
ABSTRACT
Digital education is intertwined with matters of global economics, geopolitics, as well as ongoing changes in what counts as knowledge, skills and learning. We have witnessed throughout the COVID-19 pandemic how technology has been embraced within education from online classes to innovative mobile learning approaches and evaluating humanoid robots in education is the next step. Driven by a need to keep pace with the evolving techno- and socio-economic requirements, schools and society are increasingly adopting artificial intelligence (AI) and robots in their daily activity. This paper presents a feasibility case study in digital health education where a humanoid robot was chosen to teach based on its form and function. With an imperative to establish a strong and sustainable learning space, the aim of this paper is to present results and learn about the future of digital health education from humanoid robots being deployed in digital health learning spaces. The paper concludes by highlighting key design challenges in unbundling educational approaches in the context of humanoid robots. It is intended that the outcomes of this paper will extend beyond the COVID-19 pandemic by contributing to the humanoid robot technology discussion that will push towards more futuristic artificial intelligence in and for education.
Introduction
In 2021, the paradigm of a physical classroom, human teacher and students is no longer the norm and key technological advancements are changing our educational infrastructure and where we merge the best technology with the best of human teaching (Salmon Citation2019). COVID-19 has resulted in rapid digital transformation across all parts of society and education delivery in particular. Technology adds a level of complexity to a pedagogical context and these developments create both opportunities and tensions for education and learning (Selwyn Citation2020). The driving trends in technologies can already be observed, with big data, virtual reality (VR) and augmented reality (AR) experiences, deployment of artificial intelligence and ubiquitous technology creating digital divides and affecting education (Hoadley and Uttamchandai Citation2021). These novel and emerging technologies have a role to play in the changing context of learning, teaching and assessment, and the educational sector will be undeniably and significantly influenced by AI and robots.
Although robotics has not still found its place in school curricula, a growing number of robotic interactions take place in formal and informal education. Proponents of humanoid robots in learning environments advocate that central to our digital future is the need for educational design research, with all participants in a variety of learning spaces (Cox Citation2021). The dichotomy of educational methodologies and practices aligned with the fast-paced technological innovation is the challenge (OECD Citation2016; Selwyn et al. Citation2019).
The aim of this research is to discuss what we can learn about the future of digital health education from humanoid robots being deployed in a health care facility, and what issues arise that necessitate a rethinking of such technology in education settings. The use of robots in healthcare has advanced in recent years as the demand for health care services far outpaces the availability of staff and robots are seen as a viable solution to address the shortage. Indeed, the global medical robotics market is expected to reach USD 12.7 billion by 2025 from an estimated USD 5.9 billion in 2020 at a rate of up to 20% per annum (Market and Markets, Citationn/d). One key factor propelling the growth of this market is the advantage offered by robot-assisted training in rehabilitation therapy.
This paper presents a feasibility case study in a diabetes care setting, where the humanoid robot was ‘teaching’ the patient about their diabetes self-management. The study highlights important areas concerning human behaviour and the impact of using a humanoid robot on the learning of the participant is explored. The results of our feasibility study suggest an enormous potential to deploy innovative digital transformation opportunities in health education.
Theoretical framework
Artificial intelligence in education (AIED) combines the fields of computer science, education, psychology and other facets of the learning sciences (Timms Citation2016; Gasteiger, Hellou, and Ahn Citation2021). The benefits of AI in education originates from three fundamental factors that it can firstly increase capacity and productivity of educators, secondly that it provides valuable observations to enhance teaching and learning, and support learners’ well-rounded development and lastly AI in Education can deliver autonomous learning recommendations (The Institute for Ethical AI in Education Citation2020). Undeniably influenced by AI, humanoid robots have a special appeal in education, enhancing the interaction between content-user, the student; and the content-producers, the teachers; along with presenting content material (Henkemans et al. Citation2013).
