
Abstract
Intimate Partner Violence (IPV) is a global problem and has been reported to be significantly higher for women in Low and Middle-Income Countries (LMICs). The researchers analyzed Demographic and Health Survey (DHS) data of married women in 20 LMICs to examine those most vulnerable to accepting IPV by investigating associated risk factors. The researchers revealed a higher level of acceptance of IPV among illiterate women from poorer households in remote areas. Using these findings, the authors provide insight into ensuring and enhancing the living standards of these vulnerable women by making education more readily accessible.
There is a high prevalence of intimate partner violence (IPV) against women in low- and middle-income countries (LMICs) and it becomes a greater barrier to achieving 2030 Sustainable Development Health Goals for women, children, and adolescents. However, these cases have been under-reported because of social and cultural factors that emphasize that these incidents are a private matter, particularly in these countries. Thus, researchers’ aim is to examine the factors associated with married women’s attitude toward IPV in 20 low- and middle-income countries. To the author’s knowledge, this is the first attempt to aggregate data from married women in South Asia, Sub-Saharan Africa, and East Asia and Pacific regions comprising 20 representative LMICs to measure their attitudes toward IPV. The researchers suggested some implications for policy and intervention based on the findings of this study. Firstly, both government and non-government organizations in countries where IPV acceptance is high need to pay more attention to reducing these attitudes. Secondly, policies should be revised to provide better opportunities for women by increasing their access to education. Third, policies that promote women’s autonomy should be developed and implemented. Further research into these identified factors and their potential contributions to IPV is important for the development of future prevention strategies. A broad international and interdisciplinary audience, including researchers, healthcare professionals, and students from various fields, such as public health, women’s studies, social work, and health education, can also benefit from this study by comparing its findings to their own contexts, enabling them to adapt strategies to combat IPV and promote gender equity within their own contexts. Furthermore, it facilitates cross-regional comparative studies, which encourages researchers to examine similar issues in their respective regions. Consequently, this research is a valuable resource to those seeking to address IPV on a global scale and to contribute to a broader interdisciplinary discussion regarding gender-based violence and public health.
Background
IPV is a global public health issue that significantly affects women’s lives (World Health Organization, Citation2021). The World Health Organization (WHO) defines IPV as any act or behavior committed by an intimate partner that causes physical, sexual, and psychological harm (Krug et al., Citation2002). Considering worldwide studies, over a quarter of women have experienced physical and/or sexual violence by their intimate partner (World Health Organization, Citation2021), indicating women as primary victims of IPV. IPV has widespread and long-lasting consequences for women and their families, causing both short-term and long-term adverse physical and psychological effects (Coll et al., Citation2020). Suicide, post-traumatic stress disorder, depression, anxiety, and drug or alcohol abuse are common psychological consequences of IPV (Miller et al., Citation2022; Mootz et al., Citation2021). Furthermore, severe physical health issues such as injuries and unplanned pregnancies are prevalent among women affected by IPV (Ibrahim et al., Citation2015; Sabri et al., Citation2014). These consequences and the widespread prevalence of IPV present significant barriers to women’s rights and the achievement of Sustainable Development Goal (SDG) 5.2, which aims at eradicating all forms of violence against women and girls (Bhowmik & Biswas, Citation2022; Coll et al., Citation2020).
While IPV is a recognized global concern, the prevalence rates vary across countries and regions, with LMICs at particular risk (Coll et al., Citation2020). The prevalence of IPV is particularly high in South Asia, East Asia, and Sub-Saharan Africa, ranging from 13.7% in Cambodia to 75% in Bangladesh (Bhowmik & Biswas, Citation2022; Coll et al., Citation2020; Tran et al., Citation2016). IPV prevalence has been found to be associated with a number of socio-demographic factors, including lower education level, lower socio-economic status, lower age at marriage, childhood abuse exposure, norms on the acceptability of violence, women’s decision-making power, and income (Bhowmik & Biswas, Citation2022; Coll et al., Citation2020; John et al., Citation2022; Memiah et al., Citation2021; Miller et al., Citation2022; Sanni et al., Citation2021; Weiman & Hesketh, Citation2021). Notably, the acceptance of IPV among women is a crucial factor associated with the prevalence of IPV (Serrano-Montilla et al., Citation2020). Most women who have been victimized by IPV in LMICs, especially in South Asia and Africa, consider violence to be acceptable and normal (Tran et al., Citation2016).
