
ABSTRACT
The first COVID-19 pandemic lockdown in Aotearoa New Zealand resulted in disruptions to everyday life, including changes in grocery shopping, cooking and eating. This study aimed to capture changes in behaviours and perceptions of grocery shopping and food preparation during the lockdown, and the extent to which dietary patterns changed during this period. Data were collected in an online survey of 3028 adults (89% women, mean age = 44 years, range 18–87 years, the median time in lockdown = 40 days), during Aotearoa New Zealand's lockdown Alert levels 4 (33.4%) and Level 3 (66.6%). Respondents had decreased enjoyment of grocery shopping and increased home cooking and baking from scratch. There was an overall shift toward an unhealthy dietary pattern, with some respondents reporting increased consumption of sweet snacks (41%), salty snacks (33%), alcohol (33%), and sugary drinks (20%) during the lockdown. Age moderated the effect of lockdown for nearly every measure, with adults aged under 50 years the most likely to report adverse changes to their eating behaviours and diet. Future pandemic responses by government and employers should include public health nutrition policies and mitigate the stress for younger adults and those caring for children at home.
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious respiratory disease, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The rapid emergence and spread of this disease have resulted in a COVID-19 pandemic that has caused significant social, health, and economic disruption (Adhanom Ghebreyesus Citation2020). In an attempt to halt the spread of the virus, governments worldwide enforced social distancing measures, including ‘lockdown’ that sought to reduce the movement of and contact between people. Global variations of lockdown have included curfews, quarantines, stay-at-home orders, shelter-in-place orders, and shutdowns: where only essential businesses are permitted to remain open, and schools, public buildings and the majority workplaces are required to close.
Aotearoa New Zealand's response to COVID-19 and the resulting change to our food environments
The Government's response to the first outbreak of COVID-19 in March 2020 was to ‘Go hard and go early’ with the aim of elimination of the virus (Baker et al. Citation2020; Exeter et al. Citation2020). From 23rd of March 2020 Aotearoa New Zealand was in lockdown (Alert Level 3), and two days later moved to the toughest restrictions of Alert Level 4. A national state of emergency was declared for the first time in New Zealand's history on 25th March, 2020. Everyone was asked to stay at home to break the chain of transmission of the virus, leaving their ‘bubble’ (household) only if they were essential workers, to exercise in the local neighbourhood or make trips for essential supplies, e.g. food and medicines only. Restaurants, cafes, takeaway shops (fast-food restaurants), fruit and vegetable stores, bakeries, and butchers were closed. Supermarkets and other essential shops were open with ‘one-shopper per bubble’ and physical distancing measures in place.
The country moved back to Alert level 3 at 11:59 pm Monday 27 April 2020, with takeaway shops, restaurants, and cafes reopening for contactless delivery or no physical interaction with customers (contactless pick up). Two and a half weeks later, at 11:59 pm Wednesday 13 May, the country moved out of lockdown, to Alert Level 2, ending over seven weeks of stay-at-home orders. Under Alert Level 2, some social distancing measures remained such as hospitality businesses restricted to a maximum of 100 people in the space, seated separately with one server per group, and contact tracing measures in place. The food environment did not return ‘to normal’ until Alert level 1 on 11:59pm Monday 8 June 2020, nearly a month after the last known case of COVID-19 was found and isolated in the community (Baker et al. Citation2020).
The COVID-19 pandemic created new challenges in the physical access to, and affordability of healthy food in Aotearoa New Zealand. Many cultural and social food practices (e.g. regular grocery trips, fishing, hunting and gathering kai, community gardens) and eating habits (such as regular mealtimes, eating with friends, and colleagues) were disrupted. Supermarkets and food banks struggled to meet increased demand, with many running out of necessary food supplies such as bread, pasta, flour, sugar, and yeast (Robson Citation2020; Kirkness Citation2020). Online shopping slots for pick up or delivery were full several days or weeks in advance. Meal box (uncooked food) deliveries continued and reported record numbers of new members (Anderson Citation2020; Otago Daily Times Citation2020). ‘Panic buying’ and stocking up on goods, including groceries, liquor, and tobacco products, resulted in the largest dollar value increase for March 2020 in grocery product wholesaling in over 20 years (Statistics New Zealand Citation2020a), and food prices rose (Statistics New Zealand Citation2020b).
The importance and challenge of healthy eating during a pandemic
Internationally, the public health guidance on nutrition through the epidemic has been to consume a diet based predominantly on fresh foods such as fruits, vegetables, whole grains, low-fat dairy sources, and healthy fats (olive oil and fish oil) and to limit intakes of sugary drinks and processed foods high in calories and salt (Coelho-Ravagnani et al. Citation2020). Optimum nutrition is important for mitigating the risk of morbidity due to COVID-19 by improving immunity and assisting with the regulation of sleep and mood to prevent fatigue and by lowering the risk of comorbidities (e.g. obesity, diabetes) that can worsen the progression of COVID-19 (Coelho-Ravagnani et al. Citation2020).
