
Abstract
Background: During recent years, there has been an increased focus on technology within cancer survivorship and physical activity rehabilitation. Failure to acknowledge the individuals wishes and/or limitations in the use of technology introduces risk of neglecting or excluding low-resource individuals, thus adding to an already existing inequity within cancer management. It is important to identify vulnerable sub-populations with particular needs when introducing health technology to offer appropriate rehabilitation and support individuals in taking advantage of technology in their physical activity rehabilitation. We report how a population of cancer survivors referred to municipality-based rehabilitation can be segmented, according to their receptiveness and readiness for health technology utilization, to understand their potential barriers towards using technology.
Methods: We used a cross-sectional design with convenience sampling among Danish cancer survivors (n = 305) referred to rehabilitation. Participants completed a questionnaire survey covering background information and a new tool to assess self-reported health technology readiness. Demographic, disease and behavioral factors were described in relation to the participants’ receptiveness to use technology in physical activity rehabilitation. Participants were stratified according to their health technology readiness and the resulting groups described with regards to the above-mentioned factors.
Results: Almost 30% of the participants were un-receptive to use technology in relation to physical activity rehabilitation and were characterized by being more vulnerable with regards to sociodemographic characteristics and scoring lower on dimensions related to eHealth literacy. Stratification of the participants according to their health technology readiness profile revealed four distinct profiles that were significantly different in sociodemographic, disease and behavioral factors.
Conclusion: To reduce the risk of alienating low-resource individuals when introducing health technology, evaluation of the individuals’ receptiveness to use technology in a rehabilitation context and their readiness for health technology may help tailor the extent to which technology should be offered to assist the cancer survivors.
Introduction
The number of cancer survivors living up to several decades after a cancer diagnosis continues to increase and the need for effective rehabilitation programs, combating the serious sequelae inflicted by modern anti-cancer therapies, is increasing accordingly. Physical exercise training has been shown to improve physiological and psychosocial endpoints during and after primary treatment [Citation1–3] why it is now included in national and international survivorship guidelines [Citation2,Citation4], and is adopted as part of rehabilitation services in Denmark [Citation4].
In recent years, the application of technology e.g., digital tools and information systems, have gained significant attention within cancer rehabilitation and survivorship, particularly to address logistically challenged populations (e.g., living far from hospital or health centers) with poor adoption, adherence by providing distance-based programs, monitoring and support [Citation5–7]. Despite the innovative potential of introducing technology within exercise-prescription and delivery in rehabilitation programs, randomized control trials have generally delivered poor evidence that technology-based interventions, such as wearable activity trackers and feedback systems, improves health related endpoints [Citation8,Citation9].
This may be related to a lack of addressing the diversity of individuals’ competences, motivation and their experiences related to the complexity of the technology [Citation10]. Also, the individual’s experiences with, and their abilities to utilize technology, is dynamic and context specific and may depend on social factors as well as technological constraints [Citation11]. Failure to acknowledge individuals wishes and/or limitations in the use of technology introduces risk of neglecting or excluding low-resource individuals, thus adding to an already existing inequity within cancer management [Citation12]. To this end, the concept of eHealth literacy may be an important means to understand the users’ as it reports on their knowledge, skills, perceptions and experiences with health technology [Citation13,Citation14], eHealth literacy together with the usability of the technology are important factors for adoption [Citation10]. Our group recently showed how the eHealth literacy questionnaire can be supplemented with dimensions from two other validated instruments [Citation13,Citation15,Citation16] and be applied as an index for readiness in health technology to identify possible barriers to adopt health technology, the Health Technology Readiness and Enablement Index (READHY) [Citation17]. The READHY instrument includes the users eHealth literacy, self-management and social context in contrast to e.g., the Technology Acceptance Model that focuses on perceived usefulness and ease of use and is not specifically developed within a health context [Citation18].
Here, we present a descriptive study on how cancer survivors referred to municipality-based rehabilitation can be stratified based on their self-reported receptiveness and readiness for the utilization of health technology in a physical activity rehabilitation context. The aim is to get insight of how cancer survivors grouped by their readiness for technology are receptive towards using technology in connection with exercise to propose how services can be tailored to the groups characteristics.
