
ABSTRACT
This study aimed to understand the factors influencing people’s choice to follow a diet considered healthy, and if and how these factors may contribute progress toward a higher (unhealthy) degree of preoccupation with healthy eating: orthorexia nervosa. This was achieved through mixed methods (interviews, n = 12; questionnaire, n = 82). The target group was young females in the Netherlands. Several biological, psychological, and social factors contribute to people’s healthy eating. Having concerns about chronic conditions were found to be significantly associated with a higher degree of preoccupation with healthy eating, resulting implicated in the possible onset of orthorexia nervosa.
Introduction
Health authorities around the world are stressing the importance of healthy eating as a pillar for fighting numerous non-communicable diseases (NCDs), such as heart disease, diabetes, stroke, cancer, dental caries, and asthma (Shepherd et al. Citation2006). As concerns about the negative health effects of unhealthy eating and being overweight or obese have increased, so to have policy efforts to promote healthy diets (Barnhill et al. Citation2014). In Europe, many member states have developed policies to promote healthy eating (Capacci et al. Citation2012), and these policies vary from those more paternalistic to those less intrusive (Mazzocchi et al. Citation2015). Recently, evidence has emerged on the impact that various diets have on the environment, with the EAT-Lancet Commission providing guidelines for what can be considered a healthy diet for the health and the environment (EAT-Lancet Commission Citation2019). Despite these efforts, however, healthy eating is still interpreted differently by lay people, food experts, and food authorities (Bergman et al. Citation2019). Moreover, healthy eating policies have adopted a rhetoric of empowerment, which puts a lot of emphasis on individual responsibility for health (Bergman et al. Citation2019; Haman et al. Citation2015). This individual responsibility is often interpreted as a moral duty, implying that those who do not engage in healthy dietary practices are considered ‘immoral’ (Madden and Chamberlain Citation2010).
As a consequence of the societal pressure to be healthy, in a number of Western countries, there has been an identifiable trend, wherein people bombarded with discourses on ‘healthy eating’ have started changing their eating habits in an attempt to eat ‘healthier’ (Arganini et al. Citation2012). In a representative sample from a Dutch population, it emerged that 60% of more than a thousand participants classified themselves as ‘dieters’ (de Ridder et al. Citation2017). Another study conducted in the US revealed that 45% of American adolescent girls consider themselves as ‘dieter’ and that, in general, 13–44% of men and 25–65% of women diet (de Ridder et al. Citation2017). Although the awareness of many people on their diet is certainly a step forward toward a conscious nutrition, the sense of responsibility perceived by some individuals may lead them to develop an obsession with healthy eating, characterized by excessive control over food intake, constrained behaviors, and self-surveillance (Haman et al. Citation2015). The disordered eating pattern that may emerge from the extremism of these attitudes is called orthorexia nervosa (ON).
Steven Bratman firstly mentioned orthorexia nervosa in 1997 to refer to a fixation on eating proper food to achieve improved health (Bratman Citation1997). In contrast to other eating disorders, such as anorexia nervosa, bulimia nervosa, and binge eating disorder, ON focuses on quality rather than on the quantity of foods (Andreas et al. Citation2018). Its driving force is not to achieve a thin body, but to eat healthy, natural, and unprocessed foods (Brytek-Matera Citation2012), with the consequent self-imposition of a highly specific dietary regimen (Chaki, Pal, and Bandyopadhyay Citation2013) that implies obsessive thoughts, compulsive behaviors, self-punishments, and escalating restrictions (Bratman Citation2017; Cena et al. Citation2019). Orthorexia nervosa has not been recognized as a disorder by the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The main reason for this is the lack of validated diagnostic criteria (Brytek-Matera Citation2012; Valente, Syurina, and Donini Citation2019).
Understanding the relationship that exists between healthy eating and ON is key to be able to demarcate between a desirable behavior and a mental health condition. This relationship is described by Bratman in the form of a two-step process characterizing ON, where the first step is constituted by the laudatory decision to follow a healthy diet, and the second by an intensification of such pursuit into an unhealthy obsession (Bratman Citation2017). As stated by Bratman to discourage pointing to every healthy diet as ON: “It is not the theory itself: it is the response to the theory that constitutes orthorexia” (Bratman Citation2017). A recent attempt to promote a similar construct of ON has been done by Barrada and Roncero, who conceptualized orthorexia in its broader sense, including the positive dimension of healthy eating, thus distinguishing between “healthy orthorexia” and “orthorexia nervosa” (Barrada and Roncero Citation2018; Depa, Barrada, and Roncero Citation2019).
Although this study does not consider the net division between “healthy orthorexia” and “orthorexia nervosa,” it still aims to delve into the relationship that exists between healthy eating and ON, by exploring what contributes to the transition from healthy eating to ON. This transition is not direct, but it is a gradual process resulting from the influence of several factors, as well as their interactions. Biological, psychological, and social factors are usually involved in the perpetration of a strict diet over time (Frank et al. Citation2016). Our hypothesis is that these same factors may be also responsible for the transition from healthy eating into a self-sustaining mechanism that becomes more and more extreme, up to the obsession. In line with our hypothesis, it is important to understand the factors that determine people’s healthy eating, in order to understand if and how these factors may subsequently lead to crossing the boundaries between healthy eating and obsession. We believe that more scholarly attention should be paid to the processes through which people decide to eat ‘healthy’ and how they decide what ‘healthy’ is.
