
Introduction
The area of indications for advanced colonoscopic techniques like endoscopic mucosa resection, submucosal dissection and transanal endoscopic microsurgery is increasing. The demand for expertise has therefor increased very steeply and is largely, at this time, unmet. The implementation of nationwide screening has been the latest initiative to push this situation close to the abyss. The use of advanced endoscopic procedures varies in the range from 0% to 8% of performed colonoscopies between health care regions in Denmark. This gap in accessibility seems unacceptable.
In the late 90s it became clear that cancer treatment in Denmark was lacking behind compared to countries we usually compare ourselves to, like Sweden and Norway. The survival data were substantially worse in Denmark, and we were amongst the poorest 3 or 4 countries in Europe. This led to a governmental strategy for cancer treatment, including colorectal cancer (CRC), and the first national strategy plan was published in 2000 [Citation1]. Governmental money was dedicated to this. In 2016, the 4th national cancer strategy plan was launched and, in parallel, the survival figures for Denmark improved so there is no longer any difference in long-term outcome between the Scandinavian countries [Citation2–4]. In 2014, another governmental initiative called ‘the-sooner-the-better’ was launched; dedicating grants to initiatives that focus on early diagnosis and treatment. The SATCC became part of this initiative.
A national CRC screening program was started in 2014 [Citation5] using the immunochemical fecal occult blood test (FIT) and colonoscopy. The FIT threshold has been kept at 100 ng/L buffer contrary to other countries that also were overwhelmed with more FIT positive samples than anticipated. The impact on colonoscopy demand has been excessive as seen in other countries also, but up till now, it has been handled with an average waiting time for colonoscopy of less than 1 week. In Denmark, the majority of colonoscopy activity, including advanced polypectomy procedures, is done by the surgical departments. Approximately 80% of colonoscopies in Denmark are being performed by surgeons. The introduction of screening has changed the every day of surgical departments throughout the country. Education and training of new endoscopists have become a major challenge. The development of handling advanced adenomas and early cancers are also a major challenge in the departments where endoscopies has been a sideline activity. The technological development in advanced adenoma treatment and staging has not been fully exploited in all surgical departments due to lack of resources to develop and achieve these new competencies. Neither patients nor society has harvested the full potential benefits of this development yet, and structured teaching and training programs are needed. The SPECC program in the UK launched by the Pelican Center in Basingstoke in 2016 [Citation6] and described by Mr. Brendan Moran in this issue [Citation7] is one excellent example of actively addressing this problem. The nationwide outreaching teaching program is addressing those new challenges of ‘significant polyps and early colorectal cancer treatments – SPECC’. One of the issues in focus now – especially in the ‘the-sooner-the-better’ initiative is the staging and treatment of advanced adenomas and early cancers of the colon and rectum. The Danish Cancer Society has contributed to the development of the various cancer strategy plans and other national initiatives. In 2014, we received a 5-year grant from the Danish Cancer Society to develop a national center of reference in the field of clinical excellence, teaching and research in SATCC activities. In 2017, we further became part of the ‘the-sooner-the-better’ initiative to develop a regional center of clinical excellence, teaching, education, research and development in the area of SATCC. One initiative of the SPECC program which cannot be transferred to Danish practice is the suggested principle that all advanced polypectomy procedures preferably should be sent to centralized excellence centers. It is not possible, in Denmark, for those units to handle all these cases; and it will also be regarded as unwanted by the smaller hospitals who perform a large proportion of the colonoscopies. Therefore, the strategy of the SATCC program is to disseminate competence although there most probably is a lower limit to the number of endoscopies handled to facilitate safe treatment of the rarer advanced cases.