Methods
Research design, setting and participants
This study was part of a bigger study investigating health technology readiness and motivation for training in the Copenhagen Centre for Cancer and Health [Citation17]. Briefly, the present study used a cross-sectional design with convenience sampling among citizens referred to cancer rehabilitation at the Copenhagen Centre for Cancer and Health. Rehabilitation services in the center include physical exercise, occupational therapy, dietary counseling, patient education, and psychosocial counseling. Exclusion criteria were age <18 years, insufficient cognitive function or inability to understand Danish. To minimize the risk of missing people with low literacy, participants had the opportunity to have the questionnaire read aloud and filled out by a project member.
The study was conducted in accordance with the Helsinki Declaration and was approved by the Danish Data Protection Agency (journal number 2015-55-0630). All participants received oral and written information about the study and were informed that their participation was voluntary, that they were ensured anonymity and that all data would be handled confidentially. Written informed consent was obtained from all participants before any study-related information was obtained.
Measures
Socio-demographic and disease-specific characteristics
Background information was collected via self-report. Variables can be seen in and included age, sex, education, smoking habits, cancer diagnosis, cohabitation status, additional chronic conditions, duration of daily physical activity. If they want to be more physically active (Yes/No/Maybe), to what purpose they use technology in their everyday lives, ownership of smartphone, and ownership of ordinary mobile phone/no mobile phone at all. The demographic variable education was aggregated to: comprehensive school; short education; medium education; and long education, equivalent to International Standard Classification of Education 2011 (ISCED-2011 [Citation19]) levels 1 and 2, or European Qualifications Framework (EQF [Citation20]) level 2; ISCED-2011 and EQF levels 3, 4 and 5; ISCED-2011 and EQF level 6 and; ISCED-2011 and EQF levels 7 and 8, respectively.
Table 1. Socio-demographic characteristics of the overall study population and stratified for receptiveness towards technology.
Receptiveness to supplement physical activity cancer rehabilitation with technology
As part of the background information, all participants were asked (Yes/No) ‘could you imagine supplementing your physical exercise program with technology (e.g., smartphone, computer or smartwatch)’. This variable was understood and reported as ‘receptiveness’ towards the idea of supplementing rehabilitation with technology.
The readiness and enablement index for health technology, READHY
The ‘Readiness and Enablement index for Health technology’, READHY, was used to assess health technology readiness of the participants. READHY combines dimensions from three validated and psychometrically sound questionnaires: the eHealth literacy questionnaire, eHLQ [Citation13]; the Health Education Impact Questionnaire, heiQ [Citation15]; and the Health literacy Questionnaire, HLQ [Citation16]. Together, the dimensions describe eHealth literacy (eHLQ), the individual’s self-management, i.e., knowledge of one’s own health and disease context (heiQ), as well as the social context i.e., perceived access to support from own network and/or health (HLQ). professionals (HLQ). Initial testing of the instrument is described elsewhere and involves validating the data and the context in which the data are used [Citation17].
The READHY instrument consists of 65 items covering 13 dimensions rated on a 4-point Likert scale (1 = strongly disagree to 4 = strongly agree). Each dimension is represented by an independent scale and all dimensions collectively provide a comprehensive profile of health technology readiness [Citation17].
The overall score of each dimension can be calculated as the mean of the 4–6 items comprising the dimension. If ≥ 50% of the items in a dimension are answered an average for the dimension can be calculated based on the filled in items, otherwise the entire dimension should be regarded as missing.
Statistical analyses
We explored differences with regard to age, diagnosis and sex between the study population (n = 305) and those who actively declined to participate in the study (n = 63). Descriptive statistics were reported as medians and interquartile ranges for READHY scores, socio-demographic (sex, age, education, cohabitation status), disease (diagnosis, chronic conditions) and behavioral (daily physical activity, wish to more active, smoking habits, smartphone ownership, purpose of using technology) characteristics of the overall study population. (The distribution of each scale for the entire sample, mean and standard deviation can be seen in online Appendix 1.)
Statistics were non-parametric due to variables not being normally distributed, and unequal sample sizes and heteroscedasticity of variables for subpopulations. The Mann–Whitney U test (continuous variables) or the Pearson χ2 test (frequencies) were used to test if differences existed in socio-demographic, disease and behavioral characteristics and READHY scores between receptive/un-receptive to supplement with technology. To further explore health technology readiness of the study participants, we performed a cluster analysis as described in Kayser et al. [Citation17]. In brief, we applied a combined approach using hierarchical analysis with Ward’s method for linkage to determine the optimal number of clusters for the dataset followed by the k-means method.
