
ABSTRACT
Irish children’s physical activity (PA) levels are below national guidelines. Schools are an ideal setting to promote PA but it remains challenging. This study evaluates the effectiveness of a step-back approach to Project Spraoi (PS); a facilitator (Energizer) led school-based PA intervention. Each Energizer in year one had 2 contact days per week with all classes (n = 11). A ‘step-back’ progression, with 50% less Energizer contact time, in year two and no Energizer contact in year three, was adopted. Objectively measured PA and cardiorespiratory fitness (CRF) were measured annually with the same children (n = 85). Stakeholders (children (n = 287), teachers (n = 11) and other school staff (n = 8)), participated in process evaluation data collection. After an initial increase in year one, PA levels declined in year two and three; yet all children were more active at intervention end compared to baseline (p < 0.05). The biggest barriers to implementation were a lack of time and ‘lack of Energizer contact’, with the Energizer cited as the most frequently identified facilitator by all stakeholders. This study outlines the importance of a facilitator in the long-term success of health promotion intervention delivery in a primary school context.
Introduction
Irish children (6–17 years) are recommended to accumulate at least 60 min per day of moderate-to-vigorous intensity physical activity (MVPA) or an average of at least 60 min of MVPA per day across the week, for health (Healthy Ireland Citation2016). Yet, the most recent National Report Card for Children and Adolescents graded overall physical activity levels at only a C- (Research Work Group for Ireland’s Report Card on Physical Activity in Children and Adolescents Citation2022). In terms of increasing children’s PA, the school environment has the potential to make important differences and presents several opportunities for intervention (Lavelle, Mackay, and Pell Citation2012; Van Sluijs, McMinn, and Griffin Citation2008; Vasques et al. Citation2014; Ward, Saunders, and Pate Citation2007). Effective school environments provide opportunities for interventions to embody a culture of care, and to be fully inclusive of all children; regardless of any existing racial or socio-economic background differences (Cavanagh et al. Citation2012). Therefore, researchers and policy-makers have identified schools as logical settings for intervention.
School-based PA interventions fall broadly into 5 categories: physical education (PE) curriculum, classroom activity breaks, active commuting to school, modified playgrounds, and multifaceted approaches that combine all the above to adapt the whole school environment (Gråstén Citation2017). The literature is saturated with systematic reviews demonstrating the effectiveness of school-based approaches (Dobbins et al. Citation2013; Dudley et al. Citation2011; Kriemler et al. Citation2011; Lai et al. Citation2014; Naylor et al. Citation2015), and highlighting the importance of multi-component models (Kriemler et al. Citation2011). Some effective school-based PA studies have advocated for specialist-led interventions to ensure the quality of intervention delivery (Telford et al. Citation2016; Tompsett et al. Citation2017), while others see longitudinal and cost-effective benefits to giving generalist teachers the autonomy to lead PA intervention activities (Holt, Bartee, and Heelan Citation2013; Naylor et al. Citation2006; Ryde, Booth, and Brooks Citation2018).
‘Project Spraoi’ (PS) is one such example of a specialist-led, multicomponent school-based intervention. PS is a randomized control trial (reg: ISRCTN92611015) that promotes PA and healthy eating in primary schools through an ‘Energizer’ led intervention and was delivered in Cork, Ireland. PS (www.projectspraoi.cit.ie) is based on the internationally recognized and fully evaluated ‘Project Energize’ (PENZ) (Rush et al. Citation2012). PS has been found to have a positive impact on the prevalence of overweight and obesity, as well as a wide range of health markers including cardio-respiratory fitness, PA levels, fundamental movement skills and nutritional knowledge of Irish primary school children (Bolger et al. Citation2018; Merrotsy et al. Citation2018; O’Leary et al. Citation2018). Furthermore, PS has been found to positively impact the school context and those who interact with it, including teachers, parents and pupils (O’Leary et al. Citation2019).
Many interventions developed in a research setting appear to be effective in controlled conditions but often do not translate well into less controlled, real life contexts (Durlak and DuPre Citation2008; Glasgow et al. Citation2006). Process evaluations are rarely conducted and reported alongside these interventions, thus leaving a void in understanding how to translate the implementation of seemingly effective interventions in new contexts outside the confines of their modeled research conditions (Durlak and DuPre Citation2008; Moore et al. Citation2015).
As implementation science is an emerging area in PA research (Naylor et al. Citation2015), this study sought to investigate the effectiveness of a step-back approach to the delivery of PS, in which over the course of three years, the Energizer gradually reduced contact time with the intervention school and gave class teachers increased autonomy over intervention delivery to simulate a less controlled, real life context. As the presence of the Energizer is reduced in the school, it is hypothesized that the intervention would no longer be prioritized and, as a result, the PA levels of participants would decline. In order to test this hypothesis, objectively measured PA and cardiorespiratory fitness (CRF) were measured annually with the same children (n = 85). Focus groups, interviews, surveys and PA logs were also conducted to evaluate intervention implementation and impact, dose delivered, barriers/facilitators and teacher’s attitudes towards intervention delivery.
Methods
Intervention delivery
Central to the delivery of the PS intervention was the researcher’s ability to act as an ‘Energizer’ and be an ‘agent of change’ within their intervention school(s). This included leading healthy lifestyle initiatives, modeling PA and healthy eating classes, and providing resources on PA and healthy eating to help teachers achieve the intervention goals of delivering 20 min extra daily moderate-vigorous physical activity (MVPA) to students during the school day and improving student’s nutritional knowledge and behaviors. Further details about the intervention methods are published elsewhere (Coppinger et al. Citation2016) and can be found on the Project Spraoi website (https://projectspraoi.cit.ie/).
As advocated for in the literature (Naylor et al. Citation2015), a whole school approach to intervention delivery was adopted by PS, with all classes in the school receiving equal contact time with the Energizer each week. In year one, the Energizer had 2 contact days per week in the school where all classes (n = 11) received two 20-minute, Energizer lead PA or healthy eating lessons (Delaney, Dinneen, and O’Shea Citation2015). A ‘step-back’ progression with 50% less Energizer contact time in year two and no Energizer contact in year three was adopted by the researchers to gradually give class teachers increased autonomy over intervention delivery. On the days when the Energizer was not present, each teacher was responsible for delivering 20 min MVPA to all students in their class to meet the requirements of PS.
