
Abstract
The prevalence of childhood obesity has increased at an alarming rate despite several actions to reverse this trend. It is important to focus on tackling the constraints for healthy food provisioning. We focus on identifying segments of mothers in relation to factors acting as barriers to healthy eating. Five hundred mothers in each country (Argentina, France and Denmark) completed an online survey. In each of the three countries, four segments are identified, varying mostly on working and socio-economic status, self-efficacy and attitudes to health experts. Segments of mothers who are skeptical to nutrition advice from health professionals were identified. Another important finding is that staying-at-home mothers might face more barriers to healthy eating than mothers who work outside the home. We provide suggestions for targeted interventions addressing healthy eating behaviors among mothers with different profiles.
Background
Being a parent today implies exposure to multiple discourses concerning food and health and how best to bring up one’s child. Parents encounter alarming reports concerning childhood obesity and welfare diseases in childhood […] At the same time, parents have their everyday life to handle, with work, travel, leisure activities, meal preparation and other household chores, where time, money and space determine the limits for what it is possible.
(Johansson et al., Citation2013, p. 458)
Childhood obesity has reached worrying levels in most economically developed and developing countries and represents one of the biggest challenges of the 21st century (World Health Organization, Citation2016a). The prevalence of childhood obesity in Europe and in Latin America has increased at an alarming rate due to changes in dietary patterns and lifestyles in the past decades (World Health Organization, Citation2016b). In many countries, the problem is worsening dramatically. This is the case of Argentina, where childhood obesity rates quadrupled between 1990 and 2007 (Orden et al., Citation2013).
However, in an attempt to solve the problem, health experts encounter the risk of overwhelming parents beyond their capacities for action, as exposed by Johansson et al. (Citation2013) in the quote chosen to open this article. Scholars have called attention to the judgmental moral tone of public nutritional approaches, especially toward mothers. Although not intentionally, some public health approaches might contribute to place the burden of cooking healthy meals mainly on women, who are presumed to carry solely the responsibility for families’ healthy eating (Elliott & Bowen, Citation2018; Wright et al., Citation2015).
Therefore, a supportive investigational approach is crucial, one that focuses on the constraints for healthy food provisioning among mothers, as opposed to focusing on nutrition “rules” that are difficult—if not impossible—to follow. To predict, identify and understand the factors acting as barriers to parental healthy eating with an appropriate theoretical framework is pivotal for effective promotion of healthy lifestyles and obesity prevention in childhood (Birch & Anzman, Citation2010).
In this regard, the Social Cognitive Theory (SCT) has proven to be a suitable framework to investigate mothers’ food-related behaviors that support optimal child nutrition and obesity prevention (Byrd-Bredbenner et al., Citation2011). The SCT considers a triad of factors influencing behavior adoption and change, including personal, environmental and behavioral aspects. Environmental (e.g., social/family support, barriers and constraints), personal (e.g., self-efficacy, knowledge, outcome expectations) and behavioral determinants (e.g., skills) all have an impact on food choices and vary across different cultural contexts (Bandura, Citation2002).
Given the complexity of factors influencing eating behaviors at the family level, scholars have emphasized the need for multi-disciplinary approaches to promote healthy eating habits. Social Marketing is among the disciplines that provide critical insights to improve the effectiveness of nutrition actions. The Social Marketing approach involves the application of concepts and ideas of marketing theory to achieve behavior change in a beneficial direction for individuals and societies (Lee & Kotler, Citation2015). One of the key concepts of Social Marketing—and marketing in general—is segmentation. Segments or clusters are groups of individuals who share similar wants, needs, lifestyles, behaviors and values. Identification of meaningful segments in the target audience is pivotal for effective interventions because it allows for tailoring the message to the characteristics of specific groups (Luecking et al., Citation2017).
In the light of this, the present study focuses on identifying clusters of mothers in relation to personal, behavioral, and environmental factors acting as barriers to healthy eating. We believe that a culturally diverse sample has the potential to provide a broader understanding about mothers to the greatest extent.
Cross-cultural analysis: Choice of countries
Cross-cultural studies have the potential to maximize variation in observations compared to studies of single societies, thus improving intercultural validity of insights and theories (Ember, Citation2009; Takeda & Melby, Citation2017). This seems to be particularly the case for food and nutrition studies, since different cultural groups show significant diversity in healthy eating behaviors and attitudes to food (Orji & Mandryk, Citation2014; Rodríguez-Arauz et al., Citation2016).
To perform the present analysis, two European countries and one Latin American country were included because of their distinctive cultural and social settings and their different approaches to food and meals. France was selected due to the dominant role of food in the French culture, and Denmark was selected because of the cultural contrast in this aspect. The way people associate diet and health also varies in expression in these two countries. Whereas the French are inclined to define healthy eating more in terms of balance, variety and freshness (Rozin et al., Citation1999), the Northern Europeans associate food healthiness with animal welfare, hygiene and nutrition (Bergflødt et al., Citation2012).
Another reason why Denmark was deemed interesting for the analysis is due to the higher gender equality in the Scandinavian region. Argentina is a clear contrast to this aspect, as well as in the childhood obesity rates. Argentina ranks 77 in the gender equality rank, while France and Denmark rank 8 and 2 respectively (the lower in the rank the higher the gender equality) (United Nations, Citation2018). In regard to childhood obesity rates, Argentina has a prevalence of 21.7%, contrasting with France (10.4%) and Denmark (9%) (World Health Organization, Citation2017). Another interesting aspect about Argentina is the Southern European cultural trait inherent to Argentinian food culture, a result of the history of colonization. More than its neighboring countries, the majority of Argentines are descendants of European immigrants, primarily from Italy and Spain (Meehan & Katzman, Citation2001). Therefore, it seems valuable to exam attitudes and barriers to healthy eating among Argentinians in comparison to European countries.