Colonoscopic activity in Denmark
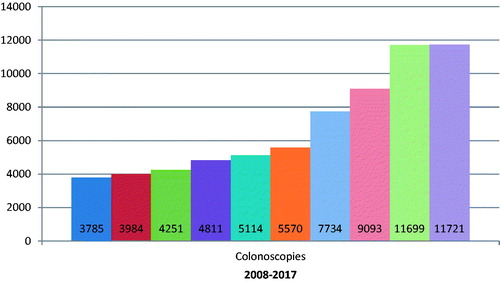
The colonoscopic activity of our surgical department has been challenging to manage (). The increase in activity started long before the introduction of population-based screening (2014). A further increase of 2–4000 colonoscopies per year is expected in the next 3–4 years. An almost steady 4% of colonoscopies lead to a renewed colonoscopy with an advanced polypectomy procedure (EMR/ESD/TEMS). There has been no national strategy to handle this development until now, and it is obvious that it is high time. It seems unavoidable that the colonoscopy quality will suffer in a period of several years until the necessary capacity of experienced endoscopists will be available. It will not only affect the quality of endoscopies and endoscopic procedures but also prevent proper endoscopic handling of early colorectal cancers and lead to an unnecessary high frequency of major procedures for early cancers. It may also cause some skepticism towards local resection of early cancers and delay its implementation. Some initiatives have been taken to train endoscopists in some healthcare regions in Denmark, but this has been initiated by dedicated surgeons and has not become national.
Figure 1. Development of colonoscopy activity in our department.
A questionnaire was sent to key persons of the different healthcare regions in Denmark asking about the approximate number of colonoscopies and the number of advanced polypectomy procedures performed reveals a vide variance in the use of advanced techniques (). Only 45% returned the questionnaire but the table illustrates the need for a national strategy and effort. A site is either a hospital or a region.
Table 1. Advanced colonoscopic procedures at different sites.
Another unfortunate aspect of the lack of competent therapeutic colonoscopists is illustrated by the fact that out of 3.639 consecutive registrations of CRC’s in the national registry, 749 cases is registered without a T stage. The majority of those are polyp cancers resected by local procedures, without a free pathological resection margin of 1 mm or more.
SATCC organization
The SATCC center was formed with the help from the Danish Cancer Society and the Health Care Regions of Denmark in 2014 to discuss, develop and disseminate knowledge in the field of advanced adenomas and early cancers in the colon and rectum. We perform research to establish safer preoperative tumor staging, indications, equipment to facilitate real-time expert consultations during colonoscopy and run a learning center. The aim is to enable state of the art, advanced endoscopic procedures and safe tumor staging to ensure that the patients are given the best treatment in the first attempt.
SATCC activities
The activities of the center are divided into: (1) Teaching; including courses, symposia’s and hands-on training programs. (2) Database hosting and management. (3) WEB page management. (4) Development and testing of new equipment and methods. (5) Development of a real-time endoscopy conference system EndoConf, and (6) Research. The activities are specified in the homepage address: http://satccenter.com/.
The database: A dedicated database for all advanced local resection procedures of the colon and rectum has been maintained since 2008. It registers all EMR, ESD and TEM procedures performed for benign and malignant disease. It currently contains detailed demographic, procedure related, complications and follow-up data on more than 3000 procedures and has been used for both quality assessment and research [Citation8,Citation9]. The database is inviting all Danish centers to enter data.
The development and testing of new equipment and methods are currently collaborating with Brüel & Kjaer (B&K), Olympus and Medtronic on the testing and development of new equipment and a program for the evaluation of Endoscopic Full-thickness Resection eFTR technique in the colon is active. A collaboration with the Maersk McKinney Moeller Robotic Center at the University of Southern Denmark is developing Machine Learning tools for endoscopy evaluation. Programs for automatic evaluation of colon cleanliness, polyp recognition and more during colonoscopy and Colon Camera Capsule Endoscopy has been developed [Citation10].
The EndoConf system has been developed in collaboration the IT department of Odense University Hospital. The system allows for real-time conference between any endoscopist in the Region of Southern Denmark and an expert at the OUH endoscopy center. Live transmission of both endoscopy and endoscopist with sound transmission through high speed secured lines has been integrated. The endosconf system is intended for discussions, during the procedure, of difficult cases and it is our hope that it might reduce the number of double endoscopies and perhaps increase the rate of ‘first time right’ interventions.