The integration of humanoid robots in education is not solely an educational issue of learning theory or pedagogical design, nor is it simply a technical matter of how to design and develop an effective robot. Constructivism and constructionism are the main theories underpinning educational robotics, where they contribute to teaching and learning practices (Piaget Citation1959; Papert Citation1980), and where problem-based and experimental learning approaches are the most usual methodologies (Hoffmann et al. Citation2015). Collaborative learning is also evidenced where robots, when matched with the instructional goals and learning intentions, are a positive teaching tool (Plauska and Damaševičius Citation2014; Belpaeme et al. Citation2018). A robot’s ability to perform repetitive tasks repeatedly, precisely, and presenting digital data in a humanoid appearance is endearing to most learners and combined with their flexibility robots allow educators to propose different models for a wide range of educational use (Spolaôr and Benitti Citation2017). Robots also facilitate learning and have been found to create an engaging environment, motivating, as well as enhancing learning performance (Alimisis Citation2013). The use of social robots with older adults in their homes found that cognitive games delivered on a robot may be a valuable addition to existing cognitive stimulation activities and was considered by participants useful in improving cognitive functioning (Gasteiger et al. Citation2021). In the healthcare setting, some research indicates that an autonomous robot can be as effective as a human clinician in the delivery of a behavioural change intervention to improve the dietary behaviour of patients (Robinson et al. Citation2020).
Rational of present study
This study sought to conduct a deeper exploration of the context and impact of an educational intervention using a social robot in a healthcare setting using a feasibility case study approach (Bryman Citation2008; Harrison et al. Citation2017). Ethical approval was gained by the University Hospital Galway Ethics committee. This feasibility case study involved the use of a humanoid robot, personalised as the Diabetes Audio Visual Educator (DAVE) which was developed by Softbank Robotics (SoftBank Robotics Citation2015). DAVE was used to demonstrate interactive health education related to diabetes disease and condition management.
Method
Design, participants, setting and sample size
The study was conducted at the outpatient diabetic centre at University Hospital Galway. Thirteen patients with diabetes (nine male, four females) were recruited, all adults. Only one participant had type 1 diabetes, with the remaining participants having type 2 diabetes. This feasibility study employed a single group repeated measures design with two time points (baseline and post-intervention).
Development of the educational intervention using DAVE
The intervention was developed in consultation with a multi-disciplinary team incorporating a public and patient involvement approach (PPI). This is where members of the public or patients are actively involved in research projects (e.g. study design) rather than just being subjects. This innovative paradigm recognises the valuable expertise of the lived experience to give novel insights to science and helps to ensure that the research questions being asked are relevant and hence impactful (Richards, Snow, and Schroter Citation2016). The project team programmed an application embedded within the DAVE robot featuring specific concise videos, in an interactive Q&A session format, explaining aspects of the diabetes disease and condition management. The selected videos in this particular study application aligned to learning outcomes addressing the topic of the self-management of hypoglycaemia; including how to use a glucometer to measure HbA1c. The eight teaching and learning resources were developed in collaboration with the diabetic nurse specialist. Authentic learning (Herod Citation2003) was central to the design and development of these materials and ‘the context in which they would be used’, with Lombardi and Oblinger (Citation2007) emphasising that this form of learning requires connection-building. In making authentic learning effective, Lombardi and Oblinger (Citation2007) describe how learners look for connections, that habits come with practice and the context has a role to play. These three principles underpinned the development and use of the videos along with best practice in designing the video tutorials appropriately for the participants (Koumi Citation2006; Ronchetti Citation2010).
DAVE was programmed to feature an artificial intelligence-based audiovisual interactive framework. The robot was able to visually recognise human features and begin the interaction that was continued between DAVE and patient through the patient’s audio feedback to questions, which was responded to by DAVE, thereby progressing the lesson and ensuring the patient was engaged.