Cultural attitudes and traditions have shaped the personalities and social standing of South Asian and most LMIC women, which play a significant role in shaping the acceptance of IPV among women (Waltermaurer, Citation2012). Within many families in LMICs, especially South Asian (SA) and Sub-Saharan African (SSA) countries, cultural norms often devalue the role of women, perpetuating violence againt them. Societal expectations and limited knowledge of legal rights hinder women’s ability to address and escape IPV, leading to high rates of IPV and low divorce rates among women in LMICs, especially in South Asia (Waltermaurer, Citation2012). Therefore, determining and addressing the factors that contribute to and reinforce these cultural attitudes is essential in reducing rates of IPV against women.
There is emerging evidence from data across LMICs that specific socio-demographic factors are associated with increased acceptance of IPV including lower education levels, lower household wealth, lower status occupations, being married, early marriage, and living in rural setting (Bhowmik & Biswas, Citation2022; Serrano-Montilla et al., Citation2020). Conversely, increasing access to mass media that promote awareness campaigns and challenge social norms related to violence has been found to be a protective factor in reducing IPV acceptance (Kelly & Payton, Citation2019).
While there is a growing body of research on attitudes toward IPV acceptance, researchers have found that only limited large-scale studies have focused on identifying these factors specifically among married women in LMICs. It is crucial to consider the attitudes of married women toward IPV acceptance, as they are a unique and vulnerable population affected by IPV (Oseni et al., Citation2022; Serrano-Montilla et al., Citation2020). Furthermore, to the author’s knowledge, there has not been any attempt to aggregate data on married women from multiple LMICs in SA, SSA, East-Asia and Pacific regions to assess their attitudes toward IPV and associated factors. Therefore, in this study researchers aimed to fill this research gap and identify the most vulnerable group of married women who accept IPV. The researchers suggest that findings of this study could help policymakers to take effective measures to reduce IPV in line with UN SDG 5.2. By examining the attitudes of married women in 20 selected LMICs, the researchers aim to assist in identifying underperforming countries in the region regarding women’s attitudes toward accepting IPV and assist them in comparing cross-border national policies for the improvement of the IPV prevalence rate.
Authors noted that several theories in the literature can be used to evaluate the associated factors and the impacts of IPV. In this study, the researchers integrated two well-known theories: Social Learning Theory (SLT) and Power Theory. According to SLT, individuals acquire attitudes and behaviors through observation, imitation, and reinforcement in their social environment, including exposure to violence-related behavior in media and cultural norms (Bandura, Citation1977; Foshee et al., Citation1999; Sellers et al., Citation2005). Several demographic factors influence how a person is exposed to different social and cultural norms, including those related to IPV, such as age, education, income, and living area. Further, the workplace environment and media also contribute to observational learning and reinforcement of attitudes and beliefs about IPV. The power theory suggests that power dynamics are key to shaping attitudes and behaviors within relationships (Bell & Naugle, Citation2008; Burelomova et al., Citation2018; Sagrestano et al., Citation1999). It is possible that power imbalances between partners may contribute to the acceptance of violence. Women with lower decision-making abilities may be more vulnerable to accepting IPV because of power imbalances, making it more difficult for them to escape abusive situations. In contrast, individuals who have greater autonomy over decision-making in their relationship will have a greater opportunity to influence their own attitudes and behaviors, including their attitudes toward IPV. In several studies on IPV, researchers have used these theories to examine factors associated with attitudes toward IPV in a comprehensive manner (Copp et al., Citation2019; Okenwa-Emegwa et al., Citation2016). By considering these theories, the researchers aimed to comprehensively identify factors associated with attitudes toward IPV among married women in LMICs.
