
Abstract
Artificial intelligence (AI) technology in professional practice is regarded as the latest disruption to challenge ethical, societal, economic, and educational paradigms. It is becoming a contemporary narrative in our healthcare and educational discourse as it is thought to improve decision-making, education, patient care, and service delivery. If such benefits are to be realized it is important to ensure that our understanding of AI is underpinned with curricula to educate healthcare professionals about AI. Practitioners can then be better informed to participate fully in digital initiatives in their field. Few if any studies articulate a clear process in curricula design for professional practice and healthcare education. Therefore, an understanding of real-world applications of AI education for most professions is limited. As a result, there is an imperative to establish a sustainable learning space for professional healthcare practice education. This paper presents novel experiences, within a virtual lab environment, for the application of AI in healthcare. We identify and problematize insights into the AI competencies required for AI in professional healthcare practice education. With reference to our novel living lab titled, the Home Health Project, we present an interconnected case study model that suggest theoretical underpinning and opportunities to develop practitioner education pedagogy using AI concepts, concluding with a three-step proposal when delivering AI curriculum for this context.
Introduction
The use of Artificial Intelligence (AI) technology in the field of healthcare education and teaching is likely to be integral in any contemporary healthcare curriculum design. Selected examples in healthcare and education include AI for clinical data systems, educational genomics mapping, healthcare social media, and ChatGPT (Burke, Citation2021; Leming et al., Citation2023; Rudolph et al., Citation2023). With the advancement of AI technologies, educators are provided with an opportunity to complement and enhance pedagogy so that their students can improve their learning and knowledge with this disruptive technology (Akyuz, Citation2020; Popenici & Kerr, Citation2017). However, we must be cognizant that AI will challenge ethical, societal, economic, and educational paradigms. AI uses software technologies or systems that are perceived to make a computer or robot think and act like a human. AI is increasingly used to impact our everyday lives by using search engines, talking with virtual assistants on phones, and using predictive text applications (Khanna et al., Citation2013; Poola, Citation2017). Indeed, AI has the potential to customize learning for any user and offer them the ability to interact, collaborate and provide more meaningful experiences in online, mobile, or blended learning (Zawacki-Richter et al., Citation2019). Xie et al. (Citation2019) argue that the application of AI to education opens the door to the development of personalized supports and adaptive eLearning systems for the learner. In healthcare, it is seen as a technology that can enhance patient safety with virtual wards becoming the latest disruption to ensure patient safety is maintained (Connolly et al., Citation2022; Vindrola-Padros et al., Citation2021; Worlikar et al., Citation2022). One specific example, include scenarios where clinical data is collated, and any abnormalities trigger a digital nudgeor alert to the healthcare provider to suggest a reduction or escalation of clinical care (Irving & Neves, Citation2021).
AI in education combines the fields of computer science, education, psychology and the learning sciences AI is in education (Timms, Citation2016). The benefits of AI in education are multi-faceted, potentially increasing capacity and productivity of educators, providing valuable observations to enhance teaching and learning, and supporting learners’ development and AI in education delivers autonomous learning recommendations (The Institute for Ethical AI in Education, Citation2020). The evolution to Education 4.0 is understood as the provision of educational platforms mediated by AI, machine learning and ubiquitous learning (Salmon, Citation2019). Although this evolution must be embraced, there is nevertheless a need to consider fundamentally what, where and how we are being influenced in our learning in an era of digital transformation and ubiquitous learning. AI is hungry for data and AI is increasingly becoming a central cog within education, with student data being the engine oil and a critical commodity (Selwyn et al., Citation2020). The emergence of new and digital technologies may pose challenges to educational democracy. Algorithms and analytics may recode formal education. The drive to collect, process and analyze student data in education has the potential to embed a feeling of technoscientific governance, which is at odds with teaching professionalism (Nardi et al., Citation2018; Zuboff, Citation2019). As educators, we need to create an awareness and pay close attention to the ecosystem of platforms and services that students and teachers work within. We need to consider fundamentally what, where and how we are gathering data, what is influencing those learning and the ethics surrounding it (Nardi et al., Citation2018; Selwyn et al., Citation2020). In an era of AI healthcare professional practice educators, professionals, teachers, and ultimately the learners, will be exposed to a broad and more diverse range of learning experiences and social interaction. It is therefore important that in an era of ubiquitous learning, by machines using our data, that we as educators maintain the value of formal education and lifelong learning.
The technology and education relationship is critical for parity and equity (Selwyn, Citation2020) and although there is a relatively positive attitude toward AI amongst professionals in our healthcare ecosystem, there is a limited understanding of the specific technical aspects of AI systems (Coakley et al., Citation2022), consequently our professional practice education must adapt. Education occurs in many contexts and settings. This article expands the traditional ‘school’ setting to that of an island, to create an engaging learning experience, understand human learning and knowledge transfer, to facilitate behavioral change. The goal of this article, in considering professional practice education, namely continuous professional development for the caring professions such as in clinical and health sciences, was to enquire if we can gain more insight into the process of curriculum design for AI in professional practice education. In order to address this, the research questions formulated were: (1) What AI competencies are needed for professional practice education? and (2) In using the Home Health project as a case study, can we develop a model for professional growth, to enhance the change necessary in professional healthcare practice education to integrate AI education?
