
ABSTRACT
Worry is an important mediator in the relation between stressors and health. This pilot study examined whether a smartphone-based in time worry-reduction training was feasible and improved physiological health (i.e. increased heart rate variability [HRV]). A total of 26 high-worriers were randomised to an experimental or active-control condition (EC and CC respectively). Participants in both conditions registered emotions 5 times daily for a month. The EC additionally received worry-reduction training with mindfulness exercises. Primary outcomes were feasibility and HRV measured at baseline, after 2 weeks (halfway), and at 4 weeks (post-intervention). Both training conditions were feasible and well received. HRV increased in the EC and CC, but this increase did not differ between conditions. Preliminary findings suggest that both training conditions are feasible and might improve HRV, which is an important predictor of cardiovascular disease. This pilot study only provided preliminary evidence, but it laid the groundwork for future randomised controlled trials that ought to include more participants and a waitlist control group in order to get more definitive evidence of the effectiveness of the intervention.
Psychosocial stress, including work stress, is a common phenomenon in industrialised countries (European Foundation, Citation2007, Citation2012). In a large European-wide survey it was for instance found that 22% of the Europeans experience work stress (Eurofound, Citation2007). This is concerning as psychosocial stress is a substantial co-determinant of organic disease, including cardiovascular disease (CVD) (e.g. Rosengren et al., Citation2004; Steptoe & Kivimaki, Citation2013). There is consensus that the negative effect of stress on health is caused by prolonged physiological activity, like prolonged low levels of heart rate variability (HRV; Brosschot, Gerin, & Thayer, Citation2006; McEwen, Citation1998). HRV refers to the variability in timing between heart beats and low levels of HRV are predictive of CVD (Hillebrand et al., Citation2013). One mechanism that mediates the negative relation between stress and low levels of HRV is worrying (Brosschot et al., Citation2006; Ottaviani et al., Citation2016). According to the perseverative cognition hypothesis, worrying prolongs the physiological activity caused by stressful events by continuously thinking about these events (Brosschot et al., Citation2006). In a recent meta-analysis, worry was indeed associated with reduced levels of HRV (Ottaviani et al., Citation2016). In effect, worry prolongs the activation of the stressor in the mind, thereby increasing its negative effect on health. Finding ways to decrease worry might therefore be a good way to reduce physiological activity, which ultimately promotes (cardiovascular) health.
Traditionally psychological interventions take place in a clinical or research setting. A crucial question has been whether new behaviour routines, which are adopted in those artificial environments, can be transferred to other contexts (e.g. daily life). Interventions that are given in clinical settings may produce effective skill acquisition when measured in these settings, but the acquired skills may not automatically translate to real life (Kalichman et al., Citation2002). Neal, Wood, and Quinn (Citation2006) argue that this is comprehensible, because environmental cues that were associated with the “old” behaviour may still trigger the occurrence of this behaviour. Therefore, training in daily life is considered critical. To translate this to worrying, which can be considered a cognitive coping strategy that people habitually use to deal with stress, it is important to repeatedly train people in their daily lives to cope with their daily stressors in a new way.
A way to train people in their daily lives is by using ecological momentary interventions (EMIs; Mehl & Conner, Citation2012). EMIs are interventions that are implemented in the daily lives of individuals using a mobile device. A meta-analysis found that EMIs can be effective in reducing stress, anxiety, and depression, even when the EMI is not supported by a mental health professional (Versluis, Verkuil, Spinhoven, van der Ploeg, & Brosschot, Citation2016). EMIs can thus greatly reduce therapist time and thereby costs. As mobile phone use is becoming a universal phenomenon, EMIs could be a good way to reach many people. Therefore, the primary focus was to test the feasibility of an in time worry-reduction EMI and to test its effectiveness on reducing physiological activity (which is associated with worry). As primary indicator of physiological activity, ambulatory measured HRV was used. HRV is typically reduced when people are worrying (Brosschot, van Dijk, & Thayer, Citation2007; Ottaviani et al., Citation2016).
The intervention that we pilot-tested was based upon a self-help intervention that has been used by Verkuil, Brosschot, Korrelboom, Reul-Verlaan, and Thayer (Citation2011) in a paper-and-pencil format. It requires individuals to recognise when they are worrying and to address these worries in a pre-structured way. Participants are encouraged to reschedule the worry to a later point when no immediate solution to the problem or worry can be thought of. Mindfulness exercises are presented afterwards to stimulate awareness to the present moment (Kabat-Zinn, Citation2003). In addition to stimulating awareness of the present moment, these exercises help individuals to become more accepting towards these present moment experiences. Mindfulness-based interventions are considered effective in reducing anxiety and depressive symptoms in both clinical and non clinical populations (e.g. Cavanagh, Strauss, Forder, & Jones, Citation2014; Goyal et al., Citation2014). Importantly, mindfulness exercises have been previously used as EMI (for a comprehensive overview of EMI studies, including but not limited to mindfulness studies, see Versluis et al., Citation2016). However, few EMIs have been thoroughly investigated using randomised controlled trials (RCTs).
