To the Editor,
A 44-year-old woman with appendiceal adenocarcinoma presented for her eleventh cycle of oxaliplatin, folinic acid (FA) and infusional 5-fluorouracil (5-FU) (e.g., FOLFOX-4). Before the chemotherapy session began, blood pressure was 120/78 mmHg, respiratory rate was 18 per minute, heart rate was 72 per minute, and temperature was 35.5°C. Roughly 30 minutes after oxaliplatin infusion was begun, she developed palpitations and dizziness followed by two episodes of syncope. Hypotension (42/20 mmHg) and bradycardia (50/min) were noted. Oxaliplatin was discontinued. Fluid resuscitation was begun, and 1 mg intravenous atropine was immediately given. Bradycardia and blood pressure recovered gradually. Later, an electrocardiogram (ECG) was performed, revealing a QT interval corrected for heart rate using the Bazett formula (QTc interval = QT interval/✓R-R interval) of 516 milliseconds (Panel A) Citation[1]. Electrolyte and enzyme data were within normal limits: sodium 141 mmol/L (135–147), potassium 4.2 mmol/L (3.5–4.9), calcium 8.7 mg/dL (8.5–10.5), magnesium 1.9 mg/dL (1.6–2.6), CPK 53 IU/L (38–174), CKMB 4.1 U/L (3–10), and troponin I 0.51 ng/mL (<0.8 ng/mL). There was neither severe headache nor focal neurologic deficit at any time. Symptoms ended within one hour; additional ECG revealed normal sinus rhythm without evidence of QT- interval prolongation (Panel B).
The long QT syndrome (LQTS) can be congenital or acquired. Congenital LQTS is a disease of transmembranous sodium and potassium ion channel proteins. Causes of acquired LQTS include drugs, electrolyte imbalance, marked bradycardia, organophosphorus compounds, subarachnoid hemorrhage, myocardial ischemia, protein sparing fasting, autonomic neuropathy and human immunodeficiency virus disease Citation[2]. LQTS is occasionally associated with torsade de pointes, and can cause sudden death.
In this case, congenital LQTS seemed unlikely due to lack of family history of syncope or sudden death. In addition, an ECG performed 5 months previously had shown sinus rhythm with cQT intervals of 426 milliseconds. The patient did not take any medications that are probable causes of QT-interval prolongation before the chemotherapy session in question. Although two episodes of syncope occurred during oxaliplatin infusion, there were none after it was discontinued. Other probable causes such as electrolyte imbalance, ischemic heart disease and central nervous system problems had already been excluded. Given no other identifiable cause of QT-interval prolongation, it is reasonable to speculate about a possible relationship between oxaliplatin and the QT-interval prolongation observed in this patient.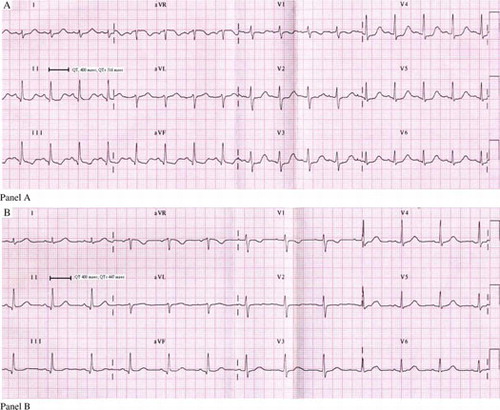
Oxaliplatin is a third-generation platinum compound with activity against colorectal cancer. It has been associated with cell membrane channelopathies Citation[3]. Adelsberger et al. suggested that oxaliplatin may alter sodium (Na+) channel kinetics in an ex-vivo rat nerve preparation Citation[4]. Because the Na+ channel plays a central role in impulse conduction in cardiac myocytes and cells of the His-Purkinje system Citation[5], alteration of Na+ channel kinetics is a possible predisposing factor for arrhythmias caused by oxaliplatin. The actual mechanism is unclear and more experimental and clinical evaluations are needed to validate the correlation between oxaliplatin and LQTS. To the best of our knowledge, our patient's LQTS had oxaliplatin as its probable cause: Physicians should be aware of arrhythmias occurring immediately after oxaliplatin infusion.
References
- Bazett HC. An analysis of the time-relation of electrocardiograms. Heart 1920; 7: 353–70
- Khan IA. Long QT syndrome. Diagnosis and management. Am Heart J 2002; 143: 7–14
- Ng M, Cunningham D, Norman AR. The frequency and pattern of cardiotoxicity observed with capecitabine used in conjunction with oxaliplatin in patients treated for advances colorectal cancer (CRC). Eur J Cancer 2005; 41: 1542–6
- Adelsberger H, Quasthoff S, Grosskreutz J, Eckel F, Lersch C. The chemotherapeutic oxaliplatin alters voltage-gated Na+ channel kinetics on rat sensory neurons. Eur J Pharmacol 2000; 406: 25–32
- Grant AO. Molecular biology of sodium channels and their role in cardiac arrhythmias. Am J Med 2001; 110: 296–305