Materials and methods
Study design & data source
The researchers conducted this study using nationally representative data from DHSs which are cross-sectional, and standardized surveys carried out in over 90 countries since 1984. An important benefit of this method is that it is possible to cross-evaluate multi-country surveys due to the consistency of the methodology and homogeneity of the variables across DHS (Gamage et al., Citation2022). A two-stage stratified cluster sampling is used in every survey conducted by DHS. A list of enumeration areas (EAs) is included in the sampling frame based on the census data. In the first stage, sample of EAs (clusters) are selected using the probability proportional to size (PPS) method; the number of clusters/EAs varies across countries. In the second stage, an equal-probability systematic-sampling method is used to select a pre-determined number of households from each EA. Then, data from the selected households are collected through face-to-face interviews (Short Fabic et al., Citation2012). In this study, the researchers used the data of only currently married female respondents from the selected surveys.
In the current study, the researchers extracted the data on currently married women aged 15-49 years from the latest DHSs in 20 selected LMICs in SA, East Asia and Pacific, and SSA as majority of the LMICs are located in these regions. The included surveys for the 20 countries are: Bangladesh (2017), India (2019), Nepal (2016), Pakistan (2017), Sri Lanka (2006), Swaziland (2006), Ghana (2014), Kenya (2014), Lesotho (2014), Nigeria (2018), Senegal (2010), Tanzania (2015), Zambia (2018), Zimbabwe (2015), Cambodia (2014), Indonesia (2017), Myanmar (2015), Papua New Guinea (2016), Philippines (2017), and Timor-Leste (2016). Due to lack of available data for specific variables of interest (i.e., women’s attitudes toward IPV), the researchers utilized the 2006 DHS survey in Sri Lanka even though the last DHS survey was carried out in 2016. The total sample size of 278,205 married women was contained in the pooled dataset.
Variables
The outcome variable was the attitudes toward married women’s acceptance of IPV. This was a binary variable assessed by asking women their opinions on whether they would justify a husband hitting or beating his wife in the following scenarios using a set of fixed five binary response (yes/no) questions: (1) she goes out without telling him, (2) she neglects the children, (3) she argues with the husband, (4) she refuses to have sex with the husband, and (5) she burns the food. Based on the previous similarly focussed studies, attitudes toward acceptance of IPV were categorized as ‘Yes’ if the respondent answered yes to any of the justifications for a husband hitting or beating his wife and as ‘No’ if respondents did not respond yes to any of the five items (Bhowmik & Biswas, Citation2022).
To gain insights into the impact of socio-demographic factors on married women’s attitudes toward IPV, ten variables such as area of residence (urban, rural); education of both respondent and her partner (none, primary, secondary, higher); respondent’s current working status (not working, working); wealth index (poorest, poorer, middle, richer, richest); respondent’s involvement in decision-making (recoded binary variable: not able to make decisions, able to make decisions about own health care, a large household purchase, and/or visits to family or relatives); sex of household head (male, female); respondent’s exposure to media (not exposed or exposed to newspapers, radio, and/or TV); the age of respondents (≤ 25 years old, > 25 years old); and respondent’s age at marriage (all binary, split by median age (19 years) were selected by researchers based on the past literature (Bhowmik & Biswas, Citation2022; Bhowmik et al., Citation2021; Coll et al., Citation2020; Gamage et al., Citation2022). Survey weight, strata, and cluster information were also extracted by researchers for modeling purposes.
Statistical analysis
Researchers utilized a large-scale survey, and a list-wise deletion was applied to missing values under the assumption that they were missing completely at random (Bhowmik et al., Citation2020; Gamage et al., Citation2022). In order to estimate the percentage of married women’s attitudes toward IPV acceptance in each selected country, a descriptive analysis was conducted. The attitudes toward acceptance of IPV among married women were mapped among the 20 selected LMICs using spatial analysis. For each country, the unweighted bivariate association between socio-demographic factors and married women’s attitudes toward IPV acceptance was assessed by researchers using the Chi-square test. In these models, researchers could not adjust for country-wide variation even with the presence of multiple random effects since countries differ in terms of sample size, population, and unobserved characteristics of households. Researchers indicated that there could be additional bias in the results due to sample size differences, such as the sample size of India being much larger than the combined sample size of all other surveys. For this reason, each survey was modeled independently as well and then combined to maintain the survey reliability (Bhowmik et al., Citation2020).