Based on literature, we hypothesize that the importance attributed to food and meals (Fischler, Citation2011; Rozin et al., Citation1999), the food and culinary culture (Gatley et al., Citation2014; Saint-Pol, Citation2015) and gender (in)equality (Beagan et al., Citation2008; Bianchi et al., Citation2000; Calasanti & Bailey, Citation1991; Fielding-Singh, Citation2017; Kan et al., Citation2011) influence the barriers to healthy eating in the family food environment, and thus, are worth investigating in diverse cultural settings.
Methods
Survey development and content
The survey included statements based on empirical research on constraints to healthy eating in the family food environment, attitudes to nutrition advice and outcome expectations of healthy eating (each of the items and respective references are available as supplementary material). The statements covered barriers along the different phases of food provisioning, such as planning, purchasing, cooking (e.g., “I lack cooking skills to prepare healthy dishes”), also including division of housework (e.g., “When I do not feel like cooking, I can get my partner to do it”). Additionally, pre-established scales were included for other important constructs of the Social Cognitive Theory: general self-efficacy (Schwarzer, Citation1993), (subjective) knowledge (Flynn & Goldsmith, Citation1999) and health consciousness (Visschers et al., Citation2013). The final “Socio-cognitive measures of maternal barriers to healthy eating” consisted of 57 statements and is available as supplementary material. All items were rated on 7-point disagree-agree Likert-type scales.
The questionnaire has been previously translated to Danish and pre-tested with a sample of 267 Danish mothers (Moura & Aschemann-Witzel, Citation2022). For the other languages, translation was done by professional translators from the marketing agency which performed the data collection, the marketing agency Userneeds, https://userneeds.com/en/. Researchers in the field of families’ eating behaviors, who are native speakers in the corresponding languages (French and Spanish) and bilingual (English), checked the translated questionnaire for word and phrasing adequacy.
Data collection
Data collection was conducted by Userneeds in October 2020. The average respondent required 14 minutes to answer the survey. To increase the statistical power and reliability of the dataset, we established two exclusion criteria: answering the survey in less than five minutes (considered not enough time to read all the questions) and answering incorrectly the attention check question: “I like to find plastic in my food” (respondents who did not answer “strongly disagree” or “disagree” were excluded) (Oppenheimer et al., Citation2009). The attention check was not applied in Denmark due to the importance attributed to trust in the Danish culture. Professionals from the marketing agency experienced that attention checks decreased the engagement of Danish respondents, who would feel distrusted by the researchers. The study was approved by Aarhus University’s ethics committee (serial number: 2019–28).
The sample size of 500 mothers per country was pre-defined considering the median sample size commonly used in cluster analysis (Dolnicar, Citation2002). To meet eligibility requirements, panel members had to be mothers of at least one child aged up to four years old (preschoolers). This age range was identified as meaningful to perceived changes in healthy eating behaviors related to motherhood (Moura & Aschemann-Witzel, Citation2020). Quotas applied to the completed survey responses ensured that the sample represented the country in terms of region of residence.
Sample characteristics
presents the sample characteristics. The mean age of women in France corresponded to the mean age of French women at birth of first child (30.6 years old) (Eurostat, Citation2018). For Danish and Argentinian (from Buenos Aires) mothers, the mean age of 32.6 and 31 (respectively) approximated to the national mean age at birth of first child (31.2 years old in Denmark and 30.6 in Buenos Aires) (Eurostat, Citation2018; Ministerio de Hacienda, Citation2015).
Table 1. Mothers’ socio-demographic characteristics.
In the three countries, the majority of mothers had one or two children who were four years old or younger. The vast majority were living with a partner and had the primary responsibility for food-related activities in the household (except for Denmark where 50% of the mothers reported to be the main responsible). In regard to educational level, the Argentinian and Danish samples comprised 75% women with a university degree, whereas in France 57% of the respondents did not have a university degree. Only in Denmark, the majority of mothers were working full time. In each of the three countries, the majority of respondents considered their financial situation to be sufficiently good.
Data analysis
The analysis strategy followed three main steps as explained below. Considering the marked cultural and social differences between countries, statistical tests were performed for each country separately.
Factor analysis
We applied an exploratory factor analysis (common factor analysis with oblimin rotation) for all the 57 items. Exploratory factor analysis (EFA) is a technique employed to explain the common causes of correlated variables and to identify empirical regularities. Therefore, EFA is a recognized method for explanatory theory generation (Haig, Citation2005).
A country-by-country EFA showed only minor cross-country differences in the items correlational factor structure. We retained items if they a) loaded with at least 0.4 on any factor, or b) loaded unequivocally on one single factor (by a factor loading of at least 0.3) (Lanario et al., Citation2020). Furthermore, resulting factors were kept if they contained at least two items and showed a sufficient reliability with Cronbach’s alpha (0.5 or higher).
The factor analysis resulted in 56 items that emerged as pertaining to seven factors (factor loading values are available as supplementary material). Two of the factors consisted of the items from two different variables (Flynn & Goldsmith, Citation1999; Schwarzer & Jerusalem, Citation1995) which we decided to divide into two subscales to retain the theoretical distinctions.
The seven scales and two sub-scales were labeled as follows: 1.a) Barriers to healthy eating, 1.b) Subjective knowledge, 2) Low interest/enjoyment in cooking, 3) Family support, 4) Barriers at the workplace, 5) Negative opinions about nutrition advice, 6.a) Preferring own capabilities versus experts’ advice, 6.b) General self-efficacy, 7) Health consciousness and outcome expectations of healthy eating. Sampling adequacy for each item in the model and for the complete model was confirmed (KMO = .989, Bartlett’s Test of Sphericity p = .000).
