the classification of eye cosmetic products, and the final part discusses the undesired effects under physical, pathogenic, and chemical insults.
Introduction
The cosmetics industry has been experiencing a steady increase in production and sales in recent years. To expand sales, companies have aimed at broader age groups (e.g., the elderly), increased marketing of anti-aging products, and considered the cultural/ethnic differences in cosmetic usage, habits, and beliefs.Citation1 As a result, cosmetic use spans a wide spectrum of ages and sexes in everyday life2 as well as the TV and film industries.Citation3 However, its application is particularly widespread among women.Citation2,Citation4 From a long list of raw ingredients, cosmetics typically contain preservatives, vehicles, antioxidants, humectants, fragrances, ultraviolet absorbers, emollients, emulsifiers, acrylates, and dyes.Citation5 Some of these ingredients pose a health risk to consumers (for a review, see references.Citation6–9)
Among potential sites of reaction to ingredients in the body, the eye and periorbital region are considered particularly sensitive due to their position and anatomy. The application of eye cosmetics to increase beauty and attractivenessCitation10 may come at the cost of discomfort, allergic reactions, and ocular changes.Citation11 Eye make-up products are known to cause inflammation,Citation11,Citation12 affect lipid layer quality and influence ocular comfortCitation12 and are key factors in the initiation and/or exacerbation of dry eye disease (DED).Citation13
Dry eye, a multifactorial condition, is characterized by symptoms of dryness and irritation of the ocular surface due to alterations in the quality or quantity of the tear film. It can be experienced at any age, but DED is particularly widespread among women and the elderly. It has been estimated that 5–50% of the population suffer from this disease,Citation14 making it one of the most common ocular conditions. DED causes a quality-of-life burden on sufferers, and its scale imposes considerable economic and medical resource usage.Citation15,Citation16
Several reviews have addressed the effect of eye cosmetic constituents on the ocular surface, leading to various ocular conditions.Citation11,Citation12,Citation17,Citation18 However, the multifactorial nature of DED makes it difficult to link a particular ingredient-driven mechanism to this condition. In addition, there are common mechanisms behind several ocular surface diseases. Therefore, here, we list the potential responses to eye cosmetics that may be involved in the development of dry eye.
The first part of this paper introduces the anatomy of the eye and DED. The second section provides an outline of the classification of eyelash cosmetics and eyelid cosmetic products. Finally, undesired effects are discussed under physical, pathogenic, and chemical insults in the third part. The terms cosmetic and make-up are used interchangeably in this review, as they are in the general population, although technically, the former includes a wide spectrum of items such as personal care products.Citation5 Additionally, the use of contact lenses was not the focus of this work.
Anatomy of eye and periorbital area
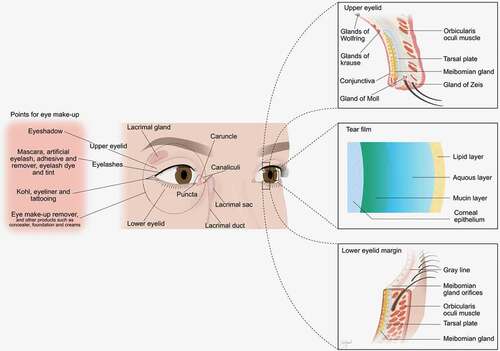
The anatomy of the human face can be classified into upper, middle, and lower regions. The eye and periorbital area are housed in the upper face, where make-up products are generally applied (). Therefore, anatomical knowledge is necessary to understand how cosmetics affect the eye.
Figure 1. Anatomy of internal and external parts of eye and periorbital area, and points for eye makeup along with the artificial eyelash, adhesive and remover.
Eyelid
The eyelid, a thin layer of skin, primarily protects the eye against mechanical trauma.Citation19 Another vital responsibility of the eyelid is related to tears by supplying essential nutrients and helping with even tear distribution over the eye, followed by drainage through the lacrimal puncta. Additionally, the eyelid maintains the globe in the correct position within the orbit and controls the amount of light entering the eye via squinting.Citation20 The eyelids comprise 5 layers: skin (epidermis and dermis), subcutaneous tissue, muscular layer, and tarsal plate.Citation21
Eyelid margin
The margin of the eyelid with ~2 mm thickness is divided by a grey line into two regions, where posteriorly it is covered with conjunctival epithelium and anteriorly with cutaneous epidermis.Citation22 This margin is the place of transition from the nonkeratinized-columnar epithelium of the conjunctiva to the keratinized-stratified squamous epithelium of the skin, referred to as the mucocutaneous junction.Citation23 The former region encompasses meibomian gland orifices, whereas the latter holds the eyelashes.24
Eyelashes
Eyelashes (cilia) protect the eye from potential incoming danger through the reflective response, defend the eye against particles using its curved shape, help to keep the moisture of the eye by minimizing airflow, filter out sunlight, and provide natural beauty. There are typically 2–3 rows of lashes on each lid rim. The upper eyelashes differ in number (100–150), length (8–12 mm), and shape (curved upward) compared to the lower ones (50–75 and 6–8 mm, respectively). With a normal lifetime of 5–12 months, the eyelashes grow ~0.15 mm per day, depending on age and the physical health of individuals. The eyelashes are housed in the muscular layer and are typically concomitant with two glands of Zeis (modified sebaceous gland) and often the apocrine gland of Moll (a modified sweat gland).Citation24
Meibomian glands
Meibomian glands (tarsal glands) secrete the tear film outer layer lipids and attenuate the evaporation of the aqueous phase, lubricate the corneal surface during blinking, retain the near-perfect optical surface necessary for visual acuity, seal the opposing lid margins during sleep, and create a protective barrier against microorganisms and particles. They are composed of 30–40 (upper lid) and 20–25 (lower lid) individual grape-like clusters in the tarsal plate, between the eyelashes and the bulbar conjunctiva. The glands of meibum constantly synthesize and secrete a complex mixture containing lipids (e.g., cholesterol, wax esters, diesters, triacylglycerol, free fatty acids, and phospholipids) and proteins (e.g., keratins, lactoferrin, lipophillins, lipocalins, phospholipid transfer proteins, surfactant proteins, and proteoglycans).Citation25,Citation26
Conjunctiva
The conjunctiva protects the soft tissues of the orbit and eyelid, maintains the aqueous and mucous layers of the tear film, is involved in immune protection, lubricates the eye, and supplies oxygen. It is a thin, highly vascularized transparent mucous membrane lining the inner surface from the corneoscleral limbus to the eyelid margins and caruncle. The conjunctiva comprises an anterior stratified columnar epithelium containing numerous unicellular mucous glands (goblet cells) and a lamina propria composed of connective tissue with blood vessels, nerves, and glands. Three distinct regions of the conjunctiva are the bulbar (white sclera), forniceal (junction zone), and palpebral (inner surface of eyelid). The accessory lacrimal exocrine glands of Krause and Wolfring are located deep within the superior fornix and slightly above the superior border of the tarsus, respectively.Citation27,Citation28
Corneal epithelium
The corneal epithelium is a barrier to water, chemicals, and microorganisms. It also provides a smooth reflective surface, protects the underlying layers from injury, and contributes to the immune response via its dendritic Langerhans cells. As an outermost layer of the cornea, the epithelium is located above the Bowman’s membrane, stroma, Descemet’s membrane, and endothelium. Its uniform structure comprises a basal layer of cylindric cells, a wing cell layer, and a surface layer of flat cells with ultrastructural microplicae and microvilli. The corneal epithelium is divided into central and peripheral regions. The epithelium of the peripheral cornea has 7–10 cell layers and holds melanocytes or Langerhans cells. In contrast, no such cells exist in the 5–7 layers of the central corneal epithelium.Citation28,Citation29
Tear film
The tear film lubricates, nourishes, and protects the ocular surface. It is a transparent fluid comprising ~98% water, with the remainder composed of electrolytes, lipids, and proteins. Based on a 3-layered structure (), a traditional model, the tear film consists of (1) an outer lipid layer secreted by meibomian glands to reduce water evaporation, (2) an intermediate aqueous layer produced by the lacrimal glands and accessory lacrimal glands of Krause and Wolfring to supply oxygen and nutrients, and (3) an inner mucus layer produced by goblet and epithelial cells of the conjunctiva to attach and spread the tears evenly. However, the Tear Film and Ocular Surface Society Dry Eye Workshop (TFOS DEWS II) depicts the tear film as a 2-layered interactive structure composed of a mucoaqueous layer and a lipid layer. Tears are classified as basal, closed eye, emotional, and reflex types according to their mode of production.Citation30,Citation31
