
Abstract
Objective: Studies have shown that a proportion of patients with aggressive non-Hodgkin lymphoma (NHL) treated with standard chemotherapy will have long-term life expectancy comparable to those in the age-adjusted general population. This systematic literature review summarizes current literature regarding health-related quality of life (HRQoL) of long-term (≥2 years) survivors of aggressive NHL.
Methods: Electronic databases (without restriction on years) and abstracts from four major oncology and HRQoL conferences from 2014 to 2017 were searched. Studies were included if HRQoL or health utility was assessed at least 2 years after NHL diagnosis. Studies focusing on central nervous system lymphoma, or indolent NHL, were excluded. Results were categorized relative to baseline (improvement, deterioration or no change) and compared to the general population (better, comparable or worse).
Results: Fourteen studies met the inclusion criteria. Twelve studies included ≥1 HRQoL instrument, and two measured health utilities using EQ-5D. Half of the studies showed improvement (5/10) and half no change (5/10) in overall HRQoL. Compared to the general population, overall HRQoL was more comparable when assessed at ≥3 years from baseline (3/3 better or comparable) versus assessment at <3 years (2/3 better or comparable). Six studies reported on the physical HRQoL domain with improvement in 4/6 studies and no change in 2/6 studies.
Conclusions: HRQoL of NHL survivors may improve from baseline and becomes more comparable to general population HRQoL with longer survival. Overall HRQoL improvement is driven mostly by improvements in the physical domain.
Introduction
Non-Hodgkin lymphoma (NHL) is the most prevalent hematologic malignancy in the United States and the fifth most deadly cancer with nearly 19,790 deaths/yearCitation1. The global percentage of NHL-caused cancer-related deaths is similar to the rate in the US at approximately 3%Citation2. Aggressive NHL, such as diffuse large B-cell lymphoma (DLBCL), is the most common subtype of NHL, and the expected survival is less than 1 year if untreatedCitation3. DLBCL represents 25–35% of new NHL cases annually. With the introduction of rituximab-based therapy (i.e. R-CHOP, a chemotherapy regimen of rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone), a significant number of patients can potentially achieve long-term survival. Maurer et al.Citation4 showed that patients with newly diagnosed DLBCL who achieved event free survival (EFS) for 24 months had a subsequent overall survival equivalent to that of the age- and sex-matched general population. In other words, patients who are event free for 24 months can potentially have a normal life expectancy.
Some studies have also investigated the health-related quality of life (HRQoL) of long-term survivors of NHL. Heutte et al.Citation5 have shown that patients experienced rapid recovery of HRQoL after autologous stem cell transplant (ASCT), using European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC-QLQ-C30). Using the Functional Assessment of Cancer Therapy: General (FACT-G) instrument, Thompson et al.Citation6 showed that aggressive NHL survivors have improving HRQoL over time, which becomes comparable to the US general population. Other instruments have also been used to measure HRQoL and health utilities in long-term survivors.
An earlier systematic literature review by Arden-Close et al.Citation7 not specific to aggressive NHL found Medical Outcomes Study 36 item Short Form Health Survey (SF-36), EORTC QLQ-C30, and Quality of Life – Cancer Survivors (QOL-CS) to be the most commonly used measures of HRQoL in lymphoma survivors and, in comparison to the general population, responses from lymphoma survivors – measured with SF-36 and EORTC QLQ-C30 – showed worse physical and social functioning, more problems with cognitive functioning and more symptoms such as fatigue and shortness of breath. However, only four studies included in the systematic review were specific to NHLCitation8–11, and only one reported HRQoL by time since baseline, which showed increasing HRQoL farther from diagnosisCitation11.
The goal of this systematic literature review is to examine the current evidence on the HRQoL of long-term survivors of aggressive NHL, measured by various HRQoL instruments. We conducted a systematic review of the literature on HRQoL or health utility among long-term (≥2 years) survivors of aggressive NHL. We aim to identify the trend in HRQoL or health utility compared to baseline and whether HRQoL of aggressive NHL survivors is comparable to the general population. This systematic literature review adds to the current literature by focusing on HRQoL in long-term survivors of aggressive NHL unlike previous reviews that had a wider focus on all lymphoma survivors.