Impact evaluation
Throughout the three year intervention, all classes (n = 11) received the intervention. This paper evaluates the impact of a step-back approach of Energizer delivery of PS on children’s PA levels, as well as a variety of health markers including CRF and PA intensity. Measures were taken at the same timepoint pre (Sept) and post (June) intervention in year one and two. In year three, a one-year post intervention (June) impact evaluation was conducted with the same cohort, allowing for longitudinal comparisons.
PA was objectively measured using triaxial ActiGraph GT3X + accelerometers (Fort Walton Beach, FL, USA) worn on the right hip during all waking hours, except for when swimming or bathing for 7 consecutive days. Parents were reminded, via daily text messages, to ensure that children wore their accelerometer each morning. ActiLife software (version 6.13.3) was used in the data analysis. Inclusion criteria required wear time of >3 days of the week, with ≥600 min recorded per day, which has been shown to give adequate reliability and power among children (Riddoch et al. Citation2007). Of 85 children who received accelerometers at baseline, 68 (80%) met these requirements. Periods of 20 min of consecutive zero counts were indicated as non-wear time (Esliger et al. Citation2005). The first day of wear time was removed from the dataset to allow for subject reactivity (Esliger et al. Citation2005). The last day of wear time (i.e. Day 7) was also excluded from analysis. Cut points developed by Evenson et al. (Citation2008), were used to compute average time spent in MVPA daily. In accordance with the validation protocol used by Evenson et al. (Citation2008), a 15-second epoch length was used to measure activity as using epoch lengths that differ from those originally used to validate the selected activity cut-points introduces significant error into resulting estimates of sedentary behavior and PA intensity levels (Banda et al. Citation2016).
Process evaluation
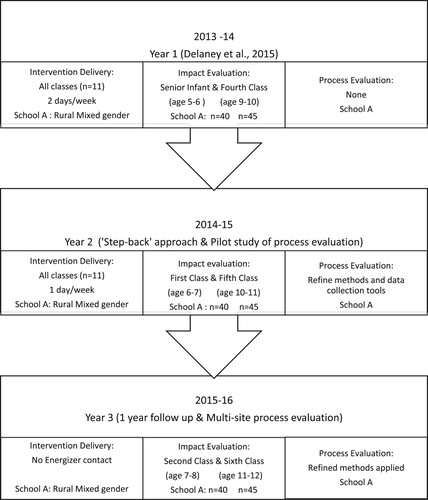
At intervention commencement in year one, a documented process evaluation component was not initially planned. As the intervention evolved, however, so too did the need and scope for a process evaluation of PS. Process evaluations are considered essential to understanding the feasibility of an intervention and identifying any necessary refinements. They can also provide important information on the decision to proceed to the next stage of evaluation (Sebire et al. Citation2019). Process evaluation ran concurrently to intervention delivery, with data collected at multiple timepoints (Sept, Mar, June) throughout the school year. The methods for process evaluation were developed and refined over three phases from 2013 to 2016 (). The schedule for process evaluation data collection was tied to the primary school calendar. Data was collected at multiple time points throughout the school year in order to capture the different intervention components from the perspective of all relevant stakeholders in the complex school environment throughout the course of the intervention. Adaptations to intervention delivery and refinement of the data collection tools throughout the course of the pilot study were enabled due to ongoing analysis and feedback of process evaluation data to intervention implementers. After the first year of implementation of PS, impact evaluation results revealed discrepancies between expected and observed results (Delaney, Dinneen, and O’Shea Citation2015). This motivated the implementation of comprehensive methods for process evaluation in year two, in order to investigate the process by which PS achieved its effects in context.
Figure 1. Summary of study progression.
The methods for process evaluation of PS were guided by the three themes outlined by Moore et al. (Citation2015); (i) implementation, (ii) context and (iii) mechanisms of impact. Themes were further subcategorized into six evaluation dimensions; (i) barriers and facilitators, (ii) adaptations, (iii) fidelity, (iv) dose delivered, (v) activities, and (vi) interactions and suitable data collection tools were identified from the literature, piloted and refined before use. Triangulation of findings was achieved by using multiple tools including surveys, PA logs, reflective journals, and semi-structured interviews, to measure the same evaluation dimension (Griffin et al. Citation2014). Furthermore, the use of a wide range of informants has been identified by Shenton (Citation2004) as another useful way of triangulating data.
PA logs were used to test the hypothesis that intervention delivery would be reduced. Teachers were asked to quantify the amount of extra daily PA they delivered, in order to examine whether the intervention (20mins extra daily MVPA) was being delivered as intended (Grant et al. Citation2013). Qualitative methods were selected as more flexible tools for examining facilitators and barriers to implementation, unexpected outcomes and participant’s interactions with intervention activities (Schneider et al. Citation2009).
Throughout the course of the school year, stakeholders, including children (n = 20), teachers (n = 11), and other school staff (n = 8) participated in some, or all, of the process evaluation data collection in order to gain a comprehensive, multi-perspective understanding of the delivery of the PS intervention from the primary actors involved ().
Table 1. Summary of process evaluation methods and participating stakeholders.
Statistical analysis
Quantitative data was analyzed using SPSS statistical analysis for Windows, version 24 (IBM Corp, Armonk NY, 2015). The alpha level required for significance for all tests was set at p < .05. Effect size was interpreted using Cohen’s classification of effect size (small 0.2 ≤ d < 0.5, medium 0.5 ≥ d < 0.8, large ≥0.8) (Cohen Citation1988). A repeat measure analysis of variance (ANOVA) was used to assess age differences in the mean markers of health between year 1 and year 3. Baseline data acted as a covariate to control for individual’s start measurements prior to the PS intervention.
