
ABSTRACT
This study empirically assesses the relationship between mothers’ education and child health using continuous and binary proxies of child health outcomes. A panel, using four waves of the National Income Dynamic Study and a battery of estimation techniques, was employed. The results suggest that maternal education plays a large and significant role in explaining child health outcomes in South Africa. Our results also suggest that maternal education is relevant in respect to stunted growth (stunting). However, the effects of maternal education vary along races, implying levels of inequality. The effects are stronger in the black and coloured populations, possibly due to educational deficits. This suggests a need in improving the educational opportunities for these groups. We suggest that maternal education can significantly contribute to reducing the high degree of inequality in South Africa.
1. Introduction
Poverty and unemployment are critical issues in many developing countries, including South Africa. Although remarkable progressFootnote1 has been made in South Africa since the first democratic elections in 1994, poverty and unemployment remain prevalent and persistent. While poverty rates have marginally declined,Footnote2 unemployment increased from 20.0% in 1994 to 25.1% in 2014 (Statistics South Africa, Citation2015). In addition, the country grapples with worsening levels of socio-economic inequality with considerable disparities across racial groups, which find their origin in the legacy of colonialism and the apartheid era.Footnote3 Particularly, significant human capital gaps in terms of education and health are observed,Footnote4 which play a key role in driving unemployment and hence, poverty (Woolard, Citation2002; Branson et al., Citation2012).
Health is particularly important because it affects the ability to acquire other forms of capital including education. Interestingly, the health of children is a significant predictor of long-term socio-economic outcomes in subsequent adulthood (Case et al., Citation2002, Citation2005; Belli et al., Citation2005; Black et al., Citation2011). Moreover, empirical literature documents the existence of a positive relationship between childhood and adult health. In effect, one’s childhood health may influence one’s adult health and education and ultimately could have an impact on the future employment prospects of the child.
The World Health Organization (WHO) indicates that half of the deaths of children under the age of five years are caused by undernutrition. In addition, malnutrition in children’s early lives may lead to stunted growth (stunting), which is detrimental to cognitive ability, thus impairing school and work performanceFootnote5 (WHO, Citation2009). In South Africa, Shisana et al. (Citation2014) find survey-based evidence that the prevalence of stunting in children of under three years is about 26.5% for boys and 25.9% for girls. Furthermore, this appears to be more prevalent with boys in informal rural areas (23.2%) than formal urban areas (13.6%). This is a possible indication of the after-effects of educational segregation along racial lines, since the Black/African group mainly inhabits rural areas. Understanding the intergenerational implications of the parents/children health overlap is therefore imperative for poverty alleviation.
Many parental factorsFootnote6 that could contribute to the health of children under the age of five years have been identified, the education of the primary caregiver being of particular consideration (Salm & Schunk, Citation2008; Chen & Li, Citation2009; Lundborg et al., Citation2011; Aizer & Currie, Citation2014). In South Africa, primary caregivers are mostly biological mothers and more than half of the children below the age of 10 years live in female-headed households (Statistics South Africa, Citation2013).Footnote7 Given that other females often take on the role of caregiver, it is not only the biological characteristics of mothers that matter for children’s health, but also those of other female caregivers in the family – including aunts, sisters, and grandmothers – as well as, in some cases, those of non-biological custodians. In substantiating this, Chen and Li’s (Citation2009) analysis of a large sample of adoptees in China is useful in that it concludes that education of non-biological caregivers significantly influences children’s health. For the purpose of this study, we argue that the female primary caregiver’s (the biological mother or non-biological custodian) education represents an important driver of human capital for future generations. Hence, a sound policy response to unemployment and/or poverty entails an understanding of the relationship between maternal education and child health.
Maternal education levels can affect child health through two main channels (mechanisms or pathways). Firstly, it is indirectly affected through increased income – through mothers being in the labour force (Lindeboom et al., Citation2009; Aslam & Kingdon, Citation2012) – which could provide better choices in terms of the affordability of care and increased prospects of better care. Secondly, a child’s health can be impacted directly through maternal health literacy (Lindeboom et al., Citation2009). This knowledge can translate into correct nutritional choices being made in the early years of children’s lives, which have been found to affect not only physical but also mental development (UNESCO, Citation2006). While these two channels are favourable to the establishing of a positive relationship between maternal education and child health, a third plausible channel exists, which, though less documented, cannot be ignored. Unlike the first two – which demonstrate a positive relationship between a mother’s education and a child’s health and future – the third alternative suggests that a mother’s education may negatively affect child health through the unavailability of educated mothers due to school and/or work demands (Glewwe & Desai, Citation1999; Case & Paxson, Citation2001; Lesiapeto et al., Citation2010). Overall, a mother’s education could have far-reaching consequences for her child’s future health, and, ultimately, productivity.