To assess the influence of the predictors on attitudes toward acceptance of IPV, generalized linear regression models (GLMs) were constructed by the researchers with quasi-binomial distributions (binary logistic regression models) on the pooled data set. In the modeling, weights, clusters and strata-based effects were adjusted for in the GLMs by the researchers as DHS data were collected at multiple levels (cluster, strata, and individual level). Furthermore, to generalize the results, the survey weights for each individual were adjusted in GLMs, commonly used in DHS surveys (Bhowmik et al., Citation2020). In addition, forest plots were created by the authors to evaluate the relationship between socio-demographic factors and attitudes toward acceptance of IPV, using the adjusted odds ratio (AOR) of the sociodemographic factors which derived from separate models that fitted for each country. A significance level of 0.05 was considered for all tests. All analysis were carried out in R (4.2.0). The modeling and mapping were performed using R-packages ‘survey’, ‘maps’, and ‘ggplot2’.
Results
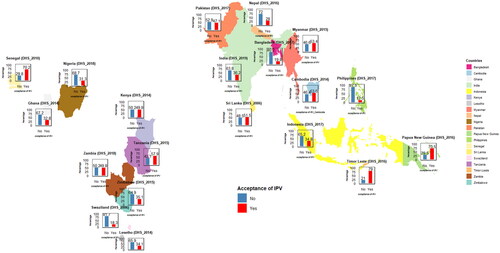
In the pooled sample of 278,205 married women, researchers noted that the highest proportion of married women (66.0%) lived in rural areas in the selected 20 LMICs. About 22.1% of the married women were aged less than 26 years old, and more than half of the married women (59.8%) in the sample were married before 20 years. Based on married women’s education levels, the highest proportion reported secondary education (38.6%), while higher education was least common, reported by only 11.9% of participants. About 53.7% of the married women were not employed. There was an approximately equal proportion of married women within the five wealth index groups (21.3%, 20.6%, 19.7%, 19.4% in poorest, poorer, middle, and richer respectively) with only slightly fewer being classified as the richest (19.0%). In regard to the partner’s education, researchers found that the majority of married women had partners with a secondary level of education (42.9%), while the least number of married women were with partners who had no education (17.9%). The majority of the married women reported that they were involved to make a decision (84.9%), and the gender of the household head of the highest proportion of the respondents was male (86.3%). About 59% of married women reported being exposed to media in some form. presents the mapping of married women’s attitudes toward acceptance of IPV among 20 selected LMICs. For the combined 20 countries’ data, approximately more than one-third (37.6%) of the married women accepted IPV, with the percentage varying from 12.5% in the Philippines to 79% in Timor Leste (79%) ().
Figure 1. Prevalence of accepting IPV among married women (in %) for 20 LMICs.
presents unweighted bivariate associations between attitudes toward IPV acceptance among married women and socio-demographic factors for each country. The researchers identified a significant association between area of residence and attitudes toward accepting IPV (p < 0.001), except in Nepal and Papua New Guinea, where married women living in rural areas were most likely to accept IPV. Authors revealed that the level of education for both respondents and their partner was significantly associated (p < 0.05) with IPV acceptance across selected LMICs, excluding Timor Leste, where a significantly higher proportion of uneducated married women showed an attitude toward IPV acceptance. Researchers found that the working status of respondents was significantly associated with IPV acceptance (p < 0.05) in most countries, except for Sri Lanka, Zambia, Ghana, Senegal, Papua New Guinea, Indonesia, and Myanmar. IPV acceptance is significantly related to wealth index, except for Sri Lanka and Papua New Guinea, where the richest married women are consistently less likely to accept IPV. Researchers observed a significant association between married women’s involvement in decision-making and their attitudes toward accepting IPV (p < 0.001), except for Nepal, Pakistan, Sri Lanka, Ghana, Swaziland, Philippine, and Indonesia, where married women who involved in decision-making were less likely to accept IPV. Authors revealed that, married women in male-dominated households were more likely to accept IPV, but this relationship was not statistically significant in more than half of the selected countries (). Media exposure was significantly associated (p < 0.05) with IPV acceptance, except for India, Swaziland, Timor Leste, and Indonesia, where married women exposed to the media showed significantly lower acceptance rate. Respondent’s age and their age at marriage were found to be significantly associated with acceptance of IPV for most of the countries.