The present study was designed as a pilot study to investigate the feasibility and the preliminary effectiveness of this 4-week in time worry-reduction training with five short training sessions per day. High-worriers were randomised to the experimental condition (EC) or active-control condition (CC; i.e. registering emotions daily). This way, all participants were under the impression that they received a training, but the training in the CC did not include the supposed benefits of the specific therapeutic techniques that were present in the EC (i.e. worry-reduction and mindfulness). Such a CC allowed us to show that secondary effects – like the act of receiving daily prompts to reflect upon one's emotions – were not the main cause of potential benefits. Of primary interest was whether the training was feasible and whether it reduced physiological activity (i.e. increased ambulatory measured HRV). Additional secondary outcomes were included that can be expected to change due to the training. Specifically, heart rate (HR) – as second indicator of physiological activity – and trait and state worry were included. Because mindfulness-based interventions have previously been successful in reducing anxiety, increasing acceptance, and improving affect, these outcomes were also included.
Finally, it was hypothesised that people are not consciously aware of a substantial part of their stress-related cognition while it can still have physiological effects (Brosschot, Citation2010; Brosschot, Verkuil, & Thayer, Citation2010). This so-called unconscious stress can obviously not be directly changed by an intervention. However, there are reasons to expect that a mindfulness training can reduce unconscious stress. The attentional skills that are learned become automatic, not needing awareness – like with all skill acquisition (e.g. walking, playing the piano) (Kabat-Zinn, Citation2013). Unconscious stress was operationalised as implicit affect (Brosschot et al., Citation2010) and was represented as an increase in implicit negative affect and a decrease in positive affect.
Altogether, we expected the EMI (a) to be a feasible intervention and (b) to reduce physiological activity (i.e. increase HRV) compared to merely registering emotions. Secondly, we expected a decrease in HR, worry (both state and trait), and trait anxiety in the EC compared to the CC. Moreover, an increase was expected in acceptance and an improvement in affect (both implicit and explicit) in the EC compared to the CC.
Method
Design
A two-arm randomised controlled pilot study was conducted between April and June 2014. Participants were randomly assigned into the EC or CC using a computerised random number generator, which was operated by a researcher who was not involved in the actual data collection. Each generated number was put in a sealed envelope and was disclosed to the research assistant after the participant was included. Participants were unaware to what condition they were allocated. The institutional review board approved of the study protocol (nr. 4689348773). RCTs that followed this pilot were registered in the Dutch trial register (i.e. NTR4827 and NTR4758).
Recruitment
Dutch students were recruited via Leiden University or via acquaintances of the research assistants using advertisements asking for high-worrying students who wanted to participate in a worry-reduction training. To determine whether the training can be clinically effective only high-worrying participants were included (i.e. to be able to bring about a reduction in worry complaints). In order to include only high-worrying individuals, a cut-off score of 45 or higher on the Penn State Worry Questionnaire was used (PSWQ; Meyer, Miller, Metzger, & Borkovec, Citation1990). This cut-off can be used as a screening for generalised anxiety disorder, a condition that is fundamentally associated with worry (Behar, Alcaine, Zuellig, & Borkovec, Citation2003). Participants were excluded if they had a CVD or received psychological treatment during the study period. Twenty-six participants (69% female), with a mean age of 26.35 (SD = 8.69), met the inclusion criteria and agreed to participate.
Outcome measures
Feasibility
User experiences were examined using forced-choice and open-ended questions. Three forced-choice questions were answered using a visual analogue scale (VAS) and one using a Likert scale. Example: “To what extent did the training interfere with your daily activities?” (scored on a VAS ranging from “not at all” to “very much”) and “How did you experience the study period?” (scored on a 5-point Likert scale ranging from “very positive” to “very negative”). An open-ended example item is “How many minutes on average did it take you to complete a training session?”
Ambulatory measured cardiac activity
The ECG signal was measured for 24 h using the ekgMove sensor (Movisens GmbH, Karlsruhe, Germany). This sensor is worn on a chest belt underneath the clothes, thereby making it possible to non-invasively measure ambulatory cardiac activity. The sensor has a resolution of 12 bits, a sampling rate of 1024 Hz, and collects a single channel ECG and data on movement acceleration (using a three-axial acceleration sensor with a sampling rate of 64 Hz). HRV and HR were obtained from the data using Movisens data-analyser software (Movisens GmbH, Karlsruhe, Germany). The software uses an automated error detection algorithm to process the raw data. The root mean square of successive differences (RMSSD) was used as an index for HRV, as this is the recommended index of HRV in studies using ambulatory assessments (Pentillä et al., Citation2001). HR was computed in beats per minute (BPM). RMSSD, HR, and movement acceleration were calculated in 30 s intervals. Intervals were excluded when HR was below 30 or above 200 BPM (e.g. Thayer & Fischer, Citation2008). Thirty-second intervals were aggregated into hourly averages. Averages were only computed when the hour contained at least 30 min of valid data points. Mean movement acceleration (measured in g) was averaged over hourly periods.