The SATCC research does focus on staging procedures of advanced adenomas and early cancers. Today candidates for local resection of early rectal cancer are allocated on the basis of T1 stage. If safe N staging could be developed, the number of candidates for local resection could increase more than 10-fold because only 20% of T1 sm3 and T2 cancers are lymph node positive and they could possible benefit from local resection if they could be safely identified.
Another area of focus of research is the use of colon camera endoscopy as a filter to reduce the number of colonoscopies [Citation9,Citation11,Citation12]. The immediate use of colon camera technique will be limited due to the current prize, but technological development will reduce the prize significantly in the coming years, partly because the prize will be reduced due to upcoming alternatives to the present PilCam colon capsule which is the only one on the marked, and partly because machine learning algorithms will take over the manual evaluation of pictures. Still some problems, especially the low rate of complete transits within the lifetime of the battery, have to be addressed.
Conclusions
The steep increase of colonoscopies during the last 10 years has affected colonoscopy quality. Further, the development of advanced colonoscopic procedures give a not fully utilized potential for less invasive treatment, reduction of treatment-related complications and safer treatment of advanced adenomas and early cancers. National strategies to increase the level of competence is needed for safer and better patient treatment and reduction of costs.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- First national strategy for cancer (Danish). [cited 2000, February]. Available from: http://www.sst.dk/∼/media/013CDA04AD384C73BA37CD47C95D931B.ashx
- Breugom AJ, Bastiaannet E, Boelens PG, et al. Oncologic treatment strategies and relative survival of patients with stage I – III rectal cancer – a EURECCA international comparison between the Netherlands, Belgium, Denmark, Sweden, England, Ireland, Spain and Lithuania. Eur J Surg Oncol. 2018;44(9):1338.
- Iversen L, Green A, Ingeholm P. Improved survival of colorectal cancer in Denmark during 2001–2012 – the efforts of several national initiatives. Acta Oncol. 2016;55:10–23.
- Winther SB, Baatrup G, Pfeiffer P, et al. Trends in colorectal cancer in the elderly in Denmark, 1980–2012. Acta Oncol. 2016;55:29–39.
- Thomsen MK, Njor SH, Rasmussen M, et al. Validity of data in the Danish Colorectal cancer Screening Database. CLEP. 2017;9:105–111.
- Moran B, Dattani M. “SPECC and SPECULATION”: is a significant polyp benign or an early colorectal cancer? How do we know and what do we do? Colorectal Dis. 2016;18:745–748.
- Moran B. The UK significant polyp and early colorectal cnacer (SPECC) program. Acta Oncol. In press.
- Al-Najami I, Rancinger CP, Larsen MK, et al. The diagnostic yield of colonoscopy stratified by indication. Gastroenterol Res Pract. 2017;2017:1.
- Al-Najami I, Rancinger CP, Larsen MK, et al. Transanal endoscopic microsurgery for advanced polyps and early cancers in the rectum – long term outcome: a STROBE compliant observational study. Medicine. 2016;95(36):e4732.
- Blandes-Vidal V, Nadimi ES, Buijs MM, et al. Capsule endoscopy vs. colonoscopy vs. histolpathology in colorectal cancer screening: matched analysis of polyp size, morphology and location estimates. Int J Coloretcal Dis. 2018;33(9):130.
- Buijs MM, Kobaek-Larsen M, Kaalby L, et al. Can coffee or chewing gum decrease transit times in colon capsule endoscopy? A randomized controlled trial. BMC Gastroenterol. 2018;18(1):95.
- Kobaek-Larsen M, Kroijer R, Dyvig AK, et al. Back-to-back colon capsule endosopy and optical colonoscopy in colorectal cancer screening individuals. Coloretcal Dis. 2018;20(6):479–485.