Participants were only included in comparative analysis if they were present during each of the intervention data collection days over the course of three years between October 2013 and May 2016. However, due to non-compliance of accelerometer wear time during follow up evaluations, the ‘intention-to-treat’ principle was applied to the PA data in order to avoid bias in the estimation of intervention effect due to reduced sample size over time (Gupta Citation2011). Those included in PA analysis at baseline, were maintained in the sample throughout all evaluation time points, with any missing values replaced by the mean/median score of the group.
The process evaluation of Project Spraoi employed the three themes described by the British MRC guidance for process evaluation; context, implementation and mechanisms of impact (Craig et al. Citation2008; Moore et al. Citation2015). Each theme was further subcategorized into key dimensions for evaluation. Interviews were recorded and transcribed verbatim. All interview transcripts were checked by a second researcher to ensure accuracy of recording. Thematic analyses were conducted on the qualitative data from the interviews and open-ended survey questions. Data was coded into categories based on Program theory using a computer assisted qualitative data analysis software (CAQDAS), Quirkos (version 2.0) (Quirkos Software Citation2021). During the coding process, CAQDAS was used to identify key words and associated synonyms across all attached data sources. Emerging themes were identified and reviewed several times to see if they still worked in relation to the new data sources. After all data was coded, subcategories were identified per theme if necessary, and when possible a distinction between inhibiting and promoting was made for each of the influencing factors. Next, the coded text was retrieved to create an overview per theme (or per subcategory). Furthermore, the frequency of counts per sub-category/theme was calculated to evaluate open-ended survey questions. Themes and subcategories identified and coded during analysis were reviewed by a second researcher to ensure consistency and compatibility throughout.
Participants
The school context in which this study was conducted was a rural mixed gender school in Cork, Ireland. The school was equipped with modest facilities which included a small tarmac yard and grass pitch on site, with limited access to an indoor hall a short distance off-site. Due to developmental differences based on children of these age ranges being at the advent of important ages for forming and understanding health habits (Coppinger et al. Citation2016; Rush et al. Citation2012) the impact evaluation sample was divided into a junior (n = 40) and senior (n = 45) cohort for the purpose of analysis. The junior cohort included males (n = 20) and females (n = 20) aged 6.03 ± 0.33 years at induction. The senior cohort included males (n = 25) and females (n = 20) aged 10.15 ± 0.35 years. Measures were taken pre and post intervention with the same junior (n = 40) and senior cohort (n = 45) in year one and two. In year three, a one-year post intervention impact evaluation was conducted with the same cohort, allowing for longitudinal comparisons.
Results
Impact evaluation
In order to control for the effect of increased stride length of children over the three-year evaluation period due to significantly increased height, change in height was used as a covariate during analysis of cardio-respiratory fitness (CRF). The time taken to complete the 550 m walk/run test decreased in both subgroups over time (), indicating increased CRF. Despite both subgroups recording faster times, a significant increase in CRF was only observed in the senior cohort (p = 0.03, ES = 0.13). Analysis of CRF revealed statistically significant age effects on 550 m run/walk time as the senior cohort recorded significantly faster times than the junior cohort with a large effect size (p < 0.0005, n2 = 0.573).
Table 2. Summary of height and CRF changes during the intervention period.
Physical activity
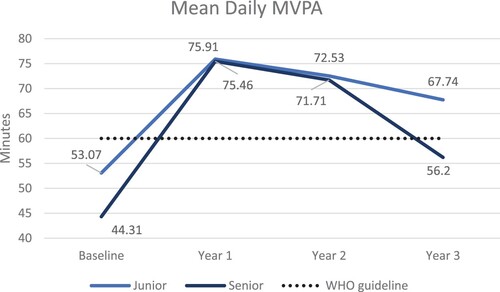
At baseline, 68 students (junior, n = 32; senior, n = 36) met the required accelerometer wear time to be included in analysis. The introduction of the PS intervention saw a significant increase in the mean daily MVPA of both subgroups at the end of year 1 when compared to their baseline measures (mean difference = 22.83 mins, p = 0.00; senior mean difference = 31.16 mins, p = 0.00) (). In the junior cohort only, the mean daily minutes of MVPA accumulated by participants between year 1 and year 3 significantly decreased (p = 0.034, n2 = 0.107). No significant changes in mean daily minutes of MVPA was noted amongst the senior cohort over the course of the intervention. Despite both subgroups PA levels decreasing as the intervention was stepped back in year two and three, the children in both subgroups were significantly more active at intervention end in year three compared to a baseline, prior to the introduction of PS (p < 0.05) ().
Figure 2. Change in mean daily MVPA over time.
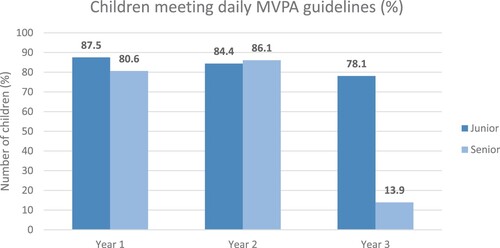
outlines the proportion of children meeting the recommended PA guidelines at each time point. The proportion of children meeting the MVPA guidelines decreased in both subgroups over the course of the three years with the greatest drop off occurring between year 2 and year 3. No significant differences were found to exist between the junior and senior cohorts in year 1 and year 2. However, in year 3, the senior cohort of sixth class children were significantly less likely to meet the recommended MVPA guidelines than their junior counterparts in second class (p = 0.00, ES = 0.64).
Figure 3. Percentage of children meeting the World Health Organisation MVPA guideline.
Implementation
PA logs were completed weekly by all class teachers (n = 11) during year 2. Teachers indicated by ticking the box, the type and time, either 5, 10, 15 or 20 min of activity delivered by them each day. The mean amount of extra daily MVPA (mins) delivered by teachers during year two of PS was analyzed using a between and within subject’s ANOVA test. The within subjects’ factor was time and the between subjects’ factor was the class taught by the relevant teacher. Teachers who taught class groups from junior infants to second class were assigned to the junior category (n = 6), while teachers who taught class groups from third class to sixth class were assigned to the senior category (n = 5). Over the course of the academic year, the mean amount of extra daily PA delivered by teachers each month varied significantly (p < 0.05, n2 = 0.68) (). The interaction effect of time and class group taught indicated that over the course of the school year, junior class teachers delivered significantly more extra daily PA than teachers of senior classes (p = 0.002, n2 = 0.355).
