
ABSTRACT
Zambia has made improvements in addressing maternal and child health in the past two decades. The COVID-19 pandemic outbreak, which could put a strain on the healthcare systems and alter how access to sexual and reproductive health services is provided, could, however, have a negative impact on the gains. Data from a recent nationally representative COVID-19 survey, conducted in April 2021, was used to examine the utilisation of antenatal care services among pregnant women during the pandemic in Zambia. Overall, 10 per cent (95% CI: 8.0–11.4) of pregnant women missed antenatal care during the COVID-19 period, signifying an increase when compared to the time before the outbreak of COVID-19. Age of a woman and level of education were associated with the risk of missing antenatal care services. The study highlights the need to improve communication to women on availability and access to sexual reproductive health services to stimulate demand and use among women during this period.
1. Introduction
Zambia has made progress in improving sexual and reproductive health (SRH) outcomes in the past two decades, especially in reducing maternal mortality, child mortality and morbidity, and increasing modern contraceptive use. Pregnancy-related mortality ratio reduced from 729 in 2001 to 278 in 2018 (Zambia Statistics Agency, Ministry of Health (MOH) Zambia, and ICF, Citation2019). Many studies have been conducted in Zambia to examine associations between women’s socio-economic and demographic factors and utilisation of different sexual and reproductive health services (Chola et al., Citation2020; Lasong et al., Citation2020; Namukoko et al., Citation2022; Nduku & Simo-Kengne, Citation2022; Simona et al., Citation2022; Phiri et al., Citation2023). These studies found that women who are older, educated, those who live in urban areas, working class or belong to rich households, were more likely to utilise SRH services. However, it is not clear whether these findings would be similar, with the on-going fear of COVID-19 pandemic, which has the potential to threaten maternal and child health care, antenatal care attendance, including facility deliveries especially in SSA counties, Zambia inclusive (Feyissa et al., Citation2020; Pfitzer et al., Citation2020; Riley et al., Citation2020). The COVID-19 pandemic has altered people’s lives not only in Zambia but also in other SSA countries. Work at home, social separation, disruption of health service delivery and fear of infection at health facility have the potential to change health-seeking behaviours of the population (Feyissa et al., Citation2020; Hashem et al., Citation2021; Kumar et al., Citation2021; Mudenda et al., Citation2022).
In Zambia, just like in many other SSA countries, the COVID-19 pandemic has put a strain on health systems and changed the landscape on access to general health as well as sexual and reproductive health service provision, including contraceptive use, antenatal care, postnatal care and sexual behaviour (Saasa & James, Citation2020; United Nations Zambia, Citation2020; Mallah et al., Citation2021; Mudenda et al., Citation2022; Ncheka et al., Citation2023). The impact of COVID-19 on the provision of sexual and reproductive health services can have direct maternal health effects such as prevention of unplanned pregnancies, unsafe abortions, obstetric complications without care, maternal deaths and newborn deaths (Kumar et al., Citation2021; Mallah et al., Citation2021). The disruption in supply of contraception methods in public facilities may compel women of reproductive age to use traditional methods such as herbs, withdrawal and lactational amenorrhea method that have proved to be ineffective in the past (Kumar et al., Citation2021; Mallah et al., Citation2021).
Since the onset of COVID-19 pandemic in Zambia and other parts of SSA, there has been limited information in the literature to understand of how various socio-demographic factors, such as maternal age, socioeconomic status, education level, marital status and access to healthcare facilities influence women's utilisation of antenatal care services during the COVID-19 period. This has been partly due to lack on national level data to adequately measure the impact on COVID-19 pandemic on SRH service utilisation While a few studies have explored the overall impact of the pandemic on healthcare utilisation in the context of SSA (Adelekan et al., Citation2020; Ferreira-Filho et al., Citation2020; Feyissa et al., Citation2020; Hashem et al., Citation2021), These studied have not specifically investigated its effects on pregnant women seeking antenatal services. Moreover, the majority of the existing research has focused on examining effect COVID-19 restrictions on general health care access in high-income countries were data is available, neglecting the experiences and challenges faced by women in low-income countries like Zambia. Therefore, it is important to have a comprehensive understanding of how the COVID-19 pandemic affected utilisation of SRH services among women of reproductive age in Zambia, in order to generate evidence to inform strengthening of SRH programming in the country amid the pandemic crisis.
Zambia as part of the countries in SSA which was heavily impacted by COVID-19 has been implementing various health measures to mitigate the effects of the pandemic on the population (Ministry of Health Zambia, Citation2020; Mallah et al., Citation2021). Zambia, like other countries in the region, developed the COVID-19 multi-sectoral response plan to address both preventive treatment and management of the pandemic. These measures included adequate provision of family planning services and commodities, especially to the vulnerable groups, such as pregnant women (Ministry of Health Zambia, Citation2020; United Nations Zambia, Citation2020). Improving access to and utilisation of maternal health services among women of reproductive age, especially during the pandemic period, is key in meeting their reproductive health needs to limit and space child-bearing (Fabic et al., Citation2015; Ferreira-Filho et al., Citation2020; Mallah et al., Citation2021)
Theoretically, the use of maternal health care services during the COVID-19 pandemic can be well understood within the underpinning of the Health Belief Model (HBM). HBM is one of the early models in the field of health behaviour. The model was created in the 1950s by social psychologists Irwin M. Rosenstock and colleagues (Jones et al., Citation2015). It is a theoretical framework that helps explain and predict health-related behaviours of a population or a group of people. It was initially developed to determine the reasons why people shunned public health screening initiatives. According to the HBM, a person's decision regarding his or her health behaviour is influenced by ones beliefs regarding their susceptibility to illness, the severity of the illness, the advantages of taking action, and the obstacles to action (Rosenthal et al., Citation1992; Zhao et al., Citation2012; Jones et al., Citation2015). This model therefore, provides explanation of the likelihood of using reproductive health services among women from the point of perceived benefits (Rosenthal et al., Citation1992; Azfredrick, Citation2016).
