
Abstract
Objective: To explore whether a primary health care (PHC) health promotion programme reaches and engages socioeconomically vulnerable groups in a community to the same extent as higher socioeconomic groups.
Design: Comparison of level of engagement and lifestyle improvements stratified by socioeconomic vulnerability level.
Setting: Hisingen PHC catchment area (130,000 inhabitants) Gothenburg, Sweden.
Participants: Men and women aged 18–79, visiting any of the eight public PHC centres during an eight-month period 2007–2008, were presented with a short intervention health questionnaire and offered a health dialogue with a nurse, including a health profile, p-glucose and blood pressure check. Participants were classified according to four socioeconomic vulnerability factors: education, employment, ethnicity and living situation.
Results: Out of 3691 participants, 27% had low education (Hisingen community level 23%), 18% were unemployed (community level 22%), and 16% were born outside Scandinavia (community level 22%). At the one-year follow-up, 2121 (57%) attended. At baseline, 3% of the individuals in the sample had three out of four socioeconomic vulnerability factors, 17% had two vulnerability factors, 43% had one vulnerability factor, and 37% had no vulnerability factors. Improved biological markers were seen in all vulnerability groups (1–3) and odds ratios for improvement were significantly higher in the most socioeconomically vulnerable group for smoking and stress compared to the group with no vulnerability factors.
Conclusion: Socioeconomically vulnerable groups were reached and lifestyle changes were accomplished to the same extent as in the higher socioeconomic groups in a PHC lifestyle intervention programme.
Primary care plays a major part in prevention of chronic diseases. However, non-pharmacological primary and secondary prevention is often less successful, especially concerning socioeconomically vulnerable groups.
The health promoting intervention programme “Pro-Health” reached and engaged socioeconomically vulnerable groups.
Participants from the socioeconomically vulnerable groups had comparable odds for lifestyle improvements after one year, compared to participants without vulnerability factors.
KEY POINTS
Introduction
International public health research clearly indicates the importance of lifestyle factors for the health status of the population.[Citation1] Also in Sweden, smoking, hazardous drinking, sedentary living and unhealthy eating habits are the greatest contributors to overall burden of disease.[Citation2] Healthy lifestyle is estimated to prevent 90% of all diabetes mellitus, 80% of all coronary heart disease and stroke and 30% of all cancers.[Citation1]
Disease prevention is an integral part of health care work, especially in primary health care (PHC).[Citation3] Primary care plays a major part in prevention of chronic diseases such as hypertension and dyslipidemia.[Citation3] However, non-pharmacological primary and secondary prevention work has been less successful.[Citation4]
The Marmot report “Closing the Gap” [Citation5] demonstrated enormous health disparities closely related to social conditions. Health inequalities based on level of education are growing despite improvements in the average health of the population.[Citation6] Marmot also emphasises that medical staff should make inquiries about patients’ lifestyle.[Citation5] Although 90% of patients would like medical staff to ask them about their lifestyle, only 30% report that they were asked.[Citation5]
The Swedish National Board of Health and Welfare has produced national guidelines for lifestyle disease prevention methods.[Citation2] These methods provide evidence for the effectiveness of supporting the individual with lifestyle changes. However, there are no guidelines concerning the effectiveness of such methods in relation to e.g. gender or socioeconomic background. There is a strong association between low socioeconomic status and unhealthy lifestyle.[Citation5,Citation7,Citation8] Interventions should be evaluated for differential socioeconomic impact.[Citation9] Implementation of a lifestyle-improvement method, “Pro-Health”, began in 2007–2008 in the Hisingen community (inhabitants 130,000) of Gothenburg.[Citation10] Several biological risk factors were significantly improved one year after intervention in more than 3600 participants. However, as community lifestyle interventions have been shown to be more effective in higher income groups,[Citation11] the present study will investigate whether the “Pro-Health” intervention programme was also suitable for the socioeconomically vulnerable groups of the community.
Aim
The aim of this study was to explore whether socioeconomically vulnerable groups in a community can be reached in primary care and engaged in a specially tailored health-promotion programme for lifestyle changes to the same extent as higher socioeconomic groups.