Figure 4. Mean extra daily PA delivered by teachers during year 2.
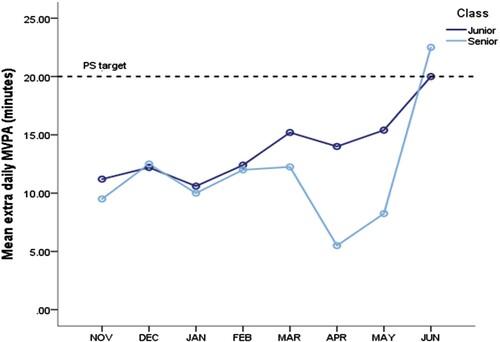
A Bonferroni post-hoc test was conducted to explore the monthly difference in the amount of extra daily MVPA delivered by teachers within the eight months of intervention implemented in year two. Although the increase in the amount of extra daily MVPA delivered by teachers over time did not occur in a linear manner, a statistically significant mean increase of 10.9 min (p = 0.005) was reported between November and June. The largest increase in the amount of extra daily MVPA delivered by teachers was between April and June (mean difference = 11.5mins, p = 0.021).
Further analysis of the PA logs using a one-sample t-test revealed discrepancies in the fidelity of intervention delivery by class teachers. The mean amount of extra MVPA delivered by teachers daily (12.2 min) was significantly lower than the PS target of 20 min from November to May (p < 0.05). Both groups did not achieve the target amount of extra daily MVPA until June ().
Contextual barriers and facilitators to intervention delivery
Barriers and facilitators to intervention delivery were primarily identified through survey data from class teachers (n = 11), interviews with children (n = 20) and support staff (n = 8). The views of the Energizer (n = 1), documented in the reflective journal, were also considered during analysis. Common themes triangulated from multiple sources (interviews, surveys, and reflective journal) were highlighted and are presented in .
Table 3. Barriers and Facilitators to intervention delivery (Year2).
The biggest barrier to the implementation of PS identified by teachers was a lack of time to deliver extra daily MVPA due to an already overcrowded curriculum. This barrier was particularly prevalent among teachers with senior classes during months of particularly low fidelity in implementing 20 min extra daily MVPA (: April & May). During these months many teachers, particularly those teaching senior classes, expressed a ‘lack of time’ and feeling of ‘pressure’ as they had ‘too many other subjects to teach’ and ‘very little time due to preparation for exams’. The second most frequently identified barrier by teachers and school staff to PA was a ‘lack of facilities and equipment’ (45%).
The Energizer was the most frequently identified facilitator by all stakeholders (teachers, parents, school staff and students). Teachers and school staff praised the ‘enthusiasm’, ‘creativity’ and ‘organisation’ of the Energizer, with one describing the Energizer as a ‘live interactive resource’. Parents identified the Energizer as being ‘a great role model’ and having ‘a positive influence’ on the school and their child’s behavior ().
Table 4. Data collection tools and methods.
Mechanisms of impact: interactions
The teacher survey assessed the teacher’s attitudes towards delivering PS and their interactions with the intervention and Energizer. At the beginning of year 2, 90.9% of teachers either disagreed or strongly disagreed that delivering 20 min extra daily MVPA was manageable. This feedback motivated adaptations to intervention delivery, by trying to incorporate the facilitators identified by teachers, such as breaking the 20minute MVPA block down into shorter activity breaks throughout the day and providing additional resources to meet the teachers’ needs, for example, cross-curricular and classroom games.
As the intervention progressed during year 2, a significant change in teachers’ attitudes towards delivering the extra 20 min MVPA daily over time was identified using a repeated measures ANOVA (p = 0.004, ES = 0.21). A significant linear increase was evident in the number of teachers who agreed that delivering 20 min extra daily MVPA was manageable (p = 0.02). Inversely, a significant linear decrease in the number of teachers who disagreed that delivering 20 min extra daily MVPA was manageable was also identified (p = 0.001).
However, during follow up evaluation at the end of year three, 75% of teachers either disagreed or strongly disagreed that delivering the 20 min MVPA was manageable. Most teachers (80%) identified ‘lack of Energizer contact’ as a barrier to intervention delivery and many (63%) suggested the need for ongoing resources to maintain intervention activities in the school. It was noted that when the Energizer no longer had a presence in the school, that the intervention was forgotten.
I think I definitely tried at the start of the year to keep PS going with my class, but when the Energizer isn’t there to keep driving it on, other programmes take its place and it gets forgotten. (Teacher – senior class group)
Discussion
The findings of this study suggest that a step-back approach to PS has a negative impact on intervention delivery. This is evidenced by a notable initial increase in MVPA during the first year, but then the levels of both the junior and senior cohorts decreased over the course of the intervention. This could be attributed to the step-back approach to intervention delivery, as the linear decrease in MVPA appears to align with the reduced Energizer contact each year. The mean difference in minutes of accumulated daily MVPA between year one and year two is −3.75 min (senior cohort) and −3.38 min (junior cohort), while the mean difference between year two and year three is −15.51 min (senior cohort) and −4.79 min (junior cohort). Based on this it seems that Energizer contact can positively influence children’s activity levels, with two contact days per week more effective than one, but one contact day more effective than none. This supports the recommendations of Tompsett et al. (Citation2017) who concluded that the most effective PA and fundamental movement skill interventions are those that are led by specialist teachers. Similarly, Telford et al. (Citation2016) reported that specialist teachers can provide higher levels of PA during PE lessons than the usual practice PE conducted by generalist classroom teachers, and that this can make a small contribution to children’s whole day PA levels. However, as the study was confined only to curricular PE class, there was no evidence to suggest that it translated to an increase in daily habitual PA or to an increase in the number of students meeting PA recommendations. Given that Domville et al. (Citation2019) has reported organizational barriers (the need for a principal/headteacher to promote PA opportunities), institutional barriers (some schools not prioritizing PA/PE), interpersonal barriers (i.e. some individuals actively reducing PA opportunities) and intrapersonal barriers (i.e. lack of specialist PE training and varying teacher interest in sport and PA), trying to promote PA in the primary school setting continues to be a challenging task. Therefore, it could be suggested that there is also a need for daily PA classes and/or supplementary PA strategies.
