
Abstract
Objectives: Feasibility testing of a psychoeducational method -The Affect School and Script Analyses (ASSA) – in a Swedish primary care setting. Exploring associations between psychological, and medically unexplained physical symptoms (MUPS).
Design: Pilot study.
Setting: Three Swedish primary care centers serving 20,000 people.
Intervention: 8 weekly 2-hour sessions with a 5–7 participant group led by two instructors - followed by 10 individual hour-long sessions.
Subjects: Thirty-six patients, 29 women (81%), on sick-leave due to depression, anxiety, or fibromyalgia.
Outcome measures: Feasibility in terms of participation rates and expected improvements of psychological symptoms and MUPS, assessed by self-report instruments pre-, one-week post-, and 18 months post-intervention. Regression coefficients between psychological symptoms and MUPS.
Results: The entire 26-hour psychoeducational intervention was completed by 30 patients (83%), and 33 patients (92%) completed the 16-hour Affect School. One-week post-intervention median test score changes were significantly favorable for 27 respondents, with p < .05 after correction for multiple testing for 9 of 11 measures (depression, anxiety, alexithymia, MUPS, general health, self-affirmation, self-love, self-blame, and self-hate); 18 months post intervention the results remained significantly favorable for 15 respondents for 7 of 11 measures (depression, alexithymia, MUPS, general health, self-affirmation, self-love, and self-hate).
Conclusions: A psychoeducational method previously untested in primary care for mostly women patients on sick-leave due to depression, anxiety, or fibromyalgia had >80% participation rates, and clear improvements of self-assessed psychological symptoms and MUPS. The ASSA intervention thus showed adequate feasibility in a Swedish primary care setting.
A pilot study of a psychoeducational intervention – The Affect School and Script Analyses (ASSA) – was performed in primary care
• The intervention showed feasibility for patients on sick-leave due to depression, anxiety, or fibromyalgia
• 92% completed the 8 weeks/16 hours Affect School and 83% completed the entire 26-hour ASSA intervention
• 9 of 11 self-reported measures improved significantly one-week post intervention
• 7 of 11 self-reported measures improved significantly 18 months post-intervention
Key Points
Introduction
Depression is the third leading contributor to the global disease burden [Citation1]. Depression has serious impact on functioning and quality of life, with associated increased prevalence of several somatic disorders, and increased all-cause mortality [Citation1,Citation2]. Major features of depression are dysphoria, anhedonia, and lack of interest [Citation3]. Depending on depression type, there is either an activation or a down-regulation of the hypothalamic-pituitary-adrenal (HPA) axis, and of the sympathetic nervous system [Citation1,Citation2,Citation4,Citation5]. In cases of increased sympathetic activity, depression is accompanied by anxiety [Citation2]. Both depression and anxiety syndromes cause a large amount of sick-leave, and increase the risk of early retirement [Citation6]. In a Swedish population sample the 5 year depression prevalence was 7%, and the anxiety prevalence 5% [Citation7]. The female/male ratio was 2:1 for both conditions [Citation7].
Fibromyalgia is characterized by chronic widespread pain and hyperalgesia, often accompanied by medically unexplained somatic symptoms, cognitive symptoms, and depression [Citation8]. The worldwide mean prevalence of fibromyalgia was 2.7% with a female/male ratio of 4:1 [Citation8].
According to Tomkins´ affect theory, affects are innate, unconscious, and strictly biological portions of emotions [Citation9–12]. Each basic affect, such as anger, fear, or shame, has a specific program involving face mimicry, body gestures, voice, and autonomous nervous and hormone system physiology [Citation9–12]. Emotions can be intertwined by both conscious feelings and unconscious affects [Citation9–13].
Alexithymia, characterized by low emotional awareness and expressiveness, has been linked to depression, anxiety, chronic benign pain, obesity, and to increased cardiovascular mortality [Citation4,Citation14–19]. In a longitudinal study, alexithymia increased the risk for developing depression, but the alexithymia characteristics also seemed to worsen during depressive episodes [Citation20]. The alexithymia prevalence was between 5–17% in a nationwide Finnish population study [Citation21]. We have previously found an alexithymia prevalence of 50% in depressed compared to 11% in non-depressed patients with type 1 diabetes [Citation14], 67% in depressed patients with type 2 diabetes [Citation4], and 36% in patients with chronic benign pain [Citation15].