The remainder of this paper is organised as follows: section 2 presents a review of the literature, while sections 3 and 4 present the methodology and empirical results respectively; section 5 provides concluding remarks and recommendations in light of the findings.
2. Literature review
Theoretically, Grossman’s human capital theoryFootnote8 provides the conceptual framework for the relationship between maternal education and child health. The basic idea is that the productivity and skills of workers can be increased by investing in them, particularly in terms of education (Becker, Citation1975; Grossman, Citation1999). This implies that a higher educational qualification could mean improved chances of employment and increased earnings. Furthermore, Grossman argues, in the health capital theory,Footnote9 that health, as a form of human capital, is distinct from other forms of human capital as it contributes to earnings in the life cycle. Grossman develops a demand for the health capital model, which has been used to empirically analyse the health production function (Zhao, Citation2008; Ajakaiye & Mwabu, Citation2012). Consequently, this study uses a reduced form of the health production function to examine the relationship between maternal education and child health outcomes in South Africa.
The relationship between parental education and child health has been widely explored in empirical literature, mainly based on cross-sectional studies (Ahmed & Iqbal, Citation2007; Chen & Li, Citation2009; Lindeboom et al., Citation2009; Lundborg et al., Citation2011; Aslam & Kingdon, Citation2012; Rawlings, Citation2015) and/or panel data methodologies (Lindeboom et al., Citation2009 Bhalotra & Clarke, Citation2013; Kemptner & Marcus, Citation2013).
In terms of cross-sectional studies, Ahmed & Iqbal (Citation2007) analyse the impact of mothers’ education on child health in Nigeria proxied by the height-for-age z score (HAZ). Their results indicate that post-primary education exhibits a significant effect on child health, while the effect of primary education, which is the first six years of formal schooling, appears insignificant. Similarly, Aslam & Kingdon (Citation2012), in a study in Pakistan, evaluate whether and how parents’ years of schooling affect child health outcomes measured as HAZ. Their results suggest that an additional year of a mother’s education significantly increases a child’s health, irrespective of gender. Likewise, Güneş (Citation2015) investigates the impact in Turkey. He finds that, overall, the completion of primary education of mothers improved their children’s health. However, his results indicate mixed effects depending on geographical characteristics and gender.
Conversely, some studies (such as Desai & Alva, Citation1998; Lesiapeto et al., Citation2010) have found no strong correlation regarding this relationship. Desai & Alva (Citation1998) analyse the Demographic and Health Survey data for 22 developing countries (South Africa not included) and report a statistically significant effect in only a few countries. Their empirical investigation is based on three markers of child health, namely the infant mortality rate, children’s HAZs, and immunisation status. These conflicting results might be attributed to unobserved heterogeneities that cannot be accounted for within a cross-sectional framework.
Panel data analysis is acknowledged for its ability to mitigate the issue of unobserved heterogeneity. Within this framework, various studies report diverse findings, depending on the contextual settings.
Findings differ in developed and developing countries. However, there are also differences when looking at findings in individual countries, developed or developing. Lindeboom et al. (Citation2009), for example, conducted a United Kingdom (UK) based study using different child health indicators. They found evidence that parental education, as proxied by schooling, improves economic opportunities, whereas there is little evidence of a causal relation between parental education and child health. Contrariwise, in another developed nation, Germany, Kemptner & Marcus (Citation2013) used a large panel data set to investigate the causal linkages between maternal education and child’s health on the one hand, and schooling outcomes on the other. They reported mixed findings. Their findings indicated that, while there is a positive effect of maternal education on an adolescent son’s health, they found no association between maternal education and health in adolescent daughters.
In the context of developing countries, Bhalotra & Clarke (Citation2013) employed a panel of 108 developing countries over a 20-year period from 1990 to 2010. They found that the increased level of a mother’s education might have contributed to significant decreases in child health proxies, as measured by child mortality. Likewise, Rawlings (Citation2015) used the China Health and Nutrition Survey (CHNS) for the period 1997–2011 to explore the impact of parental education on child health in China. Her findings suggest that maternal education, rather than paternal education, matters for child health measured by anthropometric proxies. In addition, she concludes that an additional year of maternal schooling increases a boy child’s height by 0.16 standard deviation points in comparison with that of the girl child, which was statistically insignificant. She argued that this gender bias could be the result of the preference for sons in China.
In Africa, Alemayehu Azeze & Huang (Citation2014) analyse the effect of maternal education on chronic and acute malnutrition with the use of the 2000 and 2005 Demographic and Health Surveys. Their results reveal the importance of socio-economic status in the relationship between maternal education and child health. Overall, these panel data studies reveal that, although there is a consensus on the importance of maternal education for children’s health, there are mixed and inconclusive results. This could perhaps be an indication that the relationship between maternal education and child health may well require country-specific analysis.