In the absence of the Energizer in year three, there was a significantly greater drop off in MVPA amongst the senior cohort, in comparison to their junior counterparts (p < 0.05) (). This could be attributed to the significant interaction effect between class and time identified in analysis of the PA logs which suggested that teachers of junior classes delivered significantly more MVPA to their students over the course of the school year than teachers of senior class groups (p < 0.05).
Findings from the PA logs indicate low to moderate fidelity of PS. Neither cohort achieved the target amount of extra daily MVPA (20 min) until June. Similar issues with fidelity were encountered by Naylor et al. (Citation2006) who reported that during the Action Schools! BC intervention, teachers only delivered, on average, two-thirds of the prescribed 15 min of additional daily PA. In the current study, low levels of fidelity could be linked to a lack of facilities, particularly in times of poor weather, which was identified by 45% of teachers as a barrier to intervention delivery. This is consistent with the findings of the review by Nathan et al. (Citation2018) which reported that factors such as inadequate facilities and adverse weather have been cited as barriers to the implementation of school-based interventions across seven studies.
Low intervention fidelity could also be linked to the burden of curricular time constraints which was the most frequently identified barrier to implementation of PS according to both teachers (91%) and pupils (70%). This finding supports that of Hall et al. (Citation2014) and the review conducted by Naylor et al. (Citation2015) who reported that time constraints was the most frequently (23/29 studies) noted barrier that influenced implementation of PA interventions in schools. However, Greenberg et al. (Citation2005) identified time constraints (time to prepare and deliver the PA intervention, competing demands and teacher overload) as a school level resourcing issue with increasing focus on academic achievement resulting in decreased PA opportunities in schools (Howie and Pate Citation2012). It seems curricular time constraints in this context can only be overcome if changes occur at a government policy level considering in similar developed countries such as Australia, the Department of Education has been found to exert the most influence on school priorities (Keshavarz et al. Citation2010).
Data from teacher surveys in year two revealed a statistically significant improvement in teachers’ attitudes towards delivering PS, as facilitators were maximized, and controllable barriers minimized. Rather than passively receiving interventions, participants interact with them, and outcomes are produced by these interactions in context (Pawson and Tilley Citation1997). Therefore, one could speculate that more successful implementation and, consequently, more pronounced anthropometric differences could potentially have been attained if school-related barriers had been minimized and facilitators maximized earlier in the study in year one (2013/14). Inversely, in year three when the Energizer no longer had contact with the school, teachers’ attitudes towards delivering PS worsened and interestingly the lack of Energizer contact became one of the most frequently identified barriers to implementation of PS, second only to curricular time constraints.
The availability of data relating to dose delivered by teachers enabled the researchers to interpret discrepancies between expected and observed outcomes and investigate whether the limited effects of PS were due to poor intervention design or poor fidelity (Grant et al. Citation2013; Moore et al. Citation2015). A dose–response relationship exists between PA and its associated health benefits. Specifically, improvements in health outcomes tend to increase with increasing levels of PA (Foulds, Bredin, and Charlesworth Citation2014; Williams Citation2013). The mechanisms of impact of PENZ, the intervention upon which PS is based, suggest that for children to achieve the health benefits associated with the intervention, they need to undertake 20 min extra daily MVPA through Energizer and/or teacher led ‘Huff & Puff’ sessions. Based on the teachers’ self-report PA logs, children received significantly less extra daily MVPA than the target set and therefore given the dose–response relationship, improvements in health outcomes were not maximized.
It should not be ignored, however, that PS does have the potential to have lasting positive effects on PA levels; with the children in both junior and senior cohorts found to be significantly more active at intervention end in year three compared to baseline, prior to the introduction of PS (). Children’s CRF also improved, with both cohorts recording faster times at each evaluation point. Further analysis of CRF revealed statistically significant age effects, indicating that the senior cohort recorded significantly faster times than their junior counterparts. Similar findings have been reported by Roriz De Oliveira et al. (Citation2014) among a cohort of Portuguese children, which may be explained by the increase in aerobic capacity of children as they age (Borms Citation1986).
Strengths and limitations
A key limiting factor of this study was the lack of comparable control data over the three-year evaluation period. A delayed treatment approach was employed when recruiting control schools to participate in PS, whereby participating control schools were introduced into the PS program after a period of two-years (Coppinger et al. Citation2016). Therefore, the control subgroup for this study was only valid for the first two years of evaluation before they went on to become an intervention school.
Another limiting factor was the size of the study sample. These results are based on one rural mixed gender school and as such, have limited population generalisability. Further investigation into the implementation of PS across a variety of schools is needed in order to draw more informed conclusions about the effectiveness of the PS intervention.
The strengths of the study include the longitudinally tracked data of the same participants for 3 years, the objective collection of data with regards to PA using accelerometery and the availability of process, as well as impact evaluation data.
Conclusion
The step-back approach to PS reported in this study, indicates that PS can have positive lasting effects on children’s health, fitness and PA levels. Children in both junior and senior cohorts recorded significantly more daily MVPA in year 3 than at baseline prior to the introduction of PS. Improvements were also realized in CRF over the course of the intervention. However, the gradual reduction in Energizer contact time negatively influenced the amount of daily MVPA children undertook with a significant decrease in children’s objectively measured MVPA observed between year 1 and year 3. This may also be attributable to a lack of intervention fidelity among teachers as they delivered significantly less daily MVPA than the PS target of 20 min. In order to optimize the effectiveness of PS, the barriers posed by the school context need to be addressed. The Energizer has a key role to play, as all stakeholders identify having access to a PA specialist as being the greatest facilitator to intervention delivery in a primary school context.