In Zambia, the COVID-19 pandemic has posed significant challenges to the utilisation of maternal health care services such as antenatal services, post-natal and family planning services (Ministry of Health Zambia, Citation2020; Mudenda et al., Citation2022). Therefore, analyzing this problem through the lens of the health behaviour models can provide useful insights for improving maternal health programme. The Health Belief Model, for instance, emphasises how perceived susceptibility to the COVID-19 virus and the severity of its consequences can impact pregnant women's decision-making process on whether to attend antenatal care or not. Also, fear of contracting the virus at the healthcare facilities and concerns about potential exposure to infected individuals during ANC visits may contribute to reduced utilisation rates among women. It is crucial to understand these dynamics within the context of health behaviour models in order to develop focused interventions that will address the issues and ensure that use of antenatal services during the COVID-19 period is not negatively affected.
Therefore, examining micro-level national data would be essential in providing a holistic picture of the impact of COVID-19 on sexual and reproductive health behaviour among women of reproductive age, as well as identifying the determinants of health-seeking behaviour in Zambia. Due to lack of national level micro-data in most countries in SSA regarding COVID-19 and sexual reproductive health service utilisation, it is not yet clear what individual and household level factors are influencing women’s access and utilisation of SRH care services during the COVID-19 period in SSA and Zambia in particular. Evidence from this current analysis would be useful to support generation of information to guide SRH programming and implementation in the country during the pandemic period in order to ensure that maternal health care services are adequately utilised.
Thus, the aim of this study was to assess the individual-level factors associated with non-utilisation of antenatal care services among women of reproductive age in Zambia during the COVID-19 period. The study purpose was accomplished by making use of the national representative data collected in 2021 to assess the socio-economic impact of COVID-19 on the Zambian population. The COVID-19 Socio-economic Impact Assessment (SEIA) survey collected data on access and utilisation of health services during the COVID-19 period among women of child-bearing age (15–49) during.
2. Methods and data
2.1. Data source
The study used data extracted from the 2021 Socio-economic Impact Assessment (SEIA) survey conducted in Zambia. Data were collected with the reference period 1st March 2020 to 30th April 2021. The SEIA survey drew a nationally representative sample of households selected via a two-stage stratified cluster sampling technique. The survey collected data on family planning utilisation from women aged 15–49 during the COVID-19 period. Interviews were conducted using two main questionnaires, namely, household questionnaire and individual questionnaire. The individual questionnaire included a section which captured indicators on family planning and sexual reproductive health. For our study investigation, we analysed data from the individual respondent data file, which contained all information related to women of reproductive age. This data was data collected using the individual questionnaire. Data were collected by trained field workers who were well-versed in a wide range of topics covered by the survey. A detailed explanation of the methodology is provided in the survey report (Zambia Statistics Agency, Citation2021). Furthermore, data from the DHS 2007–18 was used to compare the prevalence of antenatal care service utilisation among women before and during the COVID-19 period.
2.2. Study sample
The analysis sample for this study comprised women of child-bearing, aged 15–49 years, extracted from the COVID-19 socio-economic impact assessment survey. The survey employed a two-stage stratified cluster sample design. In the first stage, 419 Enumeration Areas (EAs) were selected and in the second stage, systematic sampling was used to select 25 households from each enumeration area (EA) to arrive at 10,490 households. All persons, 10 years and older, in the selected households (usual household members) or visitors who spent a night with the household, were eligible for an individual interview (Zambia Statistics Agency, Citation2021). For this study, a total sample of 11,055 women of reproductive age (15–49 years) were considered to analyse the prevalence of sexual and reproductive health outcomes. Furthermore, the analysis of antenatal care service utilisation was restricted to women who were pregnant during the COVID-19 period (n = 1,523). This is because these women were in need of antenatal services during the period. Therefore, all non-pregnant women were excluded in the multivariate regression model. The SEIA survey had two main questionnaires, namely; household and individual questionnaires.