For somatic symptoms which are not explained by a somatic disorder the concept ‘medically unexplained physical symptoms’ (MUPS) has been introduced [Citation9,Citation17–19]. There are several hypothesized underlying mechanisms for the development of MUPS [Citation25]. Examples are endocrine dysregulation mainly in the HPA-axis, autonomic nervous system dysfunction, and somatosensory amplification [Citation25]. Increased prevalence rates of MUPS has been linked to depression, anxiety, fibromyalgia, and alexithymia, particularly the alexithymia sub factor ‘difficulty identifying feelings’ (DIF) [Citation15,Citation22–24]. MUPS are common both in patients attending primary care and specialized hospital clinics, with prevalence rates of up to 50% [Citation23,Citation26].
Cognitive behavioral therapy (CBT) [Citation27–30] and psychoeducation [Citation31] are examples of methods used for patients with depression, anxiety, or MUPS. The ‘Affect School and Script Analysis’ (ASSA), a psychoeducational method aiming at increased emotional awareness and expressiveness, was constructed by the psychologists Bergdahl and Armelius [Citation32], inspired by Tomkins’ affect theory [Citation9–12], and its interpretation by Nathanson [Citation13] and Monsen [Citation33]. We hypothesized that psychoeducation with the ASSA method could lead to decreased psychological symptoms and MUPS in patients on sick leave due to depression, anxiety, or fibromyalgia. The primary aim of this pilot study was to try the feasibility of ASSA in a Swedish primary care setting. A secondary aim was to explore associations between symptoms of depression, anxiety, alexithymia, and MUPS.
The primary outcome measure was feasibility in terms of acceptable participation rates and expected improvements in depression, anxiety, alexithymia, MUPS, general health, and six self-image measures, assessed by self-report instruments pre-, one-week post-, and 18 months post-intervention. Secondary outcome measures were regression coefficients between depression, anxiety, alexithymia, and MUPS.
Material and methods
Study design and selection of participants
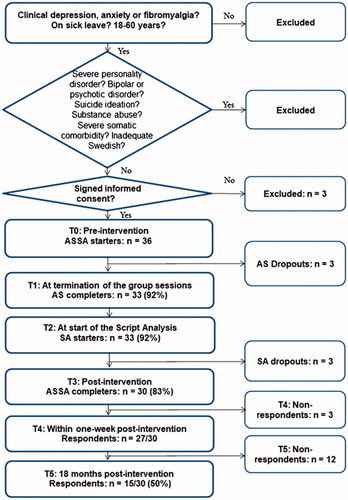
A pilot intervention study with ASSA was performed with patients from three primary care centers serving 20,000 people between 2005 and 2008 in southern Sweden. During a period of 3 months prior to each scheduled start, 39 patients on sick leave due to depression, anxiety, or fibromyalgia were clinically evaluated and found eligible for participation by five physicians including the first and last author. Three eligible patients declined participation which left 36 patients (29 women (81%), median age 39, range 27–60 years) who were enrolled in six ASSA intervention groups. For inclusion and exclusion criteria, see . Exclusion criteria were based on 1) patients with severe personality disorders, manic episodes, or psychotic symptoms could have negative impact on the other group members and the group process, 2) thoughts concerning suicide ideation in the group situation could be difficult to handle, 3) there is a risk for low participation rates for patients with drug addiction or a severe somatic comorbidity, 4) adequate knowledge of Swedish is necessary in a group situation. The participants had the following clinical diagnoses on their sick leave certificates: depression (ICD codes F32, F33) (n = 22), anxiety (ICD codes F41.0, F41.1, F41.9, F45.2) (n = 12), and fibromyalgia (ICD code M 79.7) (n = 2). There were no somatic comorbidities on the sick leave certificates.
Figure 1. Chart showing inclusion/exclusion criteria, completers/non-completers, and respondents/non-respondents to the questionnaires.
All participants provided written informed consent. The study was approved by the Regional Ethical Review Board of Linköping University, Linköping: Dnr M120-07.
Self-report instruments
Self-report instruments were distributed pre-intervention (T0), within one-week post-intervention (T4), and 18 months post-intervention (T5) ().