Home health project
The COVID19 pandemic expedited and brought to the fore the necessity for digital transformation within healthcare. As the pandemic worsened, the potential of technology in managing patients’ chronic conditions remotely was successfully demonstrated. Examples include diabetes education using humanoid robots (Connolly et al., Citation2022) or indeed hand hygiene adherence in a hospital setting (Worlikar et al., Citation2022). The Home Health project, in response to advances in digital healthcare, expands this work, creating an exemplar ecosystem in global digital health on an offshore island off the coast of Ireland.
The Home Health project is a state-of-the-art project in digital health and remote care, supported by industry and national funding agencies, aiming to investigate ways to enhance digital health infrastructure to improve patient care and evaluate novel digital health interventions. The transdisciplinary nature of the team and project objectives, provides participants, patients, stakeholders, an environment to analyze and integrate AI opportunities in professional practice. Referring to design education, applicable in this work, Buchanan (Citation1998) declared “what is new is the critical mass-comprised of individuals within design as well as individuals in other disciplines, all of whom see the possibilities for new inquiry in what is surely one of the most important and least recognized arts of human culture.” (p. 64). The project ecosystem and multidiscipline expertise will incorporate both the clinical needs of the Islanders, who are part of our projects Public Patient Involvement (PPI) group, and it will also push the boundaries of next generation digital health frontiers in utilizing latest technologies, innovations and processes.
The Home Health project, along with the remote monitoring of chronic diseases, namely hypertension, will generate a series of longitudinal physiological data. As an example, the project will explore AI methodologies using collected blood pressure measurement data to determine a patient’s necessity for an earlier appointment. Such an AI-driven model will dynamically schedule any patient’s appointment with their GP or concerned doctor’s clinic for further evaluation or treatment. This approach together with the healthcare professional’s experience enables timely clinical decision making.
In using the Home Health project as a case study for this article, we explore curriculum design and what AI competencies are necessary for professional practice curricula for the caring professions. The integration for AI in education creates change, change is identified with learning. The change occurring for the healthcare professional is due partly to the technological advancement, training and personal development and a combination of all. This article will articulate and present a model for professional growth and change when integrating AI in professional practice education in the Home Health project. Although particular to continuous professional development in this case study, elements can be adapted and applied to both undergraduate and graduate university courses.
Curriculum design
Irrespective of the specific professional practice, there is a need to productively exploit the advantages offered by technology in terms of creating adaptive and responsive learning environments supporting learning approaches, informed by the global competencies model (Andriole, Citation2017; Pisa 2018). It has been well documented that there is an immediate requirement to incorporate AI education into both undergraduate and postgraduate professional practice education, as well as professional practice continuous development. For example, medical and healthcare educators have called for the wider healthcare community to embrace AI in daily practice (Coakley et al., Citation2022; Grunhut et al., Citation2021). Meanwhile Salas-Pilco et al. (Citation2022) and Chassignol et al. (Citation2018) demonstrates how AI will reshape education. O’Connor et al. (Citation2022) also highlight the necessity for curricula to be developed for the largest healthcare workforce and educate nursing and midwifery professionals.
Curriculum creation is a dynamic process which involves the physician or teacher navigating policy frameworks to provide success for the learner (Simmons & McLean, Citation2018), it is concerned with the processes, and the outcomes that come from those processes (Priestley, Citation2011). Curriculum is therefore not a product to be delivered uncritically by practitioners through a ‘tick box’ approach (Priestley & Biesta, Citation2013), but rather is concerned with the medical professional, tutor or teacher making sense of it and developing contextualized practices (Ketelaar, et al., Citation2012). The teacher or practitioner mediates policy and develops practices according to local needs. In a classroom or clinical setting teachers and students are co-constructors of the enacted curriculum (Ball & Cohen, Citation1996; Grossman & Thompson, Citation2004), as the curriculum becomes real when it is enacted in the interactions which take place between the teacher and student (McKernan, Citation1991). Implicated in curriculum is the understanding of sense making which is enacted from policy to practice (Blignaut, Citation2008; Klien, Moon & Hoffman, Citation2006; März & Kelchtermans, Citation2013). The curriculum is not just a set of instructions for what we do but, should be considered as the framework, the resources and the ideas which frame our action (Clements, Citation2007; Priestley et al., Citation2012). The curriculum materials and resources influence the educators’ pedagogical decisions, determine curricular design and serve as a source of learning (Ball & Cohen, Citation1996; Ball & Feiman-Nemser, Citation1988; Collopy, Citation2003; Grossman & Thompson, Citation2004; Remillard, Citation2005; Wang & Paine, Citation2003). Core to the learning of curriculum is this active engagement, developing practices, encouraging curriculum as social practice, and enabling the concept of curriculum making as opposed to a sedentary curriculum implementation approach.
The knowledge and the skills developed through the curriculum are key but also of concern is how we assess and evaluate what needs to be built in, so therefore it is also about pedagogy and in particular assessment. Referring to teacher education Priestley (Citation2016, p.5) states that if we “focus on developing the capacity of young people to act within the world, and characterised by more dialogical and collaborative pedagogies, continuous approaches to assessment and higher degrees of teacher agency as they act as curriculum developers”, applicable in professional practice with additional considerations and ramifications. Assessment, and particularly formative assessment help us to identify and bridge the gap between the intended and the received curriculum and is integral in professional practice education. The two processes are not independent, but rather assessment informs the curriculum and therefore at times dictates the curriculum content (Hargreaves et al., Citation1996). Therefore, curriculum content required for AI embedded in professional practice education requires discussion which we present in the next section.