Measures
To operationalise the variable Knowledge Transfer a questionnaire was generated from the accompanying video guides in the programmed application for DAVE. The questionnaire was administered to participants at two time points – pre and post the DAVE intervention. To assess whether interacting with the intervention influences future usability, participants were invited to complete the Modified Telehealth Usability Questionnaire for DAVE (MTUQD). The MTUQD is comprised of 5 subscales. The ease of use and learning subscale consisted of 3 items (α = .89), the interface subscale consisted of 5 items (α = .90), the interface quality subscale consisted of 7 items (α = .30), the reliability subscale consisted of 4 items (α = .60) and the satisfaction and future use subscale consisted of 6 items (α = .89). The overall MTUQD was found to have very good internal consistency (α = .89). Participants also completed the Diabetes Distress Screening Scale (DDS) (Fisher et al. Citation2008), the Attitude towards Diabetes Scale (DES) (Parmanto et al. Citation2016; Anderson et al. Citation2000), and the Learning Experiences with Robots questionnaire (Chang et al. Citation2010).
The DES scales based on a 28-item attitude towards diabetes scale is further subcategorised into three subscales based on diabetes-related psychosocial self-efficacy, (i) ‘Managing the psychosocial aspects of Diabetes’ covers items about patient’s perceived ability to seek needed social support, be motivated to manage diabetes-induced stress and make diabetes-related self-decisions, (ii) ‘Assessing dissatisfaction and readiness to change’ contains items which measure patient’s perceived ability to recognise parts of their diabetes self-management plan that they are dissatisfied with and their ability to know when they are prepared and ready to make the changes in their diabetes self-management plan, (iii) ‘Setting and achieving diabetes goals’ addresses the patient’s perceived ability to recognised applicable and achievable diabetic self-management goals and overcome barriers. The DES was found to have excellent internal consistency (α = .95).
The Diabetes Distress Screen (DDS) scale is an instrument for the assessment of diabetes-related emotional distress. Items are rated on a six-level scale ranging from not a problem, a slight problem, moderate problem, somewhat serious problem, a serious problem, to a very serious problem. The Learning Experience with Robots questionnaire (LER) is a 9-item measure to assess the efficacy of the DAVE in demonstrating health education based on a 5-point Likert scale. The LER gathered data from the participants examining factors such as authenticity, engagement and learning motivation. For example, participants had to rate on a scale factors such as ‘I like to learn about my diabetes with DAVE’, ‘I would use DAVE to learn about my diabetes for a long time’ and ‘I want to use DAVE to learn about diabetes again.’ Cronbach’s alpha for the DDS and LER were found to be .93 and .95, respectively, demonstrating excellent internal consistency across the measures. The means and standard deviations (SDs) for all variables can be seen in .
Table 1. Means and standard deviations of the MTUQD, DDS, DES and LER total and subscale scores.
Results
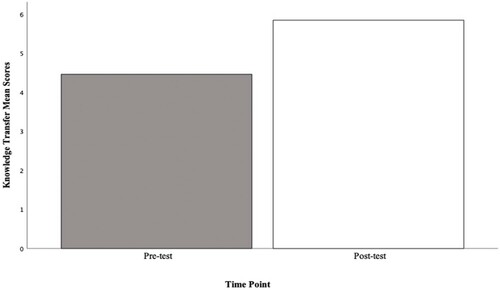
A dependent samples t-test indicated a significant difference in knowledge scores from baseline to post-intervention, with participants demonstrating a significant increase in knowledge from baseline (M = 4.46, SD = 2.18) to post-intervention (M = 5.85, SD = 2.58), (t (12) = −2.84, p = 0.15), illustrates the results.
Figure 1. Knowledge transfer scores at baseline and post-intervention.
An independent samples t-test also revealed a non-significant trend in knowledge increase between males and females with males gaining more knowledge post intervention than females (t(11) = 1.66, p = 0.13), the Mean and Standard Deviations are presented in .