One hypothesis is that the psychological effects of lockdown (increased anxiety, stress, frustration, confusion, anger, and boredom) and the deviation from usual routines would result in overeating of unhealthy foods, which in turn may exacerbate overweight and increase the risk of cardiovascular and metabolic disorders (Bhutani and Cooper Citation2020; Martinez-Ferran et al. Citation2020; Mattioli et al. Citation2020). Binge eating due to the lockdown, particularly among those already experiencing disordered eating and obesity, appears to have increased health inequities in the United States and Australia (Ashby Citation2020; Phillipou et al. Citation2020). However, home cooking is generally considered to be ‘healthier’ than eating out. Eating outside the home is associated with overweight and eating less vegetables (Lachat et al. Citation2012; Seguin et al. Citation2016), whereas home-cooked meals usually have lower total kilojoules, carbohydrates, fat, sugar, and ultra-processed foods (Wolfson and Bleich Citation2015). It is uncertain if these general findings about home cooking hold when the population is forced to cook from home, as in a pandemic lockdown.
Objectives of this research
The Covid Kai Survey collected information on adult New Zealanders’ shopping, cooking, eating and food-related media use before and during the lockdown, in an online survey from 24 April to 13 May 2020 during Aotearoa New Zealand's lockdown Alert levels 3 and 4. In this paper, we report on the main findings of the survey, including changes in the behaviours and attitudes of New Zealanders towards food purchasing and preparation during lockdown, and the extent to which eating behaviours changed during this period (specifically healthy eating behaviours, such as consumption of fruit and vegetables, lower discretionary food and beverage intake, and overall dietary patterns). Given concerns about the effect of the COVID-19 lockdown on the wellbeing of older New Zealanders (Prickett et al. Citation2020), we present data separately for those aged 50 years and over.
Materials and methods
International collaboration and questionnaire content
The Covid Kai Survey is the Aotearoa New Zealand arm of the Corona Cooking Survey, an international survey conducted in 38 countries (De Backer et al. Citationforthcoming). The online questionnaire was designed by researchers at the University of Antwerp, Belgium, and loaded onto the Qualtrics survey platform for each participating country separately. The questionnaire contained 100 items covering the topics of grocery shopping (types of store, online or in-person, experiences and reasons behind grocery shopping decisions, planning, use of nutrition panel to inform purchases), stocking up on food items during the lockdown, food preparation (behaviours and enjoyment), cooking ready-made vs. fresh/from scratch, self-perceived cooking skills, barriers to cooking and baking, sources of and decision-making about recipes, food-related influential figures/organisations/brands, food frequency questionnaire, source and importance of nutrition advice, eating behaviours, (at home, eating out, food box delivery and takeaways, online video chat meals and drinking), lockdown conditions, psychological distress, and sociodemographics.
Data collection in Aotearoa New Zealand
The Aotearoa New Zealand arm of the Corona Cooking Survey, named the Covid Kai Survey, was open from 24 April to 13 May 2020 (20 days), while the country was under COVID-19 Alert Level 4 and 3 restrictions. Ethical approval for the international study was granted by the Ethics Advisory Committee on Social and Human Science at the University of Antwerp (ref: SHW_20_46) and the Aotearoa New Zealand arm of the study by the University of Auckland Human Respondents Ethics Committee on 24 April 2020 for three years (ref: 024607).
Recruitment was through convenience/snowball sampling, promoted via social media. Stakeholders and colleagues from health and food-related organisations shared the survey invitation among their networks, and the general public disseminated the survey's social media posts via their pages. Respondents were adults 18 years or older, with no further restrictions on participation. We aimed to recruit as widely as possible in the adult population and monitored responses by demographic groups of interest at several points during data collection. Targeted advertising (NZ$550) of Facebook recruitment posts was undertaken to recruit respondents tracking with lower response rates, e.g. men, and those aged over 65 years. After completing data collection, $3200 was donated to The Foodbank Project (the Salvation Army) as koha of $1 for each near-completed survey.
Variable description
Most survey questions had a 7-point frequency response scale, and respondents were generally asked each set of items twice, reporting their behaviour before the COVID-19 crisis and at that moment (during the COVID-19 lockdown).
Enjoyment of shopping and enjoyment of food preparation was assessed by the mean of six items adapted from Hagmann et al. (Citation2020) on a 7-point response scale from strongly disagree (1) to strongly agree (7). The six items were in response to the statements: ‘Grocery shopping/Preparing food was/is (1) too time-consuming; (2) frustrating; (3) a type of relaxation for me; (4) a way I could play out my creativity, discover new things; (5) enjoyable; and (6) stressful’.
Frequency of visiting the food stores was assessed by the question ‘How do you organise your grocery shopping?’ with a 7-point response scale from never (1) to every time I went grocery shopping (7) for three statements: (1) I physically go to the supermarket, shop, market, farmer, vendor to select and buy food; (2) I order my food online and pick it up at a seller's point; and (3) I order my food online and have it delivered at home. Level of stocking up was assessed by the question ‘How much did you stock up on any of the food/items below because of the COVID-19 pandemic?’ with a list of 22 items. Responses could range from a lot less than usual (1) to a lot more than usual (7).