Segment identification through cluster analysis
We conducted a latent class analysis with the identified factors, using the software package Latent Gold (Latent GOLD version 5.1 Statistical Innovations Inc., Belmont MA) to determine whether mothers could be segmented into specific groups. The cluster analysis was carried out for each country separately, on the grounds of the cross-cultural particularities potentially shaping the segments in different ways. The factors were treated as continuous variables. The cluster solution was chosen according to the most economical model measured by the lowest Bayesian Information Criterion (BIC value). This value is lower for less complex and therefore more economical models (Mathijssen et al., Citation2012).
presents the model comparison with one to six latent classes and the corresponding BIC values. The BIC statistic for the four-class model was slightly lower than for the other models in the three countries. The findings thus indicate that the four-cluster solution was the best fit. These four clusters were distinguished from each other by the seven identified factors.
Table 2. Model fit statistics for six latent cluster models.
Segment characterization
The identified segments were compared in their socio-demographic variables and in the perceived healthiness of eating (measured by the question: “How healthy do you think you eat?” answered in a 1–7 Likert scale from 1 = Very unhealthy to 7 = Very healthy).
Analyses of variance (ANOVA) were used to examine differences between segments in regard to factor scores and other continuous variables (mother’s age, age of the youngest and age of the oldest child). A Kruskal Wallis test was performed for the non-parametric variables (e.g., number of children per mother). A post hoc analysis was performed with Games-Howell tests (when variances were not homogeneous), with Scheffé tests (for homogeneous variances—homogeneity tested by Levene’s test) and Bonferroni test (for non-parametrical variables). Likert scales were treated as intervals.
With Pearson chi-square analyses (two-sided), we investigated whether the segments differed in variables at the nominal or ordinal measurement level (household status, educational level, employment status). Data were analyzed using SPSS 27.0.
Results
The results are structured as follows. First, we describe the identified segments country by country.
We particularly point to where one segment is significantly different from others (terms as highest/lowest refer to comparisons with the other three segments). Subsequently, we specify the most relevant factors for cluster distinction across countries.
In describing the segments, we have used the terminologies privileged/underprivileged, involved/uninvolved, and self-relied, because the clusters differed mainly in the respective dimensions: Socio-economic status (SES, identified by educational level and perceived financial situation), involvement with healthy eating (identified by interest in cooking, health consciousness, perceived healthiness of eating) and reliance on health experts’ advice (factor “Preferring own capabilities versus experts’ advice”). We acknowledge that the terminology “privileged/underprivileged” might be interpreted as somewhat stigmatizing. Nevertheless, considering the crucial role played by the socio-economic status in differing the clusters, we decided to keep the terminology as such.
Tables with scores for each dimension/factor per cluster in the three countries are available as supplementary material.
Segment characterization per country
Argentina
Segment 1: Uninvolved self-relied
This segment comprises of mothers who score the highest in general barriers to healthy eating (including barriers at the workplace). The uninvolved self-relied score the second lowest on subjective knowledge, the lowest on cooking enjoyment, the lowest reliance on nutrition experts and nutrition advice and the second lowest on health consciousness and outcome expectations of healthy eating. They also score the second lowest in perceived healthy eating. At the same time, the uninvolved self-relied emerge as the second highest in self-efficacy. Regarding socio-demographic profile, segment 1 mothers are the second most likely to do the housework themselves and report medium scores in university degree and financial situation.
Segment 2: Underprivileged advice seekers
Of all segments, mothers in segment 2 are characterized by the second highest score in barriers to healthy eating, the lowest subjective knowledge, second lowest cooking enjoyment, lowest self-efficacy, lowest health consciousness and outcome expectations of healthy eating. Conversely, they emerge as the highest reliant on health experts. Underprivileged advice seekers perceive to eat the least healthily and are the ones with the lowest educational level, lowest financial situation and are the less likely to work full time outside the home.
Segment 3: Privileged advice seekers
This cluster presents the second lowest scores on barriers to healthy eating, second highest in subjective knowledge, second highest cooking enjoyment, lowest family support, second lowest barrier in the workplace, second highest reliance on experts, second highest consciousness and outcome expectations of healthy eating. They score the second highest in the perception of healthiness of eating and are likely to be the main responsible for food-related activities. Socio-demographically, privileged advice seekers are further characterized by slightly older age, by being the second most likely to work full time outside the home, to have a better financial situation and the second highest educational level.
Segment 4: Modern privileged mothers
Segment 4 emerges with the lowest barriers to healthy eating, the highest subjective knowledge, cooking enjoyment, family support, self-efficacy, health consciousness and outcome expectations. They also score the second highest in barriers at the workplace and the second lowest reliance on experts. Modern privileged mothers are the ones who state to eat the healthiest and to share the household chores equally. In regard to socio-demographics, they are most likely to have a university degree, to work full time and to have the highest financial situation. Particularly, this group is distinct from the second lowest in barriers (segment 3, above) by younger age, higher education, higher earnings and more share of household chores (more modern patterns).
France
Segment 1: Uninvolved and constrained
This segment reports the highest scores in barriers to healthy eating (including barriers at the workplace), second lowest subjective knowledge, lowest cooking enjoyment, highest negative opinion about nutrition advice, second lowest reliance on health experts and second lowest self-efficacy. The uninvolved and constrained are the ones to state to eat less healthily. Regarding socio-demographic profile, mothers in this group are in the middle scores of educational level and financial situation.
Segment 2: Underprivileged self-relied
Segment 2 is characterized by the second highest score in barriers to healthy eating, second lowest subjective knowledge, second lowest cooking enjoyment, second highest negative opinion about nutrition advice, lowest reliance on nutrition experts, lowest health consciousness and outcome expectations and the second in stating to eat the least healthily among the four clusters. Concerning socio-demographic measures, underprivileged self-relied are characterized by a slightly higher number of children and being stay-at-home mothers. They also report the lowest on financial situation and university degree.