Table 2. Means and standard deviations of between groups knowledge transfer scores at baseline and follow-up.
Intercorrelations between variables were conducted using Pearson’s correlation coefficient. The results shown in reveal a significant inverse association between knowledge and the satisfaction and future use subscale of the modified TUQ (r(10) = −0.52, p = .04).
Table 3. Summary of inter-correlations between knowledge transfer scores and the MTUQD subscales.
Discussion and conclusion, including future-facing recommendations
This feasibility study demonstrated promising findings for the use of a social robot for patient education in a diabetes day care setting. Significant improvements in patient knowledge were observed from baseline to follow-up signifying the potential of DAVE to provide health education effectively. Participants with the lowest scores at baseline perceived significantly greater benefits from DAVE. Overall, patients reported high levels of acceptance and engagement with this method of intervention and reported low or slight levels of associated diabetes distress. Obvious limitations of this study include a small sample size, no control measure, and selection biases relative to a cohort study. Notwithstanding these limitations, the current research extends the range of potential educational applications of social robots beyond well-established target areas, e.g. dementia, autism spectrum disorder to deliver health education on blood glucose management to patients with diabetes.
Within a health education setting, a framework for educational design to promote the transfer of learning by Botma et al. (Citation2015) consisted of two principles: (1) establishing a community of learning and (2) the primacy of a learning outcome. Though the creation of a sustained learning community was not extensively addressed in this study design, the study was very much guided by learning outcomes addressing the topic of the self-management of hypoglycaemia. The learning outcomes were met in the use of DAVE because when the learning involves embodiment, it has been demonstrated that learning is better for learners to interact with physical entities rather than virtual agents (Belpaeme et al. Citation2018). Similarly, this study raised the possibility of social robots delivering a range of educational interventions for other aspects of health behaviour targets (e.g. diet and exercise). While further research that replicates and extends the current results in larger scale trials is necessary to build greater confidence in its acceptability and impact, the study provides a solid basis for that research program. The development of such interventions would benefit from continued stakeholder engagement and from the integration of behaviour change techniques (BCTs) (Michie et al. Citation2013) and other relevant learnings from behavioural science to develop educational content that will also successfully impact on health behaviour change, thus significantly improving clinical outcomes. The pedagogical design considerations for robots teaching, factoring digital literacy of participants, as well as feedback data collection are all avenues for the next stage of our DAVE investigations, along with examining varied educational environments.
In leading and innovating in the field of digital education, we must recognise that the learning cycle is longer than the fast-changing technology cycle and all stakeholders need to be active agents, not just in the implementation of innovations but also in their design and development. It is without doubt that as technology advances, we recognise that artificial intelligence, robot experiences and exposure in education are powerful, but the impact of its application in health education should not be left to chance. It is intended that the outcomes of this project will extend beyond health education by creating a prototype for learning that will encourage a connected paradigm shift in education more broadly.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Alimisis, D. 2013. “Educational Robotics: Open Questions and New Challenges.” Themes in Science and Technology Education 6 (1): 63–71.
- Anderson, R. M., M. M. Funnell, J. T. Fitzgerald, and D. G. Marrero. 2000. “The Diabetes Empowerment Scale: A Measure of Psychosocial Self-Efficacy.” Diabetes Care 23 (6): 739–743. doi:https://doi.org/10.2337/diacare.23.6.739.
- Belpaeme, T., J. Kennedy, A. Ramachandran, B. Scassellati, and F. Tanaka. 2018. “Social Robots for Education: A Review.” Science Robots 3: 21. doi:https://doi.org/10.1126/scirobotics.aat5954.
- Botma, Y., G. H. Van Rensburg, I. M. Coetzee, and T. Heyns. 2015. “A Conceptual Framework for Educational Design at Modular Level to Promote Transfer of Learning.” Innovations in Education and Teaching International 52 (5): 499–509. doi:https://doi.org/10.1080/14703297.2013.866051.