Table 1. Bi-variate association (unweighted) between attitude toward acceptance of IPV (category: Yes, accepted IPV) and socio-demographic factors.
Based on results obtained from the fitted logistic regression model on pooled data after adjusting for survey weight, cluster, and strata presented in , the researchers have indicated that married women in 17 LMICs, except the Philippines and Swaziland, were more likely to be accepting IPV compared to Bangladesh. The researchers have highlighted Tanzania as the country with the highest acceptance of IPV, where married women were 18.5 (AOR = 18.46; 95% CI: 16.93, 20.13) times more likely to accept IPV compared to Bangladesh. Compared to Bangladesh, married women in the Philippines were 34.6% (AOR= 0.65; 95% CI: 0.59, 0.72) less likely to be accepting IPV.
Table 2. Weighted logistic regression fitted to attitude toward acceptance of IPV with sociodemographic factors using pooled data set (N = 278,205).
The area of residence was significantly associated with attitudes toward accepting IPV; married women living in rural areas were 25% (AOR= 1.25; 95% CI: 1.22, 1.29) more likely to accept IPV compared to married women living in urban areas. Authors noted that this association was consistent among most of the countries, except for Ghana, Timor Leste, and Zambia. Compared with the married women who had no education, married women with primary, secondary, and higher education were 8% (AOR= 0.92; (95% CI: 0.89, 0.95), 19% (AOR= 0.81; 95% CI: 0.78, 0.84), and 38% (AOR= 0.62; 95% CI: 0.59, 0.66) less likely to be accepting IPV, respectively. Similar results were found for the individual country level analysis (). Furthermore, married women from households where their partners had primary, secondary, and higher levels of education were 14% (AOR= 0.86; 95% CI: 0.83,0.89), 19% (AOR= 0.81; 95% CI: 0.78, 0.84), and 28% (AOR= 0.72; 95% CI:0.68, 0.75) less likely to hold attitudes toward accepting IPV, respectively compared to married women’s partners who were not educated. From the analysis of the country level data, researchers identified a similar association between education levels of married women’s partners and attitudes toward acceptance of IPV in all 20 countries ().
Figure 2. Forest plots of the sociodemographic factors on acceptance of IPV for 20 countries logistic regression model.
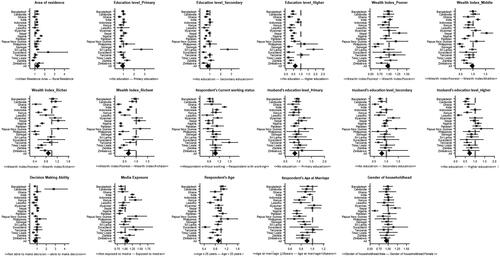
Authors revealed that wealth index was associated with married women’s attitude toward IPV, married women living in poorer, middle, richer, and richest wealth index were respectively 3% (AOR= 0.97; 95% CI: 0.94, 0.99), 4% (AOR= 0.96; 95% CI: 0.93, 0.99), 12% (AOR= 0.88, 95% CI: 0.84, 0.91), and 34% (AOR= 0.66; 95% CI: 0.63, 0.69) less likely to be accepting IPV as compared to married women living in the poorest wealth index. Compared to married women who did not currently work, married women who currently worked were 9% (AOR= 1.09; 95% CI: 1.06, 1.11) more likely to hold the attitudes toward accepting IPV. However, married women involved in household decision-making were 23% (AOR= 0.77; 95% CI: 0.75,0.80) less likely to accept IPV compared to those who were not involved in household decision making. These findings by researchers are consistent with the findings obtained from country level data ().