3. Measures
3.1. Outcome variables
The outcome variables of interest in this study were; (i) antenatal care (ANC) (ii) HIV treatment access and (iii) postnatal care (PNC) service utilisation during COVID-19 period. The SEIA defined these outcome indicators in line with the World Health Organisation’s guidelines, and therefore data was collected to measure estimates that would inform health policy and programmes to address the impact of COVID-19 in the country. The COVID-19 socio-economic impact assessment survey collected information on access and utilisation of sexual reproductive services among women of reproductive age (15–49) during the COVID-19 period in Zambia. Each outcome variable was classified as binary outcome; HIV treatment access (‘0’ representing no access and ‘1’ representing access); Antenatal visit was coded as (‘0’ representing did not miss an antenatal visit and ‘1’ representing missed an antenatal) and Postnatal access (‘0’ representing did not miss postnatal care and ‘1’ representing missed postnatal care). All the outcome variables were selected based on prior review of literature.
3.2. Independent variables
Based on literature review, we identified individual level predictors that might be associated with family planning utilisation among women in the reproductive age during the COVID-19 period. We classified these variables as socio-economic and demographic factors, and underlying health conditions. The COVID-19 survey questionnaires and data dictionary were used to identify the independent variables. The main independent variables included in this study were: age of a woman (15–24, 25–34, and 35–49 years); residence (urban, rural); province (central, Copperbelt, Eastern, Lusaka, Luapula, Muchinga, Northern, North-western, Southern and Western); employment status (employed, unemployed); marital status (never married, married, formerly married); education level (none, primary, secondary, tertiary); knowledge of COVID-19 preventive measures (yes, no); perceived knowledge of COVID-19 treatment options (yes, no); having any medical condition such as diabetes or HIV or hypertension (yes, no).
3.3. Statistical analysis
Statistical software Stata SE version 17.0 was used to perform weighted analysis, which considered the complex survey design. We performed the descriptive analysis to summarise study samples and outcome indicators. Categorical variables were presented using frequencies and percentages. Bivariate analysis was conducted to explore the association between explanatory variables and the outcome variable ‘antenatal care service utilisation’. Furthermore, we conducted a binary multivariate logistic regression to examine the determinants of utilisation antenatal care services among pregnant women during the COVID-19 period in Zambia. The choice of the analysis model was informed by the binomial distribution of the outcome variable for the study. The analysis allowed for all explanatory variables to be entered into the model to get adjusted odds ratios. The adjusted odds ratios (AOR) were calculated, along with their respective 95 per cent confidence intervals (95% CI). The ‘svy’ command in Stata software allowed for correction of under and over sampling and complex survey design.
4. Results
4.1. Description of women captured in the COVID-19 socio-economic impact assessment survey
shows the description of background characteristics of women (aged 15–49 yeas), who were included in the study analysis. The study included 11,055 women of reproductive age; of these, 1,523 were pregnant during the COVID-19 pandemic period. The mean age for the respondents was 28 years. There were more women in the age group 15–24 (41.3%) than in the older age groups. Slightly more than half (50.4%) of the respondents were residing in rural areas at the time of the survey. A larger proportion of women had attained secondary level of education. Majority of women captured in the survey were not working. Knowledge of COVID-19 was universal. However, most indicated they did not know the COVID-19 prevention measures. Similarly, majority of women (52.6%) had no knowledge of COVID-19 prevention measures.
Table 1. Percent distribution of women (15--49 years) who utilised SRH services or were pregnant by selected background characteristics, COVID-19 SEIA, 2021, Zambia.
4.2. Prevalence of sexual and reproductive health outcomes during COVID-19 period
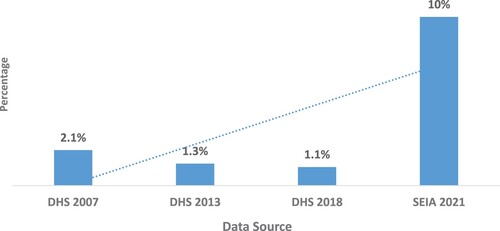
shows that the prevalence of sexual reproductive health outcomes measured by the survey. Results show that 19 per cent of women who gave birth during the COVID-19 period missed postnatal care services while 10 per cent of the pregnant women missed antenatal care services. Four per cent of women indicated that they were unable to access HIV treatment during the same period (). Trend results show that the percentage of pregnant women who missed antenatal care increased during the COVID-19 period. The study shows that there is a significant increase in the percentage of women who missed antenatal care services from 1.1 per cent as captured in 2018 DHS to 10 per cent in 2021 (). The observed increase in the proportion women who missed antenatal care services could, to some extent, be explained by women’s fear of contracting COVID-19 virus at the health facility.
Figure 1. Prevalence of sexual reproductive health outcomes in Zambia during COVID-19 period.
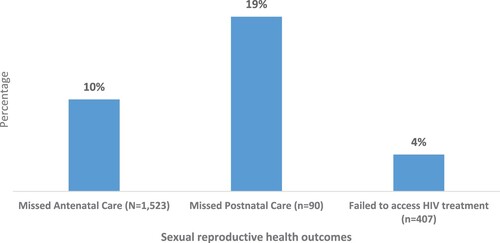
Figure 2. Trends in prevalence of women who missed antenatal care visits before and during COVID-19 period in Zambia (2007–21).
