
Abstract
Expanding access to facility-based delivery services and improving the functionality of emergency obstetric and neonatal care (EmONC) are important strategies toward achieving a maternal mortality ratio of 70 deaths per 100,000 live births by 2030. In this study the researchers assess signal functions at designated facilities in Nepal, using Nepal Health Facility Survey data for 2015 and 2021. The functionality of basic and comprehensive EmONC sites was low, declining over the six-year period. Lack of progress may partly be attributed to the COVID-19 pandemic. Nepal needs to expand EmONC sites strategically, strengthen referral systems, improve service readiness, and periodically assess service quality.
Maternal mortality reduction remains a global priority. According to an estimate for 2020, globally, one woman died every two minutes, 800 women died every day, and 287,000 women died in the year due to pregnancy-related causes (World Health Organization [WHO], Citation2023). The United Nations Sustainable Development Goal (SDG) 3.1 targets reducing the global Maternal Mortality Ratio (MMR) to 70 maternal deaths per 100,000 live births, but in 2020, the MMR was 223 maternal deaths per 100,000 live births. To achieve the target, an annual reduction rate of 11.6% between 2021 and 2030 will be required (WHO, Citation2023). Low- and middle-income countries (LMICs) contribute to 95% of these global maternal deaths, and meeting this target is challenged by fragile health systems and a lack of adequate resources. Expanding access to health facility (HF)-based obstetric services during pregnancy, delivery, and the postpartum period and improving service quality at HFs are important strategies to ensure maternal survival in LMICs.
In this paper, we present the case of Nepal, a LMIC in South Asia, to demonstrate why expanding access to HF-based delivery services and improving the functionality of emergency obstetric and neonatal care (EmONC) sites should be prioritized for maternal death reduction. The authors intend to contribute to global learning as well as improve programs and practices in LMICs on quality maternal health care service provision for women within the purview of the SDG 3.1 target of 70 MMR by 2030.
Background
Globally, the majority of maternal deaths are due to obstetric complications, and around fifteen percent of pregnancies result in obstetric complications. These require implementing certain medical interventions known as “signal functions” for EmONC at HFs (WHO, Citation2009). Therefore, having accessible and functional basic EmONC (BEmONC) or comprehensive EmONC (CEmONC) services in HFs providing delivery services is essential for maternal survival. The World Health Organization (WHO) identifies seven and nine signal functions for BEmONC and CEmONC services, respectively, as summarized in .
Table 1. Signal functions for BEmONC and CEmONC services.
Maternal mortality and emergency obstetric and newborn care services in Nepal
The MMR decreased significantly in Nepal over the past 25 years, from 539 to 151 deaths per 100,000 live births between 1996 and 2021 (MOHP et al., Citation2023; MOHP & National Statistics Office [NSO], Citation2023). Nepal continues to strive toward achieving the SDG target 3.1, which calls for a reduction in the MMR to 70 per 100,000 live births by 2030. With the nation-wide implementation of the Maternity Incentive Scheme, the Aama Program, which ensures free delivery services in HFs, and a transportation allowance for women seeking antenatal and delivery services at HFs, Nepal has made significant improvements in access to and utilization of HF-based delivery services. In 2021, 98.4% of HFs in Nepal provided antenatal care services, 51.4% provided normal low-risk delivery services, and 5.3% provided cesarean services. The population coverage of HF-based delivery services increased from 44.0% in 2011 to 79.4% in 2022 (MOHP et al., Citation2023). However, these improvements in access and coverage have not translated into corresponding improvements in meeting the standards of care for delivery and emergency obstetric services at HFs. For example, in 2021, the five essential medicines for delivery services (oxytocin, injectable antibiotics, skin antiseptic, intravenous fluid, and magnesium sulfate) were available in only 20.2% of HFs providing normal low-risk delivery services, and a skilled birth attendant was present during only 31.0% of the deliveries; similarly, when taking the pregnancy history, the provider asked about vaginal bleeding in only 47.5% of the pregnant women, and the temperature of oxytocin was maintained during only one-third (65.5%) of the deliveries (MOHP et al., Citation2022). When standards of care are not met during delivery, service quality is compromised, which increases the risk of complications for both mothers and newborns. At present, the biggest challenge to achieving further maternal mortality reductions in Nepal is the suboptimal quality of obstetric care in HFs.