Differences in socio-demographic characteristics between the resulting profiles were tested using the non-parametric Mann-Whitney U test, the Kruskal–Wallis H test (continuous variables) or the Pearson χ2 test (frequencies). For variables with significant overall effects, post-hoc analyses were performed with the purpose of creating brief descriptions of the four profiles: Dunn–Bonferoni post hoc tests were used to examine differences revealed by Kruskal–Wallis H test. Contingency table cells that deviated significantly from expected counts in the Pearson χ2 test were identified by standardized residuals exceeding the critical value of ±1.96.
All statistical analyses were performed using IBM SPSS statistics version 22 (SPSS, Chicago, IL). All statistic tests were 2-sided and significance level was set at 0.05.
Results
Participant characteristics
As described previously [Citation17], 857 cancer patients were referred to Copenhagen Center for Cancer and Health, and 368 were asked to participate. From these potential candidates, 305 (82.9%) individuals agreed to participate and 63 (17.1%) declined participation due to not wishing to participate, lack of time and lack of enthusiasm and energy. Individuals who declined participation in the study were significantly older than those agreeing to participate (median age 65.0 versus 60.0, p = .027) but did not differ with regards to distribution of cancer diagnoses and sex from the study population. Participant characteristics are depicted in , first column. The 305 participants included in the survey has a median age of 60.0 years, the majority are female (n = 216, 70.8%) and most participants are living with a spouse and/or children (n = 185, 60.7%). The most prevalent diagnosis is breast cancer (n = 121, 39.7%) and participants has mainly received treatment with surgery (n = 191, 62%) at the point of inclusion. Most participants own a smartphone (n = 249, 81.6%), the majority (n = 252, 82.6%) report they wish to be more physically active and 60 (19.7%) already use technology in connection with exercise.
Receptiveness to supplement rehabilitation-based exercise with technology
A total of 216 (70.8%) participants responds that they ‘could imagine to supplement training with technology’ (‘Receptive-group’), while 88 participants (28.9%) responds that they ‘could not imagine to supplement their rehabilitation with technology devices’ (‘Un-receptive-group’), .
Socio-demographic and disease differences
Compared to individuals who are receptive to supplement their rehabilitation program with technology-devices, individuals in the un-receptive-group () are older (median age 65.0 versus 58.0 years), there is a lower proportion with long education, a higher proportion lives alone and has additional chronic conditions besides the cancer. There is a higher proportion of smokers, and a smaller proportion who wants to be more active. Also, there is a higher proportion owning an ordinary mobile phone (not smartphone)/no mobile phone at all and a smaller proportion already using technology in connection with exercise. There is no difference regarding cancer diagnosis.
Health technology readiness
The un-receptive group on average scores significantly lower on READHY scales () relating to their skills and use of technology (eHLQ1: Using technology to process health information and eHLQ3: Ability to actively engage with digital services), their motivation (eHLQ5: Motivated to engage with digital services), and their experience of/with health technology systems (eHLQ6: Access to digital services that work and eHLQ7: Digital services that suit individual needs). Receptiveness to use health technology in connection with exercise did not relate to their capacity to cope and manage their condition (heiQ3: Self-monitoring and insight, heiQ4: Constructive attitudes and approaches and heiQ5: Skills and technique acquisition), their emotional distress (heiQ8: Emotional distress) or their interaction with social/professional networks (HLQ1: Feeling understood and supported by healthcare providers and HLQ4: Social support for health).
Table 2. Mean READHY scores stratified for participants’ receptiveness towards technology.
Readiness for utilization of health technology
When participants were stratified by READHY-scores, our cluster analysis revealed four distinctive READHY profiles. Profile 1 has lower scores relative to the other profiles on all READHY dimensions, while profile 4 has higher READHY scores on all dimensions. Profile 2 has lower scores on dimensions related to self-management and support and medium eHealth literacy scores, while profile 3 has higher READHY scores on dimensions related to self-management and support but medium READHY scores on dimensions related to eHealth literacy ().
Table 3. Four READHY profiles identified by cluster analysis.
Socio-demographic and disease differences
presents cluster profile means or observed frequencies for sociodemographic variables. The four profiles are significantly different in age, educational level, cohabitation status, number of additional chronic conditions, daily physical activity, smoking habits, ownership of technology (smartphone versus ordinary mobile phone or no mobile phone) and use of technology in connection with exercise. The profiles do not differ significantly with regards to distribution of sex and their wish to be more active. Profile 1 individuals are the oldest, there is a higher proportion with short education, that live alone, that have 2 or more chronic conditions, and a higher proportion of current smokers. Profile 1 also has the lowest proportion of smartphone owners and has a lower proportion of individuals using technology for various purposes in their everyday lives. None in profile 1 use technology in relation to exercise.