Acknowledgements
The primary schools including teachers, principals, other staff members and students from the participating schools are thanked for their support, contribution and co-operation. The authors declare that the results of the current study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. The authors declare there is no conflict of interest.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Yvonne O’Byrne
Yvonne O’ Byrne has a first-class honours degree in Sport and Exercise and undertook her PhD research in the Department of Sport, Leisure and Childhood Studies at Munster Technological University, Ireland. Yvonne was a member of the Project Spraoi research team, Ireland’s first, fully evaluated, nutrition and physical activity intervention that reached over 2000 Cork primary schoolchildren. Her research specialises in the implementation of an extensive process evaluation of Project Spraoi and the related contextual factors that affect the delivery and adoption of health promotion interventions in primary schools.
J. Dinneen
J. Dinneen has a primary degree in Physical Education from the University of Limerick and a Masters in Equality Studies from University College Dublin. Joan has taught at MTU for over 20 years, specialising in exercise and fitness instruction and health promotion. Settings based health promotion is Joan’s main research interest; she is centrally involved in the campus based health promotion initiative at MTU Cork and is also a member of the Project Spraoi research team. Over the years Joan has represented the university on local and national health promotion initiatives including Cork Sports Partnership, the National Steering Committee for GP Exercise Referral and the Register of Exercise Professionals, Ireland.
T. Coppinger
Dr T. Coppinger is a Trustee of the Academy of Nutrition Sciences, Global Lead, Academic Constituency Member of the Nutrition Society’s Membership Committee and an Associate Editor at BMC Sports Science, Medicine, and Rehabilitation. She is a registered public health nutritionist and Conferred Fellow of the Association for Nutrition. Tara has also been a board member of Munster Technological University (MTU) Research Ethics Committee for the past ten years and is the Co-Director of Project Spraoi, which won a United Nations Interagency Task Force on Non-Communicable Diseases (NCD) Award in recognition of its outstanding contribution towards the NCD related sustainable Development Goals. Tara has published over 50 internationally peer reviewed articles related to physical activity and nutritional intake.
References
- Banda, J. A., K. F. Haydel, T. Davila, M. Desai, S. Bryson, W. L. Haskell, D. Matheson, and T. N. Robinson. 2016. “Effects of Varying Epoch Lengths, Wear Time Algorithms, and Activity Cut-points on Estimates of Child Sedentary Behavior and Physical Activity from Accelerometer Data.” PLoS One 11 (3): e0150534. https://doi.org/10.1371/journal.pone.0150534.
- Bolger, L. E., L. A. Bolger, C. O’Neill, E. Coughlan, W. O’Brien, S. Lacey, and C. Burns. 2018. “Age and Sex Differences in Fundamental Movement Skills among a Cohort of Irish School Children.” Journal of Motor Learning and Development 6 (1): 81–100. https://doi.org/10.1123/jmld.2017-0003.
- Borms, J. 1986. “The Child and Exercise: An Overview.” Journal of Sports Sciences 4 (1): 3–20. https://doi.org/10.1080/02640418608732093.
- Cavanagh, T., A. Macfarlane, T. Glynn, and S. Macfarlane. 2012. “Creating Peaceful and Effective Schools through a Culture of Care.” Discourse: Studies in the Cultural Politics of Education 33: 443–455. https://doi.org/10.1080/01596306.2012.681902.
- Cohen, J. 1988. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates, Publishers.
- Coppinger, T., S. Lacey, C. O’Neill, and C. Burns. 2016. “‘Project Spraoi’: A Randomized Control Trial to Improve Nutrition and Physical Activity in School Children.” Contemporary Clinical Trials Communications 3: 94–101. https://doi.org/10.1016/j.conctc.2016.04.007.
- Craig, P., P. Dieppe, S. Macintyre, S. Michie, I. Nazareth, and M. Petticrew. 2008. “Developing and Evaluating Complex Interventions: The New Medical Research Council Guidance.” BMJ 337 (p. 185).
- Delaney, L., J. Dinneen, and J. O’Shea. 2015. “Project Spraoi: A Strategy to Improve Nutrition and Increase Physical Activity in Primary School Children.” Master’s thesis, Cork Institute of Technology.
- Dobbins, M., H. Husson, K. DeCorby, and R. L. LaRocca. 2013. “School-based Physical Activity Programs for Promoting Physical Activity and Fitness in Children and Adolescents Aged 6 to 18.” The Cochrane Database of Systematic Reviews 2. https://doi.org/10.1002/14651858.CD007651.pub2. Art. No.: CD007651.
- Domville, M. S., P. M. Watson, D. J. Richardson, and L. E. F. Graves. 2019. “Educator Perspectives on Factors Influencing Children’s School-Based Physical Activity.” Health Promotion International 34: 931–940. https://doi.org/10.1093/heapro/day041.
- Dudley, D., A. Okely, P. Pearson, and W. Cotton. 2011. “A Systematic Review of the Effectiveness of Physical Education and School Sport Interventions Targeting Physical Activity, Movement Skills and Enjoyment of Physical Activity.” European Physical Education Review 17 (3): 353–378. https://doi.org/10.1177/1356336X11416734.
- Durlak, J. A., and E. P. DuPre. 2008. “Implementation Matters: A Review of Research on the Influence of Implementation on Program Outcomes and the Factors Affecting Implementation.” American Journal of Community Psychology 41 (3–4): 327–350. https://doi.org/10.1007/s10464-008-9165-0.
- Esliger, D. W., J. L. Copeland, J. D. Barnes, and M. S. Tremblay. 2005. “Standardizing and Optimizing the use of Accelerometer Data for Free-living Physical Activity Monitoring.” Journal of Physical Activity and Health 2 (3): 366–383. https://doi.org/10.1123/jpah.2.3.366.
- Evenson, K. R., D. J. Catellier, K. Gill, K. S. Ondrak, and R. G. McMurray. 2008. “Calibration of Two Objective Measures of Physical Activity for Children.” Journal of Sports Sciences 26: 1557–1565. https://doi.org/10.1080/02640410802334196.