Trait and state worry and stressors
The 16-item PSWQ was used to measure trait worry and items were scored on a 5-point scale ranging from “not at all” to “very typical.” Higher scores indicate higher levels of trait worry. Cronbach’s alpha was good (i.e. between .82 and .92).
State worry and stressors were ambulatory assessed by asking whether the participant had worried and whether a stressful situation had been encountered in the previous period (i.e. in the time period since the last measure) (Verkuil, Brosschot, Meerman, & Thayer, Citation2012). If participants had worried, they also had to fill in the frequency and the (combined) duration in minutes of the worry episodes. Frequency and duration of state worry were used as dependent variables. When participants had encountered a stressful situation, they had to report the frequency, duration in minutes, and severity of the stressful situation on a 5-point Likert scale ranging from “not at all severe” to “very severe.”
Affect
Explicit affect was measured by asking to what extent the participant experienced the four basic emotions. The happiness score was used as an indication of positive affect and the average of the three negative emotions was used as an index for negative affect. The dependent variable explicit affect consisted only of the explicit affect questions that were answered during the three test days (scheduled at the start, halfway, and at the end of the training). So, explicit affect questions that were measured as part of the training were not included. Reliability was estimated using the method proposed by Cranford et al. (Citation2006). On the three test days, the between-person reliability was satisfactory (i.e. Rkf between 0.98 and 0.99), indicating that the ratings for explicit negative affect were stable and suitable to detect individual differences.
Implicit affect was measured with the Implicit Positive and Negative Affect Test (IPANAT; Quirin, Kazen, & Kuhl, Citation2009). The IPANAT presents participants with a nonsense word (e.g. SUKOV) and participants indicate to what extent that word represents the emotion that is jointly presented. Each of the six nonsense-words was coupled with six different emotions (i.e. three positive and three negative), resulting in 36 pairs. Each pair was scored on a 6-point Likert scale ranging from “doesn’t fit at all” to “fits very well.” To measure implicit affect during the day, each nonsense word was presented at a different moment during the day. The psychometric properties of the IPANAT are satisfactory in student populations (Quirin et al., Citation2009). For each test day, reliability coefficients were calculated for implicit positive and negative affect (Cranford et al., Citation2006). Implicit affect had adequate between-person reliability (i.e. positive affect: Rkf between 0.92 and 0.98; negative affect: between 0.71 and 0.91). So, ratings for implicit affect were stable across each day and reflect individual differences.
Trait anxiety
The 20-item trait form of the State Trait Anxiety Inventory was used to measure trait anxiety (STAI; van der Ploeg, Citation1982). Items were answered on a 4-point Likert scale (i.e. 1 = “almost never”; 4 = “almost always”). Internal consistency was good (i.e. alpha between .92 and .94).
Acceptance
The extent to which individuals accept their negative internal experiences was measured with the 10-item Acceptance and Action Questionnaire – II (AAQ-II; Dutch translation: Jacobs, Kleen, de Groot, & A-Tjak, Citation2008), which was scored on a 7-point Likert scale ranging from “never true” to “always true.” Higher scores represent a higher level of acceptance. Internal consistency was good (i.e. alpha between .89 and .91).
Training
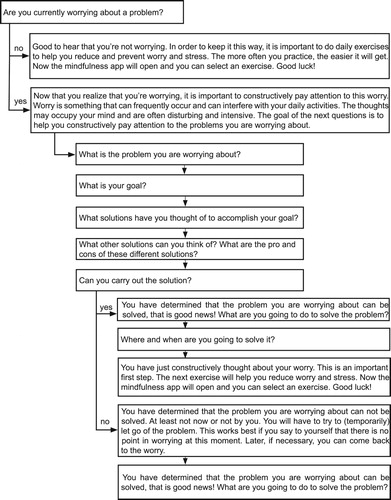
The in time training was administered using the Android-based smartphone application MovisensXS (https://xs.movisens.com). The content of the application was specifically developed for research purposes by the first author (AV). Collected data is stored via a wireless Internet connection into a secure electronic environment and can be accessed online. In the application all participants were asked to register the extent to which they experienced the four basic emotions – anger, anxiety, happiness, and sadness – using a VAS. The CC was told that repeatedly registering emotions was beneficial for health and that this was the training. The EC additionally received a worry-reduction training. This training consisted of answering a series of questions to help individuals focus their attention on the problem that was bothering them at that moment and to constructively think about it (see ). Afterwards, they were directed to the application called VGZ mindfulness coach (https://www.vgz.nl/mindfulness-coach-app), which offers 41 mindfulness exercises in audio-format. The exercises cover the central components of traditional mindfulness training; that is, breathing exercises, body scans, and mindful attention exercises (Kabat-Zinn, Citation2013). An exercise is automatically selected, however, participants are free to choose another exercise based on their preference or the duration of the exercise (i.e. varies between 1 and 37 min).
Figure 1. Questions as part of the worry-reduction training.