Segment 3: Cooking enthusiasts
The cooking enthusiasts emerge as the ones with the highest score in cooking enjoyment, second highest in subjective knowledge, second highest in positive opinion about nutrition advice, second highest self-efficacy. They are the second cluster in stating to eat the healthiest, the second most likely to work full time and the second highest in financial situation. Mothers in this group are likely to be younger.
Segment 4: Privileged and involved
Of all segments, the privileged involved report the lowest in barriers to healthy eating (including barriers at the workplace), the highest on subjective knowledge, the second highest cooking enjoyment, the highest family support, highest positive opinion about nutrition advice, second highest reliance on health experts, highest self-efficacy, and highest health consciousness and outcome expectations. Mothers in this cluster are also characterized by perceiving to eat the healthiest, the most likely to have a university degree, to work full time, to have the highest financial situation, and they tend to be slightly older.
Denmark
Segment 1: Uninvolved but receptive to advice
The uninvolved but receptive to advice report the highest barriers to healthy eating (including barriers at the workplace), the lowest subjective knowledge, lowest cooking enjoyment, lowest family support, lowest self-efficacy, lowest health consciousness and outcome expectations. Otherwise, they present the highest reliance on nutrition experts. Mothers in this cluster perceive to eat the least healthily and are more likely to do the household chores themselves. Regarding socio-demographic profile, they are characterized by a lower educational level and tend to be younger.
Segment 2: Uninvolved self-relied
Uninvolved self-relied mothers report the second lowest subjective knowledge, second lowest cooking enjoyment, highest negative opinion about nutrition advice, second lowest reliance on nutrition experts, second lowest self-efficacy, second lowest health consciousness and outcome expectation of healthy eating. They are also the second in stating to eat the least healthily. Concerning socio-demographic variables, mothers in this group are the only ones to differ significantly on (lower) financial status and the less likely to work outside the home.
Segment 3: Involved self-relied
Of all segments, segment 3 emerged as the second with lowest in barriers to healthy eating, the second highest in subjective knowledge, the second highest self-efficacy and second highest consciousness and outcome expectations. In contrast, they declare the lowest reliance on nutrition experts. The involved self-relied are also characterized by being second in perceiving to eat the healthiest and second in highest university degree.
Segment 4: Healthy eating enthusiasts
This cluster encompasses mothers with the lowest score on barriers to healthy eating (including barriers at the workplace), the highest subjective knowledge, highest cooking enjoyment, highest family support, highest positive opinion about nutrition advice, highest self-efficacy, highest consciousness and outcome expectations of healthy eating. Healthy eating enthusiasts relate to the healthiest eating, are more likely to share household activities with their partners, more likely to have a university degree, to work full time, to have the highest financial status and a slightly older age.
Country comparison
Comparing the 4-cluster solution and the characteristics across countries, some commonalities emerged (main characteristics per country can be visualized in ).
Figure 1. Segments and their characterization.
Note: The size of the circles represents the segment size and the colors indicate the comparison across countries.
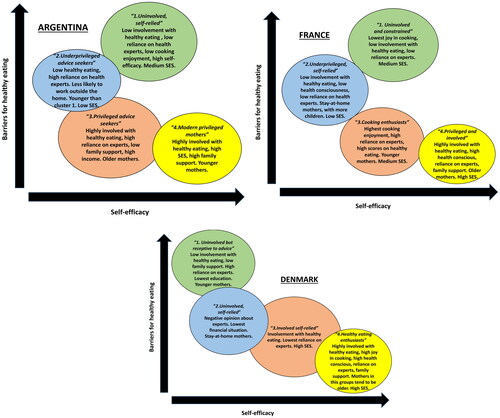
A comparable profile repeatedly surfacing is the healthy-eating-involved mother with high SES (segment 4: modern privileged mothers in Argentina, privileged and involved in France and healthy eating enthusiasts in Denmark). Across countries, they differ mostly by age (older in France and Denmark, but younger in Argentina).
A profile opposite to that emerged, composed by low healthy-eating-involved lower-SES mothers (segment 2: underprivileged advice seekers in Argentina, underprivileged self-relied in France and uninvolved, self-relied in Denmark). Respondents in this segment self-report eating less healthily and having the least interest in healthy eating (low scores on health consciousness and outcome expectations of healthy eating). Across countries, they differ by working status (stay-at-home mothers in France and Denmark) and reliance on nutrition experts (high reliance in Argentina, and low in the others).
Another segment to surface in the three countries is segment 1 which stands out with lowest scores on cooking enjoyment and low involvement in food and healthy eating. Particularly, low involvement for these mothers does not seem related to financial constraints or lower educational level. This profile differs between countries by self-efficacy (low in Denmark and France and high in Argentina) and on reliance on experts (high reliance only in Denmark).
Finally, a profile with less distinct characteristics is formed by mothers in segment 3. Respondents in segment 3 consider themselves to eat healthily and to have high health consciousness, but just not as much as segment 4. Their profile varies largely across the three countries (although in the three countries they report the second highest financial status). In Argentina, they are differentiated from the “most health involved” cluster by older age (also by potentially following older patterns like being fully responsible for household chores and having lower educational levels). In France, they stand out by the high joy of cooking, whereas in Denmark they are the “health involved ones” who tend not to rely on experts.
As exposed above, the cross-country observations pointed to marked differences in the clusters’ characteristics as well. When compared to each other, the characteristics of the segments in France and Denmark seem similar, whereas in Argentina it is slightly more distinct. For example, in Denmark and France there is a segment of stay-at-home mothers, which is absent in Argentina. In this regard, stay-at-home mothers tend to report more barriers to healthy eating and to be less involved in healthy eating (they are also likely to have a lower income).
In Argentina, the lowest SES mothers report a higher reliance on health experts. This contrasts with France, where low SES mothers are the ones to rely less on experts. In Denmark, educational level does not seem related to reliance on experts (mothers with lowest educational level in cluster 1 tend to rely on experts and so do mothers in cluster 4, the highest SES respondents).