Therefore, the objective of this research consists of two steps: first, to understand the factors that influence people choosing to follow a diet they perceive as being healthy; second, to understand if and how these factors may contribute to developing an obsession with healthy eating. We accomplished this by conducting a mixed methods study, whose qualitative component was aimed at investigating the factors leading to eating healthfully, and the quantitative one was aimed at examining if and how these factors may be involved in the progression from healthy eating to obsession in young women (18–35) in the Netherlands.
Materials and methods
This study was conducted using a mixed-methods approach, with a sequential exploratory design. The intention of this study was to focus on a potentially at-risk group to increase the chance of finding people eating healthy, whose healthy eating could have evolved into an obsession. Therefore, the target group was young females (age 18–35), as previous research indicated a higher prevalence of healthy eating in this group (Arganini et al. Citation2012). Interviews were conducted in English because of the researcher who conducted them being unfamiliar with the Dutch language. Therefore, the research was carried out around the cities of Amsterdam and Utrecht due to the higher prevalence of both Dutch natives and expats. Qualitative data collection was done through semi-structured interviews (n = 12), conducted from March 20, 2018 to April 12, 2018. Quantitative data collection was done through an online questionnaire (n = 82), delivered from May 9, 2018 to May 28, 2018. The two steps of the objective were divided between the two data collection phases.
Interviews
Sample
In accordance with what was said in the previous paragraph, inclusion criteria for participating in the interviews were: (1) being female, (2) speak English, (3) being in the age range that goes from 18 to 35 years, and (4) self-identify as a “healthy eater” (e.g. “In particular, we are interested in women (aged 18–35) living in/around Amsterdam and Utrecht, who self-identify with following a healthy diet”). Participants were recruited through an announcement posted on 13 Facebook pages. The choice of pages was made in line with the inclusion criteria, thus pages of students in Amsterdam and Utrecht and healthy eating pages were selected.
Interview guide
Semi-structured interviews were chosen as the qualitative method of inquiry. Prior to data collection, the interview was piloted and adapted as necessary. The interview guide was based upon the dynamic bio-psycho-social model of health developed by Lehman, David, and Gruber in 2017, and it was constructed in a way to investigate (1) participants’ perceptions of healthy eating, (2) how the eating pattern has changed during life, and (3) what have been bio-psycho-social factors leading them to eating healthfully. Participatory and visualization techniques were important components of the interviews. For example, participants were asked to write on a board what were the first words/sentences they had in mind when thinking about healthy eating. Moreover, they were asked to display on a timeline and discuss shortly what have been significant eating-related events in their life. By graphically displaying these events, it was possible to visualize what were the drivers for their healthy eating choices and to subsequently classify them as bio-psycho-social.
Data analysis
Interviews were manually transcribed and thematically coded using Atlas.ti version 8.2.4. The codes reflected the information needed to answer the research question. The determinants for eating healthy identified by the interviews were classified according to the bio-psycho-social model of health (Lehman, David, and Gruber Citation2017). Results of the interviews were subsequently used to construct the questionnaire.
Questionnaire
Sample
Inclusion criteria for the questionnaire were the same as for the interviews. Therefore, participants were recruited through a second announcement posted on the same Facebook pages of the interviews. The questionnaire was also personally sent by e-mail to all the people previously interviewed during the qualitative phase. However, due to the anonymous nature of the questionnaire, it was not possible to assess if all interviewees completed the questionnaire and were therefore included in the analysis.
Questionnaire design
An online questionnaire was designed to assess if there was an association between the factors previously found to be implicated in the choice of healthy eating and an increased degree of preoccupation with eating healthy, which could potentially result in ON. Before collecting data, the questionnaire was piloted on a student sample.
The questionnaire was set up using the software Qualtrics XM and was divided into two sections. The first section investigated participants’ level of preoccupation with healthy eating by using the ORTO-15 test, a diagnostic tool for ON constructed by Donini et al. (Citation2005) (see Supplemental material). To overcome the limitations of the tool, which have been extensively reported in the literature (Valente, Syurina, and Donini Citation2019), no threshold was considered to diagnose the disorder, but the questionnaire was used as a mean to obtain a range of levels of preoccupation with healthy eating, with lower scores representing higher preoccupation with healthy eating. In the second section, respondents were asked to grade from 0 to 5 how much they identify with a list of statements representing the bio-psycho-social factors leading to eating healthfully found during the interviews.
Data analysis
Analysis was performed using SPSS version 23. Descriptive statistic was performed for the sample’s demographics. One extreme ORTO-15 score (ORTO-15 = 22) was identified and replaced by a score 3 standard deviations from the mean (ORTO-15 = 24), being the lower value that is not an outlier (Field Citation2018). Assumptions of linearity, normality, homoscedasticity, and independence were checked. The scale reporting ORTO-15 scores of questionnaire respondents was considered representative of the levels of preoccupation with healthy eating, with lower scores indicative of higher preoccupation with healthy eating. Pearson’s correlation coefficient was used to assess the strength of the relationship between each factor leading to healthy eating and the level of preoccupation with healthy eating. Multiple linear regression was performed to obtain a model predicting the level of preoccupation with healthy eating from the influence exerted by the drivers to eat healthy. Forward stepwise selection based on the Akaike information criterion (AIC) was performed to select predictors to include in the model (Field Citation2018). Power calculation was performed retrospectively, in order to assess the strength of the multiple regression model according to the obtained sample size. By considering the predictors that were included in the model (n = 3), the power obtained was 99%.