Procedure
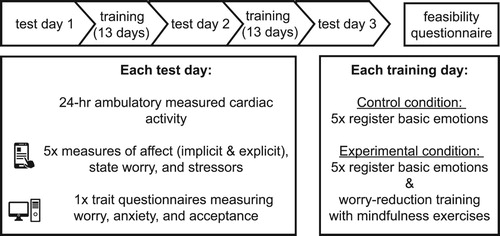
An online version of the PSWQ was sent to interested individuals to check whether they had sufficient levels of trait worry. If so, participants were contacted and screened for the other exclusion criteria. When a participant met all the inclusion criteria, a laboratory meeting was scheduled in which participants gave consent and answered demographic questions. Next, participants received information about the study schedule (see ). Specifically, participants completed three test days that were scheduled before, halfway, and at the end of the training. On these days participants received no training, but completed different assessments. First, cardiac activity was measured by wearing the ekgMove sensor from 11 am on the day to 11 am the following day. Second, the questionnaires measuring trait worry, trait anxiety, and trait acceptance were offered online and participants were asked to complete them. Third, the questions measuring state worry, stressors, implicit and explicit affect were offered on the smartphone and were to be filled in five times during the day. The MovisensXS application was used to trigger these questions between 11 am and 9.30 pm with a minimum of 45 min between triggers. The application also randomly triggered the training sessions, which were offered five times a day between 9 am and 9 pm on training days (with a minimum of 1 hr between each training session). As the usual range of triggers is between 4 and 10 per day (Mehl & Conner, Citation2012), five was considered acceptable. Participants were motivated to complete as many assessments and training sessions as possible. The triggers could be delayed for 15 min or be dismissed. To stimulate response rates, participants were rewarded 15 Euros when they answered at least 75% of the triggers. Otherwise, they received half this amount. On the last test day participants were informed that they had to fill in the feasibility questionnaire on their smartphone at post-intervention (and no reminder alarm was used).
Figure 2. Study schedule.
The necessary applications were installed on their smartphone. A smartphone was lent to participants when they did not own one. Participants were instructed about the correct use of the sensor and before each test day participants were supplied with a charged sensor.
Statistical analyses
Multilevel modelling was used to analyse whether the different outcome variables changed over time and whether this change differed per condition. For every dependent variable two multilevel models were fitted using the nlme-package in R (version 0.99.484). Model 1 included the predictor time (i.e. 0 = test day 1, 1 = test day 2, 2 = test day 3), thereby making it possible to study how individuals change over time. Model 2 also included the predictors’ condition and the Time x Condition interaction, to examine whether the change over time was different between conditions (i.e. 0 = CC and 1 = EC). A continuous time autoregressive structure was used to account for correlation in neighbouring measures. Models were fitted using a random intercept and slope, thereby allowing the value of the intercept and slope to vary between participants. Models with convergence problems were simplified by removing the random slope. Assumptions for all models were checked and considered unviolated.
RMSSD and worry duration data were log-transformed, because the raw data was not normally distributed. Untransformed means and standard deviations are reported. Models of the cardiac data were corrected for movement, which accounts for a part of HRV variance.
Results
Descriptive statistics
The total sample consisted of 26 participants (i.e. n = 11 in EC and n = 15 in CC). Demographic characteristics did not differ between conditions (see ). Four participants dropped out during test day 1. Two participants dropped out due to technical errors and two participants stopped when they became aware that the training lasted for a month (which they had failed to notice in the initial information). For these participants no physiological data was available. Demographic characteristics did not differ between non-completers and completers ().
Table 1. Means (SDs) and percentages of descriptive characteristics at baseline.
In the final sample, nine participants were in the EC and 13 participants were in the CC. Demographic characteristics did not differ between the conditions (). Mean RMSSD and HR did differ, respectively t(19) = −2.18, p = .042 and t(14.84) = 2.56, p = .022. Participants in the EC had a higher RMSSD and lower HR compared with the CC (see ). Participants completed on average 10.68 (SD = 3.04; 71%) ambulatory assessments and this number did not differ between the conditions (t(20) = −0.98, p = .341).
Primary outcomes
Feasibility
Eighteen participants (18/22, 82%) completed the feasibility questionnaire (i.e. nine in EC and nine in CC). The VASs were scored in the expected direction and no significant differences were found between conditions. The ease with which assessments could be completed on the smartphone was rated between neutral and very easy (M = 66.72, SD = 26.85), and the mean level of interference in the daily lives that participants experienced due to the training or assessments was scored between “not at all” and “neutral” (M = 39.56, SD = 29.02). All participants filled in the assessments seriously, with a score close to “very serious,” and those in the EC indicated that the mindfulness exercises were completed seriously. The length of an average training session was 2.00 min (SD = 1.50) in the CC and 6.33 min (SD = 2.45) in the EC. This difference was significant, with t(16) = −4.53 and p < .001. The log-data showed that participants completed on average 3.49 (SD = 0.77) training sessions per day and 94.27 (SD = 21.48) training sessions in total. The number of completed training sessions per day and in total was not different between conditions, t(20) = −0.74, p = .467 and t(20) = −0.77, p = .450 respectively. Lastly, the majority of participants experienced the study period as positive or neutral (i.e. 89%).