Methods
Literature search strategy
We initiated a systematic literature review based on National Institute for Health and Care Excellence (NICE) guidelinesCitation12 searching PubMed, Embase and the UK National Health Service Economic Evaluation Database (NHS EED) without restriction on years. We also searched abstracts from four major oncology and HRQoL conferences – the American Society of Hematology (ASH), the American Society of Clinical Oncology (ASCO), the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) and the International Society for Quality of Life Research (ISOQOL) – from 2014 to 2017 to capture any studies that have not yet been published. Conference abstracts were supplemented with posters where available. Additional studies were included if identified while reviewing studies that were found in the literature search. Search terms included but were not limited to: “non-Hodgkin lymphoma”, “quality of life” or “utility” and “long-term survival”. Specific instruments were also included using a search operator “OR” as an alternative to “quality of life” or “utility”. The instruments included in the search terms were EuroQol five-part questionnaire (EQ-5D), European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), Medical Outcomes Study 36 item Short Form Health Survey (SF-36), SF-6D and SF-12.
Inclusion and exclusion criteria for study selection
English language studies were included if HRQoL or health utility was longitudinally or cross-sectionally assessed at least 2 years after NHL diagnosis or treatment, or with a mean of at least 2 years after NHL diagnosis or treatment, respectively. The study was required to report HRQoL or health utility separately for survivors, defined as those patients that achieved long-term remission. We excluded reviews, editorials and study protocols. Studies were also excluded if they analyzed the same dataset as another study, did not report scores by time since baseline, focused exclusively on central nervous system (CNS) lymphoma or included ≥50% patients with indolent NHL. Study selection was conducted by two independent reviewers and any differences were discussed and resolution agreed upon.
Data extraction and qualitative analysis
Data extracted for qualitative analysis included the study identifying information, study type, industry funding, HRQoL or health utility instrument, time since baseline, length of follow-up and outcomes. Comparison to the general population was also extracted when available. When raw scores were not reported as outcomes, we used descriptive results or coefficients from an adjusted analysis to determine the trend. Manuscripts were graded using NICE scorecards for cohort studies and randomized clinical trials (RCTs) based on risk of bias in four domains – selection, performance, attrition and detection – separatelyCitation12.
To better summarize and compare the results across the included studies, domain specific results from each study were grouped into general cancer-related HRQoL domains similar to the EORTC QLQ-C30 domains (overall, physical, cognitive, emotional and social). For longitudinal comparison, the results relative to baseline were grouped into three categories: improvement, deterioration or no change. Improvement, deterioration or no change categories were defined based on statements in the original text, change in the mean score or coefficient in regression analysis compared to baseline. For cross-sectional comparison to the general population, results were grouped by outcome relative to the general population: better, comparable, worse. Adjusted analysis and significance tests (p values) were noted where available.
Results
Characteristics of the selected studies
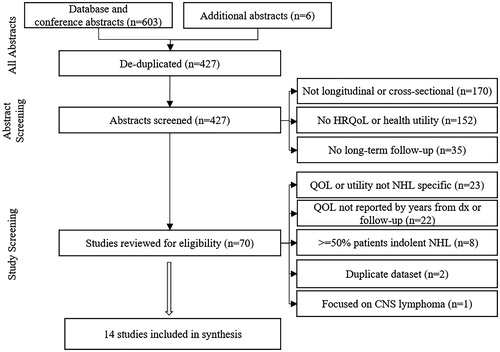
Of the 427 unique abstracts screened, 70 (16%) studies were reviewed for eligibility (). The most common reasons for exclusion from the final literature review were HRQoL or health utility not being reported specific to the NHL population (23/70; 33%) or not being reported by years from baseline or follow-up (22/70; 31%).
Figure 1. Flow diagram.