The Hospital Anxiety and Depression Scale (HADS) was used to assess symptoms of depression (HADS-D) and anxiety (HADS-A) [Citation4,Citation5,Citation14,Citation34–36]. The subscales consists of 7 statements each, with 4 response alternatives from 0 to 3. The cut off level ≥8 points, recommended by the constructors of the scale, was used for both subscales [Citation34], though according to a study of the Swedish HADS version the optimal cut-off score for both subscales was 5 [Citation35]. Using the cut-off ≥8 points for HADS-D, we have previously shown that self-reported depression was associated with alexithymia, impaired glycemic control, and with increased midnight cortisol secretion in patients with type 1 diabetes [Citation5,Citation14].
The Toronto Alexithymia Scale-20 items (TAS-20) was used to assess alexithymia [Citation24,Citation37]. It consists of 20 statements rated from 1 to 5, the cut-off ≥61 points was used [Citation24,Citation37]. TAS-20 has a three-factor structure based on the subscales DIF, difficulty describing feelings (DDF), and externally oriented thinking (EOT).
The Structural Analysis of Social Behavior assessment tool (SASB) was used to assess self-image measures [Citation38]. The questionnaire comprises 36 statements with response options on a scale from 0 to 100 with 10-point increments, which are summarized into eight clusters. Three clusters reflect positive emotions: self-affirmation, self-love, self-protection; three clusters reflect negative emotions: self-blame, self-hate, self-neglect. The two emotionally neutral clusters, self-emancipation and self-control, were not included.
The Stress and Crisis Inventory-93 (SCI-93) was designed to assess the severity of symptoms that are primarily related to the autonomous nervous system (ANS) [Citation39]. Therefore, mainly information of MUPS caused by dysfunction of the ANS can be gathered by SCI-93. The scale consists of 35 statements rated from 0 to 4 [Citation39,Citation40]. SCI-93 has shown satisfactory validity and test–retest reliability in a Swedish primary care setting [Citation39], but since there are no previous studies of MUPS assessment using SCI-93, there is no recommended cut-off for MUPS discrimination available. In a Swedish population sample mean (SD) SCI - 93 was for men/women 27.7 (±11.0)/30.2 (±12.0) [Citation40].
The EuroQol ‘health barometer’, a 100-mm visual analogue scale (VAS) measuring health-related QoL, where 100 represents worst possible health and zero represents perfect health, was used to assess general health [Citation41]. No cut-off level was used.
ASSA intervention
ASSA began with 8 group sessions – ‘the Affect School’, which were followed directly by 10 individual sessions – ‘the Script Analysis’. All 27 respondents one-week post intervention terminated ASSA within 20 weeks from the start.
Affect school - group sessions
The Affect School comprised 8 weekly, 2-hour sessions, of a 5–7 participant group. Each group was led by the two same instructors during all sessions. The instructors, one psychotherapist, one physiotherapist, and one general practitioner (GP), had all participated in the same 40-hour training course led by the constructors of the ASSA intervention. At each Affect School session, a specific hand-out was distributed, exactly the same copy for the participants as for the instructors. Altogether 8 hand-outs were distributed which contained affect and script theory, and the topics for the affect discussions. Each session focused on one or two innate affects, see the detailed protocol for the eight sessions (see Appendix). The instructors started every group session by presenting affect and script theory, followed by a group discussion. During the group sessions, the patients trained to identify, differentiate, and verbally express affects and emotions, and to identify the bodily expressions of all the innate affects [Citation9–13]. Single-event autobiographical narratives were encouraged [Citation42].
Script analysis - individual sessions
The 10 weekly Script Analysis sessions were performed with one instructor, either the physiotherapist, the GP, or one social counsellor who was recruited for this purpose only. The participants were asked to choose and focus on one or two affects they considered particularly difficult to handle. They trained to identify their own scripts, i.e. their learned patterns to handle emotions, and they were encouraged to explore alternate strategies for handling emotions.
Affect theory presented
Tomkins´ affect theory includes five basic concepts, affects, feelings, emotions, scripts, and mood [Citation9–13]. Affects are the innate, unconscious, and strictly biological portions of emotions. Each affect has a specific program involving face mimicry, body gestures, voice, and autonomous nervous and hormone system physiology. The affects are important messengers to the self, communicators to other people, motivators, and informers of good and bad. Also, they regulate drives and other affects. Features of affects are that they are contagious, automatic, abstract, intrusive, and general. The specific functions, face mimicry, body gestures, and somatic expressions of each affect are presented to the participants according to the detailed protocol. Feelings are the conscious portions of emotions. Emotions reflect biography. A triggered affect evokes memories of earlier situations and relationships where this affect has been triggered before, and in addition, other affects triggered in the earlier situations will be triggered again in the present situation. Both unconscious affects and conscious feelings can be combined into emotions. Scripts are learned patterns to handle emotions. Four major scripts for handling anger and shame are presented: ‘attack self’, ‘withdrawal’, ‘attack other’, and ‘avoidance’. Mood is defined as a persistent state of emotion.