AI curriculum in professional healthcare practice education
There have been calls for an AI curriculum for healthcare professionals to be developed. O’Connor et al. (Citation2022) highlighted the need for the discipline of nursing and midwifery to both lead and contribute. Such approaches can advantage practitioners and students in becoming more familiar and comfortable with the technologies for when they are used in clinical setting (Buchanan et al., Citation2021). Educators must prepare their students for the potential changes AI can have on healthcare (Lee et al., Citation2021). Although specific to nursing education Buchanan et al. (Citation2021) notes that a reform of the curriculum is required in both academic and clinical environments, and at all educational levels (O’Connor et al., Citation2022). Charow et al. (Citation2021) also consider the various educational levels and specifies what should be taught depending on the educational stage such as in undergraduate, postgraduate or in continuing professional development.
In relation to content delivery Lee et al. (Citation2021) elaborated in their review that many teaching approaches were advised including lectures, online modules, small group learning and the most common suggestion was experiential learning. Nurse educators should incorporate new pedagogies which include AI to help better support undergraduate students and in so doing develop appropriate AI knowledge and skills (Buchanan et al., Citation2021). This is important so that both students and practitioners gain the appropriate knowledge and skill needed for an holistic approach to AI initiatives (O’Connor et al., Citation2022). However, also important to consider is the knowledge and skill of the educators teaching students and practitioners. A recommendation by O’Connor et al. (Citation2022) includes the consideration to invest in educators’ professional development in order to be able to educate on the topic. Therefore, it seems reasonable to strongly suggest that educators develop educational approaches and understanding of pedagogy, and curriculum to better prepare healthcare students to incorporate AI health technologies into their practice.
Few healthcare practice disciplines have ignored the importance of AI for their profession. Reviews on AI in undergraduate medical and nursing education provide recommendations on the content which could be included in the curriculum such as machine learning literacy and the ethics of AI (Buchanan et al., Citation2021; Lee et al., Citation2021). Lee et al. (Citation2021) completed a scoping review regarding AI in undergraduate medical education and noted the overarching themes such as working with electronic health records, critically appraising AI systems, working with and managing AI system and their ethical and legal implications and an ongoing emphasis on biomedical knowledge and pathophysiology of disease. In relation to nursing education Buchanan et al. (Citation2021) summarized the current and predicted influences of AI health technologies recommending topics to be added to an AI curriculum such as basic informatics competencies, data analytics, predictive modeling, machine learning and engineering principles, ethics, privacy issues, digital/data literacy, big data governance, technocentric cultural competence, AI research design and robotics care and operations. In a systematic review on AI in nursing and midwifery O’Connor et al. (Citation2022) summarized the requirement of educators to design a curriculum on machine learning, natural language processing and other areas within AI. Charow et al. (Citation2021) identified AI education programs for healthcare professionals, including medical, nursing and radiology technicians. This review summarized categories regarding the content noted in the AI programs such as AI use and interpretating, as well as developing skills to discuss the results of AI algorithms. For social work education, it was also noted that there is an incentive to consider digital literacy in the curriculum, as AI will likely become routine in social work practice. They highlight three areas to consider which include (1) the content, (2) the delivery and (3) the associated threats regarding the future of social work and its education (Hodgson et al., Citation2022). Whilst there are some similarities regarding recommendations of what should be included in the AI curriculum, there appears to be no consensus. Lee et al. (Citation2021) identified many papers in their review and stated that there was no real consensus in the studies reported regarding the content and delivery of the curriculum (Lee et al., Citation2021).
Healthcare curricula is constantly updating, innovating and responding to challenges. If AI technologies are to become further embedded in educational provision, clear training and competencies expected for healthcare professionals are required. The review by Charow et al. (Citation2021) detailed these skills and competencies in the use of AI. Additionally, Gray et al. (Citation2022) surveyed healthcare education experts to explore their opinions in preparing the healthcare workforce with AI education. Respondents ranked a list of specific topics that could be considered necessary for their competence and the majority agreed on the importance of three topic areas (1) ethics, (2) machine learning and (3) criteria for judging the suitability of large data sets for use in clinical AI applications. A low number of respondents agreed that these important topics were being taught adequately (Gray et al., Citation2022). The e-Delphi study carried out by Çalışkan et al. (Citation2022) provides a list of AI competencies required by medical students, which can contribute to developing a curriculum and can also be used as a guiding theoretical framework. There were 27 competencies listed with 23 having a strong consensus and four a weak consensus, . These competencies can be considered a guide for educators to evaluate where their knowledge may be lacking, develop their knowledge and then ultimately teach their students.
Table 1. AI competencies required by medical students (adapted from Çalışkan et al., Citation2022).
A model of professional growth, integrating AI in professional practice education on the Home Health project
If AI is to be incorporated in a healthcare curriculum, we propose a model for professional practice education. Specifically, a networked model for professional development and professional growth in a changing environment aligned to the Home Health project is presented. We also provide exemplars for the domains of the model with how it may align with the professional growth of educators tasked with teaching future generations of healthcare practitioners on AI.