Abbreviations. CNS, central nervous system; HRQoL, health-related quality of life; NHL, Non-Hodgkin lymphoma; QOL, quality of life.
shows the identifying information for the 14 studies that met the inclusion criteria and were included in the final literature review sorted by average time from baseline and follow-upCitation5,Citation6,Citation11,Citation13–23. Although results for NHL survivors were not reported separately, Kim et al. was included in the final literature review because most of the sample (93%) had a history of NHL, with 83% aggressive NHL survivorsCitation21. All abstracts (3/3 by search criteria definition) and the majority of journal articles (8/11; 72%) were published within 5 years of this review. Multiple countries were represented with studies from Australia (n = 1), France (n = 1), Ireland (n = 1), Korea (n = 1), the Netherlands (n = 3), the UK (n = 1) and the US (n = 6). Six studies followed survivors longitudinally including one RCT, and eight studies evaluated HRQoL or health utility using cross-sectional analysis. Twelve of the fourteen studies measured HRQoL, while two studies measured health utilities.
Table 1. Synthesized longitudinal and cross-sectional studies, by time from diagnosis and follow-up.
In the 12 studies measuring HRQoL, various instruments were used, including those specified in the search terms (EORTC QLQ-C30 [n = 4], SF-36 [n = 4]), as well as additional HRQoL instruments, such as FACT-G (n = 4), Functional Assessment of Cancer Therapy: Lymphoma (FACT-Lym) (n = 3), Hospital Anxiety and Depression Scale (HADS) (n = 1) and Quality of Life – Cancer Survivors (QOL-CS) (n = 1). Two studies measured health utility using EQ-5D.
The four NHL-specific studies included in the prior systematic literature review by Arden-Close et al.Citation7 were found in our search and were reviewed for inclusion in the literature synthesis. Two did not report HRQoL by time since baselineCitation9,Citation10, one did not directly report on the measured HRQoLCitation8 and one was included in our reviewCitation11.
Overall health-related quality of life
Ten of the fourteen studies assessed change in overall HRQoL or health utility. Of the ten, five (50%) reported improvements while five (50%) reported no change (). Six of the ten studies included adjusted analysis of HRQoL scores to account for attrition in longitudinal studies and for differences between groups in cross-sectional studies. Four of the fourteen studies did not report significance tests when comparing two or more groups.
Table 2. Overall HRQoL trends among survivors and comparison to general population, adjusted analyses in bold.
Five of the fourteen studies compared HRQoL of long-term survivors with the general population. HRQoL was more comparable to the general population with HRQoL assessment at a later time point (≥3 years, 3/3 better or comparable; 100%) compared with HRQoL assessment at an earlier time point (<3 years, 2/3 better or comparable; 67%) ().
Health-related quality of life domains
Six of the fourteen studies assessed change in the physical, social and emotional HRQoL domains and two studies addressed change in the cognitive HRQoL domain of long-term NHL survivors ().
Table 3. HRQoL domain trends among survivors and comparison to general population, adjusted analyses in bold.
Positive change occurred most frequently in the physical- and social-related domains. Of the six studies assessing physical-related domain, four (67%) studies reported improvement and two (33%) studies reported no change or non-significant change. Of the six studies assessing social-related domain, three (50%) reported improvement, one (17%) reported mixed results (improvement using the QOL-CS and no change using the SF-36) and one (17%) reported deterioration.
Mixed results were reported in the emotional- and cognitive-related domains. Six studies reported results in emotional-related domain with improvement in two (33%), mixed results in one (improvement using the QOL-CS and no change using the SF-36; 17%), deterioration in one (17%), and no change in one (17%). Two studies reported results in the cognitive-related domain with improvement in one (50%) and no change in one (50%).
Compared to the general population, the physical-related domain is more comparable with assessment at a later time point (≥3 years, 4/4 better or comparable; 100%) compared with HRQoL assessment at an earlier time point (<3 years, 1/3 better or comparable; 33%). There was no clear trend for assessment before 3 years and after 3 years for the cognitive, social and emotional HRQoL domains.
Discussion
This systematic literature review found 14 studies assessing HRQoL or health utility for long-term survivors of aggressive NHL. HRQoL or health utility results are only reported for those study participants that responded to the questionnaire. These studies suggest that long-term aggressive NHL survivors have improved overall HRQoL compared to baseline and may have comparable overall HRQoL to the general population (i.e. after 3 years of survival). Similar results to overall HRQoL were seen for the physical-related and social-related domains. However, more mixed results occur for the emotional-related HRQoL domains compared with baseline and compared to the general population. The need for more research on long-term social and emotional support is recognized, and DLBCL survivors are being studied for better social- and emotional-related HRQoL outcomes when patients are provided with additional support servicesCitation24.