In South Africa, Medrano et al. (Citation2008) used the South African 1993 Demographic and Health Survey data to investigate the relationship between mothers’ education and child health. Using a two-stage least square estimation, they discovered a significant effect of maternal education on children less than two years of age, but not on older children. Similarly, Lesiapeto et al. (Citation2010) explored the use of anthropometric data in the rural districts of the Eastern Province and Kwa-Zulu Natal in South Africa. While they assert that there is an association between household income and children’s stunting, they find no evidence between maternal education and this. A possible explanation for this may be that the income effect is more prominent in the rural areas. Arguably, this could have implications for poverty and inequality, which are still key persistent issues in South Africa more than two decades after the first democratic elections. In spite of this, not much empirical evidence is available to address this and guide policymakers.
Following the panel approach,Footnote10 this study allows us to control for unobservable time invariant heterogeneity, which arises from the diverse socio-demographics, in terms of age and race, as well as previous racial segregation. Therefore, South Africa offers a unique context in which to analyse this relationship. In addition, we make use of two child health proxies: the continuous anthropometric measure and the binary (stunting). To the best of our knowledge, this is the first study to explore this relationship in a panel data framework in South Africa. This has been made possible with the availability of the National Income Dynamic Study (NIDS) data set, which is currently available for the years Citation2008, Citation2010, Citation2012 and Citation2014 (Leibbrandt et al., Citation2009).
3. Methodology
The present study relies on both the continuous (HAZ) and binary (stunting) proxies of child health outcomes, thus motivating the use of both linear and non-linear panel approaches.
3.1. The model
The model is adapted from the reduced form of the health production framework of Grossman (Citation1972), as used by Aslam & Kingdon (Citation2012), and of the form:(1) where:
is the child health outcome;
indicates maternal education; and
is a vector of demographic and other socio-economic characteristics (age, gender and immunisation); family background (household size) and community effects (area of residence and race) for child i at time t; and µit is the error term.
Following the literature (Thomas et al., Citation1991; Strauss & Thomas, Citation1998; Ahmed & Iqbal, Citation2007; Chen & Li, Citation2009; Aslam & Kingdon, Citation2012; Mani, Citation2014), we use the HAZ scoreFootnote11 as a measure of the child health outcome in the linear approach. Besides the HAZ, the health literature (see for example, Alemayehu Azeze & Huang, Citation2014) emphasises the role of stunting in characterising the child health status. Hence, for the non-linear approach, CHit is a binary variable describing whether a child is stunted or not. Evidence of stunting is measured, according to the WHO, as a z-score of less than two standard deviations from the reference median (WHO, Citation2006).
3.2. Estimation techniques
Equation (1) will produce consistent estimates of β, conditional upon the expectation that maternal education (MEit) and child health outcomes (CHit) are uncorrelated, with the error term (µit) (Wooldridge, Citation2002:83). Though we undertake the Wald test for exogeneity under the two-stage least squares (2SLS) approach, we are more comfortable in applying a set of estimation techniques for robustness. We therefore apply: Pooled Ordinary Least Squares (POLS), Weighted Least Squares (WLS), Fixed/Random Effects (FE or RE), and Instrumental Variable (IV) techniques in our underlying model. The least squared estimates (POLS and WLS) assume no correlation between regressors and the error term. This, however, does not hold in the presence of individual heterogeneities (), resulting in biased and inconsistent estimates. Therefore, the FE or RE is implemented, which is commonly used to mitigate the issue of heterogeneity, with the Hausman test providing the formal selection method between the FE and RE estimations.
In complementing the continuous dependent variable (HAZ) approach above, the maximum likelihood (ML) technique will be used for binary child health outcomes. This captures the determinants of the probability of stunting, of which maternal education is one. The probit model is specified below:(2) where: Pr is the probability of stunting, (HAZ stunted/HAZ not stunted);
is the cumulative distribution function; X is a vector of regressors; and β and
are the parameters.
The ML technique estimates (from the probit approach) show the probability of children’s growth being stunted. Conditional upon the notion that the estimates are consistent, the predicted conditional probability of their being stunted for an observation i is given by:(3) where
is the cumulative distribution function of the standard normal distribution and
and
are the estimates of the parameters. OLS, WLS, fixed effects/random effects (FE/RE) and ML estimates are consistent under strict exogeneity of the independent variables. However, given the plausibility of
being endogenous,Footnote12 the IV is used. In fact, our independent variable of a mother’s education is measured by years of schooling, which is not free from measurement errors. Moreover, it can be argued that maternal attributes like education can be influenced by child health, thus resulting in simultaneity. For example, a malnourished or undernourished child increases his/her susceptibility to infections, and enhances the severity thereof, thus inhibiting school attendance of the mother/caregiver. In addition, unidentified important causal factors might have been omitted, which equally result in omission bias, which is a source of endogeneity, hence justifying the use of the IV technique.