Methods
Study population
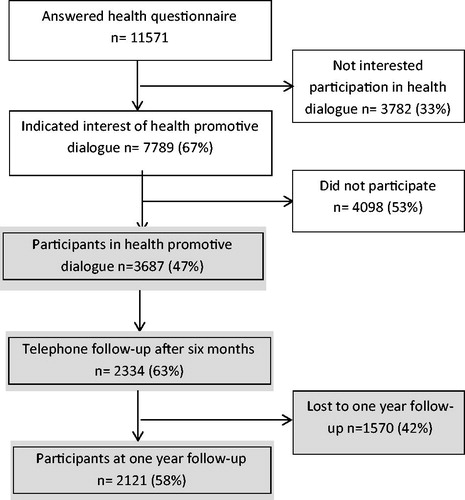
A specially tailored health-promotion programme, “Pro-Health”, for lifestyle changes in primary care, was launched in 2007–2008 [Citation10] at Hisingen. All men and women aged 18–79 visiting any of the eight public primary care centres (PCC) during a period of eight months were offered a short intervention health questionnaire. The questionnaire was used as an instrument to initiate reflection on the participant’s own lifestyle and to start a motivational process for lifestyle changes. Among all visitors, 7789 individuals were interested in an intervention and ultimately 3687 participated at baseline in a nurse health promotive dialogue lasting for about 60 min, after having completed a self-administered health profile ().[Citation10] The participants were informed that they would receive a telephone follow-up by the same nurse after six months, followed by a one-year follow-up with a health promotive dialogue, after having completed another self-administered health profile. The intervention process has earlier been described in detail.[Citation10]
Figure 1. Flow chart of the participants in the Pro-Health intervention programme. The present study refers to participants in the health promotive dialogue and one-year follow-up (grey colour).
Instruments and assessments
Waiting room health questionnaire – intervention and assessment
The health questionnaire used for waiting room screening has been described earlier.[Citation12] It was distributed at the reception desk when patients aged 18–79 attended the PCCs. It contains nine questions (with the possible responses yes, no and don’t know) concerning lifestyle, one question concerning heredity of cardiovascular disease and one question about readiness to start lifestyle change (Likert scale anchored by “not at all” to “very much”). The final question was: “Are you interested in a self-instructive health profile, a health promotive dialogue, and a blood pressure and blood sugar check?” This instrument initiates a reflection process.
Self-administered health profile – intervention and assessment
The self-administered health profile has been described previously.[Citation10,Citation12] The instrument consisted of a questionnaire distributed by the health educator (nurse or specially educated health coach), and was answered at home prior to the health promotive dialogue (approximately 1 h of reflection before the visit). The answers to the questionnaire were converted into self-instructive health profile (Hp) measures. Five of the six measures were classified as good, not so good or risk and were assessed at baseline and at one-year follow-up: smoking (good = presently not smoking or snuffing, and risk = smoking ≥ one cigarette/day or snuffing), physical activity [Citation13] (good = physically active during leisure time the last year, spending ≥2–3 h a week gardening, running, dancing, playing golf, tennis, or similar activities, not so good, or risk); stress [Citation14] (good, not so good, or risk = perception and symptoms of stress daily or almost daily, during the last six months); alcohol [Citation2] (low risk = for women ≤ nine glasses/week (corresponding to 135 cl wine/week), for men ≤14 glasses/week, not so good = women 10–14 glasses/week, men 15–19 glasses/week, risk = women ≥15 glasses/week, men ≥20 glasses/week); diet (good, not so good or risk = unbalanced diet concerning both meal order and meal composition.[Citation15] The measure risk was based on accepted lifestyle risk factors.[Citation2]
The sixth measure, view of life present and future, was indicated by a number between 1 and 10, where 1 was “worst possible” and 10 “best possible”. Change after one year was assessed from the three steps (good, not so good and risk) and for smoking two steps.
Survey questions concerning leisure time physical activity and well-being
Validated survey questions (sq) from the Gothenburg population studies were used.[Citation16] The leisure physical activity groups were classified as follows: low, intermediate, high and very high physical activity. The general well-being question was: How do you feel about your health situation (well-being)? A Likert-type scale ranging from one to seven was used. The answers were classified from excellent, couldn’t be better (one), to very poor (seven).