Table 4. Sociodemographic characteristics of the four READHY profiles based on cluster analysis.
Health technology receptiveness
The proportion of ‘receptive’ to supplement training with technology differs significantly between the four profiles. Most participants in profile 1 are un-receptive to utilize health technology (n = 29, (76.3%), followed by profile 3 (n = 24, 36.4%), while only a minor proportion are un-receptive to utilize technology in profile 2 (n = 20, 16.9%) and profile 4 (n = 24, 15.8%).
Discussion
This study is the first to describe the receptiveness and readiness to use health technology in relation to exercise cancer rehabilitation across a broad spectrum of cancer diagnosis within an everyday clinical setting. Based on a convenience sample of Danish cancer survivors referred to rehabilitation, our data highlight readiness to utilize health technology in distinguishable sub-populations.
A key finding of the present study is that a considerable proportion (∼30% of all participants) report that they ‘could not imagine to supplement their exercise-based rehabilitation with technology measures’ (‘un-receptive’ group), which corresponded with a similar study in breast cancer survivors [Citation21]. The un-receptive-group has a higher representation of vulnerable individuals that are older, has a lower educational level, is current smokers and has more additional chronic conditions. Other studies have found similar differences between users and non-users of technology [Citation22–24]. READHY-scores revealed that the un-receptive-group experience technology-specific barriers with significantly lower scores in dimensions related to their skills, motivation and user experiences, while there were no differences in READHY dimensions related to their capacity to cope with and handle their situation, the emotional impact of their disease and social/professional networks. This indicates that while this sub-population may be reluctant to engage in eHealth-interventions, proper technology-specific introduction, training and support may enable at least some un-receptive cancer survivors to utilize such options. However, reasons for being un-receptive could be related to other factors that should be further explored. For instance, a previous study showed that non-participators of a health technology randomized controlled trial were reluctant to risk changes to existing services and relationships with specific service providers that were highly valued [Citation25].
Further insight into Danish cancer survivors’ limitations for technology utilization was gained by our cluster analysis based on READHY-scores, revealing four distinct profiles with regards to their self-management, social support, eHealth literacy and socio-demographic characteristics. Profile 1 scores the lowest on all READHY domains, is older and has a higher proportion of individuals with short education, that live alone, has 2 or more chronic conditions, and who are smokers which is in line with previous findings on eHealth literacy and sociodemographic characteristics [Citation26]. In contrast, profile 4 scores the highest across domains and comprises subjects that already apply technology in relation to exercise training. There was a clear trend associated with receptiveness to utilize technology, with those un-receptive to supplement training with technology predominantly highly overrepresented in profile 1 (low self-management, social support and eHealth literacy) and rarely found in profile 4 (high self-management, social support and eHealth literacy) profiles. While the difference between low-scoring (profile 1) and high-scoring (profile 4) READHY-profiles to some extend was expected and presumably driven largely by a sociodemographic gradient [Citation26], the cluster analyses further revealed interesting sub-groups (profiles 2 and 3) scoring similarly on eHealth literacy domains but differing with regard to self-management and support. Interestingly, these two groups also seem to differ in technology rehabilitation receptiveness; however, it is the group scoring high on self-management and support (profile 3) reporting the lowest level of receptiveness, which cannot be explained by sociodemographic factors. However, profile 3 participants are more likely not to get the recommended 30 min of daily physical activity and it may be speculated that this group prefer motivational person-to-person contact over technology in relation to rehabilitation exercise.
The identification of the four READHY profiles supports the notion that imposing a standardized ‘one-size fits all’ technology supported intervention would not be appropriate in this setting as it imposes a risk of alienating particularly low-recourse, individuals.