Replication of the analysis with the ORTO-6
During data analysis, authors came across the meta-analytical simulation study conducted by Rogoza (Citation2019). This study reported interesting results regarding the elimination of items from the ORTO-15, which allows obtaining a more valid and reliable tool to assess ON: the ORTO-6. Although the analysis had already been carried out on data collected with the ORTO-15, and the development of the ORTO-6 is ongoing and still unpublished, authors decided to replicate the analysis after eliminating the items from the ORTO-15 that are suggested by the study by Rogoza (Citation2019). This was done to assess whether there are differences with the results obtained with the ORTO-15, to support the revision of the ORTO-15 test that is currently underway, and to make the study more up-to-date. The results of the second analysis will be reported separately and differences in results will be discussed in the discussion section.
Ethical considerations
Participation in this research was voluntary. Participants were young women who self-declared to eat healthy, thus they were not patients or vulnerable subjects. According to the current legislation (Wet Medische Onderzoek) in the Netherlands, no medical ethical approval was needed to conduct the research on this sample.
Research participants were not subjected to harm in any way and they have been guaranteed the right to withdraw from the study at any time. Written informed consent was obtained from interviews and survey respondents, where privacy, confidentiality, and anonymity were ensured. Finally, communication with regards to the research aim and methodology was performed with transparency and honesty.
Results
Qualitative and quantitative results will be reported integrated with each other. Interviews were aimed at understanding people’s drivers to eat what they perceived as being a healthy diet, while the questionnaire was used to assess the relationship between these drivers and the level of preoccupation with healthy eating. Five sections will follow: (1) demographics, (2) perception of healthy eating, (3) factors leading to eating healthfully, (4) preoccupation with healthy eating, (5) factors involved in major preoccupation with healthy eating.
Demographics
Qualitative sample
Twelve people applied for the interview, with a mean age of 23 years (range 19–31). The most prevalent nationalities were Dutch and British, which together accounted for half of the sample. Other nationalities were found and are reported in . The majority of the interviewees were students, with just one respondent being employed. Half of the respondents followed a vegan diet, resulting in the most common diet among the sample. However, other diets were also mentioned, which are reported in .
Table 1. Demographics of the qualitative sample
Quantitative sample
In total, 97 people started completing the online questionnaire. Respondents who left important sections of the survey incomplete were deleted, resulting in a response rate of 84.5%. Objective response rate was impossible to calculate because the announcement was published online and it is therefore impossible to know how many people came across it. Thus, 82 people completed the online questionnaire entirely, with a mean age of 24 years (SD = 3.89). The most prevalent nationalities were Dutch (27%), Italian (12%), and British (8.5%). Other nationalities were found, for example, German (6%), American (5%), Austrian (4%), and Vietnamese (4%). With regards to the employment status, 71% of respondents were students, 24% were employed, 4% were unemployed, and 1% were unable to work. The majority of respondents followed a flexitarian diet (i.e., diet with rare consumption of meat). Other diets were found, such as an omnivore diet, vegan diet, and pescetarian diet (i.e., a vegetarian diet that includes fish) ().
Figure 1. Bar chart reporting the types of diets followed by questionnaire respondents
Perception of healthy eating
Interviewees were asked to write on a board what were the first words/sentences that came to their mind when thinking about healthy eating. Although the answers varied, recurrent topics have been identified and are reported below (see for word cloud).
Figure 2. Word cloud depicting the most frequent words associated with healthy eating that participants wrote on the board during the interviews
Eight people wrote ‘balance’ and ‘moderation’ and considered these key points for a healthy diet. Foods associated with healthy eating were ‘vegetables’ (n = 8), ‘fruit’ (n = 6) and ‘whole food’ (n = 3). This can be linked to the fact that five participants followed a plant-based diet and considered veganism strongly related to healthy eating: ‘If you want to be the healthiest version of yourself […] it would be through a plant-based diet’ (Interviewee 5). Other recurring concepts were ‘natural food’ and ‘unprocessed food.’ When asked about the meaning of these words, a sense of repugnance toward the industrial processing of food appeared: ‘I want to rebel against the production process of food, it’s just completely transformed and then it enters in our bodies’ (Interviewee 2).
Factors leading to eating healthfully
During the interviews, individuals were asked to visualize on a timeline how their eating habits changed over time. This worked as an input for discussion around the main determinants for them to start eating healthy. Once the determinants were obtained from all interviewees, they were divided into biological, psychological, and social categories, following the bio-psycho-social model of health (Lehman, David, and Gruber Citation2017) ().
Table 2. Bio-psycho-social drivers to eat healthy found during interviews
Biological drivers include biological reasons to choose healthy eating; thus, they go beyond psychological issues or social influences. Suffering from particular diseases (e.g. gastritis) was shown to coincide with a change in the diet, leading to eat in a healthier way. Having food intolerances led people to be more cautious about the food they ate, thus leading them to follow a healthy diet as well: ‘I got a gluten intolerance […] and I started to be aware that, with the foods you eat, you can serve your body or not’ (Interviewee 10). Other biological drivers are the natural preference for the taste of healthy food and the decision to follow an appropriate diet in order to prepare the body for an imminent pregnancy.
