
ABSTRACT
This paper studies the association between nutrition knowledge and consumer dietary behavior using large survey data from 996 respondents in Addis Ababa, Ethiopia. We find that health was the most important factor in individuals’ food choice. However, most consumers were found to have imperfect understanding of the link between food and health. Especially, the causes and consequences of obesity were poorly understood. A considerable proportion of respondents also endorsed harmful food taboos. We found that nutrition knowledge was positively associated with more diversified diets and healthy eating attitudes and practices. Individuals with higher levels of nutrition knowledge were also more likely to reject harmful food taboos.
Introduction
Malnutrition in its various forms is a global challenge with huge social and economic costs (Gillespie and van den Bold Citation2017). Poor diets are main contributors to multiple burdens of malnutrition (Monteiro et al. Citation2013). In poor countries, monotonous staple-based diets are strongly associated with inadequate intake of micronutrients (IFPRI Citation2016). Concurrently, rapid nutrition transitions in these countries are marked by adverse dietary changes toward increased consumption of processed foods and reduced intakes of dietary fiber and fruits and vegetables (Monteiro et al. Citation2013; Popkin Citation2014). As a result, developing countries are now struggling with burdens of rising diet-related non-communicable diseases (Popkin, Adair, and Ng Citation2012).
Approaches to ending malnutrition in poor countries have focused on improving food availability and affordability (Popkin Citation2014). Yet, poor diets are not always the result of resource constraints but also of poor food choice and eating practices (Truman and Elliott Citation2019; Webb and Sheeran Citation2006). For this, insights into consumption behavior are essential for improving dietary choices to tackle different forms of malnutrition. While consumer behavior is well studied in developed countries, little is known about it in poor countries.
This study aims to understand underlying motives for consumer behavior in Addis Ababa, Ethiopia, and their relationship with nutrition knowledge. We answer the following research questions: (1) Do people with more nutrition knowledge consume more diversified diets? (2) Do they have more positive attitudes toward healthy eating? (3) Does nutrition knowledge limit endorsement of harmful food taboos about diets of children and women?
Ethiopia provides an interesting case. Like other low-income countries, it has lately witnessed transitions in its food value chains and retail landscape. Markedly, the traditional food basket is steadily changing with more preference for high-value foods, such as animal and processed foods, and increasing willingness-to-pay for convenience foods (Worku et al. Citation2017). While the nutrition transition is in its early stage and mostly affects urban areas, its malicious health effects are already observed: urban overweight/obesity rates have reached 21% for women, as compared to 4 percent in rural areas (ICF Citation2016). Like in many African countries, Ethiopia has multiple food taboos, some of which limit possibilities for consuming healthy diets. Unlike its neighboring countries, a large share of the population is Orthodox Christian and therefore, expected to respect numerous fasting periods. When fasting, people generally skip breakfast, eat mostly one meal a day late in the afternoon or evening, and abstain completely from meats, fats, eggs and dairy products. The total number of fasting days amounts to about 250 a year. Besides linger fasting periods, such as Lent and Advent, every Wednesday and Friday are observed as fast.
Studies linking nutrition knowledge to diets are rare for Eastern Africa and specifically Ethiopia. The most related study we could find studied the relationship between maternal nutrition training/knowledge and child nutrition in rural Ethiopia (Hirvonen et al. Citation2017). Similar studies covered other East African countries (Debela et al. Citation2017; Ickes et al. Citation2017; Nabugoomu et al. Citation2015). To the best of our knowledge, there are no studies for the region considering consumption of households or adults and no studies analyzing comparable motives, attitudes, and behaviors.
Methods and materials
Sampling strategy and data collection
Data were collected using a multi-stage sampling in Addis Ababa in the fall of 2017. We randomly selected 25 households (addresses) in each of 40 ketanas (city-subdistricts), which were spread over different districts and sub-cities through a sampling procedure using stratification based on food expenditure per capita and total calorie (gross) intake per individual per day (CSA, Citation2007). Melesse et al. (Citation2019) provides full descriptions of the sampling procedures. We visited the selected households at their homes for an interview. Target respondents were individuals mainly responsible for food purchase and/or preparation decisions. Unfortunately, refusal to participate was not uncommon. We had to randomly reselect 30 new households, which were distributed over 28 city-subdistricts, to approach our target sample. In the end, 996 respondents were interviewed.
Ethical approval for research protocols, process, data management, and risks related to participation in the research was obtained from the Social Sciences Ethics Committee at Wageningen University. Addis Ababa sub-city administrations granted permissions to conduct the study. All participants provided written informed consent before participation.