4.3. Antenatal care utilisation and women’s background characteristic during the COVID-19 period
shows the percentage distribution of pregnant women who missed antenatal cares services by background characteristics. Bivariate analysis reveals that some background factors were associated with women’s utilisation of antenatal care services during COVID-19 period (p < 0.01) in Zambia. Young women in the age group 15–24 years had highest percentage of those who missed antenatal care services during the COVID-19 period, and those in the age group 35–49 years had the lowest proportion. Findings also reveal that there was a relationship between level of education and antennal care utilisation during the COVID-19 period. Women with no formal education and those with primary education had a higher chance of missing antenatal care services.
Table 2. COVID-19 and sexual reproductive health.
Our study found that women who reported to have knowledge of COVID-19 treatment options had a higher chance of missing antenatal care services compared to those who had no knowledge (13.5% versus 7.5%; p < 0.01). Residence, marital status and employment status were found not to be associated with chance of missing antenatal care service.
4.4. Determinants of antenatal care service utilisation during COVID-19 period
Multivariate binary logistic regression was used to examine the influence of individual level and health factors that determine utilisation of sexual reproductive health services among women of reproductive age during the COVID-19 period in Zambia. When we controlled for the covariates in the full multivariate model, we observed that age of a woman, education, province and perceived knowledge of COVID-19 treatment options influenced utilisation of antenatal care services during the COVID-19 period in Zambia. Age of a woman was positively associated with the risk of missing antenatal care services among pregnant women. Pregnant women in the older age groups (25–34 years and 35–49 years) had lower odds of missing antenatal care services; (AOR: 0.55; 95% CI: 0.31–0.99) and (AOR: 0.54; 95% CI: 0.24–1.23), respectively. But the odds for the age group 35–49 years were not significantly different from the odds of those aged 15–24 years.
In terms of education level, it was noted that an increase in level of education was associated with reduced chance of missing antenatal care services among pregnant women. Women with secondary or tertiary level of education had odds of (AOR: 0.62; 95% CI: 0.28–1.38) and (AOR: 0.17; 95% CI: 0.03–0.94), respectively. Furthermore, an association between perceived knowledge of COVID-19 treatment options and antenatal care utilisation was observed, with women who had knowledge of COVID-19 treatment options, being 6% less likely to miss antenatal care services than those with no knowledge of treatment options. Regional variations were observed in terms utilisation of antenatal care during COVID-19 period in Zambia. Women who were living on the Copperbelt province (AOR: 0.62; 95% CI: 0.28–1.38), Luapula province (AOR: 0.62; 95% CI: 0.28–1.38) and Western province were less likely to miss ANC compared to women who were living in Lusaka. Marital status, place of residence, employment status, knowledge of COVID-19 prevention measures and having a medical condition were not associated with a risk of missing antenatal cares services ().
Table 3. Multivariate logistic regression analysis examining risk of missing antenatal care during the COVID-19 period among women of reproductive age, SEIA 2021, Zambia.
5. Discussion
For over four decades, increasing access to sexual reproductive health and other family planning services has been a major global goal of health and development programming (Alkema et al., Citation2013; Fabic et al., Citation2015; Blackwell et al., Citation2020; Kantorová et al., Citation2021). Since then, significant progress has been made in reducing unmet family planning needs, increasing contraceptive prevalence, and preventing unintended pregnancies (Cleland et al., Citation2014; Bongaarts & Hardee, Citation2019). In recent decades, the rate of progress has, however, slowed down or stalled, particularly in some countries in SSA (Fabic et al., Citation2015; May, Citation2017; Bongaarts & Hardee, Citation2019). However, the gains made in improving sexual reproductive health in SSA may be offset by further disruption of provision and access to SRH due to emerging COVID-19 variants.
Using cross-sectional data from the COVID-19 socio-economic impact assessment survey conducted in Zambia in 2021, this study sought to analyse the influence of the COVID-19 pandemic on utilisation of sexual reproductive health services in Zambia. The study has demonstrated that COVID-19 has affected utilisation of sexual reproductive and maternal health care services in Zambia. This finding is consistent with similar studies conducted in Ethiopia and United States of America, which also reported a decline in access to family planning and sexual reproductive health services (Feyissa et al., Citation2020; Lindberg et al., Citation2020; Tadesse, Citation2020; Gleason et al., Citation2021; Kassie et al., Citation2021). This study focused on the influence of socio-demographic as well as health factors on and utilisation of reproductive health services. Another study conducted in Burkina Faso and Kenya in 2020 found that 14 percent and 4 per cent of women who were not using contraception in Kenya and Burkina Faso, respectively, reported COVID-19 related reasons for non-use (Karp et al., Citation2021), highlighting the significance of establishing secure sexual reproductive health service delivery methods when health crises occur. Adelekan et al. (Citation2020) found that demand-driven usage trends for family planning services decreased in the two months prior to the COVID-19 outbreak and further decreased during the lockdown in Gauteng province of South Africa (Adelekan et al., Citation2020). Furthermore, in Sierra Leone, Sevalie et al. (Citation2021) found a reduction in the use of health services during the COVID-19 period.
The literature review reveals that there is little evidence of understanding the factors associated with sexual reproductive health outcomes during the COVID-19 pandemic in Zambia. Thus, analysis done in this study bolsters the importance of our findings to inform public health and sexual reproductive policy and programming during the COVID-19 era.