In 2021, over three-fifths of maternal deaths in Nepal occurred at HFs (MOHP & NSO, Citation2023); two-thirds of them happened during delivery and the postpartum period, and the major causes of these deaths were obstetric hemorrhage, hypertensive diseases, and infections (MOHP et al., 2023), all of which require management based on signal functions. The Government of Nepal (GON) has designated HFs providing delivery services as EmONC, BEmONC, and CEmONC sites to provide equitable access to the signal functions for pregnant women across the country (Family Welfare Division [FWD], Citation2019). EmONC sites in Nepal provide the first three signal functions, and they generally comprise Basic Health Care Centers (BHCCs) and other lower-level HFs. BEmONC services are provided by Primary Health Care Centers (PHCCs), and CEmONC services are provided by hospitals. During the Millennium Development Goal period, Nepal emphasized reducing maternal deaths by formulating policies to address barriers and implementing high impact interventions. As a result, BEmONC and CEmONC site expansion accelerated, which continued during the SDG period. In 2022, there were 226 designated CEmONC sites and 2,275 EmONC and BEmONC sites in Nepal, which include both public and private HFs (Department of Health Services [DOHS], Citation2023). The GON plans to ensure 24/7 availability of EmONC services, increase the number of CEmONC sites to cover all 77 districts, fully functionalize the BEmONC sites, and strengthen referral systems, including ambulances, means of communication, and linkages with pre-identified, fully functional CEmONC sites (FWD, Citation2019). However, optimal infrastructure, staffing, equipment, referral, and finance continue to be a challenge for the operation of the different EmONC sites.
After the promulgation of the Constitution in 2015, and Nepal’s transition to a federalized government structure in 2017, the 753 local governments are mandated to provide basic health services free of charge to Nepali citizens, including normal low-risk delivery services. In addition, the national Maternity Incentive Scheme ensures free delivery services to Nepali women, including EmONC, BEmONC, and CEmONC services (FWD, Citation2019). However, designating HFs as EmONC, BEmONC, and CEmONC sites and increasing the number of service sites does not necessarily ensure the routine availability of high-quality obstetric services. It is therefore important to assess the functionality of these EmONC, BEmONC, and CEmONC sites, which entails that the HFs are equipped to manage complications and provide the signal functions on time and as per the service standards. Evidence suggests that availability and use of EmONC can reduce maternal mortality by 85% and perinatal mortality by more than 75% (Darmstadt et al., Citation2005; Bhutta et al., Citation2008; Pasha et al., Citation2010; Pattinson et al., Citation2011) and effective BEmONC can prevent up to 40% of intrapartum neonatal and maternal mortality (Lee et al., Citation2011). In this context, our study examines the availability and functionality of the seven BEmONC and nine CEmONC signal functions at the designated sites in Nepal, compares the changes between 2015 and 2021, and provides important learnings that could be useful to other LMICs facing similar health system challenges in reducing maternal deaths.
Methods
Data source and data collection
We used data from the nationally representative, cross-sectional Nepal Health Facility Survey (NHFS) implemented in 2015 and 2021 (MOH et al., Citation2016; MOHP et al., Citation2022) under the global Demographic and Health Survey (DHS) Program. These surveys assessed public and private HFs regarding their availability and readiness to provide basic health care services and examined the process and experience of care for selected basic services. The data from these surveys is publicly available at https://dhsprogram.com/Data/.
In both NHFSs, individuals with public health, nursing, or medical qualifications were recruited as field researchers who received four weeks of training on NHFS implementation and collected data from the interviews with the HF manager and other service providers. Interviews were validated by observations. In the NHFS, a standard Service Provision Assessment (SPA) DHS tool was adapted for Nepal, and data was collected using computer-assisted personal interviews (MOH et al., Citation2016; MOHP et al., Citation2022). We analyzed data from the delivery and newborn care service module of the NHFSs, which includes an assessment of delivery service availability and readiness using the HF inventory tool. This module also includes interviews with the providers at a given HF about whether their HF is a designated BEmONC or CEmONC service site.
Sample size and weights
We analyzed a subset of the NHFS 2015 and 2021 data. In the NHFS, designated BEmONC and CEmONC service sites were oversampled, with all of them being included in the sample; in addition, to make our analysis representative of designated BEmONC and CEmONC sites overall in Nepal, we used weights, which corrected for the oversampling of the designated BEmONC and CEmONC HFs as well as any non-response. The weighted data included 26 BEmONC and 21 CEmONC sites in 2015, and 43 BEmONC and 52 CEmONC sites in 2021.
Variables
Signal function availability and functionality: In , we describe how the availability and functionality of each of the signal functions were calculated.
Table 2. Definition and measurement of variables.
We define BEmONC and CEmONC service availability as the relevant signal functions having ever been performed by the service providers at a designated BEmONC or CEmONC site. Based on the interviews with the service providers, categorical variables assess whether each of seven BEmONC and each of nine CEmONC signal functions have ever been performed by the service providers (coded 1) or have never been performed by the service provider (coded 0) across the health facility to measure availability. Overall BEmONC or CEmONC service availability is assessed through a composite index, which is coded as 1 when all relevant signal functions were available (and 0 otherwise).