Cooking from scratch (with basic ingredients) was assessed by the question ‘How often did you usually prepare the following foods from scratch?’ (also based on Hagmann et al. Citation2020), with a 7-point response scale from never (1) to every time I ate these foods (7) for three items: (1) A hot main meal from basic ingredients (e.g. starting with raw vegetables, meat); (2) Baked goods (e.g. cake, cookies, pie); and (3) Bread.
Barriers to cooking were assessed by the question ’How often did you experience the following barriers to cooking and/or baking?’, with five items based on Caraher et al. (Citation1999), each with a 7-point response scale from never (1) to every time I cooked or baked (7). The five items were: (1) Time (I didn't have time to cook or bake); (2) Cooking skills (I couldn't cook or bake); (3) Money (I didn't have the funds for the foods/ingredients I needed or wanted); (4) Access to food (I didn't have access to foods/ingredients I needed or wanted); and (5) Access to cooking facilities (I didn't have (access to) the facilities needed to cook or bake: stove, oven, kitchen equipment).
Food intake and dietary patterns were assessed with the question
How often did you eat the following (portions of) foods? Please indicate how often you had at least one portion of the following foods and drinks. For example, a serving/portion is a handful of grapes, an orange, a salad, a slice of bread, a glass of soft drink’.
Statistical analyses
The statistical software Stata 16.1 (StataCorp, Texas) was used for all analyses. Because all measures used an ordinal scale, average results before lockdown were reported as median (25th, 75th percentile). Mean changes in scores during lockdown (compared to before lockdown) were calculated with 95% confidence intervals (CI) and P-values using regression models with robust standard errors, both unadjusted and adjusted for covariates. Covariates were decided a priori to be age, gender, whether the household had children aged under 18 years, whether the household lost income due to lockdown, and time since lockdown began. The assumption was that households with children might have been affected by lockdown differently to households without children (mostly because of increased demand for childcare and homeschooling); and that households that lost income due to lockdown may have been affected differently than households that did not lose income. Adjustment for time since lockdown was included to allow for novelty or fatigue effects to be accounted for and the loosening of restrictions with the change from Level 4 to Level 3.
Survey respondents were classified as having increased a behaviour if their score for a particular behaviour had increased during lockdown, and similarly those who had a decreased score were classified as having decreased a certain behaviour during lockdown. These numbers are reported as per cent of the sample and allow a more nuanced view of the data, given the responses’ ordinal nature. To determine if age moderated the changes in behaviour during lockdown, the per cent of those who increased and decreased behaviours were calculated for each age group (less than 50 years of age; or 50 or older years of age).
Eating behaviours were assessed using the FFQ data with the ordinal scales converted to ‘serves/portions’ per day in the following food groups: fruits, vegetables, legumes, and wholemeal bread/pasta/grains; sweet snacks; salty snacks; total snacks (sum of sweet and salty snacks); white bread/pasta/grains; sugary beverages; and alcoholic beverages. Dietary patterns were determined using all 20 items from the FFQ before lockdown in a principal component analysis (PCA). A scree plot determined how many patterns were represented by the data and orthogonal rotation of the loading matrix was undertaken. Loadings on the patterns are reported in Supplementary Table 1 and those food items with the strongest loadings (>0.3) characterise the patterns. Dietary pattern scores were calculated by multiplying the loadings by the intake data for each participant and summing these together. This was then repeated using the same loadings, but with the intake data from the lockdown, period to determine the change in dietary pattern scores since lockdown.
Results
Survey completion and respondent characteristics
The survey closed with N = 4104 entries. Spam responses indicated by the software programme were removed (n = 81), along with two respondents who gave implausible ages (as the rest of their survey answers may have been unreliable) and those that were resident outside Aotearoa New Zealand (n = 28). Those that did not complete the Food Frequency Questionnaire, toward the end of the survey, were excluded from the analyses in this paper (n = 965). The median (IQR) time taken to complete the survey was 30 min (23–42 min).
Survey responses from 3028 adults (age range: 18–87 years) were used in the analyses. One-third of surveys (n = 1012) were completed under Alert Level 4, and 66.6% under Alert Level 3 (n = 2016). Time since the start of lockdown ranged from 31 days to 51 days (median: 40 days). presents respondents’ sociodemographic characteristics, in total and by two age groups (<50 years and 50+ years). Most respondents were female, with a tertiary education qualification, and identified as New Zealand European ethnicity. Mean age was 44.3 years (SD: 14.0), with the largest proportion in the 30 to less than 50 year age category (). Households ranged from sole occupant to 13 members, with a median number of three people per household (25th/75th percentile: 2/5). Half of the respondents aged under 50 years lived with children aged under 18 years old, compared to 18% of households with respondents aged 50 years or older. Half of the respondents worked full-time before lockdown, a quarter were working part-time, and a further 8% were students (either with or without a secondary job) (). Seven per cent of respondents said they struggled financially ‘all the time’, ‘very frequently’ or ‘frequently’ during the lockdown, and a further 15% said ‘sometimes’, with those aged less than 50 years of age more likely to report that they struggled financially during the lockdown (). A quarter of respondents lost at least part of their income due to the lockdown (n = 783, 25.9%), with no differences between the two age groups for this variable ().