Feasibility and observations during the group sessions
Completers of the intervention were counted at T1 and at T3 (). The instructors made observations of potential embarrassment due to the group situation, interactions between participants, and the ability to comply with the instructions to tell single-event narratives, were performed by the instructors.
Statistical analysis
Analysis of data distribution using histograms revealed that the psychological variables were not normally distributed. Data were presented as number (%), or as median (quartile (q)1, q3; min-max). Fisher´s Exact Test, McNemar Test, Wilcoxon Signed Ranks Test and Linear regression analysis (Backward) were performed. The false discovery rate (FDR) control method was used for multiple testing correction [Citation43]. SPSS® version 18 (IBM, Chicago, Illinois, USA) was used for all statistical analyses except for the FDR, which was performed with R version 3.2.4 (revised 2016-03-16 r70336), the R Foundation for Statistical Computing, www.r-project.org. P < .05 was considered statistically significant.
Results
Feasibility
The entire 26-hour psychoeducational intervention with ASSA was completed by 30 patients (83%), and 33 patients (92%) completed the 16-hour Affect School group sessions ().
Test results pre-, post-, and 18 months´ post-intervention
At baseline (T0) clinical depression was present in 22 patients (61%), clinical anxiety in 12 (33%), and fibromyalgia in 2 patients (6%). For the 22 patients with clinical depression the median (q1, q3; min-max) scores were for HADS-D 11 (9, 13; 8–19), and for HADS-A 12 (10, 15; 4-20). For the 12 patients with clinical anxiety median (q1, q3; min-max) scores were for HADS-D 6 (4, 7; 3–7), and for HADS-A 12 (9, 15; 8–16). For the two patients with fibromyalgia HADS-D was 1 and 4 points, and HADS-A was 2 and 3 points respectively.
In , the prevalence of self-reported depression, anxiety, and alexithymia at T0, T4, and T5 are presented. For 27 respondents, comparing T4 to T0, the prevalence decreased with 33% for depression (p = .004) with 37% for anxiety (p = .006), and with 22% for alexithymia (p = .070). For 15 respondents, comparing T5 to T0, the prevalence of depression decreased with 40% (p = .031).
Table 1. Prevalence of depression, anxiety, and alexithymia at baseline (T0), within one-week post-intervention (T4), and at 18 months post-intervention (T5).
In , the median test scores for all self-report instruments are presented at T0, T4 and T5. One-week post-intervention (T4) median test score changes were significantly favorable with p < .05 after correction for multiple testing for 9 of 11 measures (depression, anxiety, alexithymia, MUPS, general health, self-affirmation, self-love, self-blame, and self-hate. Eighteen months post-intervention (T5) the results remained significantly favorable for 7 of 11 measures (depression, alexithymia, MUPS, general health, self-affirmation, self-love, and self-hate) with p < .05 after correction for multiple testing. Sub analyses showed that the two alexithymia sub factors DIF and DDF were responsible for the TAS-20 improvements at T4 and T5.
Table 2. Test scores at baseline (T0), within one-week post-intervention (T4), and at 18 months post-intervention (T5).
Associations between HADS-D, HADS-a, TAS-20, and SCI-93 at baseline for 36 ASSA starters
For the 36 ASSA starters (T0), the scores for HADS-D (p = .032) and HADS-A (p = .012) were associated with the SCI-93 scores. TAS-20 total scores and the three TAS-20 sub factor scores were not associated with SCI-93 scores ().
Table 3. Baseline analyses of associations between scores for HADS-D, HADS-A, TAS-20, and for SCI-93 scores for the 36 ASSA starters (T0).
Observations during the affect school group sessions
During the first two sessions, the participants were restrained and quiet. After the third session there were no more dropouts, and a strong engagement was noted. Interactions and support between the participants were frequent. Several participants reported that it was a relief to find that other people had the same type of problem, for example panic attacks. A bias to tell general autobiographical narratives was noted, and repeated reminders to tell single-event autobiographical narratives were necessary (see Appendix).