The researchers found a significant association between exposure to media and married women’s attitudes toward accepting IPV, with married women who regularly exposed to media being 7% (AOR= 1.07; 95% CI: 1.05, 1.10) more likely to hold an attitude of accepting IPV as compared to those not exposed to media. The researchers indicated that this association between media exposure and married women’s attitudes toward accepting IPV varied across countries. Based on the results of fitted models for the individual country data, researchers revealed that married women exposed to media in eleven (Bangladesh, Ghana, Cambodia, Lesotho, Myanmar, Nigeria, Nepal, Pakistan, Sri Lanka, Tanzania, and Timor-Leste) out of the 20 selected countries had a lower tendency to justify IPV ().
Researchers found that older married women (> 25 years) were 9% (AOR= 0.91; 95% CI: 0.88, 0.93) less likely to be accepting IPV as compared to the younger group (≤ 25 years). Married women who were older than 19 years at their first marriage were 14% (AOR= 0.86; 95% CI: 0.83, 0.88) less likely to accept IPV compared to their younger counterpart (≤ 19 years). The gender of the household head was significantly associated with married women’s attitude toward acceptance of IPV, having a female household head had 5% (AOR= 0.95; 95% CI: 0.92, 0.98) less likely to hold an attitude of accepting IPV than having a male household head. Similar associations between gender of the househead and married women’s attitudes toward accepting IPV were observed by the authors in the models based on individual country data ().
Discussion
The researchers’ aim was to investigate the status of attitude toward acceptance of IPV and identify key socio-demographic factors underlying married women’s attitudes toward acceptance of IPV in 20 LMICs representing SA, East Asia and Pacific, and SSA regions. The researchers revealed a significant association between attitudes toward acceptance of IPV among married women and most of the socio-demographic factors, including married women’s level of education and their involvement in decision-making. In line with previous studies, married women with a lower level of education, having married before 19 years of age, being under 25 years of age, being in the lowest wealth quantile, not participating in household decision-making, living in rural areas, and being under a male house head were more likely to justify IPV. (Asif & Akbar, Citation2021; Bhowmik & Biswas, Citation2022; Islam et al., Citation2021; Melnikas et al., Citation2020).
In this study, researchers revealed that married women’s attitude toward acceptance of IPV was influenced by their level of education as demonstrated by previous studies (Bhowmik & Biswas, Citation2022; Serrano-Montilla et al., Citation2020; Weitzman, Citation2018). It is likely that education increases the chances for women to obtain information that allows them to develop a positive self-image and abilities, leading to changes in their perception of gender roles and attitudes toward IPV (Wang, Citation2016). According to the literature, low levels of education are associated with higher levels of gender inequality and with norms that accept violence, resulting in conflict within relationships (Antai & Antai, Citation2008; Uthman et al., Citation2009).
Researchers findings of this study are consistent with previous findings, in which the higher educational level of the husband was associated with a lower acceptance of IPV (Wang, Citation2016). Due to the relatively low incidence of domestic violence perpetrated by educated husbands and the tendency of more educated women to marry higher educated partners, there might be a low justification for IPV (Weitzman, Citation2018). Higher levels of education are accompanied by skills and knowledge that challenge traditional gender roles, leading to more equitable relationships between men and women in intimate partnership (Wang, Citation2016). Therefore, regardless of gender, higher education is associated with adherence to more progressive views on women’s rights and ultimately eliminates IPV acceptance.
Furthermore, researchers noted that extended education often delays young-age marriage, which allows women to build up their careers more successfully, making them less dependent on their partners, and enabling them to easily leave abusive relationships (Weitzman, Citation2018), thus reducing IPV prevalence and acceptance. The present study, the researchers found that age at first marriage influence women’s attitude toward accepting IPV, women who married after the age of 19 were less likely to accept IPV than those who married earlier, which is in line with findings of past studies (Islam et al., Citation2021; Melnikas et al., Citation2020). Additionally, authors found that older women were less likely to justify IPV than younger women, in line with previous findings (Bhowmik & Biswas, Citation2022; Wang, Citation2016). This could be due to the fact that young women tend to have fewer years of education, which restricts their ability to articulate new ideas and access to more information about women’s rights against IPV (Uthman et al., Citation2009).
