
Rice bodies bursitis is a clinically rare disease, most commonly found in the shoulder and knee joints (Citation1), and often secondary to diseases such as rheumatoid arthritis (RA) and infectious arthritis. Currently, there is no unified treatment protocol for RA patients with rice bodies bursitis (Citation2).
A 56-year-old male presented with recurrent swelling and pain in multiple joints over more than 2 years. Tests for rheumatoid factor and anti-cyclic citrullinated peptide antibodies were positive, leading to a diagnosis of RA. The patient was treated with steroids (prednisone 5 mg daily) in combination with disease-modifying anti-rheumatic drugs (leflunomide 10 mg daily). Despite treatment, the patient’s right knee pain and swelling persisted, and the C-reactive protein level was 39.5 mg/L. Magnetic resonance imaging (MRI) of the right knee revealed significant synovial thickening and nodule formation in the suprapatellar pouch (). Arthroscopic lavage of the knee joint was performed, yielding a large amount of white, rice-grain-like material (), which, upon pathological examination, was found to contain extensive fibrin exudation and necrotic degenerated tissue, with focal formation of inflammatory granulomas (). Considering the joint MRI, lavage findings, and pathology report, the patient was diagnosed with rice bodies bursitis secondary to RA. After joint lavage and intra-articular steroid infusion, followed by methotrexate 7.5 mg once a week and leflunomide 10 mg daily, the patient’s joint pain and swelling improved, with no recurrence. A follow-up joint MRI 1 month later showed significantly reduced synovial thickening and nodules ().
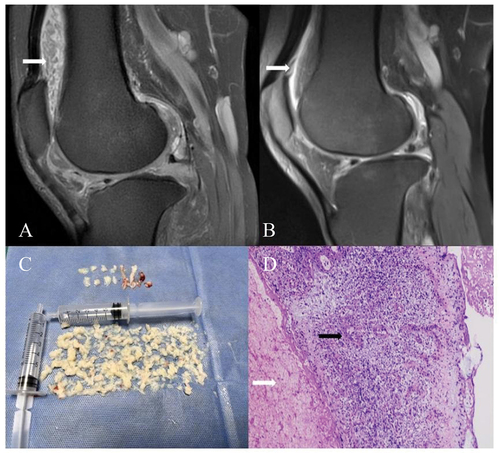
Figure 1. Magnetic resonance imaging, specimens, and pathological findings in the case. (A) Fat-suppressed T2-weighted imaging (T2WI) showing numerous ‘watermelon seed’-like rice bodies within the knee joint cavity, presenting as hypointense compared to joint effusion, with synovial proliferation. (B) Fat-suppressed T2WI showing a marked reduction in synovial proliferation. (C) Photograph of a large number of rice bodies retrieved from arthroscopic lavage. (D) Extensive fibrin exudation and necrotic degenerated tissue (white arrows), with focal formation of inflammatory granulomas (black arrows) (H&E, × 200).
The development of rice bodies bursitis secondary to RA is insidious, leading to potential misdiagnosis, missed diagnosis, or delayed treatment. In patients with large joint swelling and pain unresponsive to conventional anti-rheumatic medication, secondary rice bodies bursitis should be considered. Early joint lavage followed by anti-rheumatic treatment can improve the prognosis for RA patients.
Authors’ contributions
Fenglin Zhu collated the case report, searched the literature, and wrote the first draft. Ying Zhang collected and analysed case data, guided clinical diagnosis and treatment, and critically reviewed and revised the manuscript. Both authors approved the final manuscript.
Ethics approval and consent
This study involves a human participant, but the institutional research ethics board does not require board review for a single case report when the patient’s privacy is protected, and thus exempted this study. Participants gave informed consent to participate in the study before taking part. Written informed consent for publication of this report was obtained from the patient.
Acknowledgements
The authors thank Xuejiao Li for assistance with MRI, Min Zeng for sending the pathology report, and Director Li Chengyin for guiding the writing of this article.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Bacha R, Manzoo I, Gilani SA. Sonographic presentation of rice bodies in subacromial-subdeltoid chronic bursitis. Ultrasound J 2019;11:16.
- Guo J, Wu K, Xu Y, Yang H. Hundreds of rice bodies in the subacromial-subdeltoid bursa: report of two cases and literature review. BMC Musculoskelet Disord 2020;21:539.