Also in Argentina, mother’s slightly younger age appears to be a relevant factor for lower barriers (among higher SES mothers), whereas in Denmark it is the contrary (younger mothers indicate more barriers and less involvement with healthy eating).
Interestingly, higher self-efficacy for some clusters is related to a low reliance on nutrition advice from experts (cluster 1 in Argentina and cluster 3 in Denmark). In any case, self-efficacy seems an important factor for perceived high levels of healthy eating (although it does not stand alone as a determinant decreasing barriers). In Denmark and France, the higher the self-efficacy, the lower the barriers to healthy eating and the higher perception of eating healthily.
Discussion
Researchers aimed at investigating whether mothers of young children in three countries (Argentina, France and Denmark) could be segmented based on socio-cognitive barriers to healthy eating, and to which socio-demographic aspects these segments differ.
The present study is, to our knowledge, one of the few to consider individuals’ attitudes to nutrition advice and health experts as part of the investigation of eating behaviors. In this regard, Argentinians showed higher reliance on health professionals compared to the two other countries, especially among lower SES respondents. This finding is not surprising, since lower SES respondents might have fewer opportunities to learn and practice healthy eating and are inclined to seek information from experts. What is striking is the cross-country difference—lower SES mothers in the other two countries tended to rely the least on experts. Indeed, a certain distrust in health professionals has been previously identified among French and Danish mothers on the grounds of the complexity and contradiction of public nutrition messages and the conflict of interest in the public health domain (Moura & Aschemann-Witzel, Citation2021). Such a pattern of distrust among lower SES mothers might also be explained by the theory of cognitive dissonance (Festinger, Citation1957). Individuals may try to reduce dissonance (a feeling of discomfort caused by demands that are in conflict with own possibilities) by refuting recommendations that challenge their actual behaviors. The reason why such dissonance was found in the European countries, and not in the Latin American one, is an interesting issue to be investigated in further studies.
Another novelty of the present investigation is the finding that high self-efficacy levels can be related to low reliance on nutrition advice from experts, a relation that can only be identified in a segmentation approach. It seems that the more some mothers trust their own skills and capabilities, the less they seek for information from professionals. In other words, if you believe in your own capacities, you might tend to seek less information from others, which seems reasonable. However, high self-efficacy levels (combined with little reliance on experts) does not seem to be sufficient to decrease barriers to healthy eating. This implies that mothers might still benefit from nutrition counseling, but health professionals must consider and take into account individuals’ knowledge as central for the intervention.
In the three countries, women at risk of encountering more barriers to healthy eating are the ones with lower subjective knowledge, cooking enjoyment, educational levels, financial situation, and the ones who do not work outside the home. The fact that stay-at-home mothers report more barriers to healthy eating is remarkable, since they might have more time for food-related activities. However, working mothers report a higher budget and tend to have higher levels of education, which can explain the lower scores on barriers. Although the present study does not include information on children’s weight, the realization that stay-at-home mothers might face more barriers to healthy eating challenges the discourses pointing at the participation of women in the workforce as one of the causes for the rise in childhood obesity (De Brun et al., Citation2013; Maher et al., Citation2010).
The relation between lower scores on financial situation and educational levels (as well as on subjective knowledge, health consciousness, outcome expectations and cooking enjoyment) with lower self-declared healthy eating and more barriers is not surprising. Knowledge, health consciousness, outcome expectations, socio-economic status and education are directly associated with nutrition behaviors (Anderson et al., Citation2000; Petrovici & Ritson, Citation2006). The novelty of our results lies in the cooking enjoyment factor. Researchers have demonstrated the link between cooking skills and healthy eating behaviors (McGowan et al., Citation2017); however, the joy of cooking has been less explored by scholars and might be a factor worth addressing by health experts targeting families’ healthy eating.
Implications and recommendations
In this sub-section, we use the clusters characteristics to make suggestions for a targeted communication approach to help mothers overcome barriers to healthy eating.
Segment 1 and 2 in the three countries have the potential to benefit from an approach addressing all the social-cognitive factors of the study: subjective knowledge, cooking enjoyment, self-efficacy, family support, confidence in experts, health consciousness and outcome expectations. Self-efficacy can be improved by verbal persuasion, instructed performance, participating modeling and vicarious experience (learning with and from others) (Bandura, Citation1977). Hands-on culinary training with peers and the whole family, including experimental nutrition education, meal planning and cooking skills development are potential alternatives to build up self-efficacy for healthy eating and cooking enjoyment (Fulkerson et al., Citation2018; Harmon et al., Citation2015; Hasan et al., Citation2019). In the three countries, the sharing of household chores with the partner was related to fewer barriers to healthy eating, therefore the involvement of fathers in such tasks is crucial to increase their participation in food-related activities (increasing family support) and to reduce the burden on mothers (Calasanti & Bailey, Citation1991).
As for the French and Danish segment 2, the challenges faced by stay-at-home mothers should be considered. From the authors’ empirical analysis of a prior qualitative study (Moura & Aschemann-Witzel, Citation2020), Danish stay-at-home mothers indicate to have little or no help from their partners and families due to the very fact that they do not work outside the home. This lack of support might be responsible for the barriers to eating healthily faced by those mothers.
For segments 3 and 4 in all countries, objective measures of healthy eating should be applied to confirm healthy eating practices. There might be an opportunity to explore potential receptiveness of nutrition advice among some clusters. Once the actual healthiness of eating is confirmed (e.g., by a food frequency questionnaire), these clusters may benefit from reinforcement and feedback that confirm their successful approach to healthy eating (Prochaska et al., Citation2015).