Because of such endogeneity, the estimation of the parameter β in Equation (1), as well as the other parameters of the model, may be biased by some measure of the degree of correlation in the unobservable, affecting both and
. The estimation of Equation (1) is then conducted simultaneously with the mother’s education Equation (2) – through the two-stage least squared technique or the method of Limited Information Maximum Likelihood (LIML) – for the continuous and binary dependent variables respectively. Equation (4) is specified as follows:
(4) where MEit is the mother’s education, Zit is the instruments, Xit represents a vector of demographic and socio-economic characteristics (age, gender and immunisation); family background (household size) and community effects (area of residence and race) which is uncorrelated with the error term ℇit and correlated with MEit.
The validity of the IV type estimates crucially depends on the quality of the instruments. While it is often difficult to obtain truly exogenous instruments, we follow Aslam & Kingdon (Citation2012) in using the exposure to media as a proxy for information knowledge. Exposure to media also serves as a pathway through which maternal education affects child health outcomes. For example, an educated mother can better acquire health information useful for child health enhancement, but this is conditional on ownership of information gadgets such as radios and television sets. These gadgets can therefore be used as instruments for education in order to circumvent the issue of endogeneity.
These instruments (radios and television sets) are expected to satisfy the following two conditions: (1) being uncorrelated with the error term (that is Cov [Zit,εjs] = 0) and only indirectly correlated to the dependent variable (CHit); and (2) being strongly correlated with the endogenous variable (MEit). These exogeneity conditions are confirmed with the Sargan–Hansen test. In addition to the exogeneity test, the statistical validity of the instruments must be confirmed through the over-identification test when using more than one instrument.
3.3. Data and variable description
The data for this study is sourced from the four waves of the NIDS data set for the years Citation2008, Citation2010, Citation2012 and Citation2014. The NIDS is an ongoing longitudinal nationally representative household survey. It is the first nationally representative panel survey in South Africa and is conducted biannually by the Southern Africa Labour and Development Research Unit (SALDRU). The first wave (Citation2008) consisted of about 28,000 individuals in 7300 households across the country. The initial respondents, which are referred to as the Core Sample Members (CSM), are tracked over the years (Leibbrandt et al., Citation2009). After that, those who were present in the initial sample, as well as their spouses and children, are re-interviewed, thus creating a balanced panel. After having restricted the study to children under five years of age with female caregivers (mothers and other female primary caregivers), our sample size is 9937.
3.4. Dependent variable: child health measure
In line with the existing literature (Lindeboom et al., Citation2009; Aslam & Kingdon, Citation2012; Mani, Citation2014) and the objective of this study, our focus is on one aspect of anthropometric data of child health, which is the HAZ.Footnote13 HAZ is an indicator of child health, which measures both short- and long-term health statuses (Thomas et al., Citation1991; Strauss & Thomas, Citation1998; Behrman & Rosenzweig, Citation2005; Medrano et al. Citation2008; Chen & Li, Citation2009). It is measured as the number of standard deviations from the median height of the reference population of the same age as charted by the WHO growth standards. Therefore, HAZ closer to 0 indicate normal and well-nourished children. However, HAZs less than −2 are classified as being stunted.
3.5. Independent variable: maternal education
Education has been used in the literature as a continuous variable in terms of either years of schooling (Lindeboom et al., Citation2009; Rawlings, Citation2015) or as a categorical variable (Alemayehu Azeze & Huang, Citation2014). The educational categories range from no schooling to university qualifications. For robustness, we adopt both approaches, which helps capture level and threshold effects. Our education variable is restricted to all female caregivers.
3.6. Control variables
In this study, various demographic variables are controlled for; details provided in , and their summary statistics in .
Table 1. Description of key variables.
Table 2. Descriptive statistics.
From the descriptive statistics in , it emerges that the averages regarding educated mothers in our sample are: about 8% without schooling; and 14%, 22% and 6% with primary, secondary and tertiary levels respectively. (panel B) exhibits remarkable racial distinctions in educational categories, affecting black mothers. This is evident from the greater percentage (about 21%) in our sample with no schooling, compared with white mothers (about 4%). Tertiary education is also the lowest among mothers, followed by coloured mothers, and highest among white mothers. This could possibly be attributed to the previous apartheid era of unequal education systems in South Africa.
Furthermore, we use kernel density estimation (KDE) to estimate the probability density function of HAZ as in and . shows the overall estimate of the sample. The skewness of the density plots to the left implies deviation from the reference point of zero, the implication of which is that there are more children who are below the reference category, and who are, therefore, more likely to have poor health outcomes based on HAZ.
Figure 1. Kernel density plots of height-for-age z score (HAZ) for children under five years.