We define BEmONC and CEmONC service functionality as the relevant signal functions having been performed at a designated BEmONC or CEmONC site during the three months prior to data collection. Based on the interviews with service providers, categorical variables designate whether each of the relevant signal functions have been performed by the service providers over the relevant time period. Overall BEmONC or CEmONC service functionality is assessed through a composite index, which is coded as 1 when all relevant signal functions have been put into practice during the three months prior to data collection (and 0 otherwise).
Health facility characteristics: We used “managing authority” (public, private) and “HF types” (hospitals, PHCCs, BHCCs) as categorical variables to describe the characteristics of HFs.
Statistical analysis
We conducted (weighted) descriptive analyses, relating designated BEmONC and CEmONC sites to the managing authority and the type of HF. However, we did not disaggregate subsequent analyses by the managing authority and by HF types due to the small sample size of the private HFs (hospitals), and the BHCCs, respectively. To analyze gaps in BEmONC and CEmONC signal function availability and functionality in each of the survey years, we calculated the weighted mean (i.e., the weighted percentage) of BEmONC and CEmONC availability and functionality in 2015 and 2021. We carried out a weighted independent sample t-test to calculate the (weighted) mean difference in BEmONC and CEmONC availability and functionality between 2015 and 2021, with a level of significance of 0.05 and presenting the corresponding 95% confidence interval (CI) for the mean difference. We used Statistical Package for Social Science (SPSS) software, IBM SPSS Statistics 25, for all analyses.
Ethical approval
Both NHFS 2015 and 2021 were approved by the Nepal Health Research Council (NHRC). Our study was approved by the NHRC and Ludwig-Maximilians-Universität München (LMU Munich) Ethics Commission, Munich, Germany, in 2021.
Results
Distribution of the designated BEmONC and CEmONC sites by managing authority and HF types
We present to show the weighted distribution of designated BEmONC and CEmONC sites by managing authority and HF type in 2015 and 2021. For both years, we found that in Nepal, BEmONC sites were almost exclusively public HFs. In contrast, 50.0% of CEmONC sites in 2021 were public, fewer than in 2015 (63.8%). In 2015, all but one of the BEmONC sites were hospitals or PHCCs, but in 2021, 12 BEmONC sites (27.9%) were BHCCs. In 2015, all public CEmONC sites were hospitals; in 2021, one public CEmONC site was a PHCC.
Table 3. Weighted distribution of designated CEmONC and BEmONC sites in the total samples of NHFS 2015 and 2021.
Changes in availability and functionality of signal functions at BEmONC sites
We present to demonstrate the changes in the availability and functionality of the seven signal functions at the designated BEmONC sites over time. In both years, the availability of assisted vaginal delivery scored lowest (54.4% in 2015 and 28.5% in 2021) and administration of parenteral oxytocin scored highest (97.6% in 2015 and 89.5% in 2021), also indicating a declining trend. While the availability of two signal functions—administration of parenteral anticonvulsants and removal of retained products of conception—improved, it regressed for the other five signal functions.
Figure 1. (a) Availability of signal functions at BEmONC sites in 2015 and 2021. (b) Functionality of signal functions at BEmONC sites in 2015 and 2021.
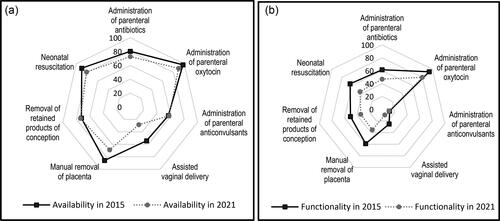
Overall, we found functionality was lower than availability, with the lowest functionality observed for the administration of parenteral anticonvulsants in 2015 (11.8%) and for assisted vaginal delivery in 2021 (9.0%). The administration of parenteral oxytocin was highest in both years but showed a declining trend (93.7% in 2015 and 79.9% in 2021). The functionality of all seven signal functions had decreased in 2021, but the decline was statistically significant only for assisted vaginal delivery (54.4% in 2015; 28.5% in 2021). We have reported the distribution of BEmONC sites by mean of signal function availability and functionality and 95% CI of the mean difference in Nepal in 2015 and 2021 in Supplementary Table A.
Low signal function availability and functionality and declining trends between the two time points are indicative of limited HF preparedness to provide the relevant service. This may place pregnant women and their newborns at high risk during obstetric complications.
In , we present the difference between signal functions available and functional at the designated BEmONC sites in 2015 and 2021. Overall, the gap between availability and functionality of the signal functions was 25.3% in 2015, and 13.7% points in 2021. In both years, the gap in availability and functionality was widest for the administration of parenteral anticonvulsants (44.8% in 2015 and 46.5% in 2021) and narrowest for the administration of parenteral oxytocin (3.9% in 2015 and 9.6% in 2021).