Resource consumption-comparisons between ASSA and individual psychotherapy
With 30 patients completing the 26-hour ASSA intervention the number of therapist hours was 30 × 10 × 1 = 300 for the individual sessions. For the 8 × 2 = 16 hours of group sessions with five participants and two instructors per group the number of therapist hours was 192 (= 30 × 16 × 2/5). The total number of therapist hours was 492 for the ASSA intervention. Individual psychotherapy for 30 patients during 26 hours would require 780 therapist hours. Thus, the ASSA intervention would need 37% less number of therapist hours than individual psychotherapy alone.
Non-response analysis
Thirty-six patients responded to the questionnaires at baseline (T0). Out of these 36 patients, 27 responded to the questionnaires at T4, 9 persons were non-completers or non-respondents at T4. There were no differences between the 9 non-completers/non-respondents and the 27 T4 respondents at baseline regarding the prevalence of self-reported depression (p > .99), anxiety (p > .99), or alexithymia (p = .69); or the median scores for SCI-93 (p = .96), EuroQol (p = .87), self-affirmation, (p = .42), self-love (p = .58), self-protection (p = .48), self-blame (p = .46), self-hate (p = .73), or self-neglect (p = .20).
Discussion
Main findings
A psychoeducational method previously untested in primary care for mostly women patients, on sick-leave due to depression, anxiety, or fibromyalgia had a >80% participation rate, and clear improvements in self-assessed psychological symptoms, general health, and MUPS. One-week post-intervention median test score changes were significantly favorable for 9 of 11 measures in the 27 respondents (depression, anxiety, alexithymia, MUPS, general health, self-affirmation, self-love, self-blame, and self-hate). At 18 months post intervention the results remained significantly favorable for 7 of 11 measures in the 15 respondents (depression, alexithymia, MUPS, general health, self-affirmation, self-love, and self-hate). The ASSA method required 37% less therapist hours than individual therapy during 26 hours.
Strengths and weaknesses of the study
Our study is the first evaluation of the ASSA psychoeducational method in a primary care setting. Since the main aim was to test feasibility the lack of a control group to compare the results of the outcome measures is a recognized weakness. However, the fact that 9 of 11 median differences of self-reported variables (corrected for multiple analyses) changed significantly in a positive direction, suggests that this may not only be attributed to the so-called Hawthorne effect. A non-response analysis was performed, and the non-respondents/non-completers did not differ from the respondents for any variable tested at baseline. Due to the small number of participants there are several possible type 2 errors. The p-values were ≤0.10 (corrected for multiple analyses) for all self-reported median differences 18 months post-intervention (T5). Few men participated, which can be explained by known gender prevalence differences for depression, anxiety, and fibromyalgia [Citation7,Citation8]. Due to the small participation rate no gender sub analyses could be performed. It could be regarded as a weakness that the Script Analyses differed between the participants, but it is a part of the method to individualize these approaches. The patients themselves must decide which affect scripts they further want to explore. According to Tomkins´ affect theory, shame is the most important affect [Citation9–13], but no patients should be forced to talk about shame if they are not prepared to do so [Citation13].
The HADS instrument was used to assess the degree and changes of anxiety and depressive symptoms, not to establish clinical diagnoses, which was performed prior to inclusion by their physicians. HADS has well known limitations [Citation36]. The advantage of the HADS instrument is however that it was constructed as a screening instrument to obtain information about anxiety and depression in patients with somatic complaints in medical wards, who were not themselves aware that their somatic symptoms could be due to a psychiatric disorder. All symptoms that could be signs of somatic disease are avoided in HADS [Citation34]. We consider that measuring decreases in median HADS scores is a more important outcome measure than scoring above or below an arbitrary cut-off level, particularly as there is no consensus in the literature of the optimal cut-off level [Citation34,Citation35]. For TAS-20, there is strong support for the generalizability of the three-factor structure across languages and cultures [Citation37]. The SCI-93 appears to reflect well symptoms of ANS dysregulation according to previous research [Citation39], but has not previously been used to explore MUPS.
Relation to existing literature
The ASSA method was previously tried for persons with high levels of chronic stress, and a similar reduction in psychological symptoms was achieved as in the present study [Citation32]. When we tried the ASSA for patients with chronic benign pain at a specialist rehabilitation center, participants reported improved social relations and decreased alexithymia, but no reductions in depression, anxiety, or MUPS, as seen in this study [Citation15]. The dropout rate in this intervention study (17%), as well as the dropout rate (8%) in our previous ASSA intervention study [Citation15], were lower than the mean dropout rate of 25% previously reported in individual or group based CBT studies [Citation28]. In a large multicenter RCT a group based psychoeducation for patients with depression showed a dropout rate of 66% [Citation31]. In a group based CBT study for patients with MUPS the majority declined participation [Citation27]. Internet based CBT can be effective in treating depression equal to treatment as usual in Swedish primary care [Citation30], but most patients express a need for human contact, real time interaction, dialogue, and guidance when treated for depression [Citation29]. The ASSA intervention offers all these aspects.