This systematic literature review adds to the literature and the systematic literature review by Arden-Close et al.Citation7 by focusing specifically on the HRQoL of aggressive NHL survivors, a topic which has been the subject of many publications since 2010. Most of the 14 studies (3/3 abstracts, 8/11 manuscripts) were published after the systematic literature review by Arden-Close et al.Citation7 and within 5 years of this review.
In this study, we attempted to consolidate and summarize the results across studies with various HRQoL instruments by using the EORTC QLQ-C30 domains and categorizing the results in qualitative scales (i.e. improvement, deterioration or no change). EORTC QLQ-C30 was used because it is the most frequently used HRQoL instrument in the studies. Additionally, it is general enough to capture most of the domains but is also cancer specific. The qualitative nature of this systematic review means the exact magnitude of the changes were not captured. However, the summary directionally shows how patients’ HRQoL changes over time across studies. Advanced meta-analytic methods, which would quantitatively assess both the direction and the magnitude of the HRQoL changes, could be used if a larger number of studies reported mean HRQoL scores at baseline and follow-up for the same HRQoL instruments.
In an effort to be more complete we supplemented the search terms “quality of life” and “utility” with common instrument names (EORTC QLQ-C30, EQ-5D, SF-36, SF-6D, and SF-12) using “OR” terms. This would capture studies that did not state HRQoL or health utility in the title or abstract. While not all HRQoL instruments were included here (e.g. FACT), it is unlikely that a manuscript was missed given that all publications included in the synthesis mention “quality of life” in the abstract regardless of instrument used.
In the included studies, patient attrition was common and could be a potential source of bias at the individual study level. Evidence for improvement in overall HRQoL would benefit from longer follow-up in longitudinal studies if large enough patient populations could be studied to account for attrition. Attrition bias is common in both the longitudinal and cross-sectional studies of aggressive NHL survivors; it is unclear in which direction the bias changes the results. Adjusted analyses attempt to control for the differences between groups caused in part by attrition bias. Because adjusted analyses control for observable characteristics using regression analysis, they provide a higher level of evidence than unadjusted analyses. We reach similar conclusions when only considering adjusted analyses (shown in bold in and ) from our systematic literature review.
Conclusions
Patients with aggressive NHL who survive more than 2 years show improvement or no change to their overall HRQoL compared with baseline, and overall HRQoL becomes more comparable to the general population with longer survival. Mixed results related to the emotional and social HRQoL domains suggest the need for supportive services among long-term aggressive NHL survivors.
Transparency
Declaration of funding
This study was funded by Kite, A Gilead Company.
Author contributions: V.W.L. and A.P. conceived the study topic. B.B. developed the systematic literature review with input from V.W.L., A.P. and J.E. All authors reviewed this manuscript and provided feedback.
Declaration of financial/other relationships
V.W.L. and A.P. have disclosed that they are paid employees of Kite, A Gilead Company. B.B. and J.E. have disclosed that they are employees at Stratevi which was retained for this work.
CMRO peer reviewers on this manuscript have received an honorarium from CMRO for their review work, but have no relevant financial or other relationships to disclose.
Acknowledgements
The authors would like to acknowledge Erin Williams for her contributions as the second independent reviewer.
Previous presentation: Preliminary results of this research were presented as a poster at Lymphoma and Myeloma 2017 Conference, New York, NY, USA, 26–28 October 2017.