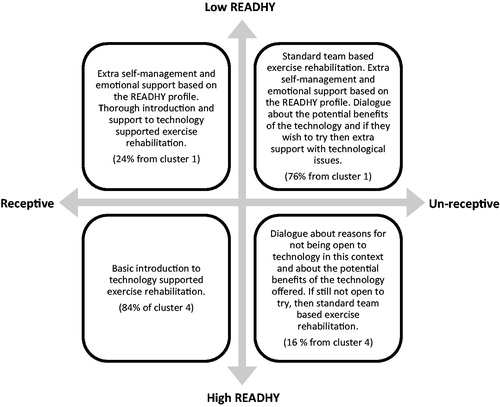
Having the skills to utilize technology does not necessarily indicate that an individual is receptive to technology in a healthcare context. Considering both individuals’ receptiveness to utilize technology as well as their readiness for health technology may be important with regard to ensuring optimized inclusion of technology for physical activity rehabilitation. Based on our findings, we propose a model for how to offer support to individuals with characteristics identifying them to belong to profiles 1 and 4 (). Interestingly, health technology readiness seems to be inversely associated with receptiveness. We therefore suggest focusing on a more personalized approach for profile 1 where it may be necessary to offer services that are not technology based. This profile is also characterized by having a lower educational level and more morbidities. They are, therefore, more vulnerable and considered to be in risk of being excluded from additional services. Whether technology may help to include these individuals remains unsolved but could include persuasive techniques, nudging or interactive gaming [Citation27].
Figure 1. Proposed model for balanced interventions based on the degree of health technology readiness and receptiveness for technology supported physical exercise.
The present study has important limitations. Due to the cross-sectional design, future research should utilize longitudinal data collection to gain insight into how the different profiles would use or not use technology in physical activity rehabilitation and what their experienced problems are. Although we did not find significant differences between the individuals who either declined participation or were not included in the study for other reasons, the sample representativeness can be questioned. A recent report demonstrated significant difference in rehabilitation referrals associated with educational level [Citation28]. Thus, the convenience sample in our study was most likely already non-representative, not mirroring those most vulnerable, suggesting the true frequency of un-receptive cancer survivors is likely higher. Also, while our sample in total was sufficient to perform cluster analyses based on READHY-scores, only breast cancer was arguably large enough to consider for meaningful diagnosis-based sub-analyses. Finally, the question ‘could you imagine supplementing your physical exercise program with technology (e.g., smartphone, computer or smartwatch)’ may introduce a bias as people who do not intend to train would answer ‘no’ independently from what they feel about technology. Also, the answer may depend on the type of technology or user interface. In our interpretation of the participants’ answers, we have conceptualized the above question as ‘receptiveness’ toward technology after a thorough discussion among the researchers. We acknowledge that this may have simplified our analysis but find that it helps us to interpret our results and understand the participants.
In conclusion, our findings show that evaluation of individuals’ receptiveness to use technology in a rehabilitation context and their readiness for health technology may identify different strata of cancer survivors with potential for personalizing rehabilitation programs according to individuals’ skills and needs. This could reduce the risk of alienating low-resource individuals when introducing health technology and identify individuals who require additional/targeted support in order to engage in technology-based interventions.
Supplemental Material
Download PNG Image (111.5 KB){kind=link}
Acknowledgments
The authors would like to thank Karen Trier, Carina Nees, Cecilie Fau Brinkløv, Mathilde Ingemann Källstrøm Damm, Sarah Leggett and Jonas Ravn for being a part of the study team and actively engaging in discussing and planning the study as well as for organizing and administering collection of questionnaires.
Disclosure statement
The authors report no conflicts of interest.
Additional information
Funding
References
- Ammitzbøll G, Søgaard K, Karlsen RV, et al. Physical activity and survival in breast cancer. Eur J Cancer. 2016;66:67–74.
- Schmitz KH, Courneya KS, Matthews C, et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc. 2010;42:1409–1426.
- Ballard-Barbash R, Friedenreich CM, Courneya KS, et al. Physical activity, biomarkers, and disease outcomes in cancer survivors: a systematic review. J Natl Cancer Inst. 2012;104:815–840.
- Danish Health Authority. Forløbsprogram for rehabilitering og palliation i forbindelse med kraeft – del afsamlet forløbsprogram for kraeft. Kbh. 2012;1–57.
- Dickinson R, Hall S, Sinclair JE, et al. Using technology to deliver cancer follow-up: a systematic review. BMC Cancer [Internet]. 2014 [cited 2018 Apr 9]; 14. Available from: http://bmccancer.biomedcentral.com/articles/10.1186/1471-2407-14-311.
- Kuijpers W, Groen WG, Aaronson NK, et al. A systematic review of web-based interventions for patient empowerment and physical activity in chronic diseases: relevance for cancer survivors. J Med Internet Res. 2013;15:e37.