Heart rate variability
The preliminary findings showed that RMSSD increased significantly over time for all participants from 37.39 (SD = 27.00) at baseline to 44.26 (SD = 22.42) at post-intervention (with B = 0.04, p = .005). The time effect remained when entering condition as predictor (B = 0.05, p = .009), but no Time x Condition interaction was observed (B = −0.02, p = .470). The magnitude of the change in RMSSD over time, based on the change in RMSSD from pre- to post-intervention, was medium (d = 0.40).
Secondary outcomes
The following outcomes were reported for exploratory purposes and should be interpreted cautiously considering the small sample size. The models for each outcome are reported in the supplemental file. displays the means and standard deviations at baseline and at post-intervention, plus the within-subject effect size.
Table 2. Means and SDs for all outcome variables at baseline and post-intervention, and the within-subject effect size across all participants.
Heart rate
Time was not a significant predictor in Models 1 and 2 for average HR. This means that HR did not decrease over time for all participants from baseline to post-intervention, with B = −1.91, p = .192 in Model 1 and B = −1.32, p = 0.461 in Model 2. The Time x Condition interaction was also not significant (B = −1.91, p = .505). The effect size was negligible (d = .002).
Trait and state worry
Model 1 showed that the decrease in trait worry from baseline (M = 58.36, SD = 9.53) to post-intervention (M = 53.09, SD = 13.82) was not significant, with B = −2.70 and p = .057. Model 2 showed that the decrease in trait worry was not significantly different between the two conditions, with B = −2.72, p = .335, and the effect of time was not significant (B = −1.58, p = .381). The reliable change index (RCI; Jacobson & Truax, Citation1991), which can produce an unbiased estimate of individual change, showed that two individuals (i.e. one in EC and one in CC) had a reliable change in trait worry from baseline to post-intervention.
For worry frequency and duration no significant main effect of time was found in either Model 1 or 2 (i.e. worry frequency: resp. B = 0.14, p = .473 and B = −0.001, p = .998; worry duration: resp. B = 0.10, p = .395 and B = −0.03, p = .816). Moreover, the change over time in worry frequency and duration was not significantly different between the two conditions, respectively B = 0.56, p = .213 and B = 0.26, p = 325).
In terms of effect sizes, the decrease in trait worry from baseline to post-intervention was medium (d = 0.41). The effect size for state worry (both frequency and duration) was between small and medium and in the opposite direction (resp. d = 0.39 and d = 0.33).
Trait anxiety, acceptance, and explicit and implicit affect
None of the predictors in Model 1 or 2 were significant for trait anxiety, acceptance, and explicit and implicit positive and negative affect. So, trait anxiety, acceptance, and affect did not change over time and the change over time was not different between the two conditions. The effect size was negligible for trait anxiety (d = 0.05), small and in the expected direction for acceptance (d = 0.24), and mixed for affect. That is, the effect size was negligible for explicit negative affect and implicit positive affect (resp. d = 0.09 and d = 0.06), and was between small and medium – and in the opposite direction – for explicit positive affect and implicit negative affect (resp. d = 0.48 and d = 0.32).
Discussion
The aim of this pilot study was to investigate the feasibility and preliminary effectiveness of an in time worry-reduction training with mindfulness exercises via a smartphone. Results showed that the implementation of the training was feasible. Specifically, the training (and the assessments) interfered little with the daily lives of participants, were easy to complete and were taken seriously. On average, more than half of the provided daily training sessions were completed (i.e. 3.5 of the 5 daily sessions; 70%). In all participants a small to medium increase in HRV was observed from baseline to post-intervention. Contrary to our expectation, however, this decrease did not differ between conditions. Moreover, no effects were found for the secondary outcomes. Specifically, no effect was found for HR, worry (both trait and state), trait anxiety, acceptance, and affect (both implicit and explicit).
With regard to the primary outcome, our preliminary results suggest that both the in time worry-reduction training with mindfulness exercises and the emotion registration can have a positive effect on HRV, which is an important predictor of CVD. Nevertheless, an increase in HRV was only expected in the condition receiving the worry-reduction training. This is interesting as it implies that merely noticing and registering emotions can have effects on health-related parameters and can thus be seen as an intervention. This is in line with Ockhuijsen, van den Hoogen, Eijkemans, Macklon, and Boivin (Citation2014) who found positive effects of emotion registration on anxiety. The experimental set-up does not allow us to test whether emotion registration in itself can be seen as an intervention, as a non-treated waitlist control condition is lacking. Future studies with a waitlist control condition are needed.