Psychological drivers were relatively easier to identify by participants. The desire to take care of the body after a challenging period (e.g. break up with a partner) was identified as a driver for healthy eating. Other psychological drivers were caring about animals and the environment, the desire to have a fit and thin body, and the tendency of expressing one’s personal identity through food choices: ‘I have a very low self-confidence, but again food is so important, especially healthy eating, because it provides you with the ability to see yourself, assess your needs and assess what you want, what you don’t want […] because sometimes I get really paranoid about what I think about myself, but having this outlet of eating which I can say what I really like, what I don’t like, it’s also important for myself’ (Interviewee 2). Additionally, being a perfectionist, with the desire to keep everything under-control, and having concerns about future chronic diseases that may derive from unhealthy eating were identified.
Many social drivers for healthy eating were also reported. A distinction was made between ‘media,’ ‘social relationships,’ and ‘environment.’ Starting from media, many people were influenced by documentaries about healthy eating (e.g. Food Inc., Cowspiracy, Forks over Knife; Fat, sick, and nearly dead). Other influences came from healthy eating blogs/communities, which share advice on nutrition and lifestyle. Instagram was the most cited social network to inspire people to eat healthy, with accounts dealing with food and lifestyle being the most influential ones. Lastly, media influenced people also through the beauty ideals they promote: ‘It’s all about beauty canons and most people start to eat healthy, to go to the gym or whatever because of society. It’s because there is so much pressure’ (Interviewee 1). Moving to social relationships, having health-conscious parents, friends, partners, or classmates was a driver for eating healthy. Furthermore, the desire to have a good physical appearance during adulthood, or even seniority, was a factor that led people to eat healthy. Finally, considering the environment, some international people living in the Netherlands identified the Dutch culture as more health conscious than their own culture, thus leading them to change their diet and to start eating healthier. Following, an environmental influence was also exerted by travels. The last environmental driver was the influence exerted by the study/work environment: ‘There are a lot of people in my environment that at school also eat in the same way so it’s just normal to have as snack your pepper, carrot or whatever’ (Participant 10).
The questionnaire required respondents to rank on a scale from 0 to 5 how much they perceived these factors have influenced their choice to eat healthy. By comparing the mean scores obtained for each determinant, the most influential ones resulted to be ‘desire to take care of the body’ (M = 3.79, SD = 1.90), ‘desire to have a fit and thin body’ (M = 3.57, SD = 1.30), ‘preference for the taste of healthy food’ (M = 3.44, SD = 1.25), ‘concerns about future chronic diseases’ (M = 3.27, SD = 1.46), and ‘desire to maintain a good appearance in adulthood/seniority’ (M = 3.06, SD = 1,61) ().
Figure 3. Plot reporting means and 95% confidence intervals of the scores obtained for each determinant by questionnaire respondents
Preoccupation with healthy eating
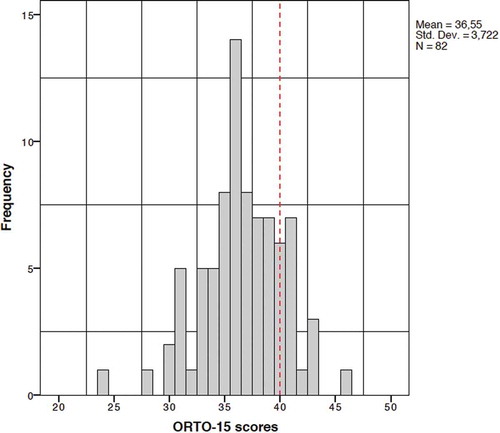
The level of preoccupation with healthy eating was assessed in the questionnaire and it was measured using the ORTO-15 test. Despite a score of 40 was suggested as the threshold below which to assess ON (Donini et al. Citation2005), no threshold was considered in this study, but the scale reporting ORTO-15 scores was considered a scale representing levels of preoccupation with healthy eating, with lower ORTO-15 scores indicative of higher (unhealthy) preoccupation with healthy eating. The average ORTO-15 score was 36.55 (SD = 3.72), with a median of 36.00 and an interquartile range of 34.75–39.00 (see ).
Figure 4. Frequency distribution of ORTO-15 scores of questionnaire respondents. The dashed-red line indicates the threshold below which the ORTO-15 would have assessed orthorexia nervosa
Replication of the analysis with the ORTO-6
The replication of the analysis performed with the ORTO-6 test resulted in an average score of 16.10 (SD = 3.34), with an interquartile range of 14.00–19.00. No threshold was considered, since the author specifically suggests the use of the revised tool for a dimensional, rather than a categorical, assessment of ON (Rogoza Citation2019).
Factors involved in major preoccupation with healthy eating
After checking assumptions, Pearson’s correlation coefficient was used to assess the strength of the relationship between each driver and the level of preoccupation with healthy eating. Medium and small-to-medium positive correlations were found for ‘food intolerances’ and preoccupation with healthy eating (r =.31; p = .004; CI = 0.092, 0.483), and ‘pressure from beauty ideals’ and preoccupation with healthy eating (r = .24; p = .030; CI = 0.052, 0.417) (Field Citation2018). This means that the more a person had been influenced by these drivers, the lower the preoccupation with healthy eating was. A small-to-medium negative correlation was found for ‘concerns about future chronic diseases’ and level of preoccupation with healthy eating (r = −.24; p = .029; CI = −0.424, −0.035) (Field Citation2018), meaning that the more a person had been influenced by this driver, the higher the preoccupation with healthy eating was.