The associations found between symptoms of anxiety, depression, and MUPS, here mainly attributed to ANS dysregulation, are in accordance with previous research [Citation22,Citation23]. However, we found no associations between alexithymia total scores, the alexithymia sub factor DIF, and MUPS, which differs from previous research [Citation15,Citation24].
The ASSA intervention and meaning of the study
The ASSA intervention method is based on Tomkins´ affect theory, which stresses that the innate affects are unconscious and strictly biological, and that each affect has a specific program for the ANS and the hormone systems [Citation9–13]. To increase emotional awareness the participants trained at every session to identify, differentiate and describe affects, feelings and emotions, and to identify the somatic expressions of all innate affects. Participants were encouraged to tell single-event autobiographical narratives, in contrast to general autobiographical narratives, which is considered important in psychotherapy [Citation42]. The group setting offers an opportunity to improve the understanding of others by listening to personal narratives and emotional expressions. This could lead to improved social relations which was achieved in our previous study [Citation15], but not tested in this study. During the Script Analysis participants learned to identify and analyze their own scripts to handle emotions, and they were encouraged to consider alternate strategies to handle emotions. The observed decreased alexithymia traits might be of importance, as alexithymia has been linked to psychiatric and psychosomatic disorders, as well as to cardiovascular mortality [Citation4,Citation14–19]. A limited ability to process emotions cognitively, as in alexithymia, may lead to amplification of the somatic sensations accompanying emotional arousal [Citation16]. In this study the participants systematically processed emotions cognitively during all sessions, and the MUPS scores decreased to levels previously found in a Swedish population sample [Citation40]. It must be noted that the instrument used in this study to explore MUPS mainly gather symptoms due to ANS dysregulation.
ASSA requires quite a high amount of therapy resources, and we have not performed any cost-benefit calculations. Yet, we must bear in mind that the total health care costs for psychiatric treatments and for somatic consequences of depression and anxiety, as well as societal costs for reduced productivity, sick-leave and early retirement are indeed very high [Citation1,Citation2,Citation6,Citation7,Citation22,Citation23,Citation26].
Further research
An RCT with ASSA tried against Basic Body Awareness is planned in a larger setting [Citation44]. ASSA could be also be tried against internet based therapy or CBT [Citation27–30]. A shortened version with only the group-based the Affect School in addition to treatment as usual could also be tried.
Conclusions
This pilot study in primary care of a psychoeducational intervention with ASSA showed promising results for patients on sick-leave due to depression, anxiety, or fibromyalgia. Feasibility, measured as participation rate, was high compared to results from other studies where individual or group based CBT, or psychoeducational interventions were tried [Citation27,Citation28,Citation31]. Our hypothesis that increased emotional awareness could decrease psychological and somatic symptoms was supported, but not proven since our study was uncontrolled.
Acknowledgements
We are indebted to Anna Lindgren, PhD, Lund University, Lund, Sweden, for her statistical skills. We also want to thank the physiotherapist J. Ahlgren who participated as instructor and performed script analyses, and the social counselor G. Carlsson who performed script analyses.
Disclosure statement
E.O.M. and R.S. have trained pre-graduate psychology students and psychotherapists in using the ASSA method at Linnaeus University, Växjö, Sweden, 2010–2016, and were instructors in the group sessions in the present study. E.O.M. also performed script analyses. H.O.T. and E.O.M. recruited patients for the present study.
Additional information
Funding
Notes on contributors
Eva O. Melin
Eva O. Melin is MD and PhD, works as a GP in primary care and as a researcher at the Department of Research and Development , Region Kronoberg, Växjö, and is affiliated to the Department of Clinical Sciences, Lund University, Lund, Sweden.
Ralph Svensson
Ralph Svensson is psychologist and psychotherapist, and works at Linnaeus University, Department of Psychology, Växjö, Sweden.