Questionnaire and key variables
We used a structured questionnaire consisted of modules on sociodemographics, food choice and consumption, eating attitudes, practices, and believes, food safety, and nutrition knowledge. Below, we discuss the questions used for the analysis in more detail.
Nutrition knowledge was assessed using questions about nutrition and health. Most questions are derived from the general nutrition knowledge questionnaire validated for developed countries (Axelson and Brinberg Citation1992; Parmenter and Wardle Citation2000), as efforts validating nutrition knowledge in developing countries have been limited (Bukenya, Muyonga, and Andrade Citation2015). Some questions were modified to reflect recent knowledge or the local context (e.g., altering food items) to enhance understanding. Our final instrument contains 43 questions capturing three domains of nutrition knowledge: (1) advice from health experts (12 questions), (2) food groups and nutrient sources (23 questions), and (3) diet–disease relationships (8 questions). The specific questions are presented in in the results section, along with the key results.
Table 1. Summary of nutrition knowledge scores for different quintiles as sub-samples
Table 2. Socioeconomic data for the study sample (n = 996)
Table 3. Nutrition knowledge
Dietary diversity was assessed using a 7-day recall for consumption of the 12 food groups distinguished by FAO (Citation2010): cereals; white roots and tubers; vegetables; fruits; meat; eggs; fish and fish products; legumes, nuts, and seeds; milk and milk products; oils and fats; sweets and sugars; and spices, condiments, and beverages. This tool is commonly used to calculate the household dietary diversity score (DDS) in poor and middle-income countries. DDS is simply the number of food groups consumed over a specified recall period. A high-quality diet contains a variety of food groups, and the DDS has been shown to be a good predictor for micronutrient adequacy and nutrition outcomes (Steyn et al. Citation2006). Specifically for Ethiopia, the household DDS is strongly and positively associated with household’s mean probability of nutrient adequacy (Mekonnen et al. Citation2020). We deviated from the standard practice of using a 24-hour recall and used a one-week recall instead. We did this to avoid biases from religious fasting: Orthodox Christians (80% of our sample) are expected to abstain from eating animals sourced foods on Wednesdays and Fridays. There were no prolonged fasting periods during data collection.
We used a range of questions to assess the underlying motives for food choice. We considered seven motives for food choice: health, taste, price, food safety, familiarity, nutritional value, easiness to prepare. We asked respondents to assess the importance of each of these motives when deciding on which food to buy on a five-point scale ranging from not at all important to very important. In addition, we used the food-choice questionnaire developed by Steptoe, Pollard, and Wardle. (Citation1995) to ask people about the importance of a number of characteristics of the food they eat on a typical day. Relevant for this paper are the health-related characteristics, such as being low in fat, containing a lot of vitamins and minerals, and being high in fiber and roughage (for details see ). Relatedly, we asked people whether they agreed or not with a set of statements about their eating behavior, for example, whether they try to limit the amount of salt added to their food and whether they tried to avoid consuming high-calorie products with poor nutritional value (details are presented in ). Finally, we asked whether people judged three potentially harmful food taboos. We selected taboos for women and children, as these are most vulnerable to food taboos in Ethiopia (Zepro Citation2015), related to the consumption of pregnant women (no green leafy vegetables and no meat, milk, yogurt and other supposedly fatty foods) and young children (no meat until 24 months) to be false or corrects (see ).
Table 4. Dietary composition (n = 996)
Table 5. Drivers of food choice (n = 996)
Statistical analysis
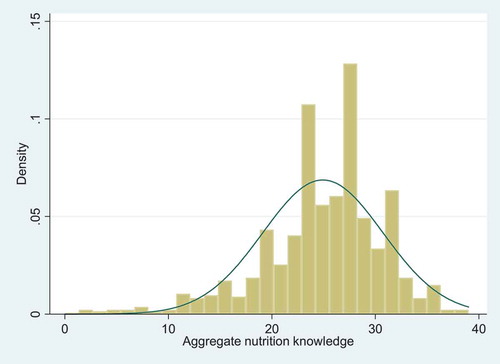
To assess the relation between nutrition knowledge on the one hand and diets and motives for food consumption on the other hand, we first created an aggregate nutrition knowledge score by simply counting the number of correct answers, which potentially ranged from 0 to 43. The actual scores obtained by the respondents ranged from 0 to 39 (see ). Next, we grouped households into quintiles according to the score they obtained (). We then calculated the distribution of variables for the diet and food choice motives over the knowledge quintiles and used ANOVA to assess whether the indicator of interest differ significantly between the knowledge quintiles. We feel that this approach does justice to the potentially not purely causal and non-linear relationship between nutrition knowledge and diets and motives of food choice. We present the p-values of the test and use a 5% significance level as a cutoff for our inferences. When groups are significantly different, we use T-test to assess differences between specific quintiles. Again, we use a 5% significance level.