- Bryman, A. 2008. Social Research Methods. 3rd edn. Oxford: Oxford University Press.
- Chang, C. W., J. H. Lee, C. Y. Wang, and G. D. Chen. 2010. “Improving the Authentic Learning Experience by Integrating Robots Into the Mixed-Reality Environment.” Computers & Education 55 (4): 1572–1578. doi:https://doi.org/10.1016/j.compedu.2010.06.023.
- Cox, A. M. 2021. “Exploring the Impact of Artificial Intelligence and Robots on Higher Education Through Literature-Based Design Fictions.” International Journal of Education Technology in Higher Education 18 (3): 1–19. doi:https://doi.org/10.1186/s41239-020-00237-8.
- Fisher, L., R. E. Glasgow, J. T. Mullan, M. M. Skaff, and W. H. Polonsky. 2008. “Development of a Brief Diabetes Distress Screening Instrument.” The Annals of Family Medicine 6 (3): 246–252. doi:https://doi.org/10.1370/afm.842.
- Gasteiger, N., H. S. Ahn, C. Gasteiger, C. Lee, J. Lim, C. Fok, B. A. MacDonald, G. H. Kim, and E. Broadbent. 2021. “Robot-Delivered Cognitive Stimulation Games for Older Adults: Usability and Acceptability Evaluation.” ACM Transactions on Human-Robot Interaction (THRI) 10 (4): 1–18. doi:https://doi.org/10.1145/3451882.
- Gasteiger, N., M. Hellou, and H. S. Ahn. 2021. “Factors for Personalization and Localization to Optimize Human–Robot Interaction: A Literature Review.” International Journal of Social Robotics, doi:https://doi.org/10.1007/s12369-021-00811-8.
- Harrison, H., M. Birks, R. Franklin, and J. Mills. 2017. “Case Study Research: Foundations and Methodological Orientations [34 Paragraphs].” Forum Qualitative Sozialforschung / Forum: Qualitative Social Research 18: 1. doi:https://doi.org/10.17169/fqs-18.1.2655.
- Henkemans, O. A. B., B. P. Bierman, J. Janssen, M. A. Neerincx, R. Looije, H. van der Bosch, and J. A. van der Giessen. 2013. “Using a Robot to Personalise Health Education for Children with Diabetes Type 1: A Pilot Study.” Patient Education and Counseling 92 (2): 174–181. doi:https://doi.org/10.1016/j.pec.2013.04.012.
- Herod, L. 2003. Adult Learning from Theory to Practice. Family Literacy Events Committee. https://jarche.com/wp-content/uploads/2015/12/adult_learning.pdf.
- Hoadley, C., and S. Uttamchandani. 2021. “Current and Future Issues in Learning, Technology, and Education Research.” Spencer Foundation 1–38. https://archive.nyu.edu/bitstream/2451/63364/2/Hoadley%20Chris%20White%20Paper%2020211020%20%28final%29.pdf.
- Hoffmann, M., L. Plumanns, L. Lenz, K. Schuster, T. Meisen, and S. Jeschke. 2015. “Enhancing the Learning Success of Engineering Students by Virtual Experiments.” In Learning and collaboration Technologies: Second international conference – international conference on human-computer interaction, edited by P. Zaphiris and A. Ioannou, 394–405. Cham: Springer.
- The Institute for Ethical AI in Education. 2020. Interim Report, Towards a shared vision of Ethical AI in Education. University of Buckingham. https://www.buckingham.ac.uk/wp-content/uploads/2020/02/Summary-The-Institute-for-Ethical-AI-in-Educations-Interim-Report-Towards-a-Shared-Vision-of-Ethical-AI-in-Education.pdf.
- Koumi, J. 2006. Designing Video and MultImedia for Open and Flexible Learning. London: Routledge.
- Lombardi, M. M., and D. G. Oblinger. 2007. “Authentic Learning for the 21st Century: An Overview.” Educause Learning Initiative 1 (2007): 1–12.