Table 4. Distribution of BEmONC sites by difference in signal functions availability and functionality in Nepal in 2015 and 2021.
Changes in availability and functionality of signal functions at CEmONC sites
In we present changes in the availability and functionality of the nine signal functions at the designated CEmONC sites between 2015 and 2021. In 2015, blood transfusion was the most available (93.9%) and administration of parenteral anticonvulsants was the least available (75.1%) signal function, whereas in 2021, cesarean delivery (98.9%) and assisted vaginal delivery (85.7%) were the most and least available, respectively. Overall, this indicates improvements in the availability of signal functions. We found the largest improvement of 12.5% points and the smallest improvement of only 1.7% points for the administration of parenteral anticonvulsants and the administration of parenteral oxytocin, respectively.
Figure 2. (a) Availability of signal functions at CEmONC sites in 2015 and 2021. (b) Functionality of signal functions at CEmONC sites in 2015 and 2021.
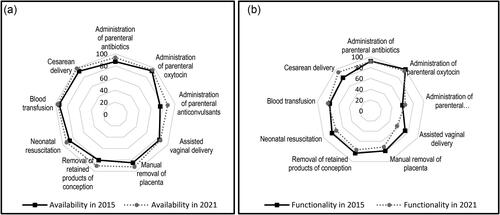
In 2015, we observed the lowest (59.7%) functionality for administration of parenteral anticonvulsants and 100% functionality for administration of parenteral oxytocin. In contrast, in 2021, we found the lowest (56.2%) functionality for assisted vaginal delivery while administration of parenteral oxytocin continued to be the most functional (96.5%) signal function. Functionality of three signal functions—cesarean delivery, parenteral administration of anticonvulsants, and blood transfusion—increased by 13.1%, 5.0%, and 3.4% points, respectively. Contrastingly, the remaining six signal functions decreased over the same time period. We observed the greatest decline of 17.3% points for assisted vaginal delivery.
These results highlight uneven progress across the different CEmONC signal functions, with improvements in functionality lagging behind improvements in availability. We reported the distribution of CEmONC sites by mean of signal function availability and functionality and 95% CI of the mean difference in Nepal in 2015 and 2021 in Supplementary Table B.
We present to show gaps between the availability and functionality of CEmONC signal functions at the two time points. Overall, the gap between signal functions available and functional was 26.1% points in 2015, increasing to 42.2% points in 2021. The gap was not uniform across the nine signal functions, with blood transfusion (17%) and assisted vaginal delivery (29.5%) having the widest gaps in 2015 and 2021, respectively. In contrast, the removal of retained products of conception (3.1%) and the administration of parenteral oxytocin (1.1%) presented the narrowest gaps in 2015 and 2021, respectively.
Table 5. Distribution of CEmONC sites by difference in signal functions availability and functionality in Nepal in 2015 and 2021.
Discussion
Key findings and locating them in the literature
Expanding access to skilled birth attendants, HF-based obstetric services, and improving the functionality of EmONC are important strategies toward achieving the maternal mortality reduction goal. Nepal adopted improving access to functional BEmONC and CEmONC sites as a key strategy to improve maternal survival. There are abundant publications on the functionality of EmONC sites in LMICs, but this is the first study of its kind in Nepal, assessing signal function availability and functionality using nationally representative samples of HFs. Over the six-year period between 2015 and 2021, both the availability and functionality of signal functions at the BEmONC sites declined. In contrast, the availability of signal functions at the CEmONC sites increased considerably, but the overall functionality of the signal functions at the CEmONC sites did not improve and, in some cases, declined. Of the nine CEmONC signal functions, only three—cesarean deliveries, parenteral administration of anticonvulsants, and blood transfusion—improved functionality over the two time points.