Table 1. Characteristics of Covid Kai Survey respondents (n = 3028).
Changes to shopping due to the lockdown
The majority of respondents (n = 2158, 71.3%) indicated that they were responsible for the household grocery shopping both before and during lockdown, and were therefore asked questions about changes in their experience of shopping during lockdown. One in six respondents were the household shopper before lockdown but not during (n = 538, 17.7%).
There was good internal reliability for the enjoyment of shopping scale, with the Cronbach's alpha being 0.85 before lockdown and 0.84 after lockdown. Three out of every four household shoppers had a decrease in their enjoyment of grocery shopping scores during lockdown, and 40% reduced the frequency with which they went to the store (). However, a greater proportion of those under 50 years of age compared to those 50 years and older increased their physical visits to grocery stores and decreased their online shopping habits over lockdown (). Overall, respondents increased online shopping frequency during lockdown, but this was mostly in those aged 50 years and over who had used online shopping less frequently before lockdown ().
Table 2. Grocery shopping, cooking and baking before and after lockdown, total respondents.
Table 3. Changes to grocery shopping, cooking and baking by age group.
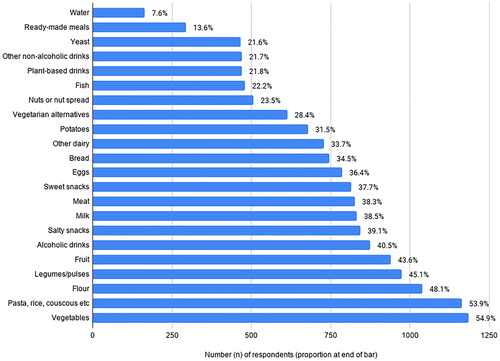
Ninety-two per cent of respondents (n = 1985 of 2158) reported that they had stocked up on food items because of COVID-19. Over half reported that they stocked up on vegetables and pasta or rice; and flour, legumes/pulses, fruit, and alcohol were also bought more commonly than usual (). Two out of every five respondents stocked up on salty snacks or sweet snacks, and around a third of respondents stocked up on basic food items such as bread, milk, and other dairy, meat, eggs, and potatoes ().
Figure 1. Food items stocked up on more than usual during the first COVID-19 lockdown (n = 2158).
Changes to food preparation due to the lockdown
There was good internal reliability for the enjoyment of food preparation scale with the Cronbach's alpha being 0.88 both before and after lockdown. Enjoyment of food preparation increased for more than half of respondents, and decreased for one in four (), with those aged under 50 years slightly more likely compared to those in the 50 years or older category to have a decreased enjoyment of food preparation (). Two out of every five respondents increased the amount of hot meals that they prepared at home from scratch with basic ingredients (), and those aged under 50 years were more likely than those aged 50 years or older to have increased the amount of meals they prepared at home from scratch (). Half of respondents increased the number of baked goods that they prepared from scratch during lockdown, and 44% increased the amount of bread that they baked (), with those aged under 50 years more likely to have increased their frequency of baking during lockdown ().
Time became less of a barrier to cooking and baking for 77% of survey respondents during lockdown. However, over half of respondents stated that access to food increased as a barrier to cooking and baking for them during the lockdown, and this barrier was highest among those aged under 50 years ().
Changes in dietary pattern and food intake during lockdown
The largest change reported by respondents in the types of food eaten during lockdown was an increased intake of sweet snacks, reported by two out of every five respondents (). Salty snack intake also increased for one-third of respondents, resulting in an increased overall frequency of eating all types of snacks for half of the respondents (). A higher proportion of respondents aged younger than 50 years increased their sweet and salty snack intake (44% and 36% respectively), compared to those aged 50 years or older (36% and 28% respectively, P < .001). One in five adults reported a decrease in sweet or salty snacks during the lockdown, but overall there was an average increase in the number of times respondents were eating snacks daily ().
Table 4. Eating behaviours before and during the COVID-19 lockdown (n = 3028).
Alcohol intake increased during lockdown for one-third of respondents, and 20% of respondents increased their sugary-drink intake during lockdown (). A higher proportion of respondents aged younger than 50 years increased their alcohol and sugary drink intake (37% and 23% respectively), compared to those aged 50 years or older (25% and 14% respectively, P < .001). However, one in 11 respondents decreased their alcohol use, and one in 8 respondents reduced their intake of sugary drinks ().
Similar proportions of respondents stated an increase and a decrease in fruit intake (18% and 21%, respectively) and vegetable intake (12% and 13%, respectively), with a minimal statistically significant decrease in vegetable intake overall (). A higher proportion of respondents aged younger than 50 years reported both a decrease (23%) or an increase (19%) in their fruit intake during lockdown, compared to those aged 50 years or older (17% and 14% respectively), and there was no evidence of a difference by age group in changes to vegetable consumption ().
Table 5. Changes in eating behaviours due to the COVID-19 lockdown, by age group (n = 3028).
