
Abstract
Open Access (OA) to research publications is a fundamental resource for the advancement of scientific research. To facilitate the transition to OA, publishers and institutions have begun negotiating the so-called transformative agreements, contracts combining access to subscription journals with the ability to publish OA. While the debate on transformative agreements is very much alive, little attention is being paid to the “green road,” the practice of openly self-archiving manuscripts that have been accepted by journals but not yet typeset. Here we focus on medical literature, showing how the green road could outperform transformative agreements as a means of increasing the full and free availability of peer-reviewed scientific papers.
Seventeen years after the Berlin DeclarationCitation1, Open Access (OA) to research publications is widely recognized as a key resource for advancement in all scientific fields and a unique opportunity to take a step forward in science as a global public good. In medicine, the availability of scientific information is fundamental to foster research and intervention activities, support programs to reduce health disparities, and facilitate informed health choices. In 2013, the World Health Organization (WHO) recognized the importance of the sharing and accessibility of research methods, results, and data as the basis for their exploitation “for practical purposes, including the improvement of health”Citation2. In 2019, the World Medical Association (WMA) reaffirmed this principle, underlining the importance of access to “timely, current, evidence-based healthcare information”Citation3. Wider availability of scientific literature is fundamental for staff members and students of universities, professional schools, and research institutes of low- and middle-income countries, where only a part of scientific journals are accessible due to budget limitations.
Although many funders and academic institutions now encourage and support open access publishing, over 50% or 40% of clinical medicine and biomedical research articles, respectively, remain closed accessCitation4. Besides, initiatives launched to provide access to articles by research groups operating in low- and middle-income countries, such as the Health Internetwork Access to Research Initiative (HINARI) launched in January 2002 by WHO in collaboration with leading scientific publishers, have not proven to be completely effectiveCitation5.
To accelerate the transition to OA, in 2018 a consortium of research funding organizations from twelve European countries with support from the European Commission and the European Research Council (cOAlition S) launched the PlanS initiativeCitation6. It is basically founded on the principles of OA that emerged from the “BBB Declarations” established by the Budapest Open Access Initiative (2002), the Bethesda Statement on Open Access Publishing (2003), and the Berlin Declaration on Open Access to Knowledge in the Sciences and Humanities (2003)Citation7. PlanS require that since 2021 results resulting from publicly-funded research must be available by publications openly accessible without restrictions. The main tools to achieve this goal are contracts negotiated between institutions and publishers that combine access to subscription journals with open access publishing at no additional cost to authors: the so-called transformative agreementsCitation8. Beyond legitimate expectations, they have raised concerns about the risk of an incomplete transition to open access (publishers may restrict access to a portion of their portfolios) and market distortions (which could exclude pure open access publishers from the agreements).
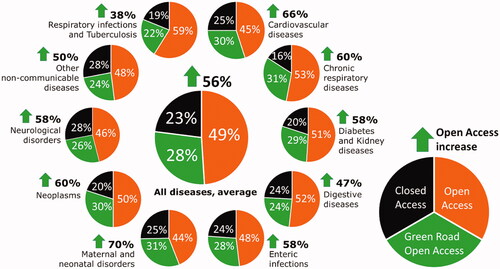
While the debate on transformative agreements is very much alive, there seems to be little focus on the “green road,” which is the practice of openly self-archiving manuscripts accepted by journals but not yet typeset (commonly referred to as post-prints)Citation9. This is unfortunate because there are two ways whereby the green road could outperform transformative agreements as a means of increasing open access. First, reducing costs: the green road does not imply any additional economic effort, whereas transformative agreements are not necessarily cheaper than current subscription deals, depending on the negotiating strength of institutions and their national consortia with publishers. In countries where research grants are limited, the costs can pass from authors to funding institutions, which can recover the additional expenses by reducing other budget items. Second, achieving results faster: undertaking the green road does not require negotiations like transformative agreements, making it quickly active. Very importantly, the potential effectiveness of the green road is supported by empirical data. In fact, by sharing not embargoed post-prints, the open-access rate of recent peer-reviewed publications (first semester 2020) covering the ten deadliest diseases in the world would have risen from 49% to 77% on average, increasing the baseline value from a minimum of 38% (respiratory infections and tuberculosis) to a maximum of 70% (maternal and neonatal diseases)Citation9 (). An important implication of these data is that the transformative agreements established so far did not prevent a significant part of publications (51%) from being closed access. It is also worth noting that with systematic use of the green road we could get important medical literature closer to the open-access rate observed for papers concerning COVID-19 (close to 90%), which may be regarded as the best case of openness in scientific publishing observed so farCitation11.