After checking assumptions, forward stepwise selection based on AIC was performed to select predictors to include in the multiple linear regression model. ‘Food intolerances,’ ‘pressure from beauty ideals,’ and ‘concerns about future chronic diseases’ were shown to be the most significant predictors of the level of preoccupation with healthy eating. A significant regression equation was found (F(3, 78) = 7.70, p < .000), with an R2 of .23. Respondents’ predicted ORTO-15 score is equal to 37.63 + 0.65 (food intolerances) – 0.79 (concerns about future chronic diseases) + 0.61 (pressure from beauty ideals), where ‘food intolerances,’ ‘concerns about future chronic diseases’ and ‘pressure from beauty ideals’ are measured on a scale from 0 to 5 according to their influence on healthy eating. ‘Food intolerances,’ ‘pressure from beauty ideals’ and ‘concerns about future chronic diseases’ were significant predictors of the level of preoccupation with healthy eating; i.e. ORTO-15 score (p = .003, p = .003, p = .02), with the formers predicting lower preoccupation with healthy eating, and the latter predicting higher preoccupation with healthy eating. A summary of the regression is reported in .
Table 3. Regression analysis summary (ORTO-15)
Replication of the analysis with the ORTO-6
The same analysis was performed by considering ORTO-6 scores. Small-to-medium negative correlation was confirmed for ‘concerns about future chronic diseases’ and preoccupation with healthy eating (r = .23; p = .037; CI = −0.004, −0.099). This means that a more a person had been influenced by this driver, the higher the preoccupation with healthy eating was, confirming the analysis with the ORTO-15. Differently from the analysis with the ORTO-15, a small-to-medium negative correlation was found for ‘desire to have a fit and thin body’ and preoccupation with healthy eating (r = .25; p = .025; CI = −0.48, −0.034). This means that a more a person had been influenced by this driver, the higher the preoccupation with healthy eating was.
Forward stepwise selection based on AIC was performed to select predictors to include in the multiple linear regression model. ‘Desire to have a fit and thin body,’ ‘food intolerances,’ and ‘concerns about future chronic diseases’ were shown to be the most significant predictors of the level of preoccupation with healthy eating. A multiple linear regression was calculated to predict the ORTO-6 score based on the influence of the drivers ‘desire to have a fit and thin body,’ ‘food intolerances,’ and ‘concerns about future chronic diseases.’ A significant regression equation was found (F(3, 78) = 3.494, p = .019), with an R2 of .12. Respondents’ predicted ORTO-6 score is equal to 18.83–0.51 (desire to have a fit and thin body) + 0.36 (food intolerances) – 0.40 (concerns about future chronic diseases), where ‘desire to have a fit and thin body,’ ‘food intolerances’ and ‘concerns about future chronic diseases’ are measured on a scale from 0 to 5 according to their influence on healthy eating. Despite the regression model being significant, ‘desire to have a fit and thin body,’ ‘food intolerances’ and ‘concerns about future chronic diseases’ were non-significant predictors of the level of preoccupation with healthy eating (p = .09, p = .08, p = .14). Having a significant model (p = .019) with non-significant predictors (p = .09, p = .08, p = .14) can be due to multicollinearity, which however was assessed and excluded. It may still be possible to get non-significant predictors and an overall significant model if two or more individual predictors are close to significant, which is likely to be the case in this analysis. A summary of the regression performed using the ORTO-6 is reported in .
Table 4. Regression analysis summary (ORTO-6)
Discussion
The purpose of this study was to understand the factors responsible for people’s choice to follow a diet perceived as healthy, and subsequently to understand if and how these factors may contribute to developing an obsession with healthy eating. Through a mixed-methods design, it was found that several biological, psychological, and social factors contribute to people’s healthy choices, the most important ones being the desire to take care of the body, the desire to have a fit body, the preference for the taste of healthy food, concerns about future chronic conditions, and the desire to have a good appearance in adulthood. Only having concerns about future chronic conditions were found to be significantly associated to a higher (unhealthy) degree of preoccupation with healthy eating, resulting in the most implicated in the possible onset of ON. Having food intolerances and being influenced by beauty ideals were shown to predict a lower degree of preoccupation with healthy eating. These findings are important since they add valuable insights to the existing literature about ON, especially contributing to the understanding of ON etiology, as recommended by previous scholars (Cena et al. Citation2019; Moroze et al. Citation2015; Scarff Citation2017).
Among the most important factors leading to eating healthfully, only having concerns about future chronic conditions was shown to be also implicated in the possible onset of ON (both by using the ORTO-15 and the ORTO-6). This finding is important for two reasons: first, because it implies that other factors may be involved in the onset of ON, not necessarily involved in the choice to eat healthy; second, because it strengthens the consolidated idea of ON being driven by the strive for health (Musolino et al. Citation2015). Having concerns about future diseases predicting a higher (unhealthy) preoccupation with healthy eating demonstrates that in today’s society people perceive to be responsible for their own health. This means that people who are already predisposed (i.e. with perfectionistic traits, obsessive tendencies, etc.) may internalize messages coming from healthy eating promotion campaigns, to the point of developing an obsession with healthy eating, confirming the findings of Greville-Harris, Smithson, and Karl (Citation2019). Furthermore, while healthy eating is strongly promoted, the food environment people are into often encourages the consumption of unhealthy food. Thus, the strong self-discipline needed to eat healthy in such an environment, and the ostracism of overweight and obesity (with their erroneous implicit association to unhealthiness), may contribute to developing ON.