On the secondary outcomes no statistically significant results were found. This may suggest that a 4-week worry-reduction training via a smartphone does not improve HR or self-reported psychological parameters. However, results (of both physiological and psychological outcomes) and their statistical significance in a pilot study should be carefully interpreted and cannot be taken as guarantee for treatment success or failure as the sample size is small (Thabane et al., Citation2010). Nevertheless, a pilot study is an important first step when developing a novel intervention and can be used to test the feasibility (e.g. Leon, Davis, & Kraemer, Citation2011). Given that feasibility testing was one of the primary aims of this study, it is surprising or paradoxical that a considerable number of participants failed to complete the feasibility questionnaire (i.e. 4/22, 18%). In other words, the procedure used to complete the feasibility questionnaire was not feasible. The low response rate could be due to forgetfulness, because no alarm was used to notify participants to complete the questionnaire – thereby allowing participants to complete the questionnaire at a preferred time. Participants were informed – at the start of the last test day – that the questionnaire had to be filled in (and that no alarm was given). Evidently, this procedure was insufficient and in the protocol for the RCT more emphasis should be placed on the necessity to complete the feasibility questionnaire and an alarm could be included as a reminder.
The study did produce useful information about the method to be used to implement an EMI. There was, for instance, no clear guideline on the number of training sessions that is acceptable for individuals. As a result, there is a high variability in the number of training sessions in EMI studies (Versluis et al., Citation2016). Based on guidelines for ambulatory assessments, this study incorporated five daily training sessions. The results showed that this is fairly acceptable as 70% of the training sessions were completed and the training sessions did not negatively interfere with participants’ daily activities. The study further showed that the randomisation procedure worked, that all answers were recorded and stored appropriately, and what kind of technical problems could arise (and how they could be solved). All in all, useful information was gathered that improved the implementation of the following RCTs.
Apart from the fact that this study was a pilot study with a small sample size, a number of limitations can be thought of. First, we did not obtain feasibility data from all participants, which indicates that the feasibility data must be interpreted cautiously. Moreover, no feasibility data was obtained from non-completers. The reasons for dropout could be related to their (potentially negative) experience with the EMI or to other study characteristics. If this were the case, the feasibility may have been presented too optimistically. To learn more about innovation failure, it is important to include dropout participants in the feasibility testing. Nevertheless, this may be difficult as those individuals may not be motivated to complete questionnaires (once they have dropped out).
A second limitation is that we did not have access to log data of the mindfulness application. Therefore, we were unable to examine variation in the use of the mindfulness exercises. This information could have helped to examine which exercises were used and whether the extent of the practice impacted the results. Ideally, one has this information, but in practice this may not always be feasible when working with commercially available applications (as our mindfulness application).
Another limitation pertains to the randomly triggered training sessions. Using random sampling has advantages, because there is variation in the timing of the training and this increases the generalisability of the training effect. However, individuals may not always have access to their smartphones or be able to complete a training session and this could reduce the number of completed trainings sessions. To account for this, individuals could delay the training for 15 min. Yet 15 min may be too short and studies should consider a longer delay period or personalise the training schedule (to suit an individual).
Despite the mentioned limitations, this pilot study offers an interesting insight; that is, it shows that it is possible to offer a training on a smartphone in daily life (even when there is no contact with a therapist). This is relevant considering that the field of mHealth – which refers to mobile health care – has been expanding and is considered to be the future for delivering (affordable) mental health care (Kazdin & Blase, Citation2011; Price et al., Citation2014). In clinical practice, therapists can use mHealth for different purposes; for instance, (a) to repeatedly assess treatment progress (and this information can be used to inform treatment choices), (b) to deliver homework assignments, psycho-education, or small exercises (like breathing exercises), or (c) to promote adherence by sending motivational or informative phrases (for more details on how mHealth can be used in clinical practice, see Price et al., Citation2014).
In conclusion, this pilot study found that a 4-week in time worry-reduction training via a smartphone was feasible. Furthermore, both the group that registered emotion daily and the group that received the worry-reduction training with mindfulness exercises showed an increased HRV. This increase did not differ between the groups. No effects were found on HR or on the psychological outcomes. As small pilot studies are believed to yield biased estimators of effect sizes (Leon et al., Citation2011), we believe that it is pivotal to examine the effectiveness of the currently developed, theory-based EMI in a RCT using the active control group as well as a waitlist control group. Still, the EMI methodology has a lot of potential, because it is a cost-effective strategy to reach many people. It can also be used in conjunction with traditional therapy (e.g. to support adherence or to increase therapy effects). Given the high levels of stress in society, it is important that easy interventions are available and smartphones offer great possibilities for this.
Disclosure statement
No potential conflict of interest was reported by the authors.
Notes on contributors
Anke Versluis is a PhD candidate at the Department of Health, Medical and Neuropsychology, Leiden University, the Netherlands. Her PhD project focuses on testing and comparing interventions aimed at reducing stress.
Bart Verkuil is an Assistant professor at the Department of Clinical Psychology, Leiden University, and clinician at Skils, a Dutch mental health care institution. He is currently studying whether transcutaneous vagus nerve stimulation is effective in reducing core problems in anxiety and depressive disorders.
Philip Spinhoven is a Professor at the Department of Clinical Psychology of Leiden University and the Department of Psychiatry of Leiden University Medical Center, the Netherlands. He is registered as a health care psychologist, psychotherapist and clinical psychologist by the Dutch Ministry of Health. His research is directed at depressive, anxiety and personality disorders. His overarching aim is to conduct translational research in which basic knowledge about determinants of these disorders is translated into evidence-based transdiagnostic preventive and curative interventions.