Figure 1. Percentage values of peer-reviewed papers (a total of 103,522 items published between January 1st and June 30th, 2020): open access (orange); closed access, but could have become open access (without embargo) using the green road (green); closed access, with the green road prohibited by publishers’ policies (black). The average value is unweighted. The value next to the green arrow indicates the increase in the open-access rate over the baseline.
The above arguments and evidence lead to the same conclusion: we urgently need a change of perspective. Authors of research and clinical studies should begin to see the green road as a real opportunity to share scientific information with a much wider audience. While the above empirical data showing its potential effectiveness to increase open access may strengthen the message, such an ambitious aim cannot be achieved without a more widespread culture of cooperationCitation12. To make it more than just a wish, scientific societies, academic and research centers, and patient advocacy organizations should take responsibility and collaborate to promote the use of the green road in medical literature in more specific and effective waysCitation11. Let's go together so as not to miss this opportunity.
Transparency
Declaration of funding
This work was supported by the Sapienza University of Rome (Italy), through the project “Setting up a network for Responsible Research and Innovation - RRI-Net” (PI116154C845CA8D). We also thank the Istituto Italiano di Antropologia for supporting this work as part of the Oasis Initiative (https://www.isita-anthropology.com/oasis).
Declaration of financial/other relationships
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contributions
All authors equally contributed in designing and drafting this manuscript and they agree to be accountable for all aspects of the work.
References
- Berlin Declaration on Open Access to Knowledge in the Sciences and Humanities; 2003. [cited 2022 Mar 16]. Available from: https://openaccess.mpg.de/Berlin-Declaration.
- World Health Organization. Research for universal health coverage. The world health report. Geneva: World Health Organization; 2013.
- World Medical Association. WMA statement on healthcare information for all. Adopted by the 70th WMA general assembly, Tbilisi, Georgia, October 2019. Ferney-Voltaire: World Medical Association; 2019.
- Piwowar H, Priem J, Larivière V, et al. The state of OA: s large-scale analysis of the prevalence and impact of open access articles. PeerJ. 2018;6:e4375.
- Villafuerte-Gálvez J, Curioso WH, Gayoso O. Biomedical journals and global poverty: is HINARI a step backwards. PLOS Med. 2007;4(6):e220.
- Rabesandratana T. European funders detail their open-access plan. Science. 2018;362(6418):983.
- Gasparyan AY, Yessirkepov M, Voronov AA, et al. Comprehensive approach to open access publishing: platforms and tools. J Korean Med Sci. 2019;34(27):e184.
- Borrego A, Anglada L, Abadal E. Transformative agreements: do they pave the way to open access? Learn Publ. 2021;34(2):216–232.
- Harnad S, Brody T, Vallières F, et al. The access/impact problem and the green and gold roads to open access. Ser Rev. 2004;30(4):310–314.
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1736–1788.
- Capocasa M, Anagnostou P, Destro Bisol G. Why (and how) COVID-19 could move us closer to the "health information for all" goal. MedRXiv 2020. 07.23.20160481.
- Destro Bisol G, Anagnostou P, Capocasa M, et al. Perspectives on open science and scientific data sharing: an interdisciplinary workshop. J Anthropol Sci. 2014;92:179–200.