- Foulds, H. J., S. S. Bredin, and S. A. Charlesworth. 2014. “Exercise Volume and Intensity: A Dose-Response Relationship with Health Benefits.” European Journal of Applied Physiology 114: 1563–1571. https://doi.org/10.1007/s00421-014-2887-9.
- Glasgow, R. E., L. M. Klesges, D. A. Dzewaltowski, P. A. Estabrooks, and T. M. Vogt. 2006. “Evaluating the Impact of Health Promotion Programs: Using the RE-AIM Framework to Form Summary Measures for Decision Making Involving Complex Issues.” Health Education Research 21 (5): 688–694. https://doi.org/10.1093/her/cyl081.
- Grant, A., S. Treweek, T. Dreischulte, R. Foy, and B. Guthrie. 2013. “Process Evaluations for Cluster-Randomised Trials of Complex Interventions: A Proposed Framework for Design and Reporting.” Trials 14: 15. https://doi.org/10.1186/1745-6215-14-15.
- Gråstén, A. 2017. “School-based Physical Activity Interventions for Children and Youth: Keys for Success.” Journal of Sport and Health Science 6 (3): 290–291. https://doi.org/10.1016/j.jshs.2017.03.001.
- Greenberg, M. T., C. E. Domitrovich, P. A. Graczyk, and J. E. Zins. 2005. “The Study of Implementation in School-based Preventive Interventions: Theory, Research, and Practice.” Promotion of Mental Health and Prevention of Mental and Behavior Disorders, (3), Washington, DC: U.S. Department of Health and Human Services.
- Griffin, T. L., M. J. Pallan, J. L. Clarke, E. R. Lancashire, A. Lyon, J. M. Parry, and P. Adab. 2014. “Process Evaluation Design in a Cluster Randomised Controlled Childhood Obesity Prevention Trial: The WAVES Study.” International Journal of Behavioural Nutrition and Physical Activity 11: 112.
- Gupta, S. K. 2011. “Intention-to-treat Concept: A Review.” Perspectives in Clinical Research 2 (3): 109–112. https://doi.org/10.4103/2229-3485.83221.
- Hall, W. J., M. Schneider, D. Thompson, S. L. Volpe, A. Steckler, J. M. Hall, and R. Fisher. 2014. “School Factors as Barriers to and Facilitators of a Preventive Intervention for Pediatric Type 2 Diabetes.” Translational Behavioral Medicine 4: 131–140. https://doi.org/10.1007/s13142-013-0226-z.
- Healthy Ireland. 2016. Get Ireland Active! The National Guidelines on Physical Activity for Ireland. Dublin: Department of Health and Department of Transport, Tourism and Sport. https://www.hse.ie/eng/about/who/healthwellbeing/our-priority-programmes/heal/physical-activity-guidelines/
- Holt, E., T. Bartee, and K. Heelan. 2013. “Evaluation of a Policy to Integrate Physical Activity into the School day.” Journal of Physical Activity and Health 10 (4): 480–487. https://doi.org/10.1123/jpah.10.4.480.
- Howie, E. K., and R. R. Pate. 2012. “Physical Activity and Academic Achievement in Children: A Historical Perspective.” Journal of Sport and Health Science 1 (3): 160–169. https://doi.org/10.1016/j.jshs.2012.09.003.
- Keshavarz, N., D. Nutbeam, L. Rowling, and F. Khavarpour. 2010. “Schools as Social Complex Adaptive Systems: A New Way to Understand the Challenges of Introducing the Health Promoting Schools Concept.” Social Science & Medicine 70: 1467–1474. https://doi.org/10.1016/j.socscimed.2010.01.034.
- Kriemler, S., U. Meyer, E. Martin, E. M. F. van Sluijs, L. B. Andersen, and B. W. Martin. 2011. “Effect of School-Based Interventions on Physical Activity and Fitness in Children and Adolescents: A Review of Reviews and Systematic Update.” British Journal of Sports Medicine 45 (11): 923–930. https://doi.org/10.1136/bjsports-2011-090186.
- Lai, S. K., S. A. Costigan, P. J. Morgan, D. R. Lubans, D. F. Stodden, J. Salmon, and L. M. Barnett. 2014. “Do School-based Interventions Focusing on Physical Activity, Fitness, or Fundamental Movement Skill Competency Produce a Sustained Impact in These Outcomes in Children and Adolescents? A Systematic Review of Follow-up Studies.” Sports Medicine 44: 67–79. https://doi.org/10.1007/s40279-013-0099-9.
- Lavelle, H. V., D. F. Mackay, and J. P. Pell. 2012. “Systematic Review and Meta-analysis of School-based Interventions to Reduce Body Mass Index.” Journal of Public Health 34 (3): 360–369. https://doi.org/10.1093/pubmed/fdr116.
- McEvilly, N. 2013. “Investigating the Place and Meaning of ‘Physical Education’ to Preschool Children: Methodological Lessons from a Research Study.” Sport, Education and Society. https://doi.org/10.1080/13573322.2012.761965
- Merriam, S. B., J. Johnson-Bailey, M. Y. Lee, Y. Kee, and M. Muhamad. 2001. “Power and Positionality: Negotiating Insider/Outsider Status within and Across Cultures.” International Journal of Lifelong Education 20 (5): 405–416.
- Merrotsy, A., A. L. McCarthy, J. Flack, S. Lacey, and T. Coppinger. 2018. “Project Spraoi: Dietary Intake, Nutritional Knowledge, Cardiorespiratory Fitness and Health Markers of Irish Primary School Children.” International Journal of Child Health and Nutrition 7: 63–73. https://doi.org/10.6000/1929-4247.2018.07.02.3.
- Moore, G., S. Audrey, M. Barker, L. Bond, C. Bonnell, W. Hardeman, L. Moore, et al. 2015. “Process Evaluation of Complex Interventions: Medical Research Council Guidance.” British Medical Journal 350: h1258. https://doi.org/10.1136/bmj.h1258.
- Nathan, N., B. Elton, M. Babic, Nicole McCarthy, Rachel Sutherland, Justin Presseau, Kirsty Seward, et al. 2018. “Barriers and Facilitators to the Implementation of Physical Activity Policies in Schools: A Systematic Review.” Preventive Medicine 107: 45–53. https://doi.org/10.1016/j.ypmed.2017.11.012.