Hans O. Thulesius
Hans O. Thulesius is MD, PhD and assistant professor, works as a GP in primary care and as a researcher at the Department of Research and Development , Region Kronoberg, Växjö, and is affiliated to Clinical Sciences, Division of Family Medicine, Lund University, Malmö, Sweden.
References
- Penninx BW, Milaneschi Y, Lamers F, et al. Understanding the somatic consequences of depression: biological mechanisms and the role of depression symptom profile. BMC Med. 2013;11:129.
- Gold PW, Chrousos GP. Organization of the stress system and its dysregulation in melancholic and atypical depression: high vs low CRH/NE states. Mol Psychiatry. 2002;7:254–275.
- Association AP. Diagnostic and statistical manual of mental disorders IV-TR. 4th ed. Washington DC: American Psychiatric Association; 2000.
- Melin EO, Thunander M, Landin-Olsson M, et al. Depression differed by midnight cortisol secretion, alexithymia and anxiety between diabetes types: a cross sectional comparison. BMC Psychiatry. 2017;17:335.
- Melin EO, Thunander M, Landin-Olsson M, et al. Depression, smoking, physical inactivity and season independently associated with midnight salivary cortisol in type 1 diabetes. BMC Endocr Disord. 2014;14:75.
- Wedegaertner F, Arnhold-Kerri S, Sittaro N-A, et al. Depression-and anxiety-related sick leave and the risk of permanent disability and mortality in the working population in Germany: a cohort study. BMC Public Health. 2013;13:145.
- Carlsson A, Wändell P, Osby U, et al. High prevalence of diagnosis of diabetes, depression, anxiety, hypertension, asthma and COPD in the total population of Stockholm, Sweden: a challenge for public health. BMC Public Health. 2013;13:670.
- Guzzo M, Iannuccelli C, Gerardi M, et al. Gender difference in fibromyalgia: comparison between male and female patients from an Italian monocentric cohort. Ann Rheum Dis. 2017;76:1379.
- Tomkins SS. Affect, imagery, consciousness: The positive affects. vol. 1. New York, US: Springer; 1962.
- Tomkins SS. Affect, imagery, consciousness. the negative affects. vol 2. New York: Springer; 1963.
- Tomkins SS. Affect, imagery, consciousness: the negative affects: Anger and fear. New York: Springer; 1991.
- Tomkins SS. Affect, imagery, consciousness. Cognition: duplication and transformation of information. Vol 4. New York: Springer; 1992.
- Nathanson DL. Shame and pride: affect, sex, and the birth of the self. New York/London: Norton; 1992.
- Melin EO, Thunander M, Svensson R, et al. Depression, obesity and smoking were independently associated with inadequate glycemic control in patients with type 1 diabetes. Eur J Endocrinol. 2013;168:861–869.
- Melin EO, Thulesius HO, Persson BA. Affect School for chronic benign pain patients showed improved alexithymia assessments with TAS-20. Biopsychosocial Med. 2010;4:1–10.
- Taylor G, Bagby R, Parker J. The alexithymia construct. A potential paradigm for psychosomatic medicine. Psychosomatics. 1991;32:153–164.
- Galderisi S, Mancuso F, Mucci A, et al. Alexithymia and cognitive dysfunctions in patients with panic disorder. Psychother Psychosom. 2008;77:182–188.
- Tolmunen T, Lehto SM, Heliste M, et al. Alexithymia is associated with increased cardiovascular mortality in middle-aged finnish men. Psychosom Med. 2010;72:187–191.
- Melin EO, Svensson R, Thunander M, et al. Gender, alexithymia and physical inactivity associated with abdominal obesity in type 1 diabetes mellitus: a cross sectional study at a secondary care hospital diabetes clinic. BMC Obes. 2017;4:21.
- Tolmunen T, Heliste M, Lehto SM, et al. Stability of alexithymia in the general population: an 11-year follow-up. Compr Psychiatry. 2011;52:536–541.
- Mattila AK, Ahola K, Honkonen T, et al. Alexithymia and occupational burnout are strongly associated in working population. J Psychosom Res. 2007;62:657–665.
- Henningsen P, Zimmermann T, Sattel H. Medically unexplained physical symptoms, anxiety, and depression: a meta-analytic review. Psychosom Med. 2003;65:528–533.
- Nimnuan C, Hotopf M, Wessely S. Medically unexplained symptoms: an epidemiological study in seven specialities. J Psychosom Res. 2001;51:361–367.