The decline in functionality of both BEmONC and CEmONC sites in Nepal may in part be explained by the health system challenges posed by the coronavirus disease (COVID)-19 pandemic. During most of 2020 and 2021, due to lockdowns, HFs were closed, or services were limited. Even when HFs were open, pregnant women were hesitant to visit them due to fear of contracting COVID-19, thereby lowering service utilization rates (Management Division [MD], Citation2021; Kc et al., Citation2020). The pandemic also affected the supply chain system, resulting in stockouts of essential commodities at HFs, limited in-person trainings, a lack of clinical guidelines and protocols at HFs, and limited monitoring and supervision. Support for HFs was provided remotely, and the focus was mainly on mitigating the direct effects of COVID-19. The impact of COVID-19 on maternal deaths in Nepal is reported in a 2021 nationally representative maternal mortality study based on verbal autopsies, where nearly 15% of the deceased women were reported to be infected with the coronavirus (MOHP & NSO, Citation2023). Several LMICs faced similar challenges during the pandemic. A study from Bangladesh, Nigeria, and South Africa published in 2021 reports a reduction in utilization of antenatal care, family planning, and immunization due to the implementation of lockdowns, a shift of focus toward the pandemic causing detriment to other health services, and resource constraints (Ahmed et al., Citation2021). Another study published in 2021 analyzed data from 37 non-governmental organization-supported HFs in Haiti, Lesotho, Liberia, Malawi, Mexico and Sierra Leone. It reported significant declines in first antenatal care visits in Haiti (18% drop) and Sierra Leone (32% drop), as well as fewer HF deliveries in all countries except Malawi during the pandemic (Aranda et al., Citation2022)
Studies across LMICs show that the availability and functionality of BEmONC and CEmONC services are generally low. In our study, the full performance of all seven BEmONC signal functions was less than five percent at both time points, which is comparable to Ghana (4.8%) but somewhat higher than in India, where no single BEmONC site performed full signal functions in a study published in 2023 (Gausman et al., Citation2023). Similarly, in our study, 35.2% and 27.9% of the CEmONC sites in 2015 and 2021, respectively, showed full CEmONC performance, which is relatively high compared to the performance reported for Argentina (8.8%) and India (23.1%), but was lower than in Ghana, where 57.1% of the sites performed full CEmONC functions in 2023 (Gausman et al., Citation2023). The availability of assisted vaginal delivery and parenteral administration of anticonvulsants performed the least amongst the signal functions in both BEmONC and CEmONC-designated sites in both years, which is comparable to the findings from a recent study in Bangladesh where assisted vaginal delivery was the least-available signal function, offered by about 35% of district hospitals, and parenteral anticonvulsants were scarcely available, ranging between 11% and 62% across HF types (Roy et al., Citation2017).
The poor performance of assisted vaginal delivery services with a declining trend between 2015 and 2021 in Nepal could be due to an increase in cesarean delivery, which had the highest availability (above 90%) and functionality (above 79%) in both years amongst the nine CEmONC signal functions. Nationally, the availability of cesarean services at HFs remained stable, 5.1% in 2015 and 5.3% in 2021 (MOHP et al, 2022), but the population coverage for cesarean deliveries almost doubled from 9.0% in 2016 to 18.3% in 2022 (MOHP et al., Citation2023). A study from Ethiopia published in 2021 reports that between 2011 and 2016, the assisted vaginal delivery rate declined from 15.8% to 9.9%, while the cesarean section rate increased from 25.4% to 33.8% (Yeshiwas & Eskinder, Citation2021). In LMICs, the rate of cesarean sections is increasing due to fear of vaginal delivery complications, including assisted delivery (Yeshiwas & Eskinder, Citation2021). Skills get lost if not used; thus, often, missing skills tend to be a greater constraint on functionality than the lack of equipment. In addition, in Nepal, the low availability and functionality of the BEmONC signal functions in the CEmONC sites further hints at the reasons behind the increasing trends and higher rates of cesarean deliveries in hospitals. Nepali women might perceive cesarean deliveries to be safer than assisted vaginal deliveries, as indicated by the Ethiopian study.
The perceived quality of care is higher for hospitals and private HFs than for lower-level HFs and public HFs; therefore, families generally choose well-equipped hospitals with medical officers or obstetricians for deliveries (Karkee et al., Citation2014), which could be the reason for the lower functionality of BEmONC sites compared to CEmONC sites. In 2021, the availability of providers trained in delivery care was 58.4% in referral hospitals, in contrast to only 31.5% in the PHCCs (MOHP et al., Citation2022), which not only indicates better training opportunities for providers in the big hospitals but also indicates the possibility of providers preferring to work in big hospitals. In Nepal, 92.7% of the 457 normal low-risk deliveries observed in a nationally representative HF-based survey in 2021 took place in hospitals, most of which were CEmONC sites (MOHP et al., Citation2022), and in another study from Nepal’s Chitwan district published in Citation2016, more than half of the women delivered at a hospital rather than in a lower-level HF (Shah, Citation2016). Important reasons for not giving birth in a lower-level HF, most of which generally comprise the EmONC and BEmONC sites, were the lack of services and facilities, such as cesarean sections, video x-rays, blood tests, medicines and equipment, skilled birth attendants, and inadequate physical facilities (Shah, Citation2016). These findings are comparable with similar studies, one published in 2016 in Gujrat, India, where 37.7% of the pregnant women traveled further to give birth at HFs that were more functional than those nearby (Salazar et al., Citation2016); another study from Ghana showed that in 2017, 32.0% of pregnant women bypassed their nearest HF, seeking care at hospitals and private HFs even though they had to pay nearly double the price (Bell et al., Citation2020). These findings clearly convey the family’s preference for CEmONC sites due to a fear of complications during delivery. In addition, these findings also indicate the importance of measuring the experience of care periodically—an important dimension of the quality of care. Improving client and public awareness of the obstetric services available and building population trust in these services are key to improving service utilization rates and clients’ satisfaction with care.