- Market and Markets. n/d. “Medical Robots Market By Product & Service [Instrument & Accessories, Robotic Systems (Surgical Robots, Rehabilitation Robots)], Application (Laparoscopy, Radiation Therapy, Pharmacy), End User (Hospital, Ambulatory Surgery)-Global Forecast To 2025.” Online. Accessed 19 November 2021. https://www.marketsandmarkets.com/Market-Reports/medical-robotic-systems-market-2916860.html.
- Michie, S., M. Richardson, M. Johnston, C. Abraham, J. Francis, W. Hardeman, M. P. Eccles, et al. 2013. “The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions.” Annals of Behavioral Medicine 46 (1): 81–95. doi:https://doi.org/10.1007/s12160-013-9486-6.
- OECD. 2016. Innovating Education and Educating for Innovation: The Power of Digital Technologies and Skills. Paris: OECD Publishing. doi:https://doi.org/10.1787/9789264265097-en
- Papert, S. 1980. Mindstorms: Children, Computers, and Powerful Ideas. New York: Basic Books.
- Parmanto, B., A. N. Lewis, Jr, K. M. Graham, and M. H. Bertolet. 2016. “Development of the Telehealth Usability Questionnaire (TUQ).” International Journal of Telerehabilitation 8 (1): 3–10. doi:https://doi.org/10.5195/ijt.2016.6196.
- Piaget, J. 1959. Language and Thought of the Child. New York: Humanities Press.
- Plauska, I., and R. Damaševičius. 2014. “Educational Robots for Internet-of-Things Supported Collaborative Learning.” In International Conference on Information and Software Technologies, edited by Dregvaite Giedre and Damasevicius Robertas, 346–358. Cham: Springer International Publishing.
- Richards, T., R. Snow, and S. Schroter. 2016. “Co-creating Health: More Than a Dream.” BMJ 345. doi:https://doi.org/10.1136/bmj.i4550.
- Robinson, N. L., J. Connolly, L. Hides, and D. J. Kavanagh. 2020. “Social Robots as Treatment Agents: Pilot Randomized Controlled Trial to Deliver a Behavior Change Intervention.” Internet Interventions 21: 100320. doi:https://doi.org/10.1016/j.invent.2020.100320.
- Ronchetti, M. 2010. “Using Video Lectures to Make Teaching More Interactive.” International Journal of Emerging Technologies in Learning (iJET) 5 (2): 45–48.
- Salmon, G. 2019. “May the Fourth Be with you: Creating Education 4.0.” Journal of Learning for Development-JL4D 6 (2): 95–115. https://jl4d.org/index.php/ejl4d/article/view/352.
- Selwyn, N. 2020. “Digital Education in the Aftermath of COVID-19: Critical Concerns and Hopes.” Techlash 1: 6–10.
- Selwyn, N., T. Hillman, R. Eynon, G. Ferreira, J. Knox, F. Macgilchrist, and J. M. Sancho-Gil. 2019. “What’s Next for Ed-Tech? Critical Hopes and Concerns for the 2020s.” Learning, Media and Technology 45 (1): 1–6.
- SoftBank Robotics. 2015. “Pepper the humanoid and programmable robot.” SoftBank Robotics. https://www.softbankrobotics.com/emea/en/pepper.
- Spolaôr, N., and F. B. V. Benitti. 2017. “Robotics Applications Grounded in Learning Theories on Tertiary Education: A Systematic Review.” Computers & Education 112: 97–107. doi:https://doi.org/10.1016/j.compedu.2017.05.001.
- Timms, M. J. 2016. “Letting Artificial Intelligence in Education Out of the Box: Educational Cobots and Smart Classrooms.” International Journal of Artificial Intelligence in Education 26 (2): 701–712. doi:https://doi.org/10.1007/s40593-016-0095-y.