Nasolacrimal duct
Tear fluid and particles attached to the ocular surface are drained by the nasolacrimal duct into the inferior meatus of the nose. Anatomically, the lacrimal passages are divided into bony and membranous lacrimal sections. The latter include the lacrimal canaliculi, lacrimal sac, and the nasolacrimal duct. The last two parts are lined by a double-layered epithelium containing superficial columnar cells and basal flattened cells. Goblet cells may also be present in the epithelial layer. During blinking, tears are wiped and pushed into the lacrimal puncta, small openings located in the nasal upper and lower eyelids. The punctum ends in the canaliculus, where the fluid drains into the lacrimal sac followed by the nasolacrimal duct canal before reaching the nasal cavity.Citation31
Dry eye disease
The normal tear film is pivotal for ocular surface health and clear vision. Any alteration in the quality or quantity of the tear film may result in DED. DED symptoms vary and include discomfort, dryness, irritation, burning, stinging, gritty/foreign body sensation, and blurred vision. DED can vary from mild signs and symptoms to severe pain with the deterioration of visual function. The associated decreased quality of life and increased consumption of medical resources impose considerable cost to patients, families, and society.Citation14,Citation32
In 2017, TFOS DEWS II defined DED as “a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, and accompanied by ocular symptoms, in which tear film instability and hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles”.Citation33 In addition, the Asian Dry Eye Society provided an alternative definition for DED as “a multifactorial disease characterized by unstable tear film causing a variety of symptoms and/or visual impairment, potentially accompanied by ocular surface damage”.Citation34
A clinically relevant classification has been used by a TFOS DEWS II report for DED. It includes two major classes: aqueous-deficient dry eye (ADDE) and evaporative dry eye (EDE). ADDE involves the failure of lacrimal secretion caused mainly by Sjögren and non-Sjögren lacrimal disease, whereas EDE is the excessive tear loss from the ocular surface mostly due to meibomian gland dysfunction or abnormal blink patterns. The combination of these two classes also exists among DED patients.Citation35,Citation36
The main aspects involved in DED are ocular-surface hyperosmolarity and inflammation, which may act together or independently. The pathogenesis of DED is mediated by various cellular and molecular components such as cytokines, chemokines, metalloproteinases, and their receptors. Hyperosmolarity caused by dysfunctional tear secretion (ADDE) and/or excessive water evaporation (EDE) leads to an inflammatory cascade followed by a vicious circle. The process can be initiated and/or worsened by intrinsic (e.g., ocular disease and immune-mediated conditions) and extrinsic (e.g., chemical, environmental, and pathogenic insults) factors.Citation37,Citation38
Eye cosmetics
Historically, cosmetics have been used by civilizations in religious rituals throughout the ancient world. The main goals were to improve beauty, promote health, and indicate social class. The eyes, often referred to as the windows to the soul and a powerful communication tool, were at the center of attention in this process. Therefore, various make-up mixtures with specific natural colors, trends, and styles have been applied for accentuating them. For instance, the use of black pigments made of ashes, soot, and antimony in the form of kohl has been documented in the early Bronze Age (c. 4000–1500 BCE), old Middle East (ancient Egypt and Mesopotamia), classical Greece, and antiquated Rome to darken the lashes, eyelids, and eyebrows.Citation11,Citation17 For millennia, stretching from ~4000 BCE through to the 21st century, the development of eye cosmetics progressed substantially. Consequently, different products with a broad range of ingredients under diverse categories have been introduced and utilized in myriad ways. Table S1 shows the common classes of materials used in different forms of eye cosmetics.
Classification
Eyelash cosmetics
Eyelash cosmetics comprise a range of products, including mascara and eyelash dye. These products perform differently depending on their formulation, material, and/or design ().
Mascara
Mascara is utilized to make the eyes appear bigger and form an intense look by darkening, stretching, and thickening the eyelashes. For dramatizing the eyes and enhancing contrast between the iris and sclera, different colors are added to the preparation. Mascara is primarily available as shades of blacks and browns, but also purples, blues, greens, yellows, and pinks. For those interested in lengthening without darkening, unpigmented products are sold on the market.Citation39
Mascara has been produced in a variety of forms, including cakes (or blocks), creams, gels, and low viscosity liquids with diverse ingredients (Table S2). Cake mascara was originally a mixture of soap and pigment, which is stamped into blocks. Two major disadvantages of this product are: 1) the requirement of a wet brush to make a paste before its application and 2) smudging and running of the formed film on the lashes with tears, perspiration, or rain due to its water solubility. Although improved water-resistant cakes are made by adding waxes, consumers prefer to use either cream or liquid forms instead. The next product, cream mascara, soon gained considerable attention because of its ease of application and less tendency to run with moisture and form clumps on the lashes. This form of mascara typically comprises dispersions of waxes and pigments in water, with a final consistency similar to vanishing cream. The cream texture with a substantial water-holding property permits to include natural and synthetic film formers to improve adhesion. However, this ability comes at the cost of shortening the application time owing to clump formation following water evaporation. Therefore, liquid in several types has found its way into mascara formulations. Liquid mascara, the most popular modern form, is divided into water-based (waxes (e.g., carnauba wax and beeswax), pigments, and resin dissolved in water), non-water-based (e.g., candelilla wax and ozokerite, pigments, and petroleum distillates) and water/non-water-based hybrid products. The latter intend to combine the beneficial effects, such as short drying time and waterproofness, from the two other categories.Citation40,Citation41
Several factors, including the desired effect, type of eyelashes, and health status of consumers, play important roles in the choice of a suitable mascara. For a make-up effect, the design of the applicator brush and the diameter of the aperture are apparently as important as the formulation of the mascara. Hence, the market success of cream and particularly liquid mascaras has partly been due to the advent of the automatic applicator, spiral-tipped wand, or wand and brush applicator.Citation11,Citation42
Eyelash dye and tint
Eyelash dye and tint involve the application of permanent and semi-permanent colorants onto the lashes to make them appear darker and thicker. The color can last for several weeks (tinting) or longer (dyeing) depending on several factors, such as the health of lashes, type of dye, skill of beauty staff, color used, application of other eye cosmetics, exposure to the sun, type of detergent, and water temperature during washing. Although fashion trends tend to dictate followers, the dyeing and tinting may also be used by individuals with naturally light-colored lashes, canities (hair greying), and vitiligo (skin pigment loss). Due to potential eye damage, the authorities have tightened regulations on colorants for coloring eyelashes. For example, the U.S. Food and Drug Administration (USFDA) has not approved any natural or synthetic color additives,Citation17,Citation40 and the EU Commission has recently allowed only relatively few ingredients for professional use in accordance with the Scientific Committee on Consumer Safety (SCCS/1553/15): the oxidative hair dye substances toluene-2,5-diamine, p-aminophenol, 2-methylresorcinol, tetraaminopyrimidine sulfate, hydroxyethyl-p-phenylenediamine sulfate, and 2-amino-3-hydroxypyridine.