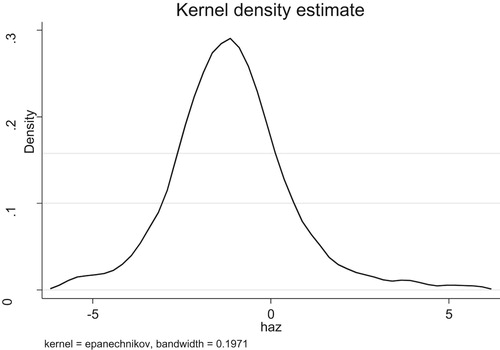
Figure 2. Kernel density plots of height-for-age z score (HAZ) for children under five years: male and female.
Note: hazm, Height-for-age z score-male; hazf, Height-for-age z score-female
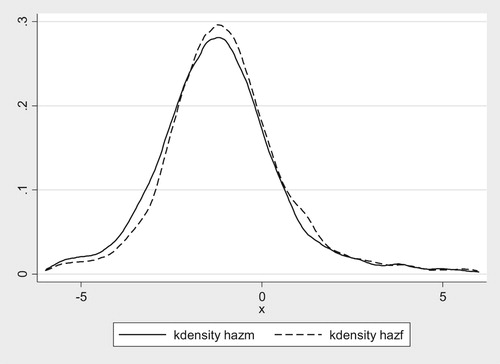
Disaggregating children by gender indicates that males have higher negative HAZ than females of the same age group, as shown on the left of the kernel density graph. This suggests that there are more male children with poorer health outcomes. This finding appears to concur with the literature, which indicates that gender biases exist in terms of children’s health. While the descriptive analysis above provides some indication of this relationship, further meaningful inference needs to be derived from the econometric analysis.
4. Empirical results
The linear panel and non-linear panel results are reported in .
Table 3. Hausman test statistics.
Table 4. Regression results of HAZ on education (years and categories) POLS, WLS and RE.
Table 5. Tests for IV (2SLS estimation).
Table 6. Regression results of POLS, WLS. RE and IV and race (blacks and coloured).
Table 7. Marginal effects of the Probit and Probit IV models: male/female.
4.1. Linear panel analysis
The linear panel results are in respect of the continuous HAZ variable. As discussed in the Methodology section, the Hausman test is the formal test on the choice between the FE and RE models to determine if the individual effects are fixed or random. The null hypothesis of the test is that the individual effects are random. The results of the test indicate a p-value of 0.3284, which is greater than the cut-off significance point of 0.05, and, therefore, we do not reject the null hypothesis. Hence, the RE model is well specified and selected.
displays the regression results of education, measured as years of schooling and educational categories, using POLS, WLS and RE and IV (for years of education). shows the tests for the IV 2SLS estimation, and , the overall results of POLS, WLS, RE and IV models, as well as the black and coloured racial groups.
In , the Lagrange multiplier (LM) test for under-identification shows that the regressor is not under-identified (p-value = 0.000).The Cragg-Donald F-statistic is relatively high (146.602) in comparison with the Stock-Yogo test critical values. We therefore reject the null hypothesis, thereby indicating that the instruments are not weak. In addition, the Sargan statistics – with a value of 1.581 and a p-value of 0.2087 – indicate instrument validity.
As shown in , after controlling for the key variables, all the models performed relatively well with stable coefficients. For example, larger household size tends to be associated with less healthy children. Older caregivers are generally better at transmitting health knowledge to child health. This variable has a non-linear effect, implying that the rate of transmission tends to reduce with age or with extreme values of age. As expected, immunisation is positive, although not significant, across all the models.
In terms of the other explanatory variables, household size has a negative effect on health and there is no significant distinction by gender. Older mothers have a significant negative effect on female children’s health and a weak positive effect on boys’ health. A negative effect of age on girls’ health tends to be weaker at extremely high maternal age. This seems to lend support to the findings of the disparate effect of education on boys and girls. Older mothers are more likely to be in the labour market than younger mothers and extremely old mothers. This, therefore, lends support to our postulated view that girls may be more vulnerable to mothers’ absence than boys and therefore the negative effect of lack of care from working mothers might outweigh the positive effects – in terms of income and knowledge and use of health related information – on the girls. This is worth investigating further and will constitute the topic of further research.
Another control variable is the area of residence. Given the comparatively poorer socio-economic conditions, the rural populace – in traditional areas and those who are farm dwellers – tend to perform lower in terms of child health compared with urban areas, which are more affluent. Most of the South African farm dwellers are farm workers, working for large-scale farmers. These constitute the poor racial groups, that is: mainly blacks and coloureds, as well as poor migrant workers (Visser, Citation2013).
The educational variables carry significant magnitude, and theoretically have the expected signs in all the regression models. An extra year of schooling gained by mothers results in a 0.87 gain in standard deviation scores. However, there is non-linearity of education, suggesting that, at higher values of education, the positive effects tend to be attenuated. This non-linearity could be explained by the fact that at higher levels of education, more time is given to the labour market at the expense of childcare.