A linear relationship in which teacher learning of new knowledge and skills influences classroom practice, and classroom practice influences student learning was proposed by Guskey (Citation1986, Citation2000). Clarke and Hollingsworth (Citation2002) on the other hand developed the Interconnected Model of Professional Growth, enabling individual paths in teacher development. Their model is adapted and used in the Home Health project, , as there is potential for its use in alternate professional practices. The model clarifies the underlying processes that mediate change, valid when incorporating AI education in professional practice training. In this context change is aligned to learning, the change occurring for the educator may be because of training, adaptation, personal development, local reform, system restructuring or change as growth or learning (Clarke & Hollingsworth, Citation2002). The model identifies four domains in which change can occur with the first three domains forming part of the professional life of the practitioner, and directly applicable to the Home Health project, . Nevertheless change can and does occur in any of the four domains, with the type of change particular to the domain.
Figure 1. The Interconnected Model of Professional Growth for Home Health (adapted from Clarke & Hollingsworth, Citation2002).
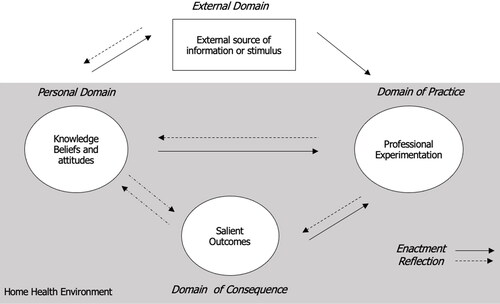
Educator change in any of the four domains is mediated through processes of enactment and reflection (Schön, Citation1987; Snyder et al., Citation1992). Reflection will occur on and in action (Rolfe, Citation2002; Schön, Citation1987), whereas enactment will occur as the practitioner “grows ever more competent in constructing positive educational experiences.” (Snyder et al., Citation1992, p. 418). The Clarke and Hollingsworth (Citation2002) model allows for practitioners to follow different paths in their learning trajectory of professional development. In using the Home Health project as a case study, we demonstrate how incorporating AI education can be embedded in a model for professional practice development. The four domains in the Clarke and Hollingsworth (Citation2002) model are (1) a personal domain, (2) the domain of practice, (3) the domain of consequences, and (4) the external domain.
The personal domain is concerned with knowledge, skills, attitudes and beliefs. For educators and healthcare practitioners change in this domain will happen as the professional acquires new knowledge, skills, attitudes or beliefs. Educators have been required to adapt their pedagogies in recent years to using technologies such as virtual tools to both teach and assess students. In the Home Health project, some clinical care will be delivered via video conferencing tools, aiming to include the full spectrum of health care professionals - care including medical, nursing, physiotherapy, speech and language therapy for example. This combined with the work-package on home care and remote monitoring of sensors for glucose, blood pressure and weight, will involve some AI behavioral change and new learning for the practitioners and patients on the island. Other AI aspects of the Home Health project will involve drone delivery to provide remote care, in for example delivering physical items (e.g. medications from clinician to patient or blood sample from patient to hospital); robot triage—robots performing preliminary assessment of patients or casualties; AI for dynamic patient appointments and AI in mixed reality education provision. The knowledge, skills and attitudes of the professional practitioners as they engage with these AI technologies will no doubt alter and change their personal domain.
Professional practitioners participate in a variety of professional arenas where they learn—in community workshops, at their professional associations, and with research projects like Home Health. All forms of professional experimentation are considered in the ‘domain of practice’. Although Clarke and Hollingsworth (Citation2002) note that the domain of practice is often limited to teachers’ experience in the classroom, they explicitly refer that professional experimentation is not limited to solely a clinical setting. Change in this domain occurs when the educators develop new curriculum materials and try out new practices and in the Home Health project, a core deliverable relates to exploring and delivering health promotion to the engaged residents and islanders. The domain of practice embodies the community involvement in the project, as the medical provision shifts its focus from care of the disease to health promotion and disease prevention.
The third domain, the domain of consequences presents the outcomes of new practices for the educators themselves and their learners. When the educator perceives these outcomes and practices as salient, change has occurred. The outcomes that are salient to an educator’s practice may include control and learner motivation, in addition to the student or practitioner developing new clinical ideas. Change in the domain of consequence is therefore firmly tied to the educators existing value system and to the inferences they draw from the practice. In embedding AI in multiple perspectives on the project, through for example virtual reality, drone delivery, home telepresence, the AI education domain of consequence will be affected for both the patient and practitioner.
The external domain is outside the professional day-to-day practice and offers alternate sources of stimuli and information to support and develop new practices. Change in this domain for both educators and healthcare practitioners such as in the Home Health project is defined as becoming aware of new ideas, practices, and/or strategies introduced and developed by others such as external stakeholders like the Health Service Executive (HSE), regulatory bodies such as the Medical Council and Nursing and Midwifery Board of Ireland are influenced.
Once regulatory authorizes publish their professional frameworks there is an immediate likelihood that higher education institutions will be required to embed the curricular reforms in their undergraduate and postgraduate offerings. With the possibility of existing curricula being enhanced, there are opportunities for interprofessional learning and these collaborative approaches are welcomed by WHO, educational approaches which enhance and strengthen healthcare systems worldwide.
Educational and clinical institutions and environments may consider the use of the interconnected model framework when considering the competencies of educators and healthcare practitioners in the area of AI. It provides a process by focusing on the individual’s personal domain, professional domain, considering the salient outcomes expected and the external domain. This is just one framework that we propose as we continue to acquire new knowledge on the area of AI we may identify more appropriate theories, models or framework to develop our competencies or develop a new approach entirely.