Eyelid cosmetic products and removers
Eyelid cosmetics are applied around the eyes to enhance the appearance by making them look big, bold, and attractive. The most popular products in this category are eyeliner and eyeshadow, and to enable them to be more easily wiped off, eye make-up remover products may be applied.
Kohl, eyeliner, and tattooing
Kohl (surma/al-kahal/kajal), one of the primitive forms of cosmetics for eyelid margins, is still popular in some parts of Africa and Asia. It is a blend of a natural lead compound, galena (lead sulphide), sulfur, antimony, carbon, iron, and chromium. Eyeliner, the modern form, is used to make the eyes bolder with illusive shapes and sizes. Based on fashion trends, it is applied outside the lash line, on the inner lid area closer to the eye, or along the waterline.Citation11,Citation43
Eyeliner can be found in the form of a cake, liquid, cream/gel, or pencil with different formulations. Cake eyeliner has similar ingredients to powdered eye shadow (Table S3) but contains surfactants for making a paste once water is added. Similar to its corresponding mascara, a wet brush is required for making and transferring the paste. Additionally, the formed pigmented film on eyelid margins is prone to smudging due to its water solubility. Although the cake form is still available, liquid eyeliner is a dominant substitute in today’s market. Liquid eyeliner formulations can be roughly categorized into two different types; water-resistant and waterproof. Intensely pigmented blends (or emulsions) in water or any other solvents represent the chemical backbone of the former compared to organic solvents or an anhydrous base in the latter case. These are applied using a fine (felt-tip) pen-like applicator or brush. Gel eyeliner has much in common with liquid eyeliner, except that it is more viscous, needs to be layered by a separate brush applicator from a pot container, holds up well and gives more control of the outcome by tending to go on sheer, and moves better with the delicate skin around the eye. Another product, pencil (or soft crayon) eyeliner, is popular because of its ease of application. Supplied in either a mechanical plastic or wooden case, it is a mixture of waxes (natural and synthetic), pigments, oils (mineral or vegetable), and emollients, such as lanolin derivatives.Citation39,Citation44,Citation45
Permanent eyeliner tattooing, also referred to as blepharopigmentation, has gained increasing attention in recent decades. It obviates the need for the daily application of eyeliner make-up and provides wearers with an enhanced dull eye. The most common pigment used in this process is black, but some others, such as navy blue, green, and brown, are also available. The micropigmentation technique is performed by implantation of dye into the superficial dermis layer at a constant depth using a tattoo machine.Citation40,Citation46,Citation47
Eyeshadow
Eyeshadow is applied to eyelids and below the eyebrows for creating depth and dimension to the eyes, making them and/or their color stand out and become more attractive. Compared to other facial make-up products, the formulation of eyeshadows requires special care to prevent scratches, infections, irritation, and toxic effects due to soft-thin skin type and proximity to the eyes.
A variety of products in the form of a paste, cream (or gel), stick (or crayon), pencil, liquid, and powder has been introduced to the market over recent decades (Table S3). Paste, the early form of eyeshadow, was popular before the Second World War. It mainly suffered from settling of its high portion of waxes or oils into eyelid creases, leading to the formation of lines. Although the release of emulsion creams offered a less greasy product, the water content necessitated preservatives against bacterial contamination and sealed packaging to reduce drying out. The anhydrous cream form, also termed cream-to-powder eyeshadow, was a highly effective alternative because it is transformed into a super soft powder following application. The high viscosity of the dehydrated emulsions assists with the uniform distribution of colorants into the cream base. However, their wearing time is short because of potential migration into the eyelid folds. In addition, these emulsions are prone to easily melt on the eyelids in hot weather. A variation on the cream-based shadow is the gel, where waxes are replaced with clay gelling agents for the thickening of oils. Among anhydrous eyeshadows, sticks and pencils have always been attractive to consumers because they can be easily carried around as well as their ease of application, are independent of brushes/applicators, and are available in long-wearing formulae. Crayon eyeshadow, their modified version, has gained even more popularity due to its wider diameter and softer property. Liquid eyeshadows are also considered convenient products to use. They are typically highly pigmented, set quickly, and sold in a sleek tube with a fluffy wand/doe foot applicator. Powder eyeshadows, either loose or pressed, are the most common form on the market. Both have similar ingredients, except that binders are added to the latter to hold the particles together.Citation39,Citation44 Recent modifications have offered baked eyeshadows, in which the prepared formula is heated in an oven/furnace rather than being pressed.
Eye make-up remover
Eye make-up remover enables applied cosmetics on the eye and surrounding area to be more easily wiped off. Chemically, such removers follow the general principle of solubility referred to as “like dissolves like”, in which substances with similar chemical characteristics are dissolved in each other.Citation8 Therefore, water alone is insufficient to effectively remove cosmetics containing lipophilic compounds,Citation11 requiring surfactants/emulsifiers in oil-based or oil-free formulations.Citation44 The remover comes in different forms, including oils, creams, balms, foams, sticks, micellar water, and saturated pads/wipes. The use of diverse raw materials in these products (Table S4) provides consumers with a variety of options based on the biocompatibility of the ingredients, effectiveness of the products, and convenience of application.Citation1,Citation45
Other products
Artificial eyelash, adhesive, and remover
These are not classed as cosmetic products under EC Regulation 1223/2009 but fall under the General Product Safety Regulation. Eyelash extensions and false eyelashes are used to create bold and attractive looks by modifying the length, volume, curl, and thickness of natural lashes. Extensions are individually adhered fibers in close proximity to the base of each natural lash using a special adhesive, whereas false (strip) ones are glued on top of them. These extensions are semi-permanent and last for several weeks, but false lashes are one-time use with the possibility of being reused 2–3 times. They are popular among those with healthy as well as damaged eyelashes resulting from negligent home care, inappropriate application of cosmetics, use of low-quality make-up products, and disease.Citation48
Both natural (e.g., silk, mink, human, and horsehair) and synthetic (e.g., polybutylene terephthalate) materials are used in the production of artificial eyelashes. The choice of adhesive depends essentially on the biological response of the wearer, type of chemicals used in false eyelashes, and the physical properties of glue after drying, such as good attachment and long retention.Citation40 Cyanoacrylate-based adhesives (Table S5), previously used for biomedical applications,Citation49 are widely marketed in response to the increasing global demand for eyelash treatment.Citation50 They are sold under different categories, such as surgical (medical), rubber latex, and sensitive/allergic (e.g., formaldehyde- and latex-free) glues. Each type of artificial eyelash has its own method of removal. For extensions, organic solvent-(liquid), cream-, gel-, and oil-based removers are available (Table S6). Besides, the natural oils such as olive, almond, and coconut often break down adhesive bonds and, therefore, are considered a safe and economical option. The oil-based removers and natural oils are also the method of choice for false eyelashes. However, specifically designed oil-free products, as well as steaming, are substitute methods for ensuring that lashes remain intact for future reuse.
In addition to the above-mentioned products, some others, such as eyelash growth-stimulating sera, primers, concealers, foundations, setting creams, face powders, bronzers, facial masks, and anti-aging gels/creams may be applied on the eyelids and periorbital area. Although each one has its own list of ingredients, they may have some in common with the popular eye cosmetics discussed above.