Lower wealth indexes lead to household stressors like financial stress, which, in turn, increase violent partnership disputes and, therefore, women’s feeling of suppression and acceptance of IPVs (Weitzman, Citation2018). Furthermore, authors noted that in households with low wealth indices, it is commonly believed that IPV against women is a patriarchal ‘right’ of the husband or partner. As a result, women in poorer households are financially dependent on their partners, which results in them accepting IPV (Bhowmik & Biswas, Citation2022; Biswas et al., Citation2017; Gracia et al., Citation2021). Similarly, in this study researchers found that a lower wealth index was found to be associated with higher level of IPV acceptance in LMICs.
Empowerment of women and their ability to make decisions have been noted as being significant influences on a range of health, social behaviors, and economic growth (Shimamoto & Gipson, Citation2019). The power of women in decision-making is an essential component of gender equality (Upadhyay et al., Citation2014). As IPV is often fueled by a lack of respect for women’s empowerment and decision-making power, it is essential to prioritize women’s right to make their own choices as a means of combating this widespread issue (Fageeh, Citation2014). In the present study, researchers revealed that the ability of women to make decisions was found to be protective of IPV justification, which is consistent with previous studies (Antai & Antai, Citation2008).
Despite some progress in terms of access to employment opportunities and improved working conditions, women in these countries still face significant challenges, including gender-based discrimination in the workplace, lower wages, and limited access to social protection (Gage & Thomas, Citation2017). However, the results of the present study reported by the researchers support the findings of previous literature (Cools & Kotsadam, Citation2017), indicating that women’s employment increases IPV acceptance. Researchers recommend further investigations, including qualitative research to see the reasons behind this unexpected outcome.
In line with previous studies, researchers found that married women in rural settings tended to justify IPV more than women in urban settings, which aligns with the findings of our study (Bhowmik & Biswas, Citation2022; Sayem et al., Citation2012). This could be due to a variety of factors such as limited access to legal protection and services, social norms, and cultural practices (Dalal et al., Citation2012; Heron & Eisma, Citation2021). In addition, rural women, having the lowest socio-economic status, are more likely to experience childhood violence, such as witnessing fathers acting violently against their mothers, and they have fewer opportunities and resources to learn about gender equity and rights to safety, thereby accepting IPV (Speizer, Citation2010).
In general, media campaigns increase awareness and women’s support networks, which reduces the acceptance of IPV (Jesmin, Citation2015). Several studies were found that women who did not have access to the media justified IPV more than others (Bhowmik & Biswas, Citation2022). Although the results obtained from the pooled data set of this study by the researchers were indicated that married women with limited access to the media were less likely to accept IPV, majority of the selected countries (11 out of 20) showed that women exposed to the media were less likely to accept IPV. Similar findings have been reported in other studies, indicating that having access to radio increased women’s likelihood of justifying IPV (Forsyth & Ward, Citation2022; Krause et al., Citation2017). Authors noted that, there may be a reason for the conflicting findings due to the content covered by the media. When media consumers are exposed to violent content that is socially endorsed and promoted, violence is more likely to be approved and practiced (Forsyth & Ward, Citation2022). Conversely, media content that discourages violence and/or exposes its consequences will reduce the likelihood of media users approving violence and engaging in it (Forsyth & Ward, Citation2022). Therefore, authors suggest that when examining the relationship between media exposure and IPV approval, it is crucial to explore the content covered by the media and the type and structure of media.