Discussion
The implications of increasing datafication of education raises significant questions about models being created and informing of human behaviors, that have been learned from machines. In professional practice the implications are crucial. Nevertheless, we are likely to accept that AI will increasingly become the engine of education, and learner or patient data the fuel, irrespective of the specific discipline. It is critical that there are conversations around ethics and technology, led in the interest of practitioners, educators and society enquiring more of the implications (Davenport & Katyal, Citation2018; Selwyn, Citation2020). Awareness of the significant and influential learning happening in our society and how our learning as citizens, educators and practitioners is intertwined with technology. The professional practitioner’s desire and innovation is necessary to lead the way, but awareness of how and where data is stored, who has access to it and if the data ultimately benefits or hinders the participant or organization is crucial. There is a necessity to highlight the extent to which we need to be alert in this era of ubiquitous computing and ubiquitous learning - by machines using our data. Adopting an agnostic view is not desirable.
Although the Home Health project is specific to the in-field practitioner it is evident from the literature that several disciplines in healthcare and professional practice are aware of the importance of needing a curriculum focusing on AI for undergraduate and postgraduate studies. These practitioners include but are not limited to nursing, midwifery, social work, radiography and medicine. Acknowledging the need for a framework to embed AI education, both the use of AI and about AI, within their profession is needed for the purposes as we have outlined. To date there is limited AI education and training available for healthcare professionals and there is a need to develop education programs for healthcare professionals (Charow et al., Citation2021). An area of future research will be best practice in how AI should be incorporated and taught to healthcare professionals and this should be led by the best evidence available.
Recent research has been carried out regarding AI in medical and nursing and midwifery education and studies have noted that there is a need for an AI curriculum and recommendations have been provided on the topics to be taught and the competencies which should be expected (Charow et al., Citation2021; O’Connor et al., Citation2022). General suggestions are considered regarding further research in the area, as highlighted in this article, this should include developing a competency driven curriculum and incorporating a more interprofessional approach on the topic of AI in healthcare education. As suggested earlier the integration is likely to be forced from regulatory agencies however educational institutions can influence the agenda of the how it might be incorporated. One example might include an interprofessional lens in order to ensure future practitioners receive the same knowledge and skills. O’Connor et al. (Citation2022) suggest considering interprofessional education as AI is integrated in all disciplines. Similarly, Charow et al. (Citation2021) provided recommendations which could be followed to help guide AI curriculum development. These recommendations included but were not limited to incorporating a multidisciplinary approach to the curriculum.
Whilst suggesting interprofessional approaches is likely a local issue competency-based curriculum as suggested by Charow et al. (Citation2021) is likely to include wider discipline and interprofessional agreement. Therefore, it is reasonable to suggest that future research funding should identify these challenges and opportunities. Additionally, how dissemination, implementation and evaluation of curriculum and teaching practices regarding AI education occurs. This is important as there few studies which have focused on programs implemented, and the evaluation of program outcomes such as student knowledge or satisfaction is absent (Lee et al., Citation2021). It is also important that the work done toward creating and implementing an AI curriculum is guided by known educational theory or frameworks. As Lee et al. (Citation2021) noted that no educational theories or frameworks were noted in the studies in their review.
Although specifically for medical education, Lee et al. (Citation2021) three step proposal when delivering AI curriculum, , could be considered for all healthcare education. First, to create a standardized set of core competencies such as knowledge or skills specific to AI education. Secondly, to create and implement an evidence and theory guided AI curriculum with planned program evaluations to help improve the curriculum. Thirdly, to make the effort to share and publish findings regarding AI curriculum creation in relation to content and delivery. It is likely that findings from each professions experimentation with the AI will likely translate impactful AI outputs such as clinical dataset or AI that contributes to point of care decision making.
Table 2. Three step proposal when delivering AI medical curriculum (Lee et al., Citation2021).
Conclusion
There has also been considerable interest internationally in how AI and related areas can be applied and taught in professional practice and lifelong education settings. This paper and the HomeHealth project is concerned with professional healthcare practice education, nevertheless there are many parallels with teacher education. For example, the implications and similarities with healthcare practice education regarding AI assessment and feedback design, development, deployment and evaluation, and teacher education are many. And while AI has promise, it currently lacks in-depth analysis of impact and raises several ethical considerations for and within teacher education (Connolly & ÓCeallaigh, Citation2023).
Models of practice in teacher education are closely aligned to paradigmatic orientations which are dominant at particular points in time (Zeichner, Citation1983) and generative AI tools, for example ChatGPT, have the potential to challenge the practice significantly, requiring the upskilling of teacher educators also. However, considering the rapid advancements in AI and its increasing significance in education, the lack of AI resources in teacher preparation and education is noteworthy (Whalen & Mouza, Citation2023). The extent to which such new technologies can and should have an impact, on pedagogical practice, remains contested and debated (Salas-Pilco et al., Citation2022; Vazhayil et al., Citation2019; Whalen & Mouza, Citation2023). Lessons from prior debates with disruptive technologies in education should be harnessed.
The professional development of teachers and teacher educators in the changing educational context has an important role to play - in promoting understanding of generative AI knowledge, assessment and feedback, defining goals and objectives, instructional design and teaching depth, scaffolding and ethics, and ensuring the development of emerging skills to underpin future directions. Therefore, uses of technology broadly classified under the umbrella of AI may have the capacity to bring real benefits to teacher education and healthcare professionals, and ultimately to their learners and patients. Nonetheless, we are still exploring what these benefits might be, how technology can interact with curriculum, pedagogy and assessment, and how we deal with challenges around issues such as privacy, surveillance, student voice and agency, among many others.