Undesired effects
A range of adverse effects on the ocular surface, tear film, and lids are associated with the use of eye make-up products. For example, mechanical trauma, tear film destabilization, immunological response, toxicity, and infection driven by ocular cosmetics may lead to inflammation,Citation11,Citation12 a key contributing factor to the vicious dry eye circle.Citation13 This process is serious in female populations because they are dominant in both presenting DED and consuming beauty products. The elderly, another sensitive population with frequent prevalence of DED, have also been targeted by cosmetic companies in recent years.Citation1 In youth, eye make-up products are also increasingly used to enhance natural beauty and simulate attractive characteristics.Citation51 The potential risk of utilizing eye cosmetics by teens to develop DED at a far earlier age is an intriguing area of research that could be explored in further studies.
Physical insults
Physical insult or mechanical trauma refers to any physical injury caused by a direct insult or blow to the eye, ranging from mild to severe. The well-known cosmetics-related corneal trauma among wearers involves poking the eye with a mascara applicator wand.Citation12 The use of a pin on the clumpiest sections of eyelashes after applying liquid mascara also risks mechanical trauma to the eye. Open wounds could be an entry point for pathogens and are an infection risk. The presence of fine nylon fibers in, for example, the base coat of two-step mascara for lash lengthening may irritate the ocular surface by being loosened and falling on it.Citation11 The direct application of eyeliner to the lid rim may block the orifices of the meibomian glands.Citation51,Citation52 Additionally, sharp pencil eyeliners can scratch the eye, although wooden cases produce less pressure than plastic ones.Citation39 The particles from eyeshadow can distribute on the tear film and may affect its stability along with increased debris formation risk.Citation52 Any changes in the volume, length (e.g., artificial lashes), and curl (e.g., lash lifting) of natural lashes can interfere with their functions with respect to debris-deflecting attributes and limiting tear evaporation.Citation53,Citation54 For instance, lengthening the eyelashes by the application of mascara or artificial lashes (or a combination of both) channels flow towards the ocular surface and causes stress.Citation54 Moreover, the natural lashes attached to extensions could fall off and cause irritation due to excessive force being applied during make-up removal by wiping (particularly waterproof make-up), inappropriate artificial lash removal, and/or poor sleeping posture (particularly on the abdomen).
Pathogenic insults
The microbiome is a collective term to describe a community of microorganisms, such as bacteria, fungi, and viruses, inhabiting a common niche such as the human body.Citation55 However, this term has been widely used for the inhabiting bacteria and distinguished from two others by the terms mycobiome and virome.Citation56 Several eye-associated microorganisms and parasites, with internal (e.g., lids, skin, nasopharynx, and birth canal) or external (e.g., water, soil, and atmosphere) origins impact ocular surface physiology both in health and disease.Citation57
Since the pioneering work of Keilty,Citation58 there has been increasing interest in identifying the structure and composition of the ocular surface bacterial inhabitants using different methods (Table S7). Despite technical challenges, the dominant bacterial genera present in a normal individual were shown to be Corynebacterium, Acinetobacter, Pseudomonas, Staphylococcus, Propionibacterium, and Streptococcus, co-occurring with the abundant Bacillus.Citation59 In contrast to bacteria, few studies have investigated fungalCitation60–63 and viralCitation60,Citation64,Citation65 communities of the human eyes. Additionally, the interactions between bacteriophages and mucosal surfacesCitation66,Citation67 for eye health and disease is an interesting subject that requires further research.
The bacterial profile of the ocular surface was shown to be affected by dry eye in several studies (). However, there was no general agreement on the prevalence of isolates due to differences in sample size, detection method (culture vs. 16S rRNA gene analysis), and dry eye diagnostic criteria.Citation68 It was hypothesized that changes in the quantity and quality of DED patients’ tear films, preventing normal tear turnover, would alter the spectrum of the ocular surface flora.Citation69 On the other hand, the microbial components such as ligands (e.g., flagellin A and lipopolysaccharide) and lipoteichoic acids influence the production of mucin, particularly MUC2 and MUC5A, resulting in epithelial stress and activation of adaptive immunity.Citation70 Therefore, a better understanding of microbial communities’ distribution on the ocular surface could be of substantial significance in the treatment of DED.Citation71
Table 1. Changes in bacterial flora on human ocular surface of non-DED and DED subjects
Eyes, particularly dry eyes, are at the risk of harmful microbial infection from eye cosmetics.Citation53,Citation76 These products provide a good medium for their growth, and contamination is facilitated by mishandling during production, inadequate preservatives, poor personal hygiene, long-term usage, multiple consumers, and product modification by users, such as adding water to mascara.Citation77 Among pathogens, significant attention has been paid to bacteria (), and scientists have been able to, for example, isolate Bacillus, which is hazardous to human health.Citation78 As shows, Bacillus has not been identified on non-DED individuals; however, it was among the only identified species in DED subjectsCitation73 (). Andersson, et al.Citation75 identified Bacillus as a bacterial biomarker for patients with DED. It can be seen from that it has been screened in different eye make-up products in several studies. In contrast, little has been done for fungalCitation76,Citation79-81 contamination and, to our knowledge, nothing for viral contamination.
Table 2. Bacterial contamination of commercially available eye makeup products
The wearers of eye cosmetics, particularly oil-based products, tend to present higher rates of demodex mites.Citation90 This common parasitosis within eyelash follicles is responsible for duct blockage.Citation51 These mites are highly prevalent in the older population with dry eye and specifically manifest symptoms of itching and cylindrical dandruff.Citation91
Chemical insults
Many hazardous cosmetic ingredients and their effects on the human ocular surfaceCitation11,Citation12,Citation17,Citation18 and body (e.g.,Citation6–9) have been previously reviewed. Among the mechanisms behind chemical insults, inflammatory responses play a central role. DED could develop secondary to inflammatory response.Citation92
The ocular immunologic defense encompasses innate, adaptive, and mucosal components. The latter contains conjunctiva- and lacrimal drainage-associated lymphoid tissue, together forming the ocular surface-associated lymphoid tissue, part of a larger common secretory immune system from the gastrointestinal-respiratory-genitourinary tracts. The ocular surface immune system is closely regulated and carefully controlled by the innate and adaptive immune responses.Citation27,Citation93 The cosmetics-induced immune response in the eye primarily affects the eyelid, tear film, conjunctiva, and cornea.Citation94
The eyelid, similar to skin across the body, may develop contact allergy (a delayed-type hypersensitivity; type IV) when exposed to a sufficient concentration of an allergen, such as some preservatives, fragrances, antioxidants, emollients, resins, pearlescent additives, and pigments containing nickel. Following re-exposure, symptoms of irritant or allergic contact dermatitis, including rash, blisters, wheals, urticarial, itchy, and burning skin appear within 24–72 h.Citation7,Citation44,Citation95,Citation96 Mechanistically, it consists of afferent (also termed induction or sensitization) phase and efferent (elicitation or challenge) phases. During the first step, skin dendritic cells are activated by a contact allergen and maturated before migrating to local lymph node(s) to stimulate antigen-specific T cells. During the second stage, subsequent encounters with the same chemical trigger the recruitment of the primed T cells to the affected location, followed by a local antigen-specific response. Because typically small compounds (<500 Da in size) can induce contact dermatitis, the process is believed to be mediated by hapten/carrier peptide complexes.Citation95 The allergen source of initial or subsequent exposures might be directly from eye cosmetics or indirectly from other products such as hair/eyebrow dyes, eyelash curlers, make-up removers, facial cleansers, shampoos/conditioners (rinsed off during showers), make-up sponges, and allergens transferred from the hands.Citation97
In addition to cell-mediated allergic reactions (Type IV), the eyelids may manifest immediate hypersensitivity (Type I) in the form of immunological contact urticaria after exposure to some hair dyes, antimicrobial agents/preservatives, fragrances, and plant- or animal-derived cosmetic ingredients.Citation98 The mechanism involves the formation of a specific IgE molecule-antigen complex on the mast cell surface at the site of exposure, which results in redness and edema along with extracutaneous symptoms (e.g., conjunctivitis) within 30–60 min (or exceptionally later) due to the release of histamine. Patients with atopic dermatitis are prone to such an immunological reaction.Citation99
Externally applied eye make-up products could migrate across the eyelid margin onto the ocular surface.Citation100 Such contamination is higher among make-up users who use eye drops at the same time.Citation101 Within the tear film, one mechanism suggests that the pro-inflammatory effects are driven by hyperosmolarity after the accumulation of hydrophilic components within the aqueous-mucin phase.Citation100 However, this suggestion was based on benzalkonium chloride, an abandoned chemical in eye make-up products today.Citation102 For the cornea and conjunctiva, the drifted make-up materials may cause irritation. Although it is not well understood, the mechanism may involve eye irritation induced by various chemical classes: cell membrane lysis, saponification, coagulation, and actions on macromolecules.Citation103 It has also been suggested that the migrated ingredients may provide an additional entry point to the DED vicious circle by activating ocular surface inflammatory pathways.Citation12
The immune system affects and partly controls the neuroendocrine network of tear secretion. The neuronal and hormonal (androgens mainly) regulation acts through the hypothalamic-pituitary-gonadal axis for the production of tears and their contents (e.g., immunoglobulins, lymphocytes, and proteins). Therefore, any disruption of the immuno-neuro-hormonal system function may result in tear film changes with consequences of DED.Citation104 For instance, the secretion of the tear film’s lipid layer may be interrupted after exposure of the meibomian gland to, for example, retinoic acid derivates, the key components for anti-aging products around the eye.Citation105 Mechanistic studies have revealed that the androgen receptor is suppressed at mRNA and protein levels,Citation106,Citation107 and retinol dehydrogenase-4 is inhibitedCitation108 by them.