Four dietary patterns were identified by principal component analysis (PCA) in the data regarding food intake before lockdown (Supplementary Table 1): a healthy pattern characterised by higher intakes of fruit, vegetables, legumes/pulses, and nuts or nut spread; an unhealthy pattern characterised by higher intakes of processed meat, sweet and salty snacks, white bread/pasta/grains and sugary drinks; a dairy pattern characterised by higher intakes of milk and other dairy products and lower intakes of plant-based milk and vegetarian alternatives; and a meat pattern with higher intakes of unprocessed fish, poultry and red meat. The variance explained within each of the four patterns ranged from 12.8% (healthy) to 8.9% (meat) (Supplementary Table 1).
During lockdown there was little change in the meat and healthy dietary pattern scores. However, there was a moderate increase in the dairy pattern and a substantial increase in the unhealthy pattern scores (). Three out of every five respondents (62.1%) had an increase in their unhealthy pattern scores during lockdown, and this was slightly more prevalent in those aged under 50 years (64.6%) than in those 50 and over (57.6%).
Discussion
These first analyses of the Covid Kai Survey of over 3,000 Aotearoa New Zealand residents found an increase in home cooking and baking from scratch during the first COVID-19 lockdown. Having more time to prepare foods meant that many experienced increased enjoyment of cooking and baking, epitomised by the baking of sourdough bread reported globally during the initial phase of the COVID-19 crisis (Easterbrook-Smith Citation2020). However, the increase in food preparation at home did not always result in healthier eating, particularly for adults aged under 50 years of age and those with children at home. Although the changes in dietary patterns found in this research were not large, there was an overall shift toward an unhealthy dietary pattern, with some respondents reporting that they consumed more sweet and salty snacks, alcohol, and sugary drinks during the lockdown.
Perhaps not surprisingly, given the increased inconvenience and stress created by physical distancing in supermarkets, grocery shopping enjoyment decreased during the lockdown, and some New Zealanders changed the way they shopped for food. Similar to US research (International Food Information Council Citation2020), an increased proportion of those aged 50 years or older shopped online for groceries, while those aged under 50 years were more likely to go in-person to buy groceries but less frequently than before lockdown. These behaviours may reflect an increase in whanaungatanga (community spirit) whereby younger people left the online shopping delivery spots free for those that needed them most or were at higher risk and the practicality that there were less online delivery slots available due to increased demand.
In our survey, over 90% of New Zealanders reported that they stocked up on some food items due to the lockdown, particularly foods that could be stored for a long time (pasta, rice, flour, and legumes), vegetables and fruit. This may not necessarily have been ‘panic buying’ as reported by the media (Peacock Citation2020), but a reflection of the decreased frequency with which people were shopping, also reported in this research. Stocking up on fruit and vegetables was a curious finding because, firstly, this did not correspond with an increased intake of fruits and vegetables during lockdown, and secondly, because most fruits and vegetables are perishable. Supermarket sales of canned fruit and vegetables increased 59% during the first week of lockdown (Bezzant Citation2020), which is consistent with stocking up of non-perishable products. However, Countdown supermarkets reported selling an unprecedented amount of fresh fruit and vegetables; 20% more than during the Christmas period (Bezzant Citation2020). Much of this increased demand may have been due to the closure of independent fruit and vegetable grocery shops and farmers’ markets during the lockdown. Certainly, it would appear from our study findings that the reported stocking up on sweet and salty snack foods resulted in an immediate increased consumption of these unhealthy products, unlike the stocking up on fruits and vegetables.
Similar to findings in other countries (Ammar et al. Citation2020; Ruiz-Roso et al. Citation2020; Scarmozzino and Visioli Citation2020; Sidor and Rzymski Citation2020), home confinement due to COVID-19 saw an overall increase in unhealthy dietary patterns. The takeaway, fast-food shops, and food delivery businesses (e.g. UberEats) were closed during Level 4 of the lockdown in Aotearoa, New Zealand, and it was hypothesised that this might improve diets (Bezzant Citation2020). However, independent grocers (e.g. ethnic food shops, fruit and vegetable stores, butcheries) were also closed during Level 4, which reduced the options for purchasing healthy food, although food box deliveries could continue if the food was uncooked. Supermarkets, corner stores (dairies), and petrol stations were the only walk-in food businesses open. These food environments in Aotearoa New Zealand are characterised by heavily-marketed and highly processed foods, which are excessively energy-dense and high in added sugar and sodium (Mackay et al. Citation2019). Additionally, there was widespread marketing on social media by fast-food, alcohol, snack, and confectionary companies during the lockdown (Collin et al. Citation2020), which may have contributed to increased purchasing of foods high in sodium, added sugar, and saturated fat (Boyland et al. Citation2016). A similar online survey found that increased unstructured time at home, boredom, and heightened stress due to the COVID-19 crisis increased snacking simply because the food was available constantly in the home, and weight gain over the lockdown was reported by 22% of respondents (Zeigler et al. Citation2020).
The diets of younger adults were the most negatively impacted by the lockdown, and this finding is also similar to studies in other countries (The Obesity Health Alliance Citation2020). Under lockdown Alert levels 4 and 3 in Aotearoa, New Zealand, schools and childcare services were closed, and teaching moved online, so most parents found themselves working from home with the additional responsibility of homeschooling and entertaining their children. The majority of respondents in the Covid Kai Survey were women, and other research in Aotearoa New Zealand has found that women with young children had the greatest increase in family demands and were more likely to report negative feelings, more work-family conflict, and decreased wellbeing (Prickett et al. Citation2020) so it is unsurprising that this was the largest group in our research to report difficulties in maintaining a healthy diet.