In making the Island a beacon for digital healthcare delivery, the Home Health project is improving patient healthcare and inadvertently developing an approach and framework for upskilling professional practitioners in AI education. This article unbundles AI in professional practice pertaining to the project, presenting a model for growth and chance for professional practice education. The model is particular to continuous professional development education of healthcare professional practitioners, however much of the learning can be adapted and applied to both undergraduate and postgraduate university courses. Although not a panacea for all technological innovation and change - education, technology and practice are always partners, discovering and disseminating new knowledge in the field; where the skills and knowledge go beyond the skills of today, but for the future. Home Health intends to exemplify this reality.
References
- Akyuz, Y. (2020). Effects of intelligent tutoring systems (ITS) on personalized learning (PL). Creative Education, 11(06), 953–978. doi:10.4236/ce.2020.116069
- Andriole, S. J. (2017). Five myths about digital transformation. MIT Sloan Management Review, 58(3). https://sloanreview.mit.edu/article/five-myths-about-digital-transformation/
- Ball, D. L., & Cohen, D. K. (1996). Reform by the book: What is—or might be—The role of curriculum materials in teacher learning and instructional reform? Educational Researcher, 25(9), 6–14. doi:10.3102/0013189X025009006
- Ball, D. L., & Feiman-Nemser, S. (1988). Using textbooks and teachers’ guides: A dilemma for beginning teachers and teacher educators. Curriculum Inquiry, 18(4), 401–423. doi:10.1080/03626784.1988.11076050
- Blignaut, S. (2008). Teachers’ sense-making and enactment of curriculum policy. Journal of Education, 43(1), 101–125. https://d1wqtxts1xzle7.cloudfront.net/17562538/joe_43-libre.pdf
- Buchanan, R. (1998). Education and professional practice in design. Design Issues, 14(2), 63–66. doi:10.2307/1511851
- Buchanan, C., Howitt, M. L., Wilson, R., Booth, R. G., Risling, T., & Bamford, M. (2021). Predicted influences of artificial intelligence on nursing education: Scoping review. JMIR Nursing, 4(1), e23933. doi:10.2196/23933
- Burke, E. (2021). Stimul.ai: Health-tech start-up with an AI cure for hospital waiting lists, Silicon Republic. https://www.siliconrepublic.com/start-ups/stimul-ai-health-tech-cork-hospital-waiting-lists
- Çalışkan, S. A., Demir, K., & Karaca, O. (2022). Artificial intelligence in medical education curriculum: An e-Delphi study for competencies. Plos One, 17(7), e0271872. doi:10.1371/journal.pone.0271872
- Chassignol, M., Khoroshavin, A., Klimova, A., & Bilyatdinova, A. (2018). Artificial Intelligence trends in education: A narrative overview. Procedia Computer Science, 136, 16–24. doi:10.1016/j.procs.2018.08.233
- Charow, R., Jeyakumar, T., Younus, S., Dolatabadi, E., Salhia, M., Al-Mouaswas, D., Anderson, M., Balakumar, S., Clare, M., Dhalla, A., Gillan, C., Haghzare, S., Jackson, E., Lalani, N., Mattson, J., Peteanu, W., Tripp, T., Waldorf, J., Williams, S., Tavares, W., & Wiljer, D. (2021). Artificial intelligence education programs for health care professionals: Scoping review. JMIR Medical Education, 7(4), e31043. doi:10.2196/31043
- Clarke, D., & Hollingsworth, H. (2002). Elaborating a model of teacher professional growth. Teaching and Teacher Education, 18(8), 947–967. doi:10.1016/S0742-051X(02)00053-7
- Clements, D. H. (2007). Curriculum research: Toward a framework for “research-based curricula”. Journal for Research in Mathematics Education, 38(1), 35–70. doi:10.2307/30034927
- Coakley, S., Young, R., Moore, N., England, A., O’Mahony, A., O’Connor, O. J., Maher, M., & McEntee, M. F. (2022). Radiographers’ knowledge, attitudes and expectations of artificial intelligence in medical imaging. Radiography (London, England: 1995), 28(4), 943–948. doi:10.1016/j.radi.2022.06.020
- Collopy, R. (2003). Curriculum materials as a professional development tool: How a mathematics textbook affected two teachers’ learning. The Elementary School Journal, 103(3), 287–311. doi:10.1086/499727
- Connolly, C., & Ó Ceallaigh, T. J. (2023). Transforming practice through innovative assessment and feedback design in teacher education: Taking stock and looking forward. In C. Connolly and T. J. Ó. Ceallaigh (Eds.), Innovating assessment and feedback design in teacher education: Transforming practice, ATEE Book Series. Routledge.
- Connolly, C., Walsh, J. C., Worlikar, H., Ryan, L., Murray, A., O’Connor, S., Kelly, J., Coleman, S., Vyas Vadhira, V., Newell, E., & O’Keeffe, D. T. (2022). New frontiers of education using humanoid robots – A case study of patient centred innovation in digital health education. Irish Educational Studies, 41(1), 107–115. doi:10.0.4.56/03323315.2021.2022514
- Davenport, T. H., Katyal, V. (2018). Every Leader’s Guide to the Ethics of AI. MIT Sloan Management Review. https://sloanreview.mit.edu/article/every-leaders-guide-to-the-ethics-of-ai/
- Guskey, T. R. (1986). Staff development and the process of teacher change. Educational Researcher, 15(5), 5–12. doi:10.3102/0013189X015005005
- Guskey, T. R. (2000). Evaluating professional development. Corwin press.