References
- Evens AM, Winter JN, Gordon LI, et al. Non-hodgkin lymphoma. Cancer Network 2015 [Last accessed 3 Nov 2017] http://www.cancernetwork.com/cancer-management/non-hodgkin-lymphoma
- Institute for Health Metrics (IHME). GBD Results Tool. Seattle (WA): IHME, University of Washington, 2015
- Morton LM, Wang SS, Devesa SS, et al. Lymphoma incidence patterns by WHO subtype in the United States, 1992–2001. Blood 2006;107:265-76
- Maurer MJ, Ghesquieres H, Jais JP, et al. Event-free survival at 24 months is a robust end point for disease-related outcome in diffuse large B-cell lymphoma treated with immunochemotherapy. J Clin Oncol 2014;32:1066-73
- Heutte N, Haioun C, Feugier P, et al. Quality of life in 269 patients with poor-risk diffuse large B-cell lymphoma treated with rituximab versus observation after autologous stem cell transplant. Leuk Lymphoma 2011;52:1239-48
- Thompson CA, Maurer MJ, Allmer C, et al. QOL at 3 years after diagnosis in aggressive lymphoma survivors. J Clin Oncol 2015;33(15 suppl):9586
- Arden-Close E, Pacey A, Eiser C. Health related quality of life (HRQoL) in survivors of lymphoma: a systematic review and methodological critique. Leuk Lymphoma 2010;51:628-40
- Bellizzi KM, Miller MF, Arora NK, et al. Positive and negative life changes experienced by survivors of non-Hodgkin’s lymphoma. Ann Behav Med 2007;34:188-99
- Bellizzi KM, Rowland JH, Arora NK, et al. Physical activity and quality of life in adult survivors of non-Hodgkin’s lymphoma. J Clin Oncol 2009;27:960-6
- Vallance JK, Courneya KS, Jones LW, et al. Differences in quality of life between non‐Hodgkin’s lymphoma survivors meeting and not meeting public health exercise guidelines. Psychooncology 2005;14:979-91
- Mols F, Aaronson NK, Vingerhoets AJ, et al. Quality of life among long-term non-Hodgkin lymphoma survivors: a population-based study. Cancer 2007;109:1659-67
- National Institute for Health and Care Excellence (NICE). Chapter 4 Developing review questions and planning the evidence review. 2014, updated 2017. Available at https://www.nice.org.uk/process/pmg20/chapter/developing-review-questions-and-planning-the-evidence-review [Last accessed 28 July 2017]
- Ruan J, Martin P, Shah B, et al. Lenalidomide plus rituximab as initial treatment for mantle-cell lymphoma. N Engl J Med 2015;373:1835-44
- Oerlemans S, Issa DE, van den Broek EC, et al. Health-related quality of life and persistent symptoms in relation to (R-)CHOP14, (R-)CHOP21, and other therapies among patients with diffuse large B-cell lymphoma: results of the population-based PHAROS-registry. Ann Hematol 2014;93:1705-15
- Oerlemans S, Mols F, Nijziel MR, et al. The course of anxiety and depression for patients with Hodgkin’s lymphoma or diffuse large B cell lymphoma: a longitudinal study of the PROFILES registry. J Cancer Surviv 2014;8:555-64
- Hudson KE, Benecha HK, Houck KL, et al. Fatigue in long-term non-Hodgkin lymphoma survivors. J Clin Oncol 2015;33(suppl):abstract e20628
- Holland RA, Bird BR, Cahill M, et al. Assessing the quality of life of non-Hodgkin lymphoma survivors: a population-based study. J Clin Oncol 2016;34(3 suppl):227
- Glaser AW, Fraser LK, Corner J, et al. Patient-reported outcomes of cancer survivors in England 1–5 years after diagnosis: a cross-sectional survey. BMJ Open 2013;3:e002317
- Jefford M, Ward AC, Lisy K, et al. Patient-reported outcomes in cancer survivors: a population-wide cross-sectional study. Support Care Cancer 201710:3171-3179
- Jensen RE, Arora NK, Bellizzi KM, et al. Health-related quality of life among survivors of aggressive non-Hodgkin lymphoma. Cancer 2013;119:672-80
- Kim SH, Kim IR, Kim SH, et al. Health-related quality of life in Korean lymphoma survivors compared with the general population. Ann Hematol 2014;93:1531-40
- Beaven AW, Samsa G, Zimmerman S, et al. Quality of life is similar between long-term survivors of indolent and aggressive non-Hodgkin lymphoma. Cancer Invest 2016;34:279-85
- Smith SK, Crespi CM, Petersen L, et al. The impact of cancer and quality of life for post-treatment non-Hodgkin lymphoma survivors. Psychooncology 2010;19:1259-67
- Parker PA, Banerjee SC, Matasar MJ, et al. Protocol for a cluster randomised trial of a communication skills intervention for physicians to facilitate survivorship transition in patients with lymphoma. BMJ Open 2016;6:e011581