The New Zealand Government's health promotion messages during the first COVID-19 lockdown were focused on infection control, mental health, physical exercise, accessing healthcare, and family violence (Te Hiringa Hauora/Health Promotion Agency Citation2020; New Zealand Government Citation2020). There were no directives about healthy eating, and the government collected little data about nutrition over this period (Ministry of Business Innovation and Employment Citation2020). Given the ongoing pandemic and commitment by the New Zealand Government to an elimination strategy (Baker et al. Citation2020), lockdowns appear very likely to be repeated. The results of this research suggest that nutrition is an important issue to consider for future lockdowns. Practical public health messaging is warranted around the importance of nutrition for immunity, how to prepare home-cooked meals, and how to avoid eating in response to stress by encouraging self-care and self-compassion, taking care to avoid stigmatisation which only exacerbates the issue (Pearl Citation2020; Puhl et al. Citation2020). Consideration should also be given to the safe opening of independent grocers, placing restrictions on marketing and promotions of unhealthy food, alcohol, and sweetened beverages during lockdown periods, and subsidising healthy foods for low-income groups.
A key strength of this research was the high participation in the online survey over the periods with the greatest restriction on movement during the COVID-19 crisis (Alert levels 4 and 3). However, the questionnaire used had a relatively high respondent burden (30 min to complete), required a moderate literacy level required for some of the questions, and relied on recall of respondents to assess and self-report changes in their behaviours before and during the lockdown. Given that the ‘before’ and ‘after’ reports were collected at the same time (i.e. during lockdown) there may be bias in the reporting of behaviours, and given that there is no comparison group, the changes observed may not be fully attributable to the lockdown. The questionnaire was not designed for a New Zealand-specific study and did not contain questions that may have been more meaningful for our population's food environment and pandemic response. As with most online surveys, the major limitation was that respondents were not randomly selected, which resulted in a high proportion of women and highly-educated participants, and most likely, people interested in food and nutrition. Relative to the population, there was low participation by Pasifika peoples, and although Māori had higher participation at 10.6% of respondents, this was still lower than expected. An additional limitation to note was that the food frequency questionnaire did not collect standard serves (often obtained with photo showcards to improve consistency in reporting (Cade et al. Citation2004)) but instead asked for portion by frequency of intake, which makes it challenging to assess dietary intake accurately. The questionnaire was designed to be easy to complete online and comparable across countries, but that did mean it was difficult to compare reported intakes with the New Zealand dietary guidelines.
Conclusion
The Covid-19 pandemic saw Aotearoa New Zealand in a ‘lockdown’ period of seven and a half weeks in April/May 2020, during which time unprecedented numbers of people stayed home, limiting their movement and economic activity. Working from home, the closure of restaurants and cafes, and some food items being unavailable in grocery stores contributed to a decreased enjoyment of grocery shopping and increased time for food preparation at home. Similar to research in other countries, the lockdown resulted in a small overall shift to an unhealthy diet, particularly increased consumption of sweet and salty snacks, alcohol and sugary drinks.
This impact of the first lockdown on New Zealanders’ shopping, cooking, and eating behaviours, and the high possibility of additional outbreaks in the coming months, emphasises the need for pandemic planning to consider ways to increase access to healthy food; restrict marketing and promotions of unhealthy food, alcohol and sweetened beverages; mitigate additional stress, particularly for younger adults; and establish clear public health nutrition messaging that avoids stigmatisation of those who are vulnerable to binge and ‘comfort’ eating.
Supplementary Table 1 Dietary Pattern Loadings
Download MS Word (15 KB)Acknowledgments
The authors would like to thank everyone that participated in the Covid Kai Survey, and those who shared the survey advertisements among their networks. The authors wish to acknowledge VLAIO (InFOOD research project) and FWO (From Food Media to Food Literacy project) for their support with the Corona Cooking Survey international study, and other members of the Corona Cooking Survey team, in particular: Drs Viktor Proesmans, Drs Jules Vrinten, Dra. Katrien Maldoy, Prof. Dr. Karolien Poels, Prof. Dr Heidi Vandebosch, Prof. Hilde Van den Bulck, Prof. Dr Maggie Geuens, Prof. Iris Vermeir, Prof. Nelleke Teughels, Prof. Dr Liselot Hudders, Prof. Dr Christophe Matthys and Prof. Dr Tim Smits.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Adhanom Ghebreyesus T. 2020. WHO Director-General’s opening remarks at the media briefing on COVID-19. Geneva; [accessed 2020 Sept 1]. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-31-august-2020.
- Ammar A, Brach M, Trabelsi K, Chtourou H, Boukhris O, Masmoudi L, Bouaziz B, Bentlage E, How D, Ahmed M, et al. 2020. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey. Nutrients. 12(16):1583.