Having food intolerances were shown to predict lower preoccupation with healthy eating. Given that ON is characterized by food exclusion (Bratman Citation1997), this could mean that excluding foods for ‘medical reason,’ would imply a more serene approach to diet, rather than excluding foods because of personal beliefs about foods (un)healthiness. Also, being influenced by beauty ideals was shown to predict lower preoccupation with healthy eating. This finding underlines the idea of ON not being driven by appearance-related reasons, and this is in accordance with what is reported by Moroze et al. (Citation2015), Catalina Zamora et al. (Citation2005) and Park et al. (Citation2011). Conversely, the study from Depa, Barrada, and Roncero (Citation2019) in support of the bidimensional nature of orthorexia (i.e. “healthy orthorexia” and “orthorexia nervosa”) reports that the main motive guiding food choices in “orthorexia nervosa” is weight control. Similarly, the replication of the present study by using the ORTO-6 reported a correlation between the desire to have a fit and thin body and ON. This confirms that further research may be needed to explore the relationship between ON and body weight and to investigate the extent to which body weight is considered a health parameter in today’s culture.
The use of mixed methods allowed splitting the objective in two parts. This ensured a more in-depth analysis during the interviews, which made it possible to construct a questionnaire more tailored to the research question. The choice of the ORTO-15 test to assess the degree of preoccupation with healthy eating was done because it has been the most used diagnostic tool for ON (Valente, Syurina, and Donini Citation2019). The choice not to consider the ORTO-15 threshold to diagnose ON was made to avoid bias, given that the test has been criticized for many reasons and by many authors (Valente, Syurina, and Donini Citation2019). In fact, if in the present study the ORTO-15 threshold had been considered, the majority of the sample would have resulted orthorexic, since the mean ORTO-15 score obtained in the present study (36.55) was below the recommended threshold (40.00). A further reflection on the methodology deserves to be made on the value of R2 obtained performing multiple linear regression. The coefficient of determination R2 measures how much of the variance of the dependent variable is explained by the predictors, with R2 = 1 indicating that all the variance is explained by the predictors, and R2 = 0 indicating the opposite (Field Citation2018). The multiple linear regression model performed in this study reported a R2 of .23, meaning that 77% of the variance is left unexplained. However, especially in social or behavioral sciences, models are not expected to include all possible relevant predictors to explain an outcome variable; therefore, R2 is usually expected to be low (Moksony Citation1990; Itaoka Citation2012, slide, 15). Additionally, it is important to note that correlations found in the present study were interpreted in line with the ranges proposed by Field (Citation2018). According to other sources, these correlations can be considered weak.
Replication of the analysis with the ORTO-6
Authors replicated the analysis by eliminating nine items from the ORTO-15 test, thus obtaining a 6-item tool overcoming most of the limitations of the ORTO-15 tool, as suggested by Rogoza (Citation2019). The correlation between having concerns about future chronic conditions and ON was found in the second analysis too, confirming the role of these concerns in contributing to the transition from healthy eating to ON. Having food intolerances were confirmed to be a protective factor for ON, predicting a lower level of preoccupation with healthy eating. Interestingly, however, the second analysis identified a desire to have a fit and thin body to be a trigger for ON. This seems to be in contrast with our first analysis, which found that being influenced by beauty ideals predicts lower orthorexic tendencies, but is in agreement with findings from Depa, Barrada, and Roncero (Citation2019), and Barnes and Caltabiano (Citation2017). A possible explanation may lie in the fact of the ORTO-6 including only six items, among which one concerns appearance (e.g. “Do you think that consuming healthy food may improve your appearance?”). This may have contributed to associating the assessment of ON to appearance-related concerns. However, this is a further indication that the relationship between ON and body image needs to be further investigated, as well as the extent to which weight control may be considered a health-related, as well as an appearance-related, behavior.
Strengths and limitations
Some limitations of this study are listed as follows. First, the size of both qualitative and quantitative samples was relatively small. Second, this study did not include people unable to speak and/or understand the English language. Third, the recruitment of participants through means of Facebook pages prevented from obtaining a fully representative sample for the Netherlands. With regard to this point, however, it’s worth saying that it was beyond the scope of this study to obtain a representative sample of healthy eaters. Instead, this study aimed to focus on a high-risk population of people who self-identify as healthy eaters, in order to explore possible risk factors for ON. Therefore, we are aware of the lack of generalizability of these findings, but we acknowledge the role of this study in generating a hypothesis, which could be investigated in the future on a population-base. Fourth, both qualitative and quantitative samples were characterized by a high prevalence of vegans and vegetarians. This impedes the generalizability of results to the broader population of healthy eaters, but also indicates that vegans and vegetarians could be more prone to self-identify as healthy eaters and more willing to share their experiences. The last limitation is that this study used the ORTO-15 test, which has been accused in the literature to: (i) overestimate ON prevalence (Valente, Syurina, and Donini Citation2019), (ii) only capture healthful eating without accompanying pathology (Dunn and Bratman Citation2016; Valente, Syurina, and Donini Citation2019), (iii) have problematic internal consistency, (iv) not take into account the obsessive-compulsive symptomatology and the distressful nature of ON (Dunn and Bratman Citation2016; Koven and Abry Citation2015), and (v) be supported by inadequate evidence that the authors followed a traditional approach for test construction (Dunn and Bratman Citation2016). However, as confirmed by Rogoza (Citation2019), instead that for categorical diagnosis, the ORTO-15 may rather be good for a dimensional assessment of ON. In fact, in the present study, the ORTO-15 was not used as a diagnostic tool, but as a tool to provide a range of levels of preoccupation with healthy eating. This alternative use of the tool allowed considering ON not as a ‘black-and-white’ disorder, but as a progression, and this can be considered a strength of this study. Moreover, a secondary analysis eliminating the items from the ORTO-15 that compromised its factorial validity had been performed and placed alongside the primary one. This additional analysis allowed comparing the results obtained by using the ORTO-15 to the ones obtained by using the ORTO-6, enhanced validation of results, and gave rise to interesting findings that can be investigated in light of the differences between the tools. Another strength has been the use of mixed methods, which allowed using the qualitative phase to inform the quantitative one, overcoming the limits that would have arisen using only one of the two methodologies.