The study found that age, education and knowledge of COVID-19 treatment options were important factors associated with utilisation of antenatal cares services among pregnant women in Zambia. Additionally, this study has revealed that residence, marital status, employment status, knowledge of COVID-19 prevention measures, and having a medical condition (diabetic status, hypertension status and HIV status) had no effect on influencing utilisation of sexual reproductive health services in women. One of the probable reasons that could have led to some women missing antenatal care, was fear of COVID-19 infections at a health facility.
Our study further showed that the odds of missing antenatal services among pregnant women, was lower among those in the age groups 25–34 and 35–49 years. This suggests that a woman’s age plays a significant role in determining the extent of sexual reproductive health service utilisation in times of the pandemic. The study further found that a woman’s age was negatively associated with use of sexual reproductive health services, implying that older woman had lower risk of missing antenatal care services. This study finding resonates with findings of a previous study conducted in Ethiopia which reported that older women were more likely to attend antenatal care during the COVID-19 pandemic period (Tadesse, Citation2020). Utilisation of antenatal care services was lower among young pregnant women, probably because some of these young women might had less knowledge about the important of accessing maternal health services, while others might not have been aware that maternal health services were provided by health facilities even during the COVID-19 period.
This study results also showed significant association between level of education and utilisation of sexual reproductive health service (antennal care) among pregnant women in Zambia. A similar finding was reported in a previous study (Tadesse, Citation2020). This finding suggests the need for women to prioritise access to education in order for them to fully appreciate the importance of accessing maternal health care services even during the COVID-19 pandemic period. Furthermore, women who had knowledge of COVID-19 treatment options had lower odds of missing antenatal care services. This finding signifies the importance of knowledge in determining health-seeking behaviour among women of reproductive age. Meeting the sexual and reproductive health needs of women of reproductive age during the COVID-19 pandemic period, has a potential to reduce further unwanted pregnancies, abortions as well as avoid child and maternal deaths. Continuing to track family planning health-seeking behaviour throughout the pandemic period will create an opportunity to identify trends and factors that will inform targeted public health interventions.
This study utilised the Health Behaviour Model to explain why some women missed antenatal care visits during the COVID-19 period in Zambia. This theory proposes that people are more inclined to engage in health-promoting actions if they believe the benefits of taking the action outweigh the difficulties or expenses associated with the action. The model assumes that individuals make rational decisions through education or communication.
In this regard, women who understand importance of attending antenatal care service as a way of monitoring pregnancy growth and early detection of pregnancy complications, are more likely to attend antenatal care (ANC) regardless of current health systems challenges, such as restrictions caused by the COVID-19 pandemic in Zambia. However, due the fear of contracting the COVID-19 virus or lack of knowledge that maternal health services were still offered during the COVID-19 restriction, some women were expected to fail to attend ANC in Zambia, despite the benefits associated with it. The findings of this showed that women who had higher education were less likely to miss ANC during the pandemic compared to those with no education. This finding affirms the assumption of the HBM that women higher education understands the benefits of ANC and therefore, they made a decision to utilise the service despite the risk of contracting the COVID-19 virus at the health facility. Furthermore, the showed that women with perceived knowledge of how to treat COVID-19 were less likely to miss ANC visits because of they could be able to adopt preventive measure when visiting the health facilities to access ANC services.
The findings of this study have significant implications for theoretical understanding of the factors associated antenatal care utilisation among pregnant women during the COVID-19 period in Zambia. Furthermore, the findings draw the attention to the potential disruptions and difficulties pregnant women encountered in accessing maternal health services during the pandemic period in Zambia. Our findings have also helped to identify vulnerable women groups that need targeted supported during the period of the pandemic to ensure their maternal health needs are met in time of crises to protect the health of both the mother and the unborn child. Thus, the evidence generated by this study will guide health policymakers in designing health policies and interventions that address the unique health care needs and concerns of pregnant women during public health emergencies may occur in the future.
Even though the full impact of the COVID-19 pandemic on women’s sexual and reproductive health experiences is not yet not fully assessed in Zambia, this study provides a snapshot of the effects of the COVID-19 pandemic on sexual and reproductive health (SRH) outcomes and family planning health-seeking behaviour among women of reproductive age (15–49) in Zambia. The prevalence of women who missed antenatal care visits, postnatal services as well as those who failed to access HIV treatment during the COVID-19 period March 2020 to April 2021 is of worrying concern for improving maternal health care in the country. The observed increased prevalence of women missing antenatal health service and postnatal health care in Zambia, could be due to lack of knowledge that sexual reproductive health and family planning services were being provided during the partial lockdown which was experienced in the country. The other reasons could be fear of contracting the COVID-19 virus from heath facility or inability to access service due to disruption in provision of the service at a health facility.
Literature shows that 60 per cent more maternal fatalities could occur if maternal health care coverage was reduced by 10–50 per cent (Riley et al., Citation2020; Murewanhema & Madziyire, Citation2021). For example, due to the disruption of health care for pregnant women and newborns, Ebola-related direct mortality in Sierra Leone ended up being roughly equal to indirect cause of mortality (Elston et al., Citation2017). The findings reported in this study, have implications both for shaping sexual and reproductive health policy, and for strengthening family planning communication initiatives, to avert future consequences of the COVID-19 on maternal health in the country.