Policy, program, and research implications
In the changing context of increased public awareness of healthcare services, most women in LMICs are using antenatal care services and giving birth in HFs. Furthermore, most deliveries in LMICs now take place in hospitals and clinics due to the suboptimal care provided in lower-level HFs (Montagu et al., Citation2017). The higher-level HFs make up the majority of the BEmONC and CEmONC sites, where people expect to receive higher-quality services, but our findings raise questions with regards to the accessibility and functionality of the vital signal functions. Not meeting service standards due to dysfunctional BEmONC and CEmONC sites increases the risk of maternal deaths during obstetric complications. Periodic assessment of these sites for readiness, adherence to the standards of care, and understanding the client’s experience of care are critical for ensuring full signal function and functionality and improving maternal survival. The functionality of these sites can be enhanced by ensuring the presence of skilled birth attendants 24/7, providing the basic amenities, equipment, essential medicines, and supplies, encouraging respectful provider behaviors, and improving the work environment for providers.
The designated CEmONC sites have remarkably increased in Nepal but are still limited, and the low availability and functionality of the signal functions in the designated BEmONC sites are concerning. Although BEmONC site expansion has been achieved as planned, our study showed that most of these sites are not functional; thus, policymakers and planners need to carefully consider the demand of the local community for services, the capabilities of the local government, the achievement of service standards, and the continuity of the services before establishing new BEmONC sites or upgrading the existing EmONC sites to BEmONC sites. The findings of our study will be useful to LMICs that are rapidly expanding EmONC sites, emphasizing that a focus on quality of care is critical. If the sites cannot attract clients, the resources will be wasted, making the health system weak. In addition, strengthening referral mechanisms to transfer pregnant women from BEmONC to CEmONC sites should be prioritized.
Improving the functionality of the existing BEmONC and CEmONC sites should be of utmost priority for LMICs. Nepal needs to carefully monitor the increase in cesarean deliveries, limit the unnecessary use of cesarean deliveries, strengthen and expand quality improvement approaches such as the Maternal and Perinatal Death Surveillance and Response (MPDSR) program (FWD & WHO , Citation2023), and teach practical skills such as instrumental vaginal deliveries. BEmONC and CEmONC sites need to be periodically assessed for functionality using the Minimum Service Standard (MSS) and other available tools, and necessary actions need to be taken to mitigate the identified gaps. Other LMICs may also benefit from the implementation of the above-described tools. In Nepal, raising public awareness of the availability of free BEmONC and CEmONC services in public HFs is important since a considerable 20.6% of Nepalese women do not give birth in HFs.
Strengths and limitations of the study
Our study used data from the nationally representative NHFS 2015 and 2021, which employed the DHS Program’s standardized Service Provision Assessment methodology to collect data on the availability and functionality of signal functions in designated BEmONC and CEmONC HFs. These surveys used computer-assisted personal interviews, intensive training for the field researchers collecting the data, standardized and pre-tested tools, and interviews validated by observations, which ensured high-quality data collection. We used the WHO recommended indicators to measure EmONC availability and functionality, thereby allowing for comparisons of results across LMICs. Our study has three major limitations: first, the sampling wasn’t done to be representative of BEmONC and CEmONC sites; second, it does not examine the BEmONC and CEmONC sites’ population coverage, which is an important United Nations process indicator on EmONC services; and third, the factors affecting signal function performance at the designated BEmONC and CEmONC sites were not examined.
Conclusion
The current pace of improvements with regards to BEmONC and CEmONC services in Nepal found in this study needs to be accelerated to achieve the maternal mortality reductions targeted through the SDGs. BEmONC and CEmONC functionality is a strong supply-side measure of the health system, and our findings indicate low health system capacity and low service readiness. The BEmONC and CEmONC sites should be well equipped with trained staff, core amenities, basic equipment, essential medicines, supplies, and guidelines that meet the standards of care and provide a good work environment for providers. In the current context of increasing HF births and the high volume of maternal deaths at HFs, particularly during delivery and the postpartum period, the overall low performance of the designated BEmONC sites and the declining functionality of the designated CEmONC sites over the two time points raise serious concerns about quality of care. In the present federal systems of government, service site expansions are happening rapidly without proper attention to service demand, resource availability to meet standards of care, or the sustainability of the sites. Thus, Nepal needs to carefully make decisions about expanding BEmONC and CEmONC service sites, considering both the population served and the sites where people travel to receive care, along with strengthening the referral systems. The quality improvement systems must regularly monitor these sites to ensure structural components and standards of care are met for achieving maternal survival.