- De Gucht V, Fischler B, Heiser W. Neuroticism, alexithymia, negative affect, and positive affect as determinants of medically unexplained symptoms. Personal Individ Diffe. 2004;36:1655–1667.
- van Ravenzwaaij J, olde Hartman T, van Ravesteijn H, et al. Explanatory models of medically unexplained symptoms: a qualitative analysis of the literature. Ment Health Fam Med. 2010;7:223–231.
- Aamland A, Malterud K, Werner EL. Patients with persistent medically unexplained physical symptoms: a descriptive study from Norwegian general practice. BMC Fam Pract. 2014;15:1.
- Arnold I, Speckens A, Van Hemert A. Medically unexplained physical symptoms: the feasibility of group cognitive-behavioural therapy in primary care. J Psychosom Res. 2004;57:517–520.
- Hans E, Hiller W. Effectiveness of and dropout from outpatient cognitive behavioral therapy for adult unipolar depression: a meta-analysis of nonrandomized effectiveness studies. J Consult Clin Psychol. 2013;81:75–88.
- Holst A, Nejati S, Björkelund C, et al. Patients’ experiences of a computerised self-help program for treating depression: a qualitative study of Internet mediated cognitive behavioural therapy in primary care. Scand J Prim Health Care. 2017;35:1–8.
- Eriksson MCM, Kivi M, Hange D, et al. Long-term effects of Internet-delivered cognitive behavioral therapy for depression in primary care – the PRIM-NET controlled trial. Scand J Prim Health Care. 2017;35:126–136.
- Dowrick C, Dunn G, Ayuso-Mateos JL, et al. Problem solving treatment and group psychoeducation for depression: multicentre randomised controlled trial. BMJ. 2000;321:1450.
- Bergdahl J, Larsson A, Nilsson LG, et al. Treatment of chronic stress in employees: subjective, cognitive and neural correlates. Scand J Psychol. 2005;46:395–402.
- Monsen J, Monsen K. Affects and affect consciousness: A psychotherapy model integrating Silvan Tomkins’s affect- and script theory within the framework of self psychology. In: Goldberg A, editor. Prog. Self Psychol. Plur. Self Psychol. vol15. Hillsdale NJ: Analytic Press; 1999, p. 287–306.
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370.
- Zöger S, Svedlund J, Holgers K-M. The Hospital Anxiety and Depression Scale (HAD) as a screening instrument in tinnitus evaluation. Int J Audiol. 2004;43:458–464.
- Roy T, Lloyd CE, Pouwer F, et al. Screening tools used for measuring depression among people with Type 1 and Type 2 diabetes: a systematic review. Diabet Med. 2012;29:164–175.
- Taylor GJ, Bagby RM, Parker JD. The 20-Item Toronto Alexithymia Scale. IV. Reliability and factorial validity in different languages and cultures. J Psychosom Res. 2003;55:277–283.
- Halvorsen MS, Monsen JT. Self-image as a moderator of change in psychotherapy Margrethe S. Halvorsen and Jon T. Monsen, Department of Psychology, University of Oslo, Oslo, Norway. Psychother Res. 2007;17:205–217.
- Ericsson A, Nyström C, Mannerkorpi K. Psychometric properties of the Stress and Crisis Inventory (SCI-93) in females with fibromyalgia and chronic widespread pain. Nord J Psychiatry. 2015;69:28–34.
- Kraft BNC, Nyström O, Pedersen C. Stressreaktion och välfärdsdata-en populationsstudie (in Swedish) [Stress reactions and welfare data-A population study]. Socialmedicinsk Tidskr 2004;3:222–229.
- Thulesius H, Alveblom AK, Hakansson A. Post-traumatic stress associated with low self-rated well-being in primary care attenders. Nord J Psychiatry. 2004;58:261–266.
- Williams JMG, Barnhofer T, Crane C, et al. Autobiographical memory specificity and emotional disorder. Psychol Bull. 2007;133:122–148.
- Glickman ME, Rao SR, Schultz MR. False discovery rate control is a recommended alternative to Bonferroni-type adjustments in health studies. J Clin Epidemiol. 2014;67:850–857.
- Melin EO, Svensson R, Gustavsson S-Å, et al. Affect school and script analysis versus basic body awareness therapy in the treatment of psychological symptoms in patients with diabetes and high HbA1c concentrations: two study protocols for two randomized controlled trials. Trials. 2016;17:221.
Appendix
Detailed protocol for the 8 group-based sessions – the Affect School