6. Conclusion
This study has shown that the COVID-19 pandemic has affected the utilisation of sexual reproductive health services among women of reproductive age in Zambia. This was evidenced by the observed increase in the proportion of pregnant women who missed antenatal care visits during the COVID-19 period, compared to the period before the pandemic. Fear of COVID-19 infection at a health facility could be one of the reasons that might have led to some women missing antenatal care services. The study also established that while some women missed postnatal care services, others were also unable to access HIV treatment during the same period. Depending on the severity of future waves, the pandemic may have a greater impact on the provision and accessibility of sexual and reproductive health services among different population groups. Thus, policy-makers should strive to ensure that universal access to SRH services during the pandemic era will be key in meeting the SRH needs of women. While paying attention to managing of the pandemic is key, policy-makers should also ensure that the health care systems meet SRH needs of women. Future research should further explore whether sexual reproductive health-seeking behaviour use during the COVID-19 era differs in relation to certain socio-demographics such as household income status, parity and cultural values in SSA countries. It is hoped that soon, data will be widely available world over, to assess in more detail, the effects of COVID-19 on sexual and reproductive health outcomes.
7. Study strengths and limitations
There are a number of limitations to be considered in this study. First, the cross-sectional nature of the study restricts causal inferences to be drawn. Second, participants’ responses could have been influenced by recall bias because they were asked to report their sexual reproductive health and health-seeking behaviour in the 12 months prior to the survey, rather than in the current year. Third, some important outcomes and independent variables such as number of children a woman has, religion, sexual activity and household income status were missing in the dataset. This made it difficult to conduct a conclusive analysis of the effects of COVID-19 on sexual reproductive health-seeking behaviour during the pandemic in Zambia. Despite the limitations, this is the first study to examine in detail the influence of the COVID-19 on sexual reproductive outcomes in Zambia. The study will thus, inform SRH programming during the pandemic in order to address the adverse effects of pandemic has on women’s health.
Consent for publication
Not applicable.
Competing interests
Authors declare no competing interest.
Author contributions
MP developed the concept for this study and wrote the background section. MP and SS performed data analysis and wrote the discussion and data interpretation text for the manuscript. HN prepared the methodology. CO performed overall review and editing of the manuscript for intellectual content. All authors have read and approved the final version of this manuscript.
Availability of data and materials
Data used this study are available upon request from Zambia Statistics Agency (https://www.zamstats.gov.zm/). Data analysis files can be provided upon request to the corresponding author ([email protected])
Acknowledgments
This work was carried out under the COVID-19 Africa Rapid grant Fund supported under the auspices of the Science Granting Councils Initiative in Sub-Saharan Africa (SGCI) and administered by South Africa’s National Research Foundation in collaboration with Canada’s International Development Research Center (IDRC), THE Swedish International Development Cooperation Agency (Sida), South Africa’s Department of Science and Innovation (DSI), the Fons de Recherche due Quebec (FRQ), the United Kingdom’s Department of International Development (DFID), United Kingdom Research and Innovation (UKRI) through the Newton Fund, and the SGCI participating councils across 15 countries in sub-Saharan Africa. It is made possible by the Demography and Population Studies Programme of the University of the Witwatersrand, South Africa through its conference on population and reproductive health dynamics under Covid-19 in Sub-Saharan Africa.
Authors would also like to express their gratitude to the Zambia Statistics Agency for authorising the use of the 2021 COVID-19 Socio-economic Impact Assessment Survey datasets and for providing the researchers with the survey report.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Adelekan, T, Mihretu, B, Mapanga, W, Nqeketo, S, Chauke, L, Dwane, Z & Baldwin, RL, 2020. Early effects of the COVID-19 pandemic on family planning utilisation and termination of pregnancy services in gauteng, South Africa: March–April 2020. Wits Journal of Clinical Medicine 2(2), 145–52. doi:10.18772/26180197.2020.v2n2a7
- Alkema, L, Kantorova, V, Menozzi, C & Biddlecom, A, 2013. National, regional, and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: A systematic and comprehensive analysis. The Lancet 381(9878), 1642–52. doi:10.1016/S0140-6736(12)62204-1
- Azfredrick, EC, 2016. Using Anderson’s model of health service utilization to examine use of services by adolescent girls in south-eastern Nigeria. International Journal of Adolescence and Youth 21(4), 523–9. doi:10.1080/02673843.2015.1124790
- Blackwell, S, Louis, JM, Norton, ME, Lappen, JR, Pettker, CM, Kaimal, A, Landy, U, Edelman, A, Teal, S & Landis, R, 2020. Reproductive services for women at high risk for maternal mortality: A report of the workshop of the society for maternal-fetal medicine, the American college of obstetricians and gynecologists, the fellowship in family planning, and the society of family planning. American Journal of Obstetrics & Gynecology 222(4), B2–B18. doi:10.1016/j.ajog.2019.12.008
- Bongaarts, J & Hardee, K, 2019. Trends in contraceptive prevalence in Sub-saharan Africa: The roles of family planning programs and education. African Journal of Reproductive Health 23(3), 96–105.