Jos F. Brosschot is a Professor by special appointment ‘psycho-physiological mechanisms of stress in daily life’ at the Department of Health, Medical and Neuropsychology, Leiden University, the Netherlands. His research focuses on the mechanisms that are responsible for the effect of the mind on the body. He has completed various laboratory and field projects examining the relation between worrying, heart activity and physical complaints.
ORCID
Anke Versluis http://orcid.org/0000-0002-9489-7925
Bart Verkuil http://orcid.org/0000-0002-9991-0690
Philip Spinhoven http://orcid.org/0000-0002-4117-335X
Jos F. Brosschot http://orcid.org/0000-0003-1472-810X
Additional information
Funding
References
- Behar, E., Alcaine, O., Zuellig, A. R., & Borkovec, T. D. (2003). Screening for generalized anxiety disorder using the Penn state worry questionnaire: A receiver operating characteristic analysis. Journal of Behavior Therapy and Experimental Psychiatry, 34(1), 25–43. doi: 10.1016/s0005-7916(03)00004-1
- Brosschot, J. F. (2010). Markers of chronic stress: Prolonged physiological activation and (un)conscious perseverative cognition. Neuroscience & Biobehavioral Reviews, 35(1), 46–50. doi: 10.1016/j.neubiorev.2010.01.004
- Brosschot, J. F., Gerin, W., & Thayer, J. F. (2006). The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research, 60, 113–124. doi: 10.1016/j.jpsychores.2005.06.074
- Brosschot, J. F., van Dijk, E., & Thayer, J. F. (2007). Daily worry is related to low heart rate variability during waking and the subsequent nocturnal sleep period. International Journal of Psychophysiology, 63(1), 39–47. doi: 10.1016/j.ijpsycho.2006.07.016
- Brosschot, J. F., Verkuil, B., & Thayer, J. F. (2010). Conscious and unconscious perseverative cognition: Is a large part of prolonged physiological activity due to unconscious stress? Journal of Psychosomatic Research, 69, 407–416. doi: 10.1016/j.jpsychores.2010.02.002
- Cavanagh, K., Strauss, C., Forder, L., & Jones, F. (2014). Can mindfulness and acceptance be learnt by self-help? A systematic review and meta-analysis of mindfulness and acceptance-based self-help interventions. Clinical Psychology Review, 34(2), 118–129. doi: 10.1016/j.cpr.2014.01.001
- Cranford, J. A., Shrout, P. E., Iida, M., Rafaeli, E., Yip, T., & Bolger, N. (2006). A procedure for evaluating sensitivity to within-person change: Can mood measures in diary studies detect change reliably? Personality and Social Psychology Bulletin, 32(7), 917–929. doi: 10.1177/0146167206287721
- European Foundation [for Improvement of Living and Working Conditions]. (2007). Fourth European working conditions survey. Luxembourg: Office for Official Publications of the European Communities.
- European Foundation [for Improvement of Living and Working Conditions]. (2012). Fifth European working conditions survey. Luxembourg: Office for Official Publications of the European Communities.
- Goyal, M., Singh, S., Sibinga, E. M. S., Gould, N. F., Rowland-Seymour, A., Sharma, R., … Haythornthwaite, J. A. (2014). Meditation programs for psychological stress and well-being. JAMA Internal Medicine, 174, 357–368. doi: 10.1001/jamainternmed.2013.13018
- Hillebrand, S., Gast, K. B., de Mutsert, R., Swenne, C. A., Jukema, J. W., Middeldorp, S., … Dekkers, O. M. (2013). Heart rate variability and first cardiovascular event in populations without known cardiovascular disease: Meta-analysis and dose-response meta-regression. Europace, 15, 742–749. doi: 10.1093/europace/eus341
- Jacobs, N., Kleen, M., de Groot, F., & A-Tjak, J. (2008). Het meten van experiëntiële vermijding: De nederlandstalige versie van de acceptance and action questionnaire (AAQ-II). Gedragstherapie, 41, 349–361.
- Jacobson, N. S., & Truax, P. (1991). Clinical significance: A statistical approach to define meaningful change in psychotherapy research. Journal of Consulting and Clinical Psychology, 59, 12–19. doi: 10.1037/0022-006X.59.1.12
- Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10, 144–156. doi: 10.1093/clipsy.bpg016
- Kabat-Zinn, J. (2013). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. New York: Bantam Books.
- Kalichman, S., Stein, J. A., Malow, R., Averhart, C., Dévieux, J., Jennings, T., … Feaster, D. J. (2002). Predicting protected sexual behaviour using the information-motivation-behaviour skills model among adolescent substance abusers in court-ordered treatment. Psychology, Health & Medicine, 7, 327–338. doi: 10.1080/13548500220139368
- Kazdin, A. E., & Blase, S. L. (2011). Rebooting psychotherapy research and practice to reduce the burden of mental illness. Perspectives on Psychological Science, 6(1), 21–37. doi: 10.1177/1745691610393527
- Leon, A. C., Davis, L. L., & Kraemer, H. C. (2011). The role and interpretation of pilot studies in clinical research. Journal of Psychiatric Research, 45, 626–629. doi: 10.1016/j.jpsychires.2010.10.008
- McEwen, B. S. (1998). Protective and damaging effects of stress mediators. New England Journal of Medicine, 338(3), 171–179. doi: 10.1056/NEJM199801153380307
- Mehl, R. M., & Conner, T. S. (2012). Handbook of research methods for studying daily life. New York: The Guilford Press.