In sum, this study provided preliminary data, which can be useful to guide a larger observational study examining ON drivers. It may be also a starting point for the development of preventive interventions for ON. It underlines that a possible driver for ON is having concerns about future chronic diseases, which however is also a driver for healthy eating. Therefore, it seems that taking these concerns to the extreme may lead to cross the boundary between healthy eating and obsession. This recalls the feeling of being personally responsible for one’s own health, which could derive from an excessive internalization of messages coming from healthy eating promotion campaigns. In a future study, it could be interesting to explore the influence of health policies emphasizing individual responsibility for health on the onset of ON.
Supplemental Material
Download MS Word (105.3 KB)Disclosure statement
Authors have no conflict of interests to declare.
Supplementary Data
Supplementary material for this article can be accessed here.
References
- Andreas, S., K. Schedler, H. Schulz, and D. O. Nutzinger. 2018. Evaluation of a German version of a brief diagnosis questionnaire of symptoms of orthorexia nervosa in patients with mental disorders (ortho-10). Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity 23 (1):75–85. doi:10.1007/s40519-017-0473-y.
- Arganini, C., A. Saba, R. Comitato, F. Virgili, and A. Turrini. 2012. Gender differences in food choice and dietary intake in modern western societies. In J. Maddock, (Ed.), Public health – social behavioral health, 4, 83–102. Rijeka, Croatia: InTech.
- Barnes, M. A., and M. L. Caltabiano. 2017. The interrelationship between orthorexia nervosa, perfectionism, body image and attachment style. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity 22 (1):177–84. doi:10.1007/s40519-016-0280-x.
- Barnhill, A., K. F. King, N. Kass, and R. Faden. 2014. The value of unhealthy eating and the ethics of healthy eating policies. Kennedy Institute of Ethics Journal 24 (3):187–217. doi:10.1353/ken.2014.0021.
- Barrada, J. R., and M. Roncero. 2018. Bidimensional structure of the orthorexia: Development and initial validation of a new instrument. Anales De Psicología/Annals of Psychology 34 (2):283–91. doi:10.6018/analesps.34.2.299671.
- Bergman, K., K. Eli, C. P. Osowski, E. Lovestam, and P. Nowicka. 2019. Public expressions of trust and distrust in governmental dietary advice in Sweden. Qualitative Health Research 29 (8):1161–73. doi:10.1177/1049732318825153.
- Bratman, S. (1997). Original essay on orthorexia. Retrieved from https://www.orthorexia.com/original-orthorexia-essay/
- Bratman, S. 2017. Orthorexia vs. theories of healthy eating. Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity 22 (3):381–85. doi:10.1007/s40519-017-0417-6.
- Brytek-Matera, A. 2012. Orthorexia nervosa – An eating disorder, obsessive-compulsive disorder or disturbed eating habit? Archives of Psychiatry and Psychotherapy 1 (1):55–60.
- Capacci, S., M. Mazzocchi, B. Shankar, J. B. Macias, W. Verbeke, F. J. Perez-Cueto, A. Koziol-Kozakowska, B. Piorecka, B. Niedzwiedzka, D. D’Addesa, et al. 2012. Policies to promote healthy eating in Europe: A structured review of policies and their effectiveness. Nutrition Reviews 70 (3):188–200. doi:10.1111/j.1753-4887.2011.00442.x.
- Catalina Zamora, M. L., B. Bote Bonaechea, F. Garcia Sanchez, and B. Rios Rial. 2005. Orthorexia nervosa. A new eating behavior disorder? Actas Espanolas De Psiquiatria 33 (1):66–68.
- Cena, H., F. Barthels, M. Cuzzolaro, S. Bratman, A. Brytek-Matera, T. Dunn, M. Varga, B. Missbach, L. M. Donini. 2019. Definition and diagnostic criteria for orthorexia nervosa: A narrative review of the literature. Eat Weight Disord 24:209–46. doi:10.1007/s40519-018-0606-y.
- Chaki, B., S. Pal, and A. Bandyopadhyay. 2013. Exploring scientific legitimacy of orthorexia nervosa: A newly emerging eating disorder. Journal of Human Sport & Exercise 8 (4):1045–53. doi:10.41100/jhse.2013.84.14.