There is some evidence that suggests that black and coloured children stand to benefit more from further educational improvements in South Africa. However, the results are not robust because of the limited sample size with respect to Asians and coloureds. We argue that, given the apartheid history of South Africa, all that is to be gained regarding education of these racial groups of mothers has not yet been gained. We suggest that the gender difference in this relationship could possibly be that girls could be more sensitive to absent mothers than boy children (Almani et al., Citation2012). The implication of this is that maternal education affects children along gender lines, boys having an advantage over girls.
4.2. Non-linear results
The results of the marginal effects are shown in .
The results of the marginal effects in the probit model indicate that one unit change in the years of mothers’ education decreases the probability of stunting by 1.83 for the overall probit model. Moreover, gender and race are found to exert a moderating effect on such a relationship. Particularly, in terms of gender, a one-unit change in years of maternal education decreases the probability of stunting by 2.17 units for males and increases the probability of stunting by 1.85 units for girls. It is also interesting to note that instrumenting for years of education reduces this probability comparatively for both males and females. In addition, the marginal effects of a mother’s education on black/African children is higher (at 0.67) than on other race groups, suggesting that, when compared with whites, black children have a higher probability of stunting.
Overall, the presented results confirm the theoretical view that maternal education has a positive and significant effect on child health, as measured by HAZ. The findings are also consistent with the studies of Medrano et al. (Citation2008) and Aslam & Kingdon (Citation2012), amongst others. Furthermore, the results also indicate the fact that maternal education affects the probability of stunting. In addition, we can infer that the results also vary along racial and gender lines, implying levels of inequality. These effects are stronger for the black and coloured populations than the white and Indian groups, possibly due to their educational deficits. These findings concur with theoretical and previous empirical literature.
5. Conclusion
This study reassesses the relationship between mothers’ education and child health in South Africa using panel survey data constructed from the (SALDRU: Citation2008, Citation2010, Citation2012, Citation2014) waves of the NIDS. Two proxies of child health outcome are employed, namely the HAZ and stunting. The empirical findings are consistent with the previous literature, particularly when endogeneity is controlled for.
The results suggest that maternal education plays a large and significant role in explaining child health outcomes in South Africa. Our results also suggest that maternal education is relevant in respect of stunting. Furthermore, considering the importance of gender and racial differences in South Africa, the evidence suggests that maternal education is more favourable for a boy than a girl. In addition, in comparison with the white and Asian races, maternal education has a more robust possible outcome for the black and coloured races. The key policy implication of this paper is that investments in education of women, especially for the African racial group, are likely to improve children’s health. This could possibly assist in alleviating poverty, and hence aid in eradicating inequality, which remains persistent in South Africa.
While non-formal education, in terms of health knowledge, might be immeasurable, this study focuses on formal education due to data availability. Likewise, the empirical set-up could not control for the possible differences in the quality of education between rural and urban areas and across regions. A natural extension of this study might therefore consist of analysing the extent to which such a relationship might be influenced by the existence of multi-level characteristics.
Acknowledgements
The authors are grateful to the Southern Africa Labour and Research Unit (SALDRU) for providing the data. The authors also express sincere appreciation to the anonymous referees for their rigorous feedback.
Disclosure statement
No potential conflict of interest was reported by the authors.
Notes
1 Over this period, poverty rates have decreased by 10% and Real Gross Domestic Product per capita has increased by 3.2% a year on average (African Economic Outlook, Citation2014).
2 This is measured using the food poverty line of ZAR 321 per month.
3 This period in South Africa’s history resulted in various laws being passed; like the Groups Area Act of 1950, which segregated the regions based on racial groups. While policies have been put in place to address these inequalities, the impact lag is relatively slow.
4 For example, only 31% of Black women are employed in comparison with white men at 73% (Department of Labour, Citation2011).
5 Although partial catch up is possible, the effect in developing countries due to poor socio-economic conditions is often more detrimental (Currie & Vogl, Citation2013).
6 Other factors that can influence children’s health include biological and environmental factors (like toxins being released and pollution being present).
7 This is as a result of previous apartheid policies, leading to male-labour migration, non-marriage, and, recently, Human Himmunodeficiency virus infection/Acquired immune deficiency syndrome (HIV/AIDS).
8 A further derivation of this theory is the human capital theory of health.
9 The health capital theory is a derivation of the human capital theory by Grossman (Citation1999).
10 Panel data has many advantages, including: identification of unobserved effects, the possibility of estimating more dynamic models, and efficiency gains.
11 The z score shows the deviations from the referenced population. Other measures are weight-for-height z score (WHZ)and weight-for-age z score (WAZ).
12 Endogeneity could result from measurement error, simultaneity and omitted errors.
13 Other anthropometric indicators include weight-for-height z score (WHZ) and weight-for-age z score (WAZ).
References
- African Economic Outlook, 2014. Macroeconomic prospects. African Development Bank. www.africaneconomicoutlook.org/en/outlook Accessed 11 July 2014.