As a final note, the results presented here highlight that individuals vary in their receptiveness and reliance on nutrition guidance (especially in the two European countries), and should therefore be approached with strategies that emphasize non-nutritional aspects of healthy eating (gastronomy of healthy foods and meals, for example). The segments which seem skeptical to nutrition advice may respond best to food-centered interventions (as opposed to nutrition-centered ones) (Poulain, Citation2009) and to strategies that alter the environment, such as nudging (Sunstein, Citation2014). Above all, health professionals must take into account clients’ prior knowledge focusing on a co-creation approach, where the client/patient remains at the center of the dietary decisions.
Limitations
As a limitation, socio-economic and cultural differences in the countries are expected to influence results and transferability of the findings to other contexts. In particular, the online nature of the survey might have prevented the participation of respondents in the lowest SES conditions (especially in Argentina and Denmark). Furthermore, the cross-sectional approach prevents us from inferring about a potential causal relationship between cluster membership and characteristics. Therefore, the findings need to be interpreted in light of the methodological bias. Objective measures of healthy eating patterns (as opposed to perception, although objective measures of dietary intake remain a challenge (Micha et al., Citation2018)) are needed to confirm the relation of the socio-cognitive barriers with actual (un)healthy eating patterns. In addition, a segmentation approach requires the researchers to make strategic decisions, especially in regard to the numbers of clusters considered adequate, which may affect the findings. Nevertheless, four profiles of consumers have been identified in previous research in Denmark (Kristensen et al., Citation2013) and France (Régnier & Masullo, Citation2009), which may indicate the present approach to be appropriate.
Conclusions
This study has identified clusters of mothers in relation to personal, behavioral, and environmental factors acting as barriers to healthy eating in three distinct countries (Argentina, France and Denmark). We have derived four profiles observed in the cross-country comparison and characterized these with regard to involvement with healthy eating and socio-demographics. The research contributes to a broader understanding of the constraints to healthy food provisioning among mothers in different statuses and contexts.
We conclude first that the different segments might be approached differently when it comes to working and socio-economic status, self-efficacy and attitudes to nutrition advice from health experts. Since working and socio-economic status are linked to differences in barriers to healthy eating, it might be possible to pre-identify mothers with higher levels of constraints by those aspects. Contrarily to current discourses, working mothers might have better preconditions for healthier eating behaviors.
Second, high levels of self-efficacy might be related to lower reliance on expert’s advice (for some profiles), and this may decrease involvement with healthy eating. In this regard, health professionals should be aware of a segment of mothers by whom nutrition advice is not well received, and might want to adapt nutrition counseling to a more co-creational food-focused approach.
Overall, we conclude that four segments with commonalities across the countries emerge. Thus, common constraints for healthy eating among mothers of young children appear to be to a certain extent generalizable in the three investigated countries (although Argentina stands alone in a few aspects).
Ultimately, findings imply that health professionals and authorities should adapt nutrition counseling and strategies to different profiles of mothers of young children.
Authors’ contributions
All authors conceptualized and contributed to the design of the study and were equally involved in the development of the survey. AFM collected and interpreted the data and wrote the first draft of the manuscript with contributions and substantial review from JAW. Both authors critically commented on subsequent versions of the article and have read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The study was approved by Aarhus University’s ethics committee (serial number: 2019-28).
Supplemental Material
Download MS Word (91.2 KB)Acknowledgements
The authors thankfully acknowledge the researchers who helped with the questionnaire translation: Gastón Ares and Leticia Vidal (Spanish), Sylvie Issanchou and Maartje Mulders (French). We also thank Pernille Nørgaard Videbaek and Violeta Stancu for the help with the analysis in Latent Gold, and Merete Elmann for the final language check of the article. Finally, we thank the Editor in Chief, Dr. Covan, and the anonymous reviewers for their constructive comments on the manuscript.
Availability of data and materials
Some of the data generated during this study are included in the article and its supplementary information file. Further datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Anderson, E. S., Winett, R. A., & Wojcik, J. R. (2000). Social-cognitive determinants of nutrition behavior among supermarket food shoppers: A structural equation analysis. Health Psychology, 19(5), 479–486. https://doi.org/10.1037/0278-6133.19.5.479
- Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215. [Database] https://doi.org/10.1037/0033-295X.84.2.191
- Bandura, A. (2002). Social cognitive theory in cultural context. Applied Psychology, 51(2), 269–290. https://doi.org/10.1111/1464-0597.00092
- Beagan, B., Chapman, G. E., D’Sylva, A., & Bassett, B. R. (2008). It’s just easier for me to do it’: Rationalizing the family division of foodwork. Sociology, 42(4), 653–671. https://doi.org/10.1177/0038038508091621
- Bergflødt, S., Amilien, V., & Skuland, S. E. (2012). Nordic food culture (s)-thoughts and perspectives by way of introduction. Anthropology of Food, S7. Retrieved from http://journals.openedition.org/aof/7296 https://doi.org/10.4000/aof.7296
- Bianchi, S. M., Milkie, M. A., Sayer, L. C., & Robinson, J. P. (2000). Is anyone doing the housework? Trends in the gender division of household labor. Social Forces, 79(1), 191–228. https://doi.org/10.2307/2675569
- Birch, L. L., & Anzman, S. L. (2010). Learning to eat in an obesogenic environment: A developmental systems perspective on childhood obesity. Child Development Perspectives, 4(2), 138–143. https://doi.org/10.1111/j.1750-8606.2010.00132.x
- Byrd-Bredbenner, C., Abbot, J. M., & Cussler, E. (2011). Relationship of social cognitive theory concepts to mothers’ dietary intake and BMI. Maternal & Child Nutrition, 7(3), 241–252. https://doi.org/10.1111/j.1740-8709.2009.00232.x
- Calasanti, T. M., & Bailey, C. A. (1991). Gender inequality and the division of household labor in the United States and Sweden: A socialist-feminist approach. Social Problems, 38(1), 34–53. https://doi.org/10.2307/800637
- De Brun, A., McCarthy, M., McKenzie, K., & McGloin, A. (2013). “Fat is your fault”. Gatekeepers to health, attributions of responsibility and the portrayal of gender in the Irish media representation of obesity. Appetite, 62, 17–26.