Figure 1. Distribution of the aggregate nutrition knowledge score (N = 996)
Characteristics of the respondents
contains descriptive information on respondents. Most respondents were female (82%), Orthodox Christian (80%) and had at least some formal education (74%). The average respondent was aged about 44 years and came from a family of about five members. The average household has resided for 25 years in its current residence and about 40% of the households moved to Addis from places more than 20 km away. About 40% of households earned less than 110 USD per month. The primary economic activity was nonpublic employment, and few households had access to a garden or a farm. Around 20% of the respondents had received remittance income. About 10% of the respondents reported having a health or nutrition-related qualification.
The male and female subsamples represent respondents with a different role in food choice. While females are almost all responsible for both food purchases (92%) and food preparation (97%), most males are responsible for purchases (98%) and not necessarily for preparation (30%).
Results
Nutrition knowledge
On average, respondents gave correct answers to 25 out of 43 answers, but as indicated before, there were substantial differences in knowledge between people. Most people were aware health experts advise higher consumption of fruits and vegetables and lower intake of sugary, fatty, and salty foods (). The need to eat more fiber was only known by 51% of respondents, and knowledge about expert advice for meat and starchy foods was even less widespread, with 42 and 25% of respondents able to reproduce the correct advice. However, we must note that there are no Ethiopia-specific messages, and the standard advice of eating less meat, or even no change in starchy foods, may not apply to many respondents. Most knew at which age to introduce solid food, but they do not know the appropriate consistency of porridge for young children.
About two-thirds of respondents knew that bread, cereals, rice, and pasta are good sources of carbohydrates. Few knew that chicken is low in carbohydrates, that fruits are low in proteins, and that proteins and vitamins are not good sources of energy. Also, a large majority falsely claimed that sunlight is an important source of vitamin C and that table salt has a lot of vitamins and minerals. As per diet–health relationships, knowledge was fairly low, ranging from 30% for causes of obesity to 71% for dietary cause of high blood pressure. Interestingly, 92% was aware that a high intake of salt might increase blood pressure.
Diet quality
On average, respondents consumed from 8.5 out of the 12 food groups (). Many individual food groups are consumed by less than 60% of households. Household DDS consistently increases with nutrition knowledge. The consumption of fruits, vegetables, legumes, nuts and seeds, and some animal-source foods, food groups associated with high-quality diets, increased with nutrition knowledge, although not between all quintiles. Yet, also the consumption of oils and fats was positively associated with nutrition knowledge.
Motives for food choices
Health was considered an important motive of food purchases for 91% of people. As health can mean different things, we also asked more specifically for the importance of food safety and nutrition. Safety was a much more prominent concern, considered important by 78 percentage of respondents. Nutritional value was only considered important by 63%. The only motive that was considered important by less people was easiness to prepare.
We see a related pattern in the answers to the questions about the food people eat on a typical day. 86% considers it important that this keeps them healthy, whereas only 71% states that it is important that the food is nutritious. The lowest-scoring factors are “low in calories” (43%) and “helps me control my weight” (48%).
Regarding specific healthy practices, most respondents (91%) indicate that they try to limit intake of salt and saturated fats (81%). Just over half try to replace conventional foods with healthier versions (55%) and avoid calorie-dense products with low nutrition (52%). A considerable proportion of respondents endorses potentially harmful food taboos. Only 49% of respondents rejected the statement that young children should not eat meat (47%). The number of rejections was somewhat higher for the statements that pregnant women should avoid the consumption of meat and milk products (62%) and green leafy vegetables (73%).
Looking at the results for the food knowledge quintiles, we see that nutrition knowledge and the importance that people give to health and nutrition in their food choices are positively related. Interestingly, we find the increase mostly between the lower quintiles. The relationship is reflected in a higher likelihood of having healthy eating practices and a lower endorsement of potentially unhealthy food taboos for people in higher knowledge quintiles. Unfortunately, food taboos do not disappear, even for the group with the highest nutritional knowledge.
Discussion
This study provides a unique insight into food consumption patterns, their underlying motives and how these are related to nutrition knowledge in Addis Ababa, Ethiopia. We found that on average households in Addis Ababa, Ethiopia, consumed 8.5 out of 12 food groups in the past 7 days. This is quite similar to the 7.9 found for urban areas by Mekonnen et al. (Citation2020), who base their results on a nationally representative survey for Ethiopia for 2015/16. That our number is somewhat higher could be due to the rapid economic development of the country in recent years and because Addis Ababa is a relatively wealthy city within the country.