- Commission, E.-L. (2019). Food, planet, health: healthy diets from sustainable food systems. https://eatforum.org/content/uploads/2019/01/EAT-Lancet_Commission_Summary_Report.pdf
- de Ridder, D., F. Kroese, C. vers, M. Adriaanse, and M. Gillebaart. 2017. Healthy diet: Health impact, prevalence, correlates, and interventions. Psychology & Health 32 (8):907–41. doi:10.1080/08870446.2017.1316849.
- Depa, J., J. R. Barrada, and M. Roncero. 2019. Are the motives for food choices different in orthorexia nervosa and healthy orthorexia? Nutrients 11 (3):697. doi:10.3390/nu11030697.
- Donini, L. M., D. Marsili, M. P. Graziani, M. Imbriale, and C. Cannella. 2005. Orthorexia nervosa: Validation of a diagnosis questionnaire. Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity 10 (2):e28–32. doi:10.1007/BF03327537.
- Dunn, T. M., and S. Bratman. 2016. On orthorexia nervosa: A review of the literature and proposed diagnostic criteria. Eating Behaviors 21:11–17. doi:10.1016/j.eatbeh.2015.12.006.
- Field, A. 2018. Discovering statistics using IBM SPSS statistics. 5th ed. London: Sage Edge.
- Frank, G. K., M. E. Shott, C. Keffer, and M. A. Cornier. 2016. Extremes of eating are associated with reduced neural taste discrimination. International Journal of Eating Disorders 49 (6):603–12. doi:10.1002/eat.22538.
- Greville-Harris, M., J. Smithson, and A. Karl. 2019. What are people’s experiences of orthorexia nervosa? A qualitative study of online blogs. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity 1–10. https://link.springer.com/article/10.1007%2Fs40519-019-00809-2
- Haman, L., N. Barker-Ruchti, G. Patriksson, and E. C. Lindgren. 2015. Orthorexia nervosa: An integrative literature review of a lifestyle syndrome. International Journal of Qualitative Studies on Health and Well-Being 10 (1):26799. doi:10.3402/ghw.v10.26799.
- Itaoka, K. (2012). Regression and interpretation low R-squared! [PowerPointslides]. Retrieved from: https://ieaghg.org/docs/General_Docs/3rd_SRN/Kenshi_Itaoka_RegressionInterpretationSECURED.pdf
- Koven, N. S., and A. W. Abry. 2015. The clinical basis of orthorexia nervosa: Emerging perspectives. Neuropsychiatric Disease and Treatment 11:385. doi:10.2147/NDT.S61665.
- Lehman, B. J., D. M. David, and J. A. Gruber. 2017. Rethinking the biopsychosocial model of health: Understanding health as a dynamic system. Social and Personality Psychology Compass 11:e12328. doi:10.1111/spc3.12328.
- Madden, H., and K. Chamberlain. 2010. Nutritional health, subjectivity and resistance: Women’s accounts of dietary practices. Health (London) 14 (3):292–309. 1177/1363459309356073.
- Mazzocchi, M., S. Cagnone, T. Bech-Larsen, B. Niedzwiedzka, A. Saba, B. Shankar, W. Verbeke, and W. B. Trail. 2015. What is the public appetite for healthy eating policies? Evidence from a cross-European survey. Health Economics, Policy, and Law 10 (3):267–92. doi:10.1017/S1744133114000346.
- Moksony, F. 1990. Small is beautiful. The use and interpretation of R2 in social research. Szociologiai Szemle, Special Issue 130–38. https://www.researchgate.net/profile/Ferenc_Moksony/publication/242329609_Small_Is_Beautiful_The_Use_and_Interpretation_of_R2_in_Social_Research/links/00b4951cc7fbd64be5000000.pdf
- Moroze, R. M., T. M. Dunn, C. J. Holland, J. Yager, and P. Weintraub. 2015. Micro thinking about micronutrients: A case of transition from obsessions about healthy eating to near-fatal “orthorexia nervosa” and proposed diagnostic criteria. sychosomatics 56 (4):397–403. doi:10.1016/j.psym.2014.03.003.
- Musolino, C., M. Warin, T. Wade, and P. Gilchrist. 2015. ‘Healthy anorexia’: The complexity of care in disordered eating. Social Science & Medicine 139:18–25. doi:10.1016/j.socscimed.2015.06.030.
- Park, S. W., J. Y. Kim, G. J. Go, E. S. jeon, H. J. Pyo, and Y. J. Kwon. 2011. Orthorexia nervosa with hyponatremia, subcutaneous emphysema, pneumomediastimum, pneumothorax, and pancytopenia. Electrolyte & Blood Pressure 9 (1):32–37. doi:10.5049/EBP.2011.9.1.32.
- Rogoza, R. 2019. Investigating the structure of ORTO-15: A meta-analytical simulation study. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity 24 (2):363–65. doi:10.1007/s40519-018-0621-z.
- Scarff, J. R. 2017. Orthorexia nervosa: An obsession with healthy eating. Federal Practitioner 34 (6):36.
- Shepherd, J., A. Harden, R. Rees, G. Brunton, J. Garcia, S. Oliver, and A. Oakley. 2006. Young people and healthy eating: A systematic review of research on barriers and facilitators. Health Education Research 21 (2):239–57. doi:10.1093/her/cyh060.
- Valente, M., E. V. Syurina, and L. M. Donini. 2019. Shedding light upon various tools to assess orthorexia nervosa: A critical literature review with a systematic search. Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity. doi:10.1007/s40519-019-00735-3.