This case study of Nepal provides important learnings for other LMICs that are working toward reducing maternal mortality. The key challenges facing LMICs are similar and rooted in weak and vulnerable health systems. Although the program or intervention strategies might differ from country to country, the key strategy to ensure maternal mortality reductions is the provision of uninterrupted, high-quality obstetric services to women through strategic expansion of EmONC sites, strengthening referral systems, improving service readiness, and periodically assessing service quality.
Supplemental Material
Download Zip (18.1 KB)Acknowledgments
The authors would like to acknowledge the Demographic and Health Survey Program for providing public access to the 2015 and 2021 Nepal Health Facility Survey data set. The authors would also like to thank the health facility, service providers, and the women who consented to participate in these surveys.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Ahmed, T., Rahman, A. E., Amole, T. G., Galadanci, H., Matjila, M., Soma-Pillay, P., Gillespie, B., Arifeen, S. E., & Anumba, D. (2021). The effect of COVID-19 on maternal newborn and child health (MNCH) services in Bangladesh, Nigeria and South Africa: Call for a contextualised pandemic response in LMICs. International Journal for Equity in Health, 20(1), 77. https://doi.org/10.1186/s12939-021-01414-5
- Aranda, Z., Binde, T., Tashman, K., Tadikonda, A., Mawindo, B., Maweu, D., Boley, E. J., Mphande, I., Dumbuya, I., Montaño, M., Clisbee, M., Mvula, M. G., Ndayizigiye, M., Casella Jean-Baptiste, M., Varney, P. F., Anyango, S., Grépin, K. A., Law, M. R., Mugunga, J. C., Hedt-Gauthier, B., … Fulcher, I. R. (2022). Disruptions in maternal health service use during the COVID-19 pandemic in 2020: Experiences from 37 health facilities in low-income and middle-income countries. BMJ Global Health, 7(1), e007247. https://doi.org/10.1136/bmjgh-2021-007247
- Bell, G., Macarayan, E. K., Ratcliffe, H., Kim, J. H., Otupiri, E., Lipsitz, S., Hirschhorn, L., Awoonor-Williams, J. K., Nimako, B. A., Ofosu, A., Leslie, H., Bitton, A., & Schwarz, D. (2020). Assessment of bypass of the nearest primary health care facility among women in Ghana. JAMA Network Open, 3(8), e2012552. https://doi.org/10.1001/jamanetworkopen.2020.12552
- Bhutta, Z. A., Ali, S., Cousens, S., Ali, T. M., Haider, B. A., Rizvi, A., Okong, P., Bhutta, S. Z., & Black, R. E. (2008). Alma-Ata: Rebirth and Revision 6 Interventions to address maternal, newborn, and child survival: What difference can integrated primary health care strategies make? Lancet (London, England), 372(9642), 972–989. https://doi.org/10.1016/S0140-6736(08)61407-5
- Department of Health Services (DOHS). (2023). Annual Report 2021-2022. Integrated Health Management Information System. Management Division, Department of Health Services, Ministry of Health and Population, Teku, Kathmandu Nepal.
- Darmstadt, G. L., Bhutta, Z. A., Cousens, S., Adam, T., Walker, N., & de Bernis, L. (2005). Evidence-based, cost-effective interventions: How many newborn babies can we save? Lancet (London, England), 365(9463), 977–988. https://doi.org/10.1016/S0140-6736(05)71088-6
- Family Welfare Division (FWD). (2019). Nepal safe motherhood and newborn health road map 2030. Family Welfare Division, Teku, Kathmandu, Nepal.
- Family Welfare Division (FWD) & World Health Organization (WHO). (2023). Maternal and Perinatal Death Surveillance and Response (MPDSR) (pp. 1–4). Government of Nepal, Ministry of Health and Population, Department of Health Services, Family Welfare Division, Nepal.