- Roberts AL, Fisher A, Smith L, et al. Digital health behaviour change interventions targeting physical activity and diet in cancer survivors: a systematic review and meta-analysis. J Cancer Surviv. 2017;11:704–719.
- Jakicic JM, Davis KK, Rogers RJ, et al. Effect of wearable technology combined with a lifestyle intervention on long-term weight loss: the IDEA randomized clinical trial. JAMA. 2016;316:1161.
- Finkelstein EA, Haaland BA, Bilger M, et al. Effectiveness of activity trackers with and without incentives to increase physical activity (TRIPPA): a randomised controlled trial. Lancet Diabetes Endocrinol. 2016;4:983–995.
- Monkman H, Kushniruk AW. The consumer health information system adoption model. Stud Health Technol Inform. 2015;218:26–31.
- Griebel L, Enwald H, Gilstad H, et al. eHealth literacy research—Quo vadis? Inform. Health Soc Care. 2017;43:427–442.
- Dalton SO, Schüz J, Engholm G, et al. Social inequality in incidence of and survival from cancer in a population-based study in Denmark, 1994–2003: summary of findings. Eur J Cancer. 2008;44:2074–2085.
- Kayser L, Karnoe A, Furstrand D, et al. A multidimensional tool based on the eHealth literacy framework: development and initial validity testing of the eHealth literacy questionnaire (eHLQ). J Med Internet Res. 2018;20:e36.
- Norgaard O, Furstrand D, Klokker L, et al. The e-health literacy framework: a conceptual framework for characterizing e-health users and their interaction with e-health systems. Int J KMEL. 2015;7:522–540.
- Osborne RH, Elsworth GR, Whitfield K. The Health Education Impact Questionnaire (heiQ): an outcomes and evaluation measure for patient education and self-management interventions for people with chronic conditions. Patient Educ Couns. 2007;66:192–201.
- Osborne RH, Batterham RW, Elsworth GR, et al. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health. 2013;13:658.
- Kayser L, Rossen S, Karnoe A, et al. Development of the Multidimensional Readiness and Enablement Index for Health Technology (READHY) Tool to Measure Individuals’ Health Technology Readiness: Initial Testing in a Cancer Rehabilitation Setting. J Med Internet Res. [Internet]. 2018 [cited 2018 Dec 12]; forthcoming/in press. Available from: http://preprints.jmir.org/ preprint/10377/accepted.
- Chuttur M. Overview of the Technology Acceptance Model: Origins, Developments and Future Directions. Indiana University, USA. Sprouts Work. Pap. Inf. Syst. [Internet]; 2009. Available from: http://sprouts.aisnet.org/9-37.
- UNESCO, editor. ISCED 2011 operational manual: guidelines for classifying national education programmes and related qualifications. Paris: OECD; 2015.
- European Commision: Descriptors defining levels in the European Qualifications Framework (EQF) [Internet]. European Commision -Learning Opportunities and Qualifications in Europe [cited 2018 Dec 12]. Available from: https://ec.europa.eu/ploteus/en/content/descriptors-page.
- Phillips SM, Conroy DE, Keadle SK, et al. Breast cancer survivors’ preferences for technology-supported exercise interventions. Support Care Cancer. 2017;25:3243–3252.
- Vroman KG, Arthanat S, Lysack C. “Who over 65 is online?” Older adults’ dispositions toward information communication technology. Comput Hum Behav. 2015;43:156–166.
- Åkerberg A, Söderlund A, Lindén M. Technologies for physical activity self-monitoring: a study of differences between users and non-users. Open Access J Sports Med. 2017; 8:17–26.
- Yamin CK, Emani S, Williams DH, et al. The digital divide in adoption and use of a personal health record. Arch Intern Med. 2011;171:568–574.
- Sanders C, Rogers A, Bowen R, et al. Exploring barriers to participation and adoption of telehealth and telecare within the Whole System Demonstrator trial: a qualitative study. BMC Health Serv Res. 2012;12:220.
- Neter E, Brainin E. eHealth literacy: extending the digital divide to the realm of health information. J Med Internet Res. 2012;14:e19.
- Kayser L, Nøhr C, Bertelsen P, et al. Theory and practice in digital behaviour change: a matrix framework for the co-production of digital services that engage, empower and emancipate marginalised people living with complex and chronic conditions. Informatics. 2018;5:41.
- Moustsen IR, Larsen SB, Vibe-Petersen J, et al. Social position and referral to rehabilitation among cancer patients. Acta Oncol. 2015;54:720–726.