- Anderson I. 2020 Mar 23. Coronavirus: leap in demand for home meal delivery services in New Zealand. Stuff New Zealand; [accessed 2020 May 1] https://www.stuff.co.nz/national/health/coronavirus/120487497/coronavirus-leap-in-demand-for-home-meal-delivery-services-in-new-zealand.
- Ashby NJS. 2020. Impact of the COVID-19 pandemic on unhealthy eating in populations with obesity. Obesity. 28(10):1802–1805.
- De Backer C, Teunissen L, Cuykx I, Decorte P, Pabian S, Gerritsen S, Matthys C, Al Sabbah H, Van Royen K., The Corona Cooking Survey study group. Forthcoming. An evaluation of the COVID-19 pandemic and social distancing policies in relation to planning, selecting, and preparing healthy meals: An observational study in 38 countries worldwide. Frontiers in Nutrition.
- Baker MG, Wilson N, Anglemyer A. 2020. Successful elimination of Covid-19 transmission in New Zealand. The New England Journal of Medicine. 383(8):e56.
- Bezzant N. 2020 Jun 21. Booze, baking and biking in our bubbles: studies reveal Kiwis’ health during lockdown. Stuff New Zealand. https://www.stuff.co.nz/national/health/coronavirus/300035805/booze-baking-and-biking-in-our-bubbles-studies-reveal-kiwis-health-during-lockdown.
- Bhutani S, Cooper JA. 2020. COVID-19 related home confinement in adults: weight gain risks and opportunities. Obesity. 28(9):1576–1577.
- Boyland E, Nolan S, Kelly B, Tudur-Smith C, Jones A, Halford J, Al E. 2016. Advertising as a cue to consume: a systematic review and meta-analysis of the effects of acute exposure to unhealthy food and nonalcoholic beverage advertising on intake in children and adults. The American Journal of Clinical Nutrition. 103(2):519–533.
- Cade JE, Burley VJ, Warm DL, Thompson RL, Margetts BM. 2004. Food-frequency questionnaires: a review of their design, validation and utilisation. Nutrition Research Reviews. 17(1):5–22.
- Caraher M, Dixon P, Lang T, Carr-Hill R. 1999. The state of cooking in England: the relationship of cooking skills to food choice. British Food Journal. 101(8):590–609.
- Coelho-Ravagnani CDF, Corgosinho FC, La F, Ziegler F, Marques C, Prado M, Laviano A, Mota F. 2020. Dietary recommendations during the COVID-19 pandemic. Nutrition Reviews. doi:10.1093/nutrit/nuaa067.
- Collin J, Ralston R, Hill S, Westerman L. 2020. Signalling virtue, promoting harm: unhealthy commodity industries and COVID-19. Geneva; [accessed 2020 Sept 10]. https://ncdalliance.org/resources/signalling-virtue-promoting-harm.
- Crozier SR, Inskip HM, Barker ME, Lawrence WT, Cooper C, Robinson SM. 2010. Development of a 20-item food frequency questionnaire to assess a prudent dietary pattern among young women in Southampton. European Journal of Clinical Nutrition. 64(1):99–104.
- Easterbrook-Smith G. 2020. By bread alone: baking as leisure, performance, sustenance, during the COVID-19 crisis. Leisure Sciences. doi:10.1080/01490400.2020.1773980.
- Exeter DJ, Paynter J, Bullen C. 2020. Responding to COVID-19 in the Liverpool City Region: going hard and going early in New Zealand Policy Brief. Liverpool; [accessed 2020 Sept 10]. https://www.liverpool.ac.uk/media/livacuk/publicpolicyamppractice/covid-19/PB024.pdf.
- Hagmann D, Siegrist M, Hartmann C. 2020. Acquisition of cooking skills and associations with healthy eating in Swiss adults. The Journal of Nutrtion Education and Behavior. 52(5):483–491.
- Te Hiringa Hauora/Health Promotion Agency; 2020. COVID-19: update from Te Hiringa Hauora/Health Promotion Agency; [accessed 2020 Sep 1]. https://www.hpa.org.nz/news/covid-19-update-from-te-hiringa-hauora-health-promotion-agency-0.
- International Food Information Council. 2020. Covid-19 impact on food purchasing, eating behaviors, and perceptions of food safety. [accessed 2020 May 10]. https://foodinsight.org/wp-content/uploads/2020/04/COVID-19-Consumer-Research.April2020.pdf.
- Kirkness L. 2020 Mar 31. Covid 19 coronavirus: what happened to all of New Zealand’s flour? [accessed 2020 Apr 4]. https://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=12321246.
- Lachat C, Nago E, Verstraeten R, Roberfroid D, Van Camp J, Kolsteren P. 2012. Eating out of home and its association with dietary intake: a systematic review of the evidence. Obesity Reviews. 13(4):329–346.
- Mackay S, Ni Mhurchu C, Swinburn B, Eyles H, Young L, Gontijo de Castro T. 2019. State of the food supply: New Zealand 2019. Auckland; [accessed 2020 May 20]. https://auckland.figshare.com/articles/State_of_the_Food_Supply_New_Zealand_2019/9636710.