Biological variables
Systolic and diastolic blood pressure (right arm, sitting position, after five min’s rest), capillary p-glucose (mmol/L, non-fasting), weight (kg), body mass index (BMI) (kg/m2), waist circumference (WC) (cm, standing position at the level midway between the lower rib margin and the iliac crest) and waist-hip ratio (WHR) (cm/cm, waist circumference divided by hip circumference) were measured at baseline and one-year follow-up.[Citation10]
Intervention
The intervention consisted of (i) the health questionnaire, (ii) the health profile, (iii) the health promotive dialogue,[Citation10] and (iv) a choice of activities for the participants after the health promotive dialogue. The participants could choose either activities on their own, or in the communities (by contacting community “health counters”). Those who were in need of help within the PCC were offered this as well; stop-smoking groups, overweight groups, and individual help for those with hazardous drinking. Community health counters offered open training groups and anti-stress groups.
Socioeconomic vulnerability factors
A check-list with four questions was distributed at the health promotive dialogue concerning education, employment, ethnicity and living situation. Socioeconomic vulnerability was defined as having three or more of four of the following socioeconomic vulnerability factors; (i) low education (≤nine years in primary school), (ii) unemployed or being on sick-leave at the time of health promotive dialogue, (iii) born outside Scandinavia, and (iv) living alone.[Citation17]
Reachability
Reachability was defined in the following way: proportion participating in Pro-Health intervention study compared to community level, and was analysed by comparing the distribution of vulnerability factors to Hisingen Community population statistics 2007.[Citation18]
Engagement
Engagement in lifestyle promoting programmes is usually defined by participation rate and level of participation and outcome of engagement is measured by change in risk factors and/or change of lifestyle.[Citation19] In the present study, engagement was explored in the following way: change in risk factors and lifestyle changes after participation in Pro-Health 2007–2008. Engagement was analysed by exploring degree of change of variables (biological, health profile and survey questions) one year after baseline examination in relation to socioeconomic vulnerability.
Statistical methods
Analyses were performed using parametric tests for normally distributed data and nonparametric tests for non-normal distributions (). Logistic regression analyses were performed to compute odds ratios (OR) with 95% confidence intervals (CI) (). Differences were considered statistically significant at p < 0.05. t-Test was used for analysis of continuous variables and chi-square test for categorical variables. In order to compare the change from baseline to one-year follow-up between the various socioeconomic vulnerability groups (i.e. 0–4 vulnerability factors), logistic regression analyses were used with adjustment for age and gender. Each variable was dichotomised (negative change + unchanged; positive change) and the desirable direction of each variable was identified, and OR and 95% CI for direction of change (i.e. decrease or increase) were calculated.
Table 1. Distribution (%) of various vulnerability factors among all participants in the health promotion programme Pro-Health at baseline and at one-year follow-up. Hisingen population as comparison.
Table 2. Distribution of age and number of participants in the different age groups.
Table 3. Descriptive variables at baseline; body mass index (BMI), waist hip ratio (WHR), waist circumference, p-glucose, p-glucose ≥7, systolic and diastolic blood pressure, view of life present and future, smoking, physical activity, take away stress, alcohol, diet, take away stratified for socioeconomic factor, i.e. living situation, education, employment and ethnicity (n = 3687).
Table 4. Comparison of change from baseline to one-year follow-up between the different groups with 0, 1, 2 and ≥3 socioeconomic vulnerability factors. Logistic regression analysis; age and gender included in the analysis. Dichotomisation by undesired change + unchange; desired change. Reduction of risk factor/increase of health behaviour indicated as improvement.
The study was approved by the Regional Ethical Board at the University of Gothenburg, Sweden.