- Gray, K., Slavotinek, J., Dimaguila, G. L., & Choo, D. (2022). Artificial intelligence education for the health workforce: Expert survey of approaches and needs. JMIR Medical Education, 8(2), e35223. doi:10.2196/35223
- Grossman, P., Thompson, C. (2004). Curriculum materials: Scaffolds for new teacher learning? A research report. Document R-04-1. https://eric.ed.gov/?redir=http%3a//www.ctpweb.org
- Grunhut, J., Wyatt, A. T., & Marques, O. (2021). Educating future physicians in artificial intelligence (AI): An integrative review and proposed changes. Journal of Medical Education and Curricular Development, 8, 23821205211036836. doi:10.1177/23821205211036836
- Hargreaves, A., Earl, L. M., & Ryan, J. (1996). Schooling for change: Reinventing education for early adolescents. Routledge.
- Hodgson, D., Goldingay, S., Boddy, J., Nipperess, S., & Watts, L. (2022). Problematising artificial intelligence in social work education: Challenges, issues and possibilities. The British Journal of Social Work, 52(4), 1878–1895. doi:10.1093/bjsw/bcab168
- Irving, G., & Neves, A. L. (2021). What next for COVID Oximetry and virtual ward? The British Journal of General Practice: The Journal of the Royal College of General Practitioners, 71(710), 425–426. doi:10.3399/bjgp21X717041
- Ketelaar, E., Beijaard, D., Boshuizen, H. P. A., & Den Brok, P. J. (2012). Teachers’ positioning towards an educational innovation in the light of ownership, sense-making and agency. Teaching and Teacher Education, 28(2), 273–282. doi:10.1016/j.tate.2011.10.004
- Khanna, S., Sattar, A., & Hansen, D. (2013). Artificial intelligence in health–The three big challenges. The Australasian Medical Journal, 6(5), 315–317. doi:10.4066/AMJ.2013.1758
- Klein, G., Moon, B., & Hoffman, R. R. (2006). Making sense of sensemaking 1: Alternative perspectives. IEEE Intelligent Systems, 21(4), 70–73. doi:10.1109/MIS.2006.75
- Lee, J., Wu, A. S., Li, D., & Kulasegaram, K. M. (2021). Artificial intelligence in undergraduate medical education: A scoping review. Academic Medicine: Journal of the Association of American Medical Colleges, 96(11S), S62–S70. doi:10.1097/ACM.0000000000004291
- Leming, M., Das, S., & Im, H. (2023). Adversarial confound regression and uncertainty measurements to classify heterogeneous clinical MRI in Mass General Brigham. Plos One, 18(3), e0277572. doi:10.1371/journal.pone.0277572
- März, V., & Kelchtermans, G. (2013). Sense-making and structure in teachers’ reception of educational reform. A case study on statistics in the mathematics curriculum. Teaching and Teacher Education, 29, 13–24. doi:10.1016/j.tate.2012.08.004
- McKernan, J. (1991). Reconceptualizing the post‐primary curriculum: A grid‐matrix for the design and evaluation of a core curriculum. Irish Educational Studies, 10(1), 188–204. doi:10.1080/0332331910100119
- Nardi, B., Tomlinson, W., Patterson, D., Chen, J., Pargman, D., Raghavan, B., & Penzenstadler, B. (2018). Computing within limits. Communications of the ACM, 61(10), 86–93. doi:10.1145/3183582
- O’Connor, S., Yan, Y., Thilo, F. J., Felzmann, H., Dowding, D., & Lee, J. J. (2022). Artificial intelligence in nursing and midwifery: A systematic review. Journal of Clinical Nursing, 32(13-14), 2951–2968. doi:10.1111/jocn.16478
- PISA Global Competence. (2018). Image of global competence graphic, OECD.org. https://www.oecd.org/pisa/pisa-2018-global-competence.htm
- Poola, I. (2017). How artificial intelligence in impacting real life everyday. International Journal for Advance Research and Development, 2(10), 96–100. www.IJARnD.com.
- Popenici, S. A., & Kerr, S. (2017). Exploring the impact of artificial intelligence on teaching and learning in higher education. Research and Practice in Technology Enhanced Learning, 12(1), 22. doi:10.1186/s41039-017-0062-8
- Priestley, M. (2016). A perspective on learning outcomes in curriculum and assessment. National Council for Curriculum and Assessment (NCCA). http://hdl.handle.net/1893/23225
- Priestley, M. (2011). Whatever happened to curriculum theory? Critical realism and curriculum change. Pedagogy, Culture and Society, 19(2), 221–237. doi:10.1080/14681366.2011.582258
- Priestley, M., & Biesta, G. (Eds.). (2013). Reinventing the curriculum: New trends in curriculum policy and practice. A&C Black.