- Dolnicar, S. (2002). A review of unquestioned standards in using cluster analysis for data-driven market segmentation. Retrieved 2021, September 8, from https://ro.uow.edu.au/commpapers/273.
- Elliott, S., & Bowen, S. (2018). Defending motherhood: Morality, responsibility, and double binds in feeding children. Journal of Marriage and Family, 80(2), 499–520. https://doi.org/10.1111/jomf.12465
- Ember, C. R. (2009). Cross-cultural research methods (2nd ed.). Rowman Altamira.
- Eurostat (2018). Mean age of women at childbirth and at birth of first child. Retrieved 2020 Nov 10, from https://ec.europa.eu/eurostat/databrowser/view/tps00017/default/table?lang=en.
- Festinger, L. (1957). A theory of cognitive dissonance (Vol. 2): Stanford University Press.
- Fielding-Singh, P. (2017). Dining with dad: Fathers’ influences on family food practices. Appetite, 117, 98–108. https://doi.org/10.1016/j.appet.2017.06.013
- Fischler, C. (2011). Commensality, society and culture. Social Science Information, 50(3–4), 528–548. https://doi.org/10.1177/0539018411413963
- Flynn, L. R., & Goldsmith, R. E. (1999). A short, reliable measure of subjective knowledge. Journal of Business Research, 46(1), 57–66. https://doi.org/10.1016/S0148-2963(98)00057-5
- Fulkerson, J. A., Friend, S., Horning, M., Flattum, C., Draxten, M., Neumark-Sztainer, D., Gurvich, O., Garwick, A., Story, M., & Kubik, M. Y. (2018). Family home food environment and nutrition-related parent and child personal and behavioral outcomes of the Healthy Home Offerings via the Mealtime Environment (HOME) Plus program: A randomized controlled trial. Journal of the Academy of Nutrition and Dietetics, 118(2), 240–251. https://doi.org/10.1016/j.jand.2017.04.006
- Gatley, A., Caraher, M., & Lang, T. (2014). A qualitative, cross cultural examination of attitudes and behaviour in relation to cooking habits in France and Britain. Appetite, 75, 71–81.
- Haig, B. D. (2005). Exploratory factor analysis, theory generation, and scientific method. Multivariate Behavioral Research, 40(3), 303–329. https://doi.org/10.1207/s15327906mbr4003_2
- Harmon, B. E., Smith, N., Pirkey, P., Beets, M. W., & Blake, C. E. (2015). The impact of culinary skills training on the dietary attitudes and behaviors of children and parents. American Journal of Health Education, 46(5), 283–292. https://doi.org/10.1080/19325037.2015.1056862
- Hasan, B., Thompson, W. G., Almasri, J., Wang, Z., Lakis, S., Prokop, L. J., Hensrud, D. D., Frie, K. S., Wirtz, M. J., Murad, A. L., Ewoldt, J. S., & Murad, M. H. (2019). The effect of culinary interventions (cooking classes) on dietary intake and behavioral change: A systematic review and evidence map. BMC Nutrition, 5(1), 29. https://doi.org/10.1186/s40795-019-0293-8
- Johansson, B., Ossiansson, E., Dreas, J. A., & Mårild, S. (2013). Proper food and a tight budget: German and Swedish parents reflecting on children, food and health. Food, Culture & Society, 16(3), 457–477. https://doi.org/10.2752/175174413X13673466711921
- Kan, M. Y., Sullivan, O., & Gershuny, J. (2011). Gender convergence in domestic work: Discerning the effects of interactional and institutional barriers from large-scale data. Sociology, 45(2), 234–251. https://doi.org/10.1177/0038038510394014
- Kristensen, D. B., Askegaard, S., & Jeppesen, L. H. (2013). If it makes you feel good it must be right’: Embodiment strategies for healthy eating and risk management. Journal of Consumer Behaviour, 12(4), 243–252. https://doi.org/10.1002/cb.1427
- Lanario, J. W., Hyland, M. E., Menzies-Gow, A., Mansur, A. H., Dodd, J. W., Fowler, S. J., Jones, R. C., & Masoli, M. (2020). Validation of subscales of the Severe Asthma Questionnaire (SAQ) using exploratory factor analysis (EFA). Health and Quality of Life Outcomes, 18(1), 1–10. Retrieved from https://doi.org/10.1186/s12955-020-01593-9
- Lee, N. R., & Kotler, P. (2015). Social marketing: Changing behaviors for good (5th ed.). Sage Publications.
- Luecking, C. T., Hennink-Kaminski, H., Ihekweazu, C., Vaughn, A., Mazzucca, S., & Ward, D. S. (2017). Social marketing approaches to nutrition and physical activity interventions in early care and education centres: A systematic review. Obesity Reviews, 18(12), 1425–1438. https://doi.org/10.1111/obr.12596
- Maher, J., Fraser, S., & Wright, J. (2010). Framing the mother: Childhood obesity, maternal responsibility and care. Journal of Gender Studies, 19(3), 233–247. https://doi.org/10.1080/09589231003696037
- Mathijssen, J., Janssen, M., van Bon-Martens, M., & van de Goor, I. (2012). Adolescents and alcohol: an explorative audience segmentation analysis. BMC Public Health, 12(1), 742.
- McGowan, L., Caraher, M., Raats, M., Lavelle, F., Hollywood, L., McDowell, D., Spence, M., McCloat, A., Mooney, E., & Dean, M. (2017). Domestic cooking and food skills: A review. Critical Reviews in Food Science and Nutrition, 57(11), 2412–2431. https://doi.org/10.1080/10408398.2015.1072495
- Meehan, O. L., & Katzman, M. A. (2001). Argentina: The social body at risk. In M. Nasser, M. A. Katzman, & R. Gordon (Eds.), Eating disorders and cultures in transition (pp. 148–162). Brunner Routledge.