- Meyer, T. J., Miller, M. L., Metzger, R. L., & Borkovec, T. D. (1990). Development and validation of the penn state worry questionnaire. Behaviour Research and Therapy, 28, 487–495. doi: 10.1016/0005-7967(90)90135-6
- Neal, D. T., Wood, W., & Quinn, J. M. (2006). Habits—A repeat performance. Current Directions in Psychological Science, 15, 198–202. doi: 10.1111/j.1467-8721.2006.00435.x
- Ockhuijsen, H., van den Hoogen, A., Eijkemans, M., Macklon, N., & Boivin, J. (2014). The impact of a self-administered coping intervention on emotional well-being in women awaiting the outcome of IVF treatment: A randomized controlled trial. Human Reproduction, 29, 1459–1470. doi: 10.1093/humrep/deu093
- Ottaviani, C., Lonigro, A., Medea, B., Couyoumdjian, A., Thayer, J. F., Verkuil, B., & Brosschot, J. F. (2016). Physiological concomitants of perseverative cognition: A systematic review and meta-analysis. Psychological Bulletin, 142, 231–259. doi: 10.1037/bul0000036
- Pentillä, J., Helminen, A., Jartti, T., Kuusela, T., Huikuri, H. V., Tulppo, M. P., … Scheinin, H. (2001). Time domain, geometical and frequency domain analysis of cardiac vagal outflow: Effects of various respiratory patterns. Clinical Physiology, 21, 365–376. doi: 10.1046/j.1365-2281.2001.00337.x
- Price, M., Yuen, E. K., Goetter, E. M., Herbert, J. D., Forman, E. M., Acierno, R., & Ruggiero, K. J. (2014). Mhealth: A mechanism to deliver more accessible, more effective mental health care. Clinical Psychology & Psychotherapy, 21(5), 427–436. doi: 10.1002/cpp.1855
- Quirin, M., Kazen, M., & Kuhl, J. (2009). When nonsense sounds happy or helpless: The implicit positive and negative affect test (IPANAT). Journal of Personality and Social Psychology, 97, 500–516. doi: 10.1037/a0016063
- Rosengren, A., Hawken, S., Ôunpuu, S., Sliwa, K., Zubaid, M., Almahmeed, W. A., … Yusuf, S. (2004). Association of psychosocial risk factors with risk of acute myocardial infarction in 11 119 cases and 13 648 controls from 52 countries (the INTERHEART study): case-control study. The Lancet, 364, 953–962. doi: 10.1016/s0140-6736(04)17019-0
- Steptoe, A., & Kivimaki, M. (2013). Stress and cardiovascular disease: An update on current knowledge. Annual Review of Public Health, 34, 337–354. doi: 10.1146/annurev-publhealth-031912-114452
- Thabane, L., Ma, J., Chu, R., Cheng, J., Ismaila, A., Rios, L. P., … Goldsmith, C. H. (2010). A tutorial on pilot studies: The what, why and how. BMC Medical Research Methodology, 10(1), 42. doi: 10.1186/1471-2288-10-1
- Thayer, J. F., & Fischer, J. E. (2008). Heart rate variability, overnight urinary norepinephrine and C-reactive protein: Evidence for the cholinergic anti-inflammatory pathway in healthy human adults. Journal of Internal Medicine, 265, 439–447. doi: 10.1111/j.1365-2796.2008.02023.x
- van der Ploeg, H. M. (1982). De zelf-beoordelings vragenlijst (STAI-DY): de ontwikkeling en validatie van een Nederlandstalige vragenlijst voor het meten van angst. Tijdschrift voor psychiatrie, 24, 576–588.
- Verkuil, B., Brosschot, J. F., Korrelboom, K., Reul-Verlaan, R., & Thayer, J. F. (2011). Pretreatment of worry enhances the effects of stress management therapy: A randomized clinical trial. Psychotherapy and Psychosomatics, 80, 189–190. doi: 10.1159/000320328
- Verkuil, B., Brosschot, J. F., Meerman, E. E., & Thayer, J. F. (2012). Effects of momentary assessed stressful events and worry episodes on somatic health complaints. Psychology & Health, 27, 141–158. doi: 10.1080/08870441003653470
- Versluis, A., Verkuil, B., Spinhoven, P., van der Ploeg, M. M., & Brosschot, J. F. (2016). Changing mental health and positive psychological well-being using ecological momentary interventions: A systematic review and meta-analysis. Journal of Medical Internet Research, 18(6), e152. doi: 10.2196/jmir.5642