Results
The health questionnaire was answered by 11,571 participants (). Among these, 7789 individuals were interested in an intervention and ultimately 3687 participated at baseline in a nurse health promotive dialogue lasting for about 60 min, after having completed a self-administered health profile (). Health questionnaires for those who chose and chose not to participate in the nurse health promotive dialogue were compared. Those who chose to participate exhibited more readiness to initiate lifestyle change.[Citation10] At the one-year follow-up, 2121 (58%) participated.
presents baseline data concerning the distribution of individual socioeconomic vulnerability factors among all participants in the health promotion programme at baseline and at one-year follow-up. The population of Hisingen was used for comparison. Prevalence of socioeconomic vulnerability factors in the participants corresponded well to the community level. Age group, number and gender of participants are presented in .
shows descriptive variables (mean values and SDs) at baseline (n = 3687) for men and women stratified by socioeconomic factors, i.e. living situation, education, employment and ethnicity. There were statistically significant differences for all variables in the groups stratified by the different socioeconomic factors.
The group of married/cohabiting participants had significantly higher WHR and p-glucose compared to singletons. Singletons rated their view of life, both presently and regarding the future as significantly poorer than those who were married/cohabiting. Singletons smoked significantly more than married/cohabiting and perceived significantly more stress.
Participants with low education showed significantly higher BMI, WHR, waist circumference, p-glucose, systolic and diastolic blood pressure than did participants with higher education (high school/university), whereas the group with higher education perceived significantly more stress.
Participants who were unemployed or on sick leave had significantly higher BMI than the participants who were employed. Participants who were unemployed or on sick leave had a significantly more pessimistic view of life both currently and regarding the future than did employed participants. Those who were unemployed or on sick leave smoked significantly more, were more physically inactive and perceived significantly more stress than the employed.
The participants born outside Scandinavia had significantly higher BMI, WHR, systolic and diastolic blood pressure compared to Scandinavian born. The participants born outside Scandinavia rated their view of life both currently and regarding the future significantly poorer, they were more physically inactive and perceived more stress compared to Scandinavian born participants. On the other hand, Scandinavian born had significantly higher alcohol consumption and a more unhealthy diet than those born outside Scandinavia.
Change after one year – engagement
A total of 2121 participants (58%) attended the one-year follow-up (). Here, we have added also another assessment, closer to the bio-psycho-social reality. Willingness to change was examined using results from the intervention from baseline to one-year follow-up. Reduction of risk factors and increase of health behaviour was indicated as improvement. Behaviour improvement was defined as a change of one or two steps in the health profile. Individuals in the most vulnerable socioeconomic group (≥3 identified socioeconomic vulnerability factors) constituted 3% of participants in the follow-up (compared to 4% at baseline), 17% had two vulnerability factors (compared to 18% at baseline), 43% had one (compared to 42% at baseline) and 37% had no vulnerability factors (compared to 36% at baseline). The groups with 1, 2 and ≥3 socioeconomic vulnerability factors did not differ concerning positive lifestyle improvements from the group with no factors, with exception for stress perception, which improved in all groups with vulnerability factors. In the group with ≥3 vulnerability factors smoking also improved (). The group with one and two socioeconomic vulnerability factors showed significantly lower odds for improvement concerning physical activity. The group with one vulnerability factor showed higher odds for improvement concerning diastolic blood pressure and present view of life ().
Discussion
Our results show that socioeconomically vulnerable groups in a community can be reached and engaged in a health promotion programme for lifestyle changes in primary care to the same or almost the same extent as higher socioeconomic groups. The distribution of levels of education, unemployment/sick leave and participants born outside Scandinavia only showed small differences between participants and the population of Hisingen in the same age groups. The odds for improved lifestyle from baseline to one-year follow-up were close to equivalent in the groups with differing socioeconomic vulnerability levels. The group identified as most vulnerable even showed statistically significant higher odds for improvement concerning perception of stress and smoking compared to the group with no vulnerability factors.
The strengths of the study are the high number of participants and the unselected target group, as well as the extensiveness of the intervention’s target area, including eight PCCs representing both urban as well as rural areas within a well-defined, large district. The high number of participants, 3687, was 47% of the individuals initially interested in health promotive dialogue, which in a conventional intervention can seem to be a low participation rate. In the special method design of Pro-Health, adapted for primary care, where motivation and self-determination are cornerstones, this participation rate is very acceptable. All interested individuals have the possibility of returning to the PCC whenever it is more convenient.