- Chola, M, Hlongwana, K & Ginindza, TG, 2020. Patterns, trends, and factors associated with contraceptive use among adolescent girls in Zambia (1996 to 2014): A multilevel analysis. BMC Women’s Health 20(1), 185. doi:10.1186/s12905-020-01050-1
- Cleland, J, Harbison, S & Shah, IH, 2014. Unmet need for contraception: Issues and challenges. Studies in Family Planning 45(2), 105–22.
- Elston, JW, Cartwright, C, Ndumbi, P & Wright, J, 2017. The health impact of the 2014–15 Ebola outbreak. Public Health 143, 60–70.
- Fabic, MS, Choi, Y, Bongaarts, J, Darroch, JE, Ross, JA, Stover, J, Tsui, AO, Upadhyay, J & Starbird, E, 2015. Meeting demand for family planning within a generation: The post-2015 agenda. The Lancet 385(9981), 1928–31. doi:10.1016/S0140-6736(14)61055-2
- Ferreira-Filho, ES, de Melo, NR, Sorpreso, ICE, Bahamondes, L, Simões, RDS, Soares-Júnior, JM & Baracat, EC, 2020. Contraception and reproductive planning during the COVID-19 pandemic. Expert Review of Clinical Pharmacology 13(6), 615–22. doi:10.1080/17512433.2020.1782738
- Feyissa, GT, Tolu, LB & Ezeh, A, 2020. Impact of COVID-19 pandemic on sexual and reproductive health and mitigation measures: The case of Ethiopia. African Journal of Reproductive Health 24(2), 4.
- Gleason, N, Banik, S, Braverman, J & Coleman, E, 2021. The impact of the COVID-19 pandemic on sexual behaviors: findings from a national survey in the United States. The Journal of Sexual Medicine 18(11), 1851–62. doi:10.1016/j.jsxm.2021.08.008
- Hashem, NM, Abdelnour, SA, Alhimaidi, AR & Swelum, AA, 2021. Potential impacts of COVID-19 on reproductive health: scientific findings and social dimension. Saudi Journal of Biological Sciences 28(3), 1702–12. doi:10.1016/j.sjbs.2020.12.012
- Jones, CL, Jensen, JD, Scherr, CL, Brown, NR, Christy, K & Weaver, J, 2015. The health belief model as an explanatory framework in communication research: Exploring parallel, serial, and moderated mediation. Health Communication 30(6), 566–76. doi:10.1080/10410236.2013.873363
- Kantorová, V, Wheldon, MC, Dasgupta, ANZ, Ueffing, P & Castanheira, HC, 2021. Contraceptive use and needs among adolescent women aged 15–19: Regional and global estimates and projections from 1990 to 2030 from a Bayesian hierarchical modelling study. PLOS ONE 16(3), e0247479. doi:10.1371/journal.pone.0247479
- Karp, C, Wood, SN, Guiella, G, Gichangi, P, Bell, SO, Anglewicz, P, Larson, E, Zimmerman, L & Moreau, C, 2021. Contraceptive dynamics during COVID-19 in sub-saharan Africa: Longitudinal evidence from Burkina Faso and Kenya. BMJ Sexual & Reproductive Health 47(4), 252–60. doi:10.1136/bmjsrh-2020-200944
- Kassie, A, Wale, A & Yismaw, W, 2021. Impact of coronavirus diseases-2019 (COVID-19) on utilization and outcome of reproductive, maternal, and newborn health services at governmental health facilities in south west Ethiopia, 2020: Comparative cross-sectional study. International Journal of Women’s Health 13, 479–88. doi:10.2147/IJWH.S309096
- Kumar, N, Janmohamed, K, Nyhan, K, Forastiere, L, Zhang, W-H, Kågesten, A, Uhlich, M, Sarpong Frimpong, A, Van de Velde, S, Francis, JM, Erausquin, JT, Larrson, E, Callander, D, Scott, J, Minichiello, V & Tucker, J, 2021. Sexual health (excluding reproductive health, intimate partner violence and gender-based violence) and COVID-19: A scoping review. Sexually Transmitted Infections 97(6), 402–10. doi:10.1136/sextrans-2020-054896
- Lasong, J, Zhang, Y, Gebremedhin, SA, Opoku, S, Abaidoo, CS, Mkandawire, T, Zhao, K & Zhang, H, 2020. Determinants of modern contraceptive use among married women of reproductive age: A cross-sectional study in rural Zambia. BMJ Open 10(3), e030980. doi:10.1136/bmjopen-2019-030980
- Lindberg, LD, VandeVusse, A, Mueller, J & Kirstein, M, 2020. Early impacts of the COVID-19 pandemic: Findings from the 2020 guttmacher survey of reproductive health experiences. Guttmacher Institute. doi:10.1363/2020.31482.
- Mallah, SI, Ghorab, OK, Al-Salmi, S, Abdellatif, OS, Tharmaratnam, T, Iskandar, MA, Sefen, JAN, Sidhu, P, Atallah, B, El-Lababidi, R & Al-Qahtani, M, 2021. COVID-19: Breaking down a global health crisis. Annals of Clinical Microbiology and Antimicrobials 20(1), 35. doi:10.1186/s12941-021-00438-7
- May, JF, 2017. The politics of family planning policies and programs in sub-saharan Africa. Population and Development Review 43, 308–29.