- Ahmed, M & Iqbal, K, 2007. Is there any threshold in mother’s education and child health relationship? Evidence from Nigeria. Carleton College Department of Economics. Working Series.
- Aizer, A & Currie, J, 2014. The intergenerational transmission of inequality: Maternal disadvantage and health at birth. Science 344(6186), 856–861. doi: 10.1126/science.1251872
- Ajakaiye, O & Mwabu, G, 2012. Health effects of socioeconomic status: Methods and findings. African Development Review 24(4), 291–301. doi: 10.1111/1467-8268.12005
- Alemayehu Azeze, A & Huang, WC, 2014. Maternal education, linkages and child nutrition in the long and short-run: Evidence from the Ethiopia demographic and health surveys. International Journal of African Development 1(2), 3.
- Almani, AS, Abro, A & Mugheri, RA, 2012. Study of the effect of working mothers on development of children in Pakistan. International Journal of Humanities and Social Science 2(11), 164–171.
- Aslam, M & Kingdon, GG, 2012. Parental education and child health – understanding the pathways of impact in Pakistan. World Development 40(10), 2014–2032. doi: 10.1016/j.worlddev.2012.05.007
- Becker, GS, 1975. Human Capital: A theoretical and empirical analysis, with special reference to education, Becker, GS, 2d ed. National Bureau of Economic Research: distributed by Columbia University Press, New York
- Behrman, JR & Rosenzweig, MR, 2005. Does increasing women's schooling raise the schooling of the next generation? Reply. The American Economic Review 95(5), 1745–1751. doi: 10.1257/000282805775014263
- Belli, PC, Bustreo, F & Preker, A, 2005. Investing in children's health: What are the economic benefits? Bulletin of the World Health Organization 83(10), 777–784.
- Bhalotra, S & Clarke, D, 2013. Maternal education and maternal mortality: Evidence from a large panel and various natural experiments. Universities of Essex and Oxford, Mimeo.
- Black, SE, Devereux, PJ, Ashenfelter, O & Card, D, 2011. In Ashenfelter, O & Card, D (Eds.), Handbook of labor economics, Vol. IVb, pp.1487–1541 Chapter Recent developments in intergenerational mobility.
- Branson, N, Garlick, J, Lam, D, Leibbrandt, M, 2012. Education and inequality: The South African case. A Southern Africa labour and development research unit working paper number 75. Elsevier, Amsterdam.
- Case, A, Fertig, A & Paxson, C, 2005. The lasting impact of childhood health and circumstance. Journal of health economics 24(2), 365–389. doi: 10.1016/j.jhealeco.2004.09.008
- Case, A, Lubotsky, D & Paxson, C, 2002. Economic status and health in childhood: The origins of the gradient. The American Economic Review 92(5), 1308–1334. doi: 10.1257/000282802762024520
- Case, A & Paxson, C, 2001. Mothers and others: Who invests in children’s health? Journal of Health Economics 20(3), 301–328. doi: 10.1016/S0167-6296(00)00088-6
- Chen, Y & Li, H, 2009. Mother’s education and child health: Is there a nurturing effect? Journal of Health Economics 28(2), 413–426. doi: 10.1016/j.jhealeco.2008.10.005
- Currie, J & Vogl, T, 2013. Early-life health and adult circumstance in developing countries. Annual Review of Economics 5(1), 1–36. doi: 10.1146/annurev-economics-081412-103704
- Department of Labour, 2011. http://www.labour.gov.za/DOL/downloads/documents/annual-reports/labour-market-bulletin-report/2011-2012/lmb2012fullreport.pdf Accessed 12 October 2015.
- Desai, S & Alva, S, 1998. Maternal education and child health: Is there a strong causal relationship? Demography 35(1), 71–81. doi: 10.2307/3004028
- Glewwe, P & Desai, J, 1999. Child health and mothers’ education in Ghana. In The economics of school quality investments in developing countries. UK: Palgrave Macmillan, London, 295–326.
- Grossman, M, 1972. On the concept of health capital and the demand for health. Journal of Political economy 80(2), 223–255. doi: 10.1086/259880
- Grossman, M, 1999. The human capital model of the demand for health (No. w7078). National Bureau of Economic Research, London.
- Güneş, PM, 2015. The role of maternal education in child health: Evidence from a compulsory schooling law. Economics of Education Review 47, 1–16. doi: 10.1016/j.econedurev.2015.02.008
- Kemptner, D & Marcus, J, 2013. Spillover effects of maternal education on child’s health and health behavior. Review of Economics of the Household 11(1), 29–52. doi: 10.1007/s11150-012-9161-x
- Leibbrandt, M., Woolard, I & de Villiers, L, 2009. Methodology: Report on NIDS Wave 1. NIDS Technical Paper, no. 1. Southern Africa labour and development research unit, Cape Town. http://nids.uct.ac.za/publications/citations/2009 Accessed 10 July 2017.