A limitation is the lack of a control group. Within the context of ordinary primary care it is not always possible, either for practical or ethical reasons, to have separate intervention and control groups. For individually orientated interventions, the randomised controlled trial (RCT) is the desirable design. Population-based intervention with its complexity is more likely to encounter limitations, when the RCT design is used.[Citation20] In the Inter99 study, an RCT investigating the effects of an individualised lifestyle consultation on ischemic heart disease, participation was highly unevenly distributed among different socioeconomic groups.[Citation21]
Overall, the participants in Pro-Health, regardless of socioeconomic status, improved their lifestyle during the follow-up year.[Citation10] Similar results in primary care based intervention programmes have been observed in e.g. Habo, Live for life.[Citation22]
In a Belgian intervention study men from high socioeconomic status showed greatest improvement.[Citation23]
In our study, being married was associated with higher WHR and p-glucose compared to singletons, which could indicate a higher cardiovascular risk of cohabitants. In the UK national breast screening programme,[Citation24] women who were married (or living with a partner) had a similar risk of developing IHD, but lower IHD mortality, compared to single women.
The associations shown in our study between low education and higher BMI, WHR, WC, p-glucose, systolic and diastolic blood pressure are in accordance with previous studies.[Citation17,Citation25–28]
Dealing with unequal health is one of our greatest challenges. Pro-Health, a structured method, seems to be a suitable way to handle this. Participants from the various socioeconomic vulnerability groups showed comparable odds for lifestyle improvements during the follow-up year. Our results are mainly in agreement with studies from Finland,[Citation29,Citation30] where socioeconomic status did not seem to have any impact on the effectiveness of lifestyle intervention in individuals at high risk of type 2 diabetes.[Citation29] In another Finnish study, there were no significant differences in traditional cardiovascular risk factors according to educational attainment between differing socioeconomic status groups either at baseline or at follow-up.[Citation30] All groups responded positively to lifestyle counseling. In a Danish study of GPs’ and patients’ communication about lifestyle, GPs were recommended to focus on the patient’s frame of reference, which supports the “Pro-Health” method based on reflection on the participant’s own lifestyle and motivation for change.[Citation31]
In conclusion, health-promoting intervention programmes, launched at the PCC level, where the individual's current motivation and own risk apprehension are valued, seem to be a feasible method to reach and engage also socioeconomically vulnerable groups of patients to initiate and perform long standing lifestyle changes. The promising results must be interpreted with caution due to lack of control group.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- Alwan A. Global status report on noncommunicable diseases 2010. Geneva: World Health Organization; 2011.
- Disease Prevention in the Swedish Healthcare System: health situation, national guidelines and implementation. Stockholm: Socialstyrelsen, The National Board of Health and Welfare; 2011.
- Lindblad U, Ek J, Eckner J, et al. Prevalence, awareness, treatment, and control of hypertension: rule of thirds in the Skaraborg project. Scand J Primary Health Care. 2012;30:88–94.
- Ebrahim S, Taylor F, Ward K, et al. Multiple risk factor interventions for primary prevention of coronary heart disease. Cochrane Database Syst Rev. 2011;CD001561. doi: 10.1002/14651858.CD001561.pub3.
- Marmot M, Friel S, Bell R, et al. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372:1661–1669.
- The commission for a socially sustainable Malmö [Internet]. 2013 [cited Mar 1]. Available from: http://www.malmo.se/Commission-for-a-Socially-Sustainable-Malmoe-in-English.html.
- Marmot M. Social determinants of health inequalities. Lancet. 2005;365:1099–1104.
- Swedish National Institute of Public Health. Living habits. Progress report 2009. Available from: http://www.cabdirect.org/abstracts/20103321311.html.
- McGill R, Anwar E, Orton L, et al. Are interventions to promote healthy eating equally effective for all? Systematic review of socioeconomic inequalities in impact. BMC Public Health. 2015;15:457.
- Blomstrand A, Ariai N, Baar AC, et al. Implementation of a low-budget, lifestyle-improvement method in an ordinary primary healthcare setting: a stepwise intervention study. BMJ Open. 2012;2:e001154.
- Adler NE, Newman K. Socioeconomic disparities in health: pathways and policies. Health Aff (Millwood). 2002;21:60–76.