The chronic inflammatory infiltrate (mostly lymphocytes and neutrophils) has been seen in accumulated black pigments containing high levels of lead in the lacrimal sac and surrounding tissue in several kohl consumers.Citation109 In other studies, kohl use was shown to be associated with high blood lead concentration and low hemoglobin levels.Citation110,Citation111 Lead, similar to other heavy metals, is toxicCitation6,Citation112; however, no corneal toxicity in humans has been linked to it.Citation11 According to EC Regulation 1223/2009, lead and its compounds are prohibited in cosmetics.
Although some ingredients, such as preservatives, in cosmetics are known to adversely affect biological systems,Citation9 particularly the eyes,Citation11 the lack of evidence and/or their very low levels in final products have not convinced regulatory agencies to ban them. For example, parabens (methylparaben, ethylparaben), phenoxyethanol, and chlorphenesin have been reported to be toxic to immortalized human meibomian gland epithelial cells.Citation113 In addition, methylparaben and ethylparaben have been associated with the signs and symptoms of DED.Citation114
Conclusions and future work
A range of adverse effects on the ocular surface, tear film, and lid are associated with the use of eye make-up products. For example, physical, pathogenic, and chemical insults driven by these products may lead to inflammation. Dry eye, a multifactorial disease, could develop secondary to the inflammatory response. This disease is most prominent in women, a dominant population both in presenting DED and consuming beauty products. The elderly, a sensitive population with a frequent prevalence of DED, are also at risk owing to their increased consumption of such products. Although the regulatory agencies are continually reviewing ingredients, it is also the responsibility of the manufacturers to ensure the clinical safety of their formulations’ constituents. On the other hand, eye care practitioners must be updated about newly released products, and consumers/patients should increase their awareness. Considering the widespread use of these products, further research on a broader range of eye cosmetics with long-term exposure and potential mixture toxicity would assist in establishing more effective safety guidelines. There is an apparent lack of studies on DED and eye make-up products.
Author contributions
Conceptualization and Writing – Original Draft Preparation: M.Y. (Toxicologist), Writing – Review: K.B.P.E (Chemist), T.P.U. (Ophthalmologist).
Supplemental Material
Download PDF (203.1 KB)Acknowledgments
The authors thank Sara Tellefsen for her assistance in drawing the illustrations.
Disclosure statement
No potential conflict of interest was reported by the author(s)
Supplementary materials
Supplemental data for this article can be accessed on the publisher’s website.
Additional information
Funding
References
- Winter R. A consumer’s dictionary of cosmetic ingredients: complete information about the harmful and desirable ingredients found in cosmetics and cosmeceuticals. New York (NY): Harmony; 2009.
- Ramshida A, Manikandan K. Cosmetics usage and its relation to sex, age and marital status. Int J Soc Sci Res. 2014;3:46–55.
- Davis G, Hall M. The makeup artist handbook: techniques for film, television, photography, and theatre. Amsterdam (The Netherlands): Routledge; 2012.
- Scanlon JR, Scanlon J. The gender and consumer culture reader. New York (NY): NYU Press; 2000.
- Hamilton T, de Gannes GC. Allergic contact dermatitis to preservatives and fragrances in cosmetics. dermatitis. 2011;16:1–4.
- Okereke J, Udebuani A, Ezeji E, Obasi K, Nnoli M. Possible health implications associated with cosmetics: a review. Sci J Pub Health. 2015;3(5):58. doi:https://doi.org/10.11648/j.sjph.s.2015030501.21.
- Zulaikha S, Norkhadijah S, Praveena S. Hazardous ingredients in cosmetics and personal care products and health concern: a review. Pub Health Res. 2015;5:7–15.
- Banerjee K. Cosmetics–care, concerns and caution. Int J Innovations Pharm Sci. 2018;6:14–31.
- Khan AD, Alam MN. Cosmetics and their associated adverse effects: a review. J Appl Pharm Sci Res. 2019;2(1):1–6.
- Jones AL, Russell R, Ward R. Cosmetics alter biologically-based factors of beauty: evidence from facial contrast. Evol Psychol. 2015;13(1):147470491501300113. doi:https://doi.org/10.1177/147470491501300113.
- Ng A, Evans K, North RV, Jones L, Purslow C. Impact of eye cosmetics on the eye, adnexa, and ocular surface. Eye Cont Lens. 2016;42(4):211–20. doi:https://doi.org/10.1097/ICL.0000000000000181.
- Wang MT, Craig JP. Investigating the effect of eye cosmetics on the tear film: current insights. Clin Optom. 2018;10:33. doi:https://doi.org/10.2147/OPTO.S150926.
- Bron AJ, de Paiva CS, Chauhan SK, Bonini S, Gabison EE, Jain S, Knop E, Markoulli M, Ogawa Y, Tfos PV. DEWS II pathophysiology report. Ocul Surf. 2017;15:438–510.
- Stapleton F, Alves M, Bunya VY, Jalbert I, Lekhanont K, Malet F, Na K-S, Schaumberg D, Uchino M, Vehof J. Tfos dews ii epidemiology report. Ocul Surf. 2017;15(3):334–65. doi:https://doi.org/10.1016/j.jtos.2017.05.003.
- Barabino S, Labetoulle M, Rolando M, Messmer EM. Understanding symptoms and quality of life in patients with dry eye syndrome. Ocul Surf. 2016;14(3):365–76. doi:https://doi.org/10.1016/j.jtos.2016.04.005.
- McDonald M, Patel DA, Keith MS, Snedecor SJ. Economic and humanistic burden of dry eye disease in Europe, North America, and Asia: a systematic literature review. Ocul Surf. 2016;14(2):144–67. doi:https://doi.org/10.1016/j.jtos.2015.11.002.
- Coroneo MT, Rosenberg ML, Cheung LM. Ocular effects of cosmetic products and procedures. Ocul Surf. 2006;4(2):94–102. doi:https://doi.org/10.1016/S1542-0124(12)70031-9.