- Martinez-Ferran M, delaGuía-Galipienso F, Sanchis-Gomar F, Pareja-Galeano H. 2020. Metabolic impacts of confinement during the COVID-19 pandemic due to modified diet and physical activity habits. Nutrients. 12:6.
- Mattioli AV, Ballerini Puviani M, Nasi M, Farinetti A. 2020. COVID-19 pandemic: the effects of quarantine on cardiovascular risk. European Journal of Clinical Nutrition. 74(6):852–855.
- Ministry of Business Innovation and Employment. 2020. COVID-19 research database. [accessed 2020 Sep 1]. https://www.mbie.govt.nz/science-and-technology/science-and-innovation/research-and-data/nzris/covid-19-research-database/.
- New Zealand Government. 2020. Unite against COVID-19: health and wellbeing. [accessed 2020 Sep 1]. https://covid19.govt.nz/health-and-wellbeing/.
- Otago Daily Times. 2020 Mar 23. Coronavirus: so long McNuggets, food delivery services remain open. [accessed 2020 Apr 3]. https://www.odt.co.nz/star-news/star-national/coronavirus-so-long-mcnuggets-food-delivery-services-remain-open.
- Peacock C. 2020 Mar 1. Panic-buying hits headlines after first coronavirus case. RNZ Mediawatch [accessed 2020 Apr 3]. https://www.rnz.co.nz/national/programmes/mediawatch/audio/2018736380/panic-buying-hits-headlines-after-first-coronavirus-case.
- Pearl RL. 2020. Weight stigma and the “quarantine-15”. Obesity. 28(7):1180–1181.
- Phillipou A, Meyer D, Neill E, Tan EJ, Toh WL, Van Rheenen TE, Rossell SL. 2020. Eating and exercise behaviors in eating disorders and the general population during the COVID-19 pandemic in Australia: initial results from the COLLATE project. International Journal of Eating Disorders. 53(7):1158–1165.
- Prickett KC, Fletcher M, Chapple S, Nguyen Doan CS. 2020. Life in lockdown: the economic and social effect of lockdown during Alert Level 4 in New Zealand. Wellington; [accessed 2020 Sept 2] http://hdl.handle.net/10063/9022.
- Puhl RM, Lessard LM, Larson N, Eisenberg ME, Neumark-Stzainer D. 2020. Weight stigma as a predictor of distress and maladaptive eating behaviors during COVID-19: longitudinal findings from the EAT study. Annals of Behavioral Medicine. 54(10):738–746.
- Robson S. 2020 Mar 25. Food banks face Covid-19 lockdown issues - demand high, supplies low. Radio New Zealand; [accessed 2020 Apr 4]. https://www.rnz.co.nz/news/national/412593/food-banks-face-covid-19-lockdown-issues-demand-high-supplies-low.
- Ruiz-Roso MB, de Carvalho Padilha P, Mantilla-Escalante DC, Ulloa N, Brun P, Acevedo-Correa D, Arantes Ferreira Peres W, Martorell M, Aires MT, de Oliveira Cardoso L, et al. 2020. Covid-19 confinement and changes of adolescent’s dietary trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients. 12(6):1807.
- Scarmozzino F, Visioli F. 2020. Covid-19 and the subsequent lockdown modified dietary habits of almost half the population in an Italian sample. Foods. 9(5):675.
- Seguin RA, Aggarwal A, Vermeylen F, Drewnowski A. 2016. Consumption frequency of foods away from home linked with higher body mass index and lower fruit and vegetable intake among adults: a cross-sectional study. Journal of Environmental and Public Health. 3074241.
- Sidor A, Rzymski P. 2020. Dietary choices and habits during COVID-19 lockdown: experience from Poland. Nutrients. 12(6):1–13.
- Statistics New Zealand. 2020a Jun 9. Media release: Record increase for grocery wholesalers in March quarter. Wellington; [accessed 2020 Sep 1]. https://www.stats.govt.nz/news/record-increase-for-grocery-wholesalers-in-march-quarter.
- Statistics New Zealand. 2020b May 20. Food price index: April 2020. Wellington; [accessed 2020 Sep 1].https://www.stats.govt.nz/information-releases/food-price-index-april-2020.
- The Obesity Health Alliance. 2020. Briefing: How are COVID-19 measures affecting the food environment? London. [accessed 2020 Sept 4] http://obesityhealthalliance.org.uk/wp-content/uploads/2020/05/OHA-polling-data-summary-final.pdf.
- Vereecken CA, Maes L. 2003. A Belgian study on the reliability and relative validity of the health behaviour in school-aged children food-frequency questionnaire. Public Health Nutrition. 6(6):581–588.
- Vereecken CA, Rossi S, Giacchi MV, Maes L. 2008. Comparison of a short food-frequency questionnaire and derived indices with a seven-day diet record in Belgian and Italian children. International Journal of Public Health. 53(6):297–305.
- Wolfson JA, Bleich SN. 2015. Is cooking at home associated with better diet quality or weight-loss intention? Public Health Nutrition. 18(8):1397–1406.
- Zeigler Z, Forbes B, Lopez B, Pedersen G, Welty J, Deyo A, Kerekes M. 2020. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obesity Research & Clinical Practice. 14(3):210–216.