- Naylor, P. J., H. M. Macdonald, J. A. Zebedee, K. E. Reed, and H. A. McKay. 2006. “Lessons Learned from Action Schools! BC—an ‘Active School’ Model to Promote Physical Activity in Elementary Schools.” Journal of Science and Medicine in Sport 9 (5): 413–423. https://doi.org/10.1016/j.jsams.2006.06.013.
- Naylor, P. J., L. Nettlefold, D. Race, C. Hoy, M. C. Ashe, J. W. Higgins, and H. McKay. 2015. “Implementation of School Based Physical Activity Interventions: A Systematic Review.” Preventive Medicine 72: 95–115. https://doi.org/10.1016/j.ypmed.2014.12.034.
- O’Leary, M., E. Rush, S. Lacey, C. Burns, and T. Coppinger. 2018. “Cardiorespiratory Fitness is Positively Associated with Waist to Height Ratio and School Socio Economic Status in Irish Primary School Aged Children.” Journal of Sport and Health Research 10: 389–402.
- O’Leary, M., E. Rush, S. Lacey, C. Burns, and T. Coppinger. 2019. “Project Spraoi: Two Year Outcomes of a Whole School Physical Activity and Nutrition Intervention Using the RE-AIM Framework.” Irish Educational Studies 38 (2): 219–243. https://doi.org/10.1080/03323315.2019.1567368.
- Pawson, R., and N. Tilley. 1997. “An Introduction to Scientific Realist Evaluation”.
- Quirkos Software. 2021. Quirkos. Edinburgh.
- Research Work Group for Ireland’s Report Card on Physical Activity in Children and Adolescents. 2022. “The 2022 Ireland North and South Report Card on Physical Activity for Children and Adolescents: Summary.” Accessed May 9, 2023. https://activehealthykidsireland.org.
- Riddoch, C. J., C. Mattocks, K. Deere, J. Saunders, J. Kirkby, K. Tilling, and A. R. Ness. 2007. “Objective Measurement of Levels and Patterns of Physical Activity.” Archives of Disease in Childhood 92 (11): 963–969. https://doi.org/10.1136/adc.2006.112136.
- Roriz De Oliveira, M. S., A. Seabra, D. Freitas, J. C. Eisenmann, and J. Maia. 2014. “Physical Fitness Percentile Charts for Children Aged 6–10 from Portugal.” The Journal of Sports Medicine and Physical Fitness 54 (6): 780–792.
- Rush, E., P. Reed, S. McLennan, T. Coppinger, D. Simmons, and D. Graham. 2012. “A School-Based Obesity Control Programme: Project Energize. Two-Year Outcomes.” British Journal of Nutrition 107 (4): 581–587. https://doi.org/10.1017/S0007114511003151.
- Ryde, G. C., J. N. Booth, and N. E. Brooks. 2018. “The Daily Mile: What Factors are Associated with its Implementation Success?” PLoS One 13: e0204988. https://doi.org/10.1371/journal.pone.0204988.
- Schneider, M., M. J. Hall, A. E. Hernandez, K. Hindes, G. Montez, T. Pham, L. Rosen, et al. 2009. “Rationale, Design and Methods for Process Evaluation in the HEALTHY Study.” International Journal of Obesity 33: S60–S67. https://doi.org/10.1038/ijo.2009.118.
- Sebire, S. J., K. Banfield, R. Jago, Mark J. Edwards, Rona Campbell, Ruth Kipping, Peter S. Blair, et al. 2019. “A Process Evaluation of the PLAN-A Intervention (Peer-Led Physical Activity Intervention for Adolescent Girls).” BMC Public Health 19: 1203. https://doi.org/10.1186/s12889-019-7545-z.
- Shenton, A. K. 2004. “Strategies for Ensuring Trustworthiness in Qualitative Research Projects.” Education for Information 22: 63–75. https://doi.org/10.3233/EFI-2004-22201.
- Telford, R. M., R. D. Telford, L. S. Olive, T. Cochrane, and R. Davey. 2016. “Why are Girls Less Physically Active than Boys? Findings from the Look Longitudinal Study.” PLoS ONE 11 (3): e0150041. https://doi.org/10.1371/journal.pone.0150041.
- Thomas, J. R., J. K. Nelson, and S. J. Silverman. 2015. “Research methods in physical activity.” 7th Edition, Human Kinetics, USA. ISBN: 978-1-4504-7044-5.
- Tompsett, C., R. Sanders, C. Taylor, and S. Cobley. 2017. “Pedagogical Approaches to and Effects of Fundamental Movement Skill Interventions on Health Outcomes: A Systematic Review.” Sports Medicine 47 (9): 1795–1819. https://doi.org/10.1007/s40279-017-0697-z.
- Van Sluijs, E. M. F., A. M. McMinn, and S. J. Griffin. 2008. “Effectiveness of Interventions to Promote Physical Activity in Children and Adolescents: Systematic Review of Controlled Trials.” British Journal of Sports Medicine 42 (8): 653–657.
- Vasques, C., P. Magalhães, A. Cortinhas, P. Mota, J. Leitão, and V. P. Lopes. 2014. “Effects of Intervention Programs on Child and Adolescent BMI: A Meta-Analysis Study.” Journal of Physical Activity and Health 11 (2): 426–444. https://doi.org/10.1123/jpah.2012-0035.
- Ward, D. S., R. P. Saunders, and R. R. Pate. 2007. Physical Activity Interventions in Children and Adolescents. Champaign, IL: Human Kinetics.
- Westcott, H. L., and K. S. Littleton. 2005. “Exploring Meaning in Interviews with Children.” In Researching Children’s Experience: Approaches and Methods, edited by S. Greene and D. Hogan, 141–157. London: SAGE.
- Williams, P. T. 2013. “Dose-response Relationship of Physical Activity to Premature and Total All-cause and Cardiovascular Disease Mortality in Walkers.” PLoS One 8: e78777.