- Ministry of Health Zambia, 2020. Environmentl and Social Committment Plan (ESCP) for COVID-19 emergency response projects [Strategy]. Ministry of Health. https://www.moh.gov.zm/?wpfb_dl = 148.
- Mudenda, S, Chileshe, M, Mukosha, M, Hikaambo, CN, Banda, M, Kampamba, M, Mwila, K, Banda, DC, Mufwambi, W & Daka, V, 2022. Zambia’s response to the COVID-19 pandemic: Exploring lessons, challenges and implications for future policies and strategies. Pharmacology & Pharmacy 13(1), Article 1, 11–33. doi:10.4236/pp.2022.131002
- Murewanhema, G & Madziyire, MG, 2021. COVID-19 restrictive control measures and maternal, sexual and reproductive health issues: Risk of a double tragedy for women in sub-Saharan Africa. The Pan African Medical Journal 40, 122. doi:10.11604/pamj.2021.40.122.27946
- Namukoko, H, Likwa, RN, Hamoonga, TE & Phiri, M, 2022. Unmet need for family planning among married women in Zambia: Lessons from the 2018 demographic and health survey. BMC Women’s Health 22(1), 137. doi:10.1186/s12905-022-01709-x
- Ncheka, JM, Menon, JA, Davies, EB, Paul, R, Mwaba, SOC, Mudenda, J, Wharrad, H, Toutounchi, P & Glazebrook, C, 2023. Factors influencing COVID-19 health protective behaviours in Zambian university students with symptoms of low mood. BMC Public Health 23(1), 336. doi:10.1186/s12889-023-15073-4
- Nduku, PM & Simo-Kengne, D, 2022. Drivers of contraceptive use choice in Zambia. African Journal of Reproductive Health 26(5), 13–27. Article 5.
- Pfitzer, A, Lathrop, E, Bodenheimer, A, RamaRao, S, Christofield, M, MacDonald, P, Arnold, B, Bhatnagar, N, Mielke, E & Mikulich, M, 2020. Opportunities and challenges of delivering postabortion care and postpartum family planning during the COVID-19 pandemic. Global Health: Science and Practice 8(3), 335–43. doi:10.9745/GHSP-D-20-00263
- Phiri, M, Odimegwu, C & Kalinda, C, 2023. Unmet need for family planning among married women in sub-Saharan Africa: A meta-analysis of DHS data (1995 - 2020). Contraception and Reproductive Medicine 8(1), 3. doi:10.1186/s40834-022-00198-5
- Riley, T, Sully, E, Ahmed, Z & Biddlecom, A, 2020. Estimates of the potential impact of the COVID-19 pandemic on sexual and reproductive health In Low- and middle-income countries. International Perspectives on Sexual and Reproductive Health 46, 73. doi:10.1363/46e9020
- Rosenthal, DA, Hall, C & Moore, SM, 1992. AIDS, adolescents, and sexual risk taking: A test of the health belief model. Australian Psychologist 27(3), 166–71. doi:10.1080/00050069208257605
- Saasa, S & James, S, 2020. COVID-19 in Zambia: Implications for family, social, economic, and psychological well-being. Journal of Comparative Family Studies 51(3/4), 347–59.
- Sevalie, S., Youkee, D., van Duinen, A. J., Bailey, E., Bangura, T., Mangipudi, S., Mansaray, E., Odland, M. L., Parmar, D., & Samura, S. (2021). The impact of the COVID-19 pandemic on hospital utilisation in Sierra Leone. BMJ Global Health, 6(10), e005988.
- Simona, S, Lumamba, C, Moyo, F, Ng’andu, E & Phiri, M, 2022. The influence of contextual factors on maternal healthcare utilization in sub-saharan Africa: A scoping review of multilevel models [preprint]. Sexual and Reproductive Health. doi:10.1101/2022.03.15.22272437.
- Tadesse, E, 2020. Antenatal care service utilization of pregnant women attending antenatal care in public hospitals during the COVID-19 pandemic period. International Journal of Women’s Health 12, 1181–8. doi:10.2147/IJWH.S287534
- United Nations Zambia, 2020. COVID-19 Emergency appeal plan [strategy plan]. United Nations, Lusaka.
- Zambia Statistics Agency, 2021. Socio-Economic impact assessment of COVID-19 (SEIA) on households in Zambia. Zambia Statistics Agency, Lusaka. https://www.zamstats.gov.zm/.
- Zambia Statistics Agency, Ministry of Health (MOH) Zambia, and ICF, 2019. Zambia demographic and health survey 2018 [survey report]. Zambia Statistics Agency, Ministry of Health, and ICF, Lusaka and Rockville.
- Zhao, J, Song, F, Ren, S, Wang, Y, Wang, L, Liu, W, Wan, Y, Xu, H, Zhou, T, Hu, T, Bazzano, L & Sun, Y, 2012. Predictors of condom Use behaviors based on the health belief model (HBM) among female Sex workers: A cross-sectional study in Hubei province, China. PLOS ONE 7(11), e49542. doi:10.1371/journal.pone.0049542