- Tang K, Lu S-Y, Ma D-L, Leung C-H, Lee -S-S, Lin S-W, Wang H-M D. A review on common ingredients of periocular cosmetics and their hazards. Curr Org Chem. 2015;19(1):30–38. doi:https://doi.org/10.2174/1385272819666141107225726.
- Sundaram V, Barsam A, Barker L, Khaw PT. Training in ophthalmology. New York: Oxford University Press; 2016.
- Dutton JJ, Gayre GS, Proia AD. Diagnostic atlas of common eyelid diseases. Boca Raton (FL): CRC Press; 2007.
- Tintinalli JE, Stapczynski JS, Ma OJ, Cline D, Meckler GD, Yealy DM. Tintinalli’s emergency medicine: a comprehensive study guide. New York (NY): McGraw-Hill Education New York; 2016.
- Mustardé JC, Whitaker LA. Repair and reconstruction in the orbital region. A Practical Guide. Plas Recon Sur. 1981;67(5):692. doi:https://doi.org/10.1097/00006534-198105000-00024.
- Gunasegaran J. Textbook of histology and practical guide. New Delhi (India): Elsevier Health Sciences; 2014.
- Jordan D, Mawn L, Anderson RL. Surgical anatomy of the ocular adnexa: a clinical approach. New York (NY): Oxford University Press; 2012.
- Jeyalatha MV, Qu Y, Liu Z, Ou S, He X, Bu J, Li S, Reinach PS, Liu Z, Li W. Function of meibomian gland: contribution of proteins. Exp Eye Res. 2017;163:29–36. doi:https://doi.org/10.1016/j.exer.2017.06.009.
- McCulley JP, Shine WE. Meibomian gland function and the tear lipid layer. Ocul Surf. 2003;1(3):97–106. doi:https://doi.org/10.1016/S1542-0124(12)70138-6.
- Holland EJ, Mannis MJ, Lee WB. Ocular surface disease: cornea, conjunctiva and tear film. London (UK): Elsevier Health Sciences; 2013.
- Pavan-Langston D. Manual of ocular diagnosis and therapy. Philadelphia (PA): Lippincott Williams & Wilkins; 2008.
- Sridhar MS. Anatomy of cornea and ocular surface. Indian J Ophthalmol. 2018;66:190.
- Yazdani M, Kbp E, Rootwelt H, Shahdadfar A, Øa U, Utheim TP. Tear metabolomics in dry eye disease: a review. Int J Mol Sci. 2019;20(15):3755. doi:https://doi.org/10.3390/ijms20153755.
- Paulsen F. The human nasolacrimal ducts. Berlin (Germany): Springer Science & Business Media; 2003.
- Nelson JD, Helms H, Fiscella R, Southwell Y, Hirsch JD. A new look at dry eye disease and its treatment. Adv Ther. 2000;17(2):84–93. doi:https://doi.org/10.1007/BF02854841.
- Craig JP, Nichols KK, Akpek EK, Caffery B, Dua HS, Joo C-K, Liu Z, Nelson JD, Nichols JJ, Tsubota K, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–83. doi:https://doi.org/10.1016/j.jtos.2017.05.008.
- Tsubota K, Yokoi N, Shimazaki J, Watanabe H, Dogru M, Yamada M, Kinoshita S, Kim H-M, Tchah H-W, Hyon JY. New perspectives on dry eye definition and diagnosis: a consensus report by the Asia dry eye society. Ocul Surf. 2017;15(1):65–76. doi:https://doi.org/10.1016/j.jtos.2016.09.003.
- Nelson JD, Craig JP, Akpek EK, Azar DT, Belmonte C, Bron AJ, Clayton JA, Dogru M, Dua HS, Foulks GN. TFOS DEWS II introduction. Ocul Surf. 2017;15(3):269–75. doi:https://doi.org/10.1016/j.jtos.2017.05.005.
- Ding C, Tóth-Molnár E, Wang N, Lacrimal Gland ZL. Ocular surface, and dry eye. J Ophthalmol. 2016;2016. doi:https://doi.org/10.1155/2016/7397694.
- Baudouin C, Irkeç M, Messmer EM, Benítez‐del‐Castillo JM, Bonini S, Figueiredo FC, Geerling G, Labetoulle M, Lemp M, Rolando M. Clinical impact of inflammation in dry eye disease: proceedings of the ODISSEY group meeting. Acta Ophthalmol. 2018;96(2):111–19. doi:https://doi.org/10.1111/aos.13436.
- Clayton JA. Dry eye. Curr Ophthalmol Rep. 2018;378:2212–23.
- Baki G, Alexander KS. Introduction to cosmetic formulation and technology. New Jersey (USA): John Wiley & Sons; 2015.
- Draelos ZD. Cosmetics and dermatologic problems and solutions. Boca Raton (FL): CRC press; 2011.
- Barel AO, Paye M, Maibach HI. Handbook of cosmetic science and technology. Boca Raton (FL): CRC press; 2014.
- Draelos ZD. Cosmetic dermatology: products and procedures. UK: John Wiley & Sons; 2016.
- Diamandopoulos AA. Organic and inorganic cosmetics in the preclassical Eastern Mediterranean. Int J Dermatol. 1996;35(10):751–56. doi:https://doi.org/10.1111/j.1365-4362.1996.tb00659.x.
- Draelos ZD. Special considerations in eye cosmetics. Clin in Dermatol. 2001;19(4):424–30. doi:https://doi.org/10.1016/S0738-081X(01)00204-8.
- Begoun P. The complete beauty bible: the ultimate guide to smart beauty. Pennsylvania: Rodale Inc; 2004.
- Roenigk RK, Roenigk HH. Roenigk & Roenigk’s dermatologic surgery: principles and practice. Boca Raton (FL): CRC press; 1996.
- Goldberg H, Berger Y, Bassat IB, Barequet I. Inadvertent corneal pigmentation following cosmetic blepharopigmentation. Am J Ophthalmol Case Rep. 2018;12:52–54. doi:https://doi.org/10.1016/j.ajoc.2018.09.002.
- Connor J, Godfrey S, Milsom G. BTEC national beauty therapy sciences. Oxford (UK): Heinemann; 2004.
- Vernengo AJ. Adhesive materials for biomedical applications. Adhes Appl Prop. 2016;6:111–33.
- Lindström I, Suojalehto H, Henriks-Eckerman M-L, Suuronen K. Occupational asthma and rhinitis caused by cyanoacrylate-based eyelash extension glues. Occup Med. 2013;63(4):294–97. doi:https://doi.org/10.1093/occmed/kqt020.
- Murube J. Ocular cosmetics in modern times. Ocul Surf. 2013;2(11):60–64. doi:https://doi.org/10.1016/j.jtos.2013.01.005.
- Guillon J-P, Layer AL. Observation, differential diagnosis, and classification. Adv Exp Med Biol. 1998;438:309–13.
- O’Dell LE, Sullivan AG, Periman LM. Suffering for beauty: harmful ingredients and trends in cosmetics. Adv Ocul Care. 2016:12–16.
- Amador GJ, Mao W, DeMercurio P, Montero C, Clewis J, Alexeev A, Hu DL. Eyelashes divert airflow to protect the eye. J R Soc Interface. 2015;12(105):20141294. doi:https://doi.org/10.1098/rsif.2014.1294.
- Shivaji S. Connect between gut microbiome and diseases of the human eye. J Biosci. 2019;44(5):110. doi:https://doi.org/10.1007/s12038-019-9931-1.
- Trujillo-Vargas CM, Schaefer L, Alam J, Pflugfelder SC, Britton RA, de Paiva CS. The gut-eye-lacrimal gland-microbiome axis in Sjögren Syndrome. Ocul Surf. 2020;18(2):335–44. doi:https://doi.org/10.1016/j.jtos.2019.10.006.