- Priestley, M., Edwards, R., Priestley, A., & Miller, K. (2012). Teacher agency in curriculum making: Agents of change and spaces for manoeuvre. Curriculum Inquiry, 42(2), 191–214. doi:10.1111/j.1467-873X.2012.00588.x
- Remillard, J. T. (2005). Examining key concepts in research on teachers’ use of mathematics curricula. Review of Educational Research, 75(2), 211–246. doi:10.3102/00346543075002211
- Rolfe, G. (2002). Reflective practice: Where now? Nurse Education in Practice, 2(1), 21–29. doi:10.1054/nepr.2002.0047
- Rudolph, J., Tan, S., & Tan, S. (2023). ChatGPT: Bullshit spewer or the end of traditional assessments in higher education? Journal of Applied Learning & Teaching, 6(1), 342–363. doi:10.37074/jalt.2023.6.1.9
- Salmon, G. (2019). May the fourth be with you: Creating education 4.0. Journal of Learning for Development, 6(2), 95–115. https://jl4d.org/index.php/ejl4d/article/view/352 doi:10.56059/jl4d.v6i2.352
- Salas-Pilco, S. Z., Xiao, K., & Hu, X. (2022). Artificial intelligence and learning analytics in teacher education: A systematic review. Education Sciences, 12(8), 569. doi:10.3390/educsci12080569
- Schön, D. A. (1987). Educating the reflective practitioner: Towards a new design for teaching and learning in the professions. Jossey-Bass.
- Selwyn, N. (2020). Digital education in the aftermath of COVID-19: Critical concerns and hopes. Techlash, 1, 6–10. https://der.monash.edu/wp-content/uploads/2020/06/TECHLASH-01-COVID-education.pdf
- Selwyn, N., Hillman, T., Eynon, R., Ferreira, G., Knox, J., Macgilchrist, F., & Sancho-Gil, J. M. (2020). What’s next for Ed-Tech? Critical hopes and concerns for the 2020s. Learning, Media and Technology, 45(1), 1–6. doi:10.1080/17439884.2020.1694945
- Simmons, J., & MacLean, J. (2018). Physical education teachers’ perceptions of factors that inhibit and facilitate the enactment of curriculum change in a high-stakes exam climate. Sport, Education and Society, 23(2), 186–202. doi:10.1080/13573322.2016.1155444
- Snyder, J., Bolin, F., & Zumwalt, K. (1992). Curriculum implementation In P. Jackson (Ed.), Handbook of research on curriculum (pp. 402–435). Macmillan.
- The Institute for Ethical AI in Education. (2020). Interim Report, Towards a shared vision of Ethical AI in Education. University of Buckingham. https://www.buckingham.ac.uk/wp-content/uploads/2020/02/Summary-The-Institute-for-Ethical-AI-in-Educations-Interim-Report-Towards-a-Shared-Vision-of-Ethical-AI-in-Education.pdf
- Timms, M. J. (2016). Letting artificial intelligence in education out of the box: Educational cobots and smart classrooms. International Journal of Artificial Intelligence in Education, 26(2), 701–712. doi:10.1007/s40593-016-0095-y
- Vazhayil, A., Shetty, R., Bhavani, R. R., Akshay, N. (2019, December). Focusing on teacher education to introduce AI in schools: Perspectives and illustrative findings. In 2019 IEEE Tenth International Conference on Technology for Education (T4E) (pp. 71–77). IEEE. doi:10.3390/educsci12080569
- Vindrola-Padros, C., Singh, K. E., Sidhu, M. S., Georghiou, T., Sherlaw-Johnson, C., Tomini, S. M., Inada-Kim, M., Kirkham, K., Streetly, A., Cohen, N., & Fulop, N. J. (2021). Remote home monitoring (virtual wards) for confirmed or suspected COVID-19 patients: A rapid systematic review. EClinicalMedicine, 37, 100965. doi:10.1016/j.eclinm.2021.100965
- Wang, J., & Paine, L. W. (2003). Learning to teach with mandated curriculum and public examination of teaching as contexts. Teaching and Teacher Education, 19(1), 75–94. doi:10.1016/S0742-051X(02)00087-2
- Whalen, J., & Mouza, C. (2023). ChatGPT: Challenges, opportunities, and implications for teacher education. Contemporary Issues in Technology and Teacher Education, 23(1), 1–23. https://www.learntechlib.org/primary/p/222408/.
- Worlikar, H., Vadhiraj, V. V., Murray, A., O’Connell, J., Connolly, C., Walsh, J. C., & O’Keeffe, D. T. (2022). Is it feasible to use a humanoid robot to promote hand hygiene adherence in a hospital setting? Infection Prevention in Practice, 4(1), 100188. doi:10.1016/j.infpip.2021.100188
- Xie, H., Chu, H. C., Hwang, G. J., & Wang, C. C. (2019). Trends and development in technology enhanced adaptive/personalized learning: A systematic review of journal publications from 2007 to 2017. Computers & Education, 140, 103599. doi:10.1016/j.compedu.2019.103599
- Zawacki-Richter, O., Marín, V., Bond, M., & Gouverneur, F. (2019). Systematic review of research on artificial intelligence applications in higher education – Where are the educators? International Journal of Educational Technology in Higher Education, 16(1), 1–27. doi:10.1186/s41239-019-0171-0
- Zeichner, K. M. (1983). Alternative paradigms of teacher education. Journal of Teacher Education, 34(3), 3–9. doi:10.1177/002248718303400302
- Zuboff, S. (2019). Surveillance capitalism and the challenge of collective action. In New Labor Forum (Vol. 28, No. 1, pp. 10–29). Los Angeles, CA: SAGE Publications.