- Gausman, J., Pingray, V., Adanu, R., Bandoh, D. A. B., Berrueta, M., Blossom, J., Chakraborty, S., Dotse-Gborgbortsi, W., Kenu, E., Khan, N., Langer, A., Nigri, C., Odikro, M. A., Ramesh, S., Saggurti, N., Vázquez, P., Williams, C. R., & Jolivet, R. R. (2023). Validating indicators for monitoring availability and geographic distribution of emergency obstetric and newborn care (EmoNC) facilities: A study triangulating health system, facility, and geospatial data. PloS One, 18(9), e0287904. https://doi.org/10.1371/journal.pone.0287904
- Karkee, R., Lee, A. H., & Pokharel, P. K. (2014). Women’s perception of quality of maternity services: A longitudinal survey in Nepal. BMC Pregnancy and Childbirth, 14(1), 45. https://doi.org/10.1186/1471-2393-14-45
- Kc, A., Gurung, R., Kinney, M. V., Sunny, A. K., Moinuddin, M., Basnet, O., Paudel, P., Bhattarai, P., Subedi, K., Shrestha, M. P., Lawn, J. E., & Målqvist, M. (2020). Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: A prospective observational study. The Lancet Global Health, 8(10), e1273–e1281. https://doi.org/10.1016/s2214-109x(20)30345-4
- Lee, A. C., Cousens, S., Darmstadt, G. L., Blencowe, H., Pattinson, R., Moran, N. F., Hofmeyr, G., Haws, R. A., Bhutta, S., & Lawn, J. E. (2011). Care during labor and birth for the prevention of intrapartum-related neonatal deaths: A systematic review and Delphi estimation of mortality effect. BMC Public Health, 11(Suppl 3), S10. https://doi.org/10.1186/1471-2458-11-S3-S10
- Management Division (MD). (2021). Assess impact of COVID-19 pandemic in selected health services with estimation of ‘excess maternal deaths’. Government of Nepal Ministry of Health and Population Department of Health Service Management Division Integrated Health Information Management Section Kathmandu.
- Ministry of Health and Population (MOHP), New ERA, & ICF. (2022). Nepal health facility survey final report 2021. Ministry of Health and Population, Nepal.
- Ministry of Health and Population (MOHP), New ERA, & ICF. (2023). Nepal demographic and health survey final report 2022. Ministry of Health and Population, Nepal.
- Ministry of Health and Population (MOHP), & National Statistics Office (NSO). (2023). National population and housing census 2021: Nepal maternal mortality study 2021. Ministry of Health and Population, Nepal.
- Ministry of Health (MOH), New ERA, NHSSP, & ICF. (2016). Nepal health facility survey final report 2015. Ministry of Health, Nepal.
- Montagu, D., Sudhinaraset, M., Diamond-Smith, N., Campbell, O., Gabrysch, S., Freedman, L., Kruk, M. E., & Donnay, F. (2017). Where women go to deliver: Understanding the changing landscape of childbirth in Africa and Asia. Health Policy and Planning, 32(8), 1146–1152. https://doi.org/10.1093/heapol/czx060
- Pasha, O., Goldenberg, R. L., McClure, E. M., Saleem, S., Goudar, S. S., Althabe, F., Patel, A., Esamai, F., Garces, A., Chomba, E., Mazariegos, M., Kodkany, B., Belizan, J. M., Derman, R. J., Hibberd, P. L., Carlo, W. A., Liechty, E. A., Hambidge, K. M., Buekens, P., … Wright, L. L. (2010). Communities, birth attendants and health facilities: A continuum of emergency maternal and newborn care (the global network’s EmONC trial). BMC Pregnancy and Childbirth, 10(1), 82. https://doi.org/10.1186/1471-2393-10-82
- Pattinson, R., Kerber, K., Buchmann, E., Friberg, I. K., Belizan, M., Lansky, S., Weissman, E., Mathai, M., Rudan, I., Walker, N., & Lawn, J. E. (2011). Stillbirths: How can health systems deliver for mothers and babies? Lancet (London, England), 377(9777), 1610–1623. https://doi.org/10.1016/S0140-6736(10)62306-9
- Roy, L., Biswas, T. K., & Chowdhury, M. E. (2017). Emergency obstetric and newborn care signal functions in public and private facilities in Bangladesh. PloS One, 12(11), e0187238. https://doi.org/10.1371/journal.pone.0187238
- Shah, R. (2016). Bypassing birthing centres for childbirth: A community-based study in rural Chitwan Nepal. BMC Health Services Research, 16(1), 6–7. https://doi.org/10.1186/s12913-016-1848-x
- Salazar, M., Vora, K., & Costa, A. D. (2016). Bypassing health facilities for childbirth: A multilevel study in three districts of Gujarat, India. Global Health Action, 9(1), 32178. https://doi.org/10.3402/gha.v9.32178
- World Health Organization (WHO). (2009). Monitoring emergency obstetric care: A handbook. World Health Organization.
- World Health Organization (WHO). (2023). Trends in maternal mortality 2000 to 2020: Estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. World Health Organization.
- Yeshiwas, A., & Eskinder, K. (2021). Trends in operative delivery in Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia: A 5 years. Retrospective review. Ethiopian Journal of Health Sciences, 31(6), 1199. https://doi.org/10.4314/ejhs.v31i6.15