- Micha, R., Coates, J., Leclercq, C., Charrondiere, U. R., & Mozaffarian, D. (2018). Global dietary surveillance: Data gaps and challenges. Food and Nutrition Bulletin, 39(2), 175–205.
- Ministerio de Hacienda. (2015). La fecundidad en la Ciudad Autónoma de Buenos Aires: situación al año 2015. Retrieved from https://www.estadisticaciudad.gob.ar/eyc/wp-content/uploads/2017/01/ir_2017_1100.pdf
- Moura, A. F., & Aschemann-Witzel, J. (2020). A downturn or a window of opportunity? How Danish and French parents perceive changes in healthy eating in the transition to parenthood. Appetite, 150, 104658. https://doi.org/10.1016/j.appet.2020.104658
- Moura, A. F., & Aschemann-Witzel, J. (2021). Perspectives on sugar consumption expressed on social media by French-speaking and Danish-speaking parents. Social Science & Medicine (1982), 270, 113636.
- Moura, A. F., & Aschemann-Witzel, J. (2022). Barriers to healthy eating: a theory-driven questionnaire for mothers of young children [Manuscript submitted for publication]. Department of Management, Aarhus University.
- Oppenheimer, D. M., Meyvis, T., & Davidenko, N. (2009). Instructional manipulation checks: Detecting satisficing to increase statistical power. Journal of Experimental Social Psychology, 45(4), 867–872. https://doi.org/10.1016/j.jesp.2009.03.009
- Orden, A. B., Bucci, P. J., & Petrone, S. (2013). Trends in weight, height, BMI and obesity in schoolchildren from Santa Rosa (Argentina), 1990–2005/07. Annals of Human Biology, 40(4), 348–354. https://doi.org/10.3109/03014460.2013.778329
- Orji, R., & Mandryk, R. L. (2014). Developing culturally relevant design guidelines for encouraging healthy eating behavior. International Journal of Human-Computer Studies, 72(2), 207–223. https://doi.org/10.1016/j.ijhcs.2013.08.012
- Petrovici, D. A., & Ritson, C. (2006). Factors influencing consumer dietary health preventative behaviours. BMC Public Health, 6(1), 222.
- Poulain, J.-P. (2009). Sociologie de l’obésité [Sociology of Obesity]. Presses universitaires de France.
- Prochaska, J. O., Redding, C. A., & Evers, K. E. (2015). The transtheoretical model and stages of change. In K. Glanz, B. Rimer, & K. Viswanath (Eds.), Health behavior: Theory, research, and practice (5th ed., Vol. 97). Jossey-Bass.
- Régnier, F., & Masullo, A. (2009). Obésité, goûts et consommation. Revue Française de Sociologie, 50(4), 747–773. https://doi.org/10.3917/rfs.504.0747
- Rodríguez-Arauz, G., Ramírez-Esparza, N., & Smith-Castro, V. (2016). Food attitudes and well-being: The role of culture. Appetite, 105, 180–188. https://doi.org/10.1016/j.appet.2016.05.019
- Rozin, P., Fischler, C., Imada, S., Sarubin, A., & Wrzesniewski, A. (1999). Attitudes to food and the role of food in life in the USA, Japan, Flemish Belgium and France: Possible implications for the diet–health debate. Appetite, 33(2), 163–180.
- Saint-Pol, T. (2015). Déterminants sociaux et culturels de l’alimentation. In Institut national de la santé et de la recherche médicale (Inserm) (Ed.), Inégalités sociales de santé en lien avec l’alimentation et l’activité physique (1st ed., pp. 217–235). Pôle expertise collective ITMO Santé Publique, Aviesan.
- Schwarzer, R. (1993). Measurement of perceived self-efficacy: Psychometric scales for cross-cultural research. Freie Universität Berlin, Instituit fúr Psychologie.
- Schwarzer, R., & Jerusalem, M. (1995). Generalized self-efficacy scale. In J. Weinman, S. Wright, & M. Johnston (Eds.), Measures in health psychology: A user’s portfolio. Causal and control beliefs (Vol. 1, pp. 35–37). NFER-Nelson.
- Sunstein, C. R. (2014). Nudging: a very short guide. Journal of Consumer Policy, 37(4), 583–588. https://doi.org/10.1007/s10603-014-9273-1
- Takeda, W., & Melby, M. K. (2017). Spatial, temporal, and health associations of eating alone: A cross-cultural analysis of young adults in urban Australia and Japan. Appetite, 118, 149–160. https://doi.org/10.1016/j.appet.2017.08.013
- United Nations. (2018). Human Development Reports. Table 5: Gender Inequality Index. United Nations Development Program. Retrieved 2020 October 15, from. http://hdr.undp.org/en/composite/GII.
- Visschers, V. H., Hartmann, C., Leins-Hess, R., Dohle, S., & Siegrist, M. (2013). A consumer segmentation of nutrition information use and its relation to food consumption behaviour. Food Policy. 42, 71–80. https://doi.org/10.1016/j.foodpol.2013.07.003
- World Health Organization. (2016a). Global Strategy on Diet, Physical Activity and Health: Childhood overweight and obesity. Retrieved 2018, February 18, from https://www.who.int/dietphysicalactivity/childhood/en/.
- World Health Organization. (2016b). Report of the commission on ending childhood obesity. World Health Organization.
- World Health Organization. (2017). Prevalence of obesity among children and adolescents. Global Health Observatory data repository. Global Health Observatory data repository. Retrieved 2019, July 20, from http://apps.who.int/gho/data/view.main.BMIPLUS2C05-09v?lang=en.
- Wright, J., Maher, J., & Tanner, C. (2015). Social class, anxieties and mothers’ foodwork. Sociology of Health & Illness, 37(3), 422–436.