- Blomstrand A, Lindqvist P, Carlsson IE, et al. Low-budget method for lifestyle improvement in primary care: experiences from the Göteborg Health Profile Project. Scand J Primary Health Care. 2005;23:82–87.
- Saltin B, Grimby G. Physiological analysis of middle-aged and old former athletes. Comparison with still active athletes of the same ages. Circulation. 1968;38:1104–1115.
- Rosengren A, Tibblin G, Wilhelmsen L. Self-perceived psychological stress and incidence of coronary artery disease in middle-aged men. Am J Cardiol. 1991;68:1171–1175.
- Nordic Nutrition Recommendations. 2012. Integrating nutrition and physical activity. 5th ed. Copenhagen: Nordic Council of Ministers; 2014:002.
- Sullivan M, Karlsson J, Bengtsson C, et al. “The Goteborg Quality of Life Instrument” – a psychometric evaluation of assessments of symptoms and well-being among women in a general population. Scand J Primary Health Care. 1993;11:267–275.
- Govil SR, Weidner G, Merritt-Worden T, et al. Socioeconomic status and improvements in lifestyle, coronary risk factors, and quality of life: the Multisite Cardiac Lifestyle Intervention Program. Am J Public Health. 2009;99:1263–1270.
- City of Gothenburg, statistics [Internet]. [cited 2014 Nov 11]. Available from: http://www.goteborgstad.statistik.se.html.
- Hadgkiss EJ, Jelinek GA, Taylor KL, et al. Engagement in a program promoting lifestyle modification is associated with better patient-reported outcomes for people with MS. Neurol Sci. 2015;36:845–852.
- Sanson-Fisher RW, Bonevski B, Green LW, et al. Limitations of the randomized controlled trial in evaluating population-based health interventions. Am J Prev Med. 2007;33:155–161.
- Bender AM, Jorgensen T, Helbech B, et al. Socioeconomic position and participation in baseline and follow-up visits: the Inter99 study. Eur J Prev Cardiol. 2012;21:899–905.
- Lingfors H, Lindstrom K, Persson LG, et al. Evaluation of “Live for Life”, a health promotion programme in the County of Skaraborg, Sweden. J Epidemiol Comm Health. 2001;55:277–282.
- De Craemer M, De Decker E, Verloigne M, et al. The effect of a kindergarten-based, family-involved intervention on objectively measured physical activity in Belgian preschool boys and girls of high and low SES: the ToyBox-study. Int J Behav Nutr Phys Activ. 2014;11:38.
- Floud S, Balkwill A, Canoy D, et al. Marital status and ischemic heart disease incidence and mortality in women: a large prospective study. BMC Med. 2014;12:42.
- Cabrera C, Helgesson O, Wedel H, et al. Socioeconomic status and mortality in Swedish women: opposing trends for cardiovascular disease and cancer. Epidemiol. 2001;12:532–536.
- Kaplan GA, Keil JE. Socioeconomic factors and cardiovascular disease: a review of the literature. Circulation. 1993;88:1973–1998.
- Mead EL, Gittelsohn J, Roache C, et al. A community-based, environmental chronic disease prevention intervention to improve healthy eating psychosocialfactors and behaviors in indigenous populations in the Canadian Arctic. Health Educ Behav. 2013;40:592–602.
- Blomstrand A, Blomstrand C, Ariai N, et al. Stroke incidence and association with risk factors in women: a 32-year follow-up of the Prospective Population Study of Women in Gothenburg. BMJ Open. 2014;4:e005173.
- Rautio N, Jokelainen J, Oksa H, et al. Socioeconomic position and effectiveness of lifestyle intervention in prevention of type 2 diabetes: one-year follow-up of the FIN-D2D project. Scand J Public Health. 2011;39:561–570.
- Siren R, Eriksson JG, Peltonen M, et al. Impact of health counselling on cardiovascular disease risk in middle aged men: influence of socioeconomic status. PLoS One. 2014;9:e88959.
- Guassora AD, Beck Nielsen S, Reventlow S. Deciding if lifestyle is a problem: GP risk assessments or patient evaluations? A conversation analytic study of preventive consultations in general practice. Scand J Primary Health Care. 2015;33:191–198.