Dietary diversity ranged from 7.5 in the lowest nutrition knowledge quintile to 9.3 in the highest quintile, with gradual increases in between. The likelihood that a household had consumed fruits, vegetables, legumes, nuts, and seeds, and oils and fats increased with knowledge. The only other study about the relation between nutrition knowledge and diets in Ethiopia that we could find studied the impact of maternal nutrition knowledge on children’s dietary diversity in rural areas in northwestern Ethiopia. Hirvonen et al. (Citation2017) found a positive relation, but only in areas with relatively good market access. Similar positive relations between maternal nutrition knowledge and children’s diets and nutrition were found for other Eastern African countries, such as Kenya (Debela et al. Citation2017), Tanzania (Nabugoomu et al. (Citation2015) and Uganda (Ickes et al. Citation2017).
Relatively few respondents considered nutritional value and important food choice motive, and many had little knowledge about the nutrient content of different food groups was limited. A limited share of respondents had insight in the causes and consequences of obesity. Relatedly, attitude statements on avoiding obesity were considered important by less than half of respondents, and relatively few people agree with healthy eating practices related to weight control. Both attitudes and practices related to obesity improved with nutrition knowledge but are still concerning for the highest quintiles. This may be understandable, as obesity is a relatively new problem in Ethiopia. However, obesity rates are rising rapidly in Addis Ababa, especially among adult women (Wolle et al. Citation2020).
Many respondents supported potentially harmful food taboos. For example, only half of respondents rejected the statement that children younger than two years of age should not be given meat and meat products. This belief can be very damaging, as there is a strong association between stunting and the consumption of animal-source foods in Eastern and Southern Africa (and other developing regions) (Heady, Hirvonen, and Hoddinott Citation2018). The prevalence of stunting is high in Ethiopia, ranging from 15% in Addis Ababa to 46% in less developed regions (ICF Citation2016), where we would expect the food taboos to be even more adhered to. Also, the food taboos for pregnant women could harm child nutrition in the crucial first 1000 days. Believe in food taboos decreases with nutrition knowledge, but is present even in the highest knowledge quintile.
The data thus give elaborate information about nutrition knowledge, consumer motives, and dietary choices and show clear patterns in their relationships. However, the dataset does not allow for causal inference. In addition, we have not studied which factors moderate the relation between knowledge and behavior.
In conclusion, this study provides a unique insight in the consumption behavior and motives of urban consumers in Ethiopia, using a large, representative survey among consumers in Addis Ababa. Ethiopia presents an exceptional context, even in the East Africa region, with a large population of Orthodox Christians, many of whom adhere to strict fasting rules, high rates of undernutrition combined with rising levels of obesity. Key findings are that nutrition knowledge is positively related to healthy attitudes, practices, and diet quality. People still adhere to food taboos that may harm child nutrition and development and that knowledge about obesity is still very limited. Future nutrition education practices should explicitly target (incorrect) beliefs about dietary practices of children and women and introduce the topic of obesity to counter the negative effects of the food transition.
Declaration of interest
The authors declare no conflicts of interest in connection with this article.
Additional information
Funding
References
- Axelson, M. L., and D. Brinberg. 1992. The measurement and conceptualization of nutrition knowledge. Journal of Nutrition Education 24 (5):239–46. doi:10.1016/S0022-3182(12)81238-6.
- Bukenya, R., J. Muyonga, and J. Andrade. 2015. Development and validation of a general nutrition knowledge questionnaire for adults in Uganda. Journal of Nutrition Education and Behavior 47 (4):S62. doi:10.1016/j.jneb.2015.04.165.
- Central Statistical Agency (CSA) of Ethiopia. 2007. Statistical report, household income, consumption and expenditure survey 2004/05. Volume II, Number 394, Addis Ababa.
- Debela, B. L., K. M. Demmler, R. Rischke, and M. Qaim. 2017. Maternal nutrition knowledge and child nutritional outcomes in urban Kenya. Appetite 116:518–26. doi:10.1016/j.appet.2017.05.042.
- Food and Agriculture Organization of the United Nations (FAO). 2010. Guidelines for measuring household and individual dietary diversity. Rome, Italy: FAO.
- Gillespie, S., and M. van den Bold. 2017. Agriculture, food systems, and nutrition: Meeting the challenge. Global Challenges 1 (3):1600002. doi:10.1002/gch2.201600002.