- Ozkan J, Willcox MD. The ocular microbiome: molecular characterisation of a unique and low microbial environment. Curr Eye Res. 2019;44(7):685–94. doi:https://doi.org/10.1080/02713683.2019.1570526.
- Keilty RA. The bacterial flora of the normal conjunctiva with comparative nasal culture study. Am J Ophthalmol. 1930;13(10):876–79. doi:https://doi.org/10.1016/S0002-9394(30)92437-3.
- Delbeke H, Younas S, Casteels I, Joossens M. Current knowledge on the human eye microbiome: a systematic review of available amplicon and metagenomic sequencing data. Acta Ophthalmol. 2020;99(1):16–25.
- Wen X, Miao L, Deng Y, Bible PW, Hu X, Zou Y, Liu Y, Guo S, Liang J, Chen T. The influence of age and sex on ocular surface microbiota in healthy adults. Invest Ophthalmol Vis Sci. 2017;58(14):6030–37. doi:https://doi.org/10.1167/iovs.17-22957.
- Sai Prashanthi G, Jayasudha R, Chakravarthy SK, Padakandla SR, SaiAbhilash CR, Sharma S, Bagga B, Murthy SI, Garg P, Shivaji S. Alterations in the ocular surface fungal microbiome in fungal keratitis patients. Microorganisms. 2019;7(9):309. doi:https://doi.org/10.3390/microorganisms7090309.
- Shivaji S, Jayasudha R, Prashanthi GS, Chakravarthy SK, Sharma S. The human ocular surface fungal microbiome. Invest Ophthalmol Vis Sci. 2019;60(1):451–59. doi:https://doi.org/10.1167/iovs.18-26076.
- Wu TG, Mitchell BM, Carothers TS, Coats DK, Brady-mccreery KM, Paysse EA, Wilhelmus KR. Molecular analysis of the pediatric ocular surface for fungi. Curr Eye Res. 2003;26(1):33–36. doi:https://doi.org/10.1076/ceyr.26.1.33.14253.
- Doan T, Akileswaran L, Andersen D, Johnson B, Ko N, Shrestha A, Shestopalov V, Lee CS, Lee AY, Van Gelder RN. Paucibacterial microbiome and resident DNA virome of the healthy conjunctiva. Invest Ophthalmol Vis Sci. 2016;57(13):5116–26. doi:https://doi.org/10.1167/iovs.16-19803.
- Lee AY, Akileswaran L, Tibbetts MD, Garg SJ, Van Gelder RN. Identification of torque teno virus in culture-negative endophthalmitis by representational deep DNA sequencing. Ophthalmol. 2015;122(3):524–30. doi:https://doi.org/10.1016/j.ophtha.2014.09.001.
- Barr JJ, Auro R, Furlan M, Whiteson KL, Erb ML, Pogliano J, Stotland A, Wolkowicz R, Cutting AS, Doran KS. Bacteriophage adhering to mucus provide a non–host-derived immunity. Proc Natl Acad Sci USA. 2013;110(26):10771–76. doi:https://doi.org/10.1073/pnas.1305923110.
- Barr JJ. A bacteriophages journey through the human body. Immunol Rev. 2017;279(1):106–22. doi:https://doi.org/10.1111/imr.12565.
- Li Z, Gong Y, Chen S, Li S, Zhang Y, Zhong H, Wang Z, Chen Y, Deng Q, Jiang Y. Comparative portrayal of ocular surface microbe with and without dry eye. J Microbiol. 2019;57(11):1025–32. doi:https://doi.org/10.1007/s12275-019-9127-2.
- Hori Y, Maeda N, Sakamoto M, Koh S, Inoue T, Tano Y. Bacteriologic profile of the conjunctiva in the patients with dry eye. Am J Ophthalmol. 2008;146(5):729–734. e721. doi:https://doi.org/10.1016/j.ajo.2008.06.003.
- Miller D, Iovieno A. The role of microbial flora on the ocular surface. Curr Opin Allergy Clin Immunol. 2009;9(5):466–70. doi:https://doi.org/10.1097/ACI.0b013e3283303e1b.
- Grzybowski A, Brona P, Kim SJ. Microbial flora and resistance in ophthalmology: a review. Graefes Arch Clin Exp Ophthalmol. 2017;255(5):851–62. doi:https://doi.org/10.1007/s00417-017-3608-y.
- Seal D, McGill J, Mackie I, Liakos G, Jacobs P, Goulding N. Bacteriology and tear protein profiles of the dry eye. Br J Ophthalmol. 1986;70(2):122–25. doi:https://doi.org/10.1136/bjo.70.2.122.
- Graham JE, Moore JE, Jiru X, Moore JE, Goodall EA, Dooley JS, Hayes VE, Dartt DA, Downes CS, Moore TC. Ocular pathogen or commensal: a PCR-based study of surface bacterial flora in normal and dry eyes. Invest Ophthalmol Vis Sci. 2007;48(12):5616–23. doi:https://doi.org/10.1167/iovs.07-0588.
- Willis KA, Postnikoff CK, Freeman AB, Rezonzew G, Nichols KK, Gaggar A, Lal CV. The closed eye harbors a unique microbiome in dry eye disease. medRxiv. 2020.
- Andersson J, Vogt JK, Dalgaard MD, Pedersen O, Holmgaard K, Heegaard S. Ocular surface microbiota in patients with aqueous tear-deficient dry eye. Ocul Surf. 2020;19:210–217.
- Pack LD, Wickham MG, Enloe RA, Hill DN. Microbial contamination associated with mascara use. Optometry J Am Optom Assoc. 2008;79(10):587–93. doi:https://doi.org/10.1016/j.optm.2008.02.011.
- Wilson LA, Ahearn DG. Pseudomonas-induced corneal ulcers associated with contaminated eye mascaras. Am J Ophthalmol. 1977;84(1):112–19. doi:https://doi.org/10.1016/0002-9394(77)90334-8.
- Pitt T, McClure J, Parker M, Amezquita A, McClure P. Bacillus cereus in personal care products: risk to consumers. Int J Cosmet Sci. 2015;37(2):165–74. doi:https://doi.org/10.1111/ics.12191.
- Baqer Y, Mohammed B, Obaid K, Hlail Z. CFS of lactobacillus: a natural agent against bacterial contamination of cosmetics tools. Inter J Adv Biol Res. 2014;4:258–64.
- Dadashi L, Dehghanzadeh R. Investigating incidence of bacterial and fungal contamination in shared cosmetic kits available in the women beauty salons. Health Promot Perspect. 2016;6(3):159. doi:https://doi.org/10.15171/hpp.2016.25.
- El-Bazza Z, El-Tablawy S, Hashem A, Nasser H. Evaluation of the microbial contamination of some eye-make up products before and after use. Biohealth Sci Bullet Malysia. 2009;1:68–75.
- Dawson NL, Reinhardt DJ. Microbial flora of in-use, display eye shadow testers and bacterial challenges of unused eye shadows. Appl Environ Microbiol. 1981;42(2):297–302. doi:https://doi.org/10.1128/aem.42.2.297-302.1981.
- Abdelaziz AA, Ashour M, Hefni H, El‐Tayeb O. Microbial contamination of cosmetics and personal care items in Egypt—eye shadows, mascaras and face creams. J Clin Pharm Ther. 1989;14(1):21–28. doi:https://doi.org/10.1111/j.1365-2710.1989.tb00217.x.
- Abdelaziz A, Alkofahi A. Microbiological profile of selected samples of” Al-Kohl” eye cosmetics in northern Jordanian provinces before and after use. Zentralbl Bakteriol Mikrobiol Hyg B. 1989;187:244–53.