- Lesiapeto, MS, Smuts, CM, Hanekom, SM, Du Plessis, J & Faber, M, 2010. Risk factors of poor anthropometric status in children under five years of age living in rural districts of the Eastern Cape and KwaZulu-Natal provinces, South Africa. South African Journal of Clinical Nutrition 23(4), 202–207. doi: 10.1080/16070658.2010.11734339
- Lindeboom, M, Llena-Nozal, A & van der Klaauw, B, 2009. Parental education and child health: Evidence from a schooling reform. Journal of Health Economics 28(1), 109–131. doi: 10.1016/j.jhealeco.2008.08.003
- Lundborg, P, Nordin, M & Rooth, DO, 2011. The intergenerational transmission of human capital: Exploring the role of skills and health using data on adoptees and twins.
- Mani, S, 2014. Socioeconomic determinants of child health: Empirical evidence from Indonesia. Asian Economic Journal 28(1), 81–104. doi: 10.1111/asej.12026
- Medrano, P, Rodríguez, C & Villa, E, 2008. Does mother’s education matter in child’s health? Evidence from South Africa. South African Journal of Economics 76(4), 612–627. doi: 10.1111/j.1813-6982.2008.00210.x
- Rawlings, SB, 2015. Parental education and child health: Evidence from an education reform in China. CINCH Working Paper 2015/11.
- Salm, M & Schunk, D, 2008. The role of childhood health for the intergenerational transmission of human capital: Evidence from administrative data. IZA. 39 p. ZA Discussion Paper; no. 3646.
- Shisana, O, Labadarios, D, Rehle, T, Simbayi, L, Zuma, K, Dhansay, A, Reddy, P, Parker, W, Hoosain, E, Naidoo, P, & Hongoro, C, 2014. The South African national health and nutrition examination survey, 2012: SANHANES-1: The health and nutritional status of the nation. HSRC Press, Pretoria.
- Southern Africa Labour and Development Research Unit. National Income Dynamics Study, 2008. Wave 1 [dataset]. Version 6.1. Cape Town: Southern Africa Labour and Development Research Unit [producer], 2016. Cape Town: DataFirst [distributor], 2016.
- Southern Africa Labour and Development Research Unit. National Income Dynamics Study, 2010–2011. Wave 2 [dataset]. Version 3.1. Cape Town: Southern Africa Labour and Development Research Unit [producer], 2016. Cape Town: DataFirst [distributor], 2016.
- Southern Africa Labour and Development Research Unit. National Income Dynamics Study, 2012. Wave 3 [dataset]. Version 2.1. Cape Town: Southern Africa Labour and Development Research Unit [producer], 2016. Cape Town: DataFirst [distributor], 2016.
- Southern Africa Labour and Development Research Unit. National Income Dynamics Study, 2014–2015. Wave 4 [dataset]. Version 1.1. Cape Town: Southern Africa Labour and Development Research Unit [producer], 2016. Cape Town: DataFirst [distributor], 2016. Pretoria: Department of Planning Monitoring and Evaluation [commissioner], 2014.
- Statistics, SA, 2013. Quarterly labour force survey, 3rd quarter. Statistics SA, Pretoria.
- Statistics, SA, 2015. Employment, unemployment, skills and economic growth: An exploration of household survey evidence on skills development and unemployment between 1994 and 2014.
- Strauss, J & Thomas, D, 1998. Health, nutrition, and economic development. Journal of Economic Literature 36(2), 766–817.
- Thomas, D, Strauss, J & Henriques, MH, 1991. How does mother's education affect child height? Journal of Human Resources, 26, 183–211. doi: 10.2307/145920
- UNESCO (United Nations Educational, Scientific and Cultural Organization), 2006. EFA global monitoring report. Strong foundations: Early childhood care and education. UNESCO, Paris.
- Visser, G, 2013. Looking beyond the urban poor in South Africa: The new terra incognita for urban geography? Canadian Journal of African Studies/La Revue Canadienne Des études Africaines 47(1), 75–93. doi: 10.1080/00083968.2013.770593
- Woolard, I, 2002. An overview of poverty and inequality in South Africa. Unpublished briefing paper. HSRC, Pretoria.
- Wooldridge, J, 2002. Econometric analysis of cross section and panel data. The MIT Press, Cambridge, MA.
- WHO (World Health Organization), 2006. WHO child growth standards: Length/height for age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age, methods and development. World Health Organization.
- World Health Organization and Unicef, 2009. WHO: Multicentre growth reference study group. WHO child growth standards: Length/Height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. WHO, Geneva.
- Zhao, S, 2008. Application of human capital theory in China in the context of the knowledge economy. The International Journal of Human Resource Management 19(5), 802–817. doi: 10.1080/09585190801991145