- Heady, D., K. Hirvonen, and J. Hoddinott. 2018. Animal sourced foods and child stunting. American Journal of Agricultural Economics 100 (5):1302–19. doi:10.1093/ajae/aay053.
- Hirvonen, K., J. Hoddinott, B. Minten, and D. Stifel. 2017. Children’s diets, nutrition knowledge, and access to markets. World Development 95:303–15. doi:10.1016/j.worlddev.2017.02.031.
- ICF. 2016. Ethiopia demographic and health survey 2016. Addis Ababa, Ethiopia, and Rockville, MD: CSA and ICF.
- Ickes, S. B., C. Baguma, C. A. Brahe, J. A. Myhre, L. S. Adair, M. E. Bentley, and A. S. Ammerman. 2017. Maternal participation in a nutrition education program in Uganda is associated with improved infant and young child feeding practices and feeding knowledge: A post-program comparison study. BMC Nutrition 3 (1):32. doi:10.1186/s40795-017-0140-8.
- IFPRI. 2016. Global Nutrition Report 2016: From Promise to Impact - Ending Malnutrition by 2030. International Food Policy Research Institute, Washington, DC.
- Mekonnen, D. A., E. F. Talsma, L. Trijsburg, V. Linderhof, T. Achterbosch, A. Nijhuis, R. Ruben, and I. D. Brouwer. 2020. Can household dietary diversity inform about nutrient adequacy? Lessons from a food systems analysis in Ethiopia. Food Security 1–17. doi:10.1007/s12571-020-01056-5.
- Melesse, M. B., M. van den Berg, A. de Brauw, and G. T. Abate. 2019. Understanding urban consumers’ food choice behavior in Ethiopia to promote demand for healthy foods. ESSP Working Paper. IFPRI.
- Monteiro, A., J. Moubarac, G. Cannon, W. Ng, and B. Popkin. 2013. Ultra-processed products are becoming dominant in the global food system. Obesity Reviews 14 (S2):21–28. doi:10.1111/obr.12107.
- Nabugoomu, J., A. Namutebi, A. N. Kaaya, and G. Nasinyama. 2015. Nutrition education influences child feeding knowledge attitudes and practices of caregivers in Uganda. American Journal of Health Research 3 (2):82–90. doi:10.11648/j.ajhr.20150302.15.
- Parmenter, K., and J. Wardle. 2000. Evaluation and design of nutrition knowledge measures. Journal of Nutrition Education 32 (5):269–77. doi:10.1016/S0022-3182(00)70575-9.
- Popkin, B. M. 2014. Nutrition, agriculture and the global food system in low- and middle-income countries. Food Policy 47:91–96. doi:10.1016/j.foodpol.2014.05.001.
- Popkin, B. M., L. S. Adair, and S. W. Ng. 2012. Global nutrition transition and the pandemic of obesity in developing countries. Nutrition Reviews 70 (1):3–21. doi:10.1111/j.1753-4887.2011.00456.x.
- Steptoe, A., T. M. Pollard, and J. Wardle. 1995. Development of a measure of the motives underlying the selection of food: The food choice questionnaire. Appetite 25:267–84. doi:10.1006/appe.1995.0061.
- Steyn, N. P., J. H. Nel, G. Nantel, G. Kennedy, and D. Labadarios. 2006. Food variety and dietary diversity scores in children: Are they good indicators of dietary adequacy? Public Health Nutrition 9 (5):644–50. doi:10.1079/PHN2005912.
- Truman, E., and C. Elliott. 2019. Barriers to food literacy: A conceptual model to explore factors inhibiting proficiency. Journal of Nutrition Education and Behavior 51 (1):107–11. doi:10.1016/j.jneb.2018.08.008.
- Webb, T. L., and P. Sheeran. 2006. Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychological Bulletin 132 (2):249–68. doi:10.1037/0033-2909.132.2.249.
- Wolle, A., K. Hirvonen, A. de Brauw, K. Baye, and G. T. Abate. 2020. Household food consumption patterns in Addis Ababa, Ethiopia. ESSP working paper 139. IFPRI.
- Worku, H. I., M. Dereje, B. Minten, and K. Hirvonen. 2017. Diet transformation in Africa: The case of Ethiopia. Agricultural Economics 48 (S1):73–86. doi:10.1111/agec.12387.
- Zepro, N. B. 2015. Food taboos and misconceptions among pregnant women of Shashemene District, Ethiopia. Science Journal of Public Health 3 (3):410–16. doi:10.11648/j.sjph.20150303.27.