- Guleria A. Isolation and identification of bacteria from different cosmetic samples and to check antimicrobial activity of antibiotics on bacteria isolated. Int J Scientific Res. 2014;3:462–65. doi:https://doi.org/10.15373/22778179/FEB2014/153.
- Nandi S, Mandal S. Bacteriological profiling of commercially available eye cosmetics and their antibiotic susceptibility pattern. Transl Biomed. 2016;7:3. doi:https://doi.org/10.21767/2172-0479.100080.
- Eldesoukey R, Alqhtani B, Alqhtani A, Alqhtani A, Alqhtani A. Comparative microbiological study between traditional and modern cosmetics in Saudi Arabia. Enz Eng. 2016;5(146):2. doi:https://doi.org/10.4172/2329-6674.1000146.
- Bashir A, Lambert P. Microbiological study of used cosmetic products: highlighting possible impact on consumer health. J Appl Microbiol. 2019;128(2):598–605. doi:https://doi.org/10.1111/jam.14479.
- Noor A, Rabih W, Alsaedi A, Al-Otaibi M, Alzein M, Alqireawi Z, Mobarki K, AlSharif R, Alfaran H. Isolation and identification of microorganisms in selected cosmetic products tester. Afr J Microbiol Res. 2020;14(9):536–40. doi:https://doi.org/10.5897/AJMR2020.9399.
- Irfan S. Meibomian gland dysfunction. Pak J Ophthalmol. 2019;35(1):63–72.
- Cheng AM, Hwang J, Dermer H, Galor A. Prevalence of ocular demodicosis in an older population and its association with symptoms and signs of dry eye. Cornea. 2020;40(8):995–1001.
- Javadi M-A, Feizi S. Dry eye syndrome. J Ophthalmic Vis Res. 2011;6:192–98.
- Zhang X, Qu Y, He X, Ou S, Bu J, Jia C, Wang J, Wu H, Liu Z, Li W. Dry eye management: targeting the ocular surface microenvironment. Int J Mol Sci. 2017;18(7):1398. doi:https://doi.org/10.3390/ijms18071398.
- Norris MR, Bielory L. Cosmetics and ocular allergy. Curr Opin Allergy Clin Immunol. 2018;18(5):404–10. doi:https://doi.org/10.1097/ACI.0000000000000474.
- Vukmanović S, Sadrieh N. Skin sensitizers in cosmetics and beyond: potential multiple mechanisms of action and importance of T-cell assays for in vitro screening. Crit Rev Toxicol. 2017;47(5):422–39. doi:https://doi.org/10.1080/10408444.2017.1288025.
- Adams RM, Maibach HI, Clendenning W, Fisher A, Jordan W, Kanof N, Larsen W, Mitchell J, Rudner E, Schorr W. A five-year study of cosmetic reactions. J Am Acad Dermatol. 1985;13(6):1062–69. doi:https://doi.org/10.1016/S0190-9622(85)70258-7.
- Zirwas MJ. Contact dermatitis to cosmetics. Clin Rev Allergy Immunol. 2019;56(1):119–28. doi:https://doi.org/10.1007/s12016-018-8717-9.
- Goossens A. Contact-allergic reactions to cosmetics. J Allergy (Cairo). 2011;2011.
- Verhulst L, Goossens A. Cosmetic components causing contact urticaria: a review and update. Cont Dermatit. 2016;75(6):333–44. doi:https://doi.org/10.1111/cod.12679.
- Malik A, Claoué C. Transport and interaction of cosmetic product material within the ocular surface: beauty and the beastly symptoms of toxic tears. Cont Lens Anterior Eye. 2012;35(6):247–59. doi:https://doi.org/10.1016/j.clae.2012.07.005.
- Goto T, Zheng X, Gibbon L, Ohashi Y. Cosmetic product migration onto the ocular surface: exacerbation of migration after eyedrop instillation. Cornea. 2010;29(4):400–03. doi:https://doi.org/10.1097/ICO.0b013e3181bd4756.
- Geis PA, Steinberg D. Response to: Malik and Claoue–transport and interaction of cosmetic product material within the ocular surface: beauty and the beastly symptoms of toxic tears. Cont Lens Anterior Eye. 2013;36(3):151. doi:https://doi.org/10.1016/j.clae.2013.01.008.
- Scott L, Eskes C, Hoffmann S, Adriaens E, Alepée N, Bufo M, Clothier R, Facchini D, Faller C, Guest R. A proposed eye irritation testing strategy to reduce and replace in vivo studies using bottom–up and top–down approaches. Toxicol In Vitro. 2010;24(1):1–9. doi:https://doi.org/10.1016/j.tiv.2009.05.019.
- Niederkorn JY, Dana MR. Immune system and the eye. In: Yorio T, Clark AF, Wm B, editors. Ocular therapeutics: eye on new discoveries. New York (NY): Elsevier; 2008. p. 199–237.
- Knop E, Knop N, Millar T, Obata H, Sullivan DA. The international workshop on meibomian gland dysfunction: report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Invest Ophthalmol Vis Sci. 2011;52(4):1938–78. doi:https://doi.org/10.1167/iovs.10-6997c.
- Ubels JL, Veenstra E, Ditlev J, Ingersoll K. Interactions of testosterone and all-trans retinoic acid in regulation of androgen receptor expression in rat lacrimal gland. Exp Eye Res. 2003;77(6):741–48. doi:https://doi.org/10.1016/j.exer.2003.07.006.
- Ubels JL, Wertz JT, Ingersoll KE, Jackson IRS, Aupperlee MD. Down-regulation of androgen receptor expression and inhibition of lacrimal gland cell proliferation by retinoic acid. Exp Eye Res. 2002;75(5):561–71. doi:https://doi.org/10.1006/exer.2002.2054.
- Karlsson T, Vahlquist A, Kedishvili N, Törmä H. 13-cis-retinoic acid competitively inhibits 3α-hydroxysteroid oxidation by retinol dehydrogenase RoDH-4: a mechanism for its anti-androgenic effects in sebaceous glands? Biochem Biophys Res Commun. 2003;303(1):273–78. doi:https://doi.org/10.1016/S0006-291X(03)00332-2.
- Hidayat A, Weatherhead R, al-Rajhi A, Johnson F. Conjunctival and lacrimal sac pigmentation by kohl (eyeliner). Br J Ophthalmol. 1997;81(5):418–418. doi:https://doi.org/10.1136/bjo.81.5.415d.
- Al-Ashban R, Aslam M, Kohl SA. (surma): a toxic traditional eye cosmetic study in Saudi Arabia. Public Health. 2004;118(4):292–98. doi:https://doi.org/10.1016/j.puhe.2003.05.001.
- Goswami K. Eye cosmetic ‘surma’: hidden threats of lead poisoning. Indian J Clin Biochem. 2013;28(1):71–73. doi:https://doi.org/10.1007/s12291-012-0235-6.
- Safavi S, Najarian R, Rasouli-Azad M, Masoumzadeh S, Ghaderi A, Eghtesadi R. A narrative review of heavy metals in cosmetics; health risks. Int J Pharm Sci Res. 2019;11:182–90.
- Wang J, Liu Y, Kam WR, Li Y, Sullivan DA. Toxicity of the cosmetic preservatives parabens, phenoxyethanol and chlorphenesin on human meibomian gland epithelial cells. Exp Eye Res. 2020;108057. doi:https://doi.org/10.1016/j.exer.2020.108057.
- Pontelli RC, Rocha BA, Garcia DM, Pereira LA, Souza MC, Barbosa JF, Rocha EM. Endocrine disrupting chemicals associated with dry eye syndrome. Ocul Surf. 2020;18(3):487–93. doi:https://doi.org/10.1016/j.jtos.2020.01.001.