The researchers revealed significant heterogeneity in attitudes toward IPV among women across 20 LMICs in SA, SSA, and East Asia and Pacific regions. Researchers found that more than half of married women in Timor Leste, Papua New Guinea, Senegal, Tanzania, Cambodia, Myanmar, and Sri Lanka justified IPV whereas in almost all other countries around 20% of married women accepted IPV, with the lowest percentage of acceptance of IPV observed in the Philippines. Consequently, many women in Asian LMICs (SA and East Asia) are at risk of IPV as a result of high acceptance rates. Women in these LMICs are more likely to be limited in their autonomy because of the sociocultural context; they are also more likely adhere to traditional norms that women are not supposed to participate in household decisions and that they are more vulnerable to spousal violence (Asif & Akbar, Citation2021; Bhowmik & Biswas, Citation2022; Sayem et al., Citation2012).
To the author’s knowledge, this is the first attempt to aggregate data from married women in SA, SSA, and East Asia and Pacific regions comprising 20 representative LMICs. In this study, analyses were conducted on pooled dataset and country level data. This study provided scope to identify the vulnerable group of married women by considering a large number of representative LMICs around the globe. This study’s findings can be used for comparisons between countries and enable policy makers to make the decision for better improvement.
While the researchers uncovered valuable insights into married women’s attitudes toward IPV in LMICs, this study does have some limitations. Firstly, the researchers focused only on married women between 15 and 49 years of age since DHSs only consider women between 15-49 years old; women older than 49 years of age were left out of this study and their attitudes toward IPV could differ. Secondly, DHS only assessed attitudes toward physical abuse without including other types of violence, such as mental or emotional abuse, limiting the study to only physical IPV due to the lack of data availability. Thirdly, the survey data did not contain any qualitative information, such as background information on the media women were exposed to or their opinions on patriarchal norms. Qualitative information would have been helpful to get a better understanding of the root causes of having attitudes toward IPV acceptance and validating the quantitative findings. Finally, since the researchers obtained data based on a cross-sectional study setting, causal interpretations cannot be made. Considering these limitations, careful consideration to be made when interpreting the results of the current study.
Conclusion
In this study, data was analyzed by the researchers from the latest DHSs conducted in 20 selected LMICs to evaluate the current status of married women’s attitude toward IPV and to determine the factors influencing married women’s attitudes toward accepting IPV in predicting the most vulnerable group of women. Across countries, married women’s attitude toward acceptance of IPV differs widely, but it is most common in LMICs in Asia and Sub-Saharan Africa region. The researchers found that married women living in the poorest households, having low levels of education, getting married at a young age, living in a male-dominated household, having employment, not being able to make decisions, and living in rural areas were the most vulnerable groups to IPV acceptance. In the future, researchers should investigate these identified factors and how they may contribute to the acceptance of IPV for use in developing preventative strategies. Effective and feasible intervention programs are necessary at the country level for this group of women to support the achievement of SDG 5.2 by 2030, which aims to eliminate all forms of violence against women, especially in Asian region, which has a higher acceptance of IPV.
Ethics statement
De-identified secondary datasets are provided upon request by the DHS program authority. The authors obtained permission from DHS to use the above-mentioned surveys. Further, this study was approved by the Swinburne University of Technology Human Research Ethics Committee (approval number: 20226572-10707).
Authors’ contributions
This study was conceptualized by LG and JB. The study design was developed by LG, while the screening and analysis of the data were performed by LG, JB, and PA. The initial draft of the manuscript was prepared by LG. JB, MN, and PA reviewed the draft manuscript and provided their feedback. The final manuscript was read and approved by all the authors.
Supplemental Material
Download MS Word (90.7 KB)Acknowledgments
The study was conducted as a part of the PhD study at the Swinburne University of Technology in Australia, and we thank the university for providing a Tuition Fee Scholarship (TFS). The authors would like to thank Department of Census and Statistics in Sri Lanka for providing data of DHS 2006 in Sri Lanka.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The secondary data sets analyzed in the current study are freely available upon request from the DHS website (http://dhsprogram.com/data/available-datasets).
Additional information
Funding
References
- Antai, D. E., & Antai, J. B. (2008). Attitudes of women toward intimate partner violence: A study of rural women in Nigeria. Rural and Remote Health, 8(3), 996. https://doi.org/10.22605/RRH996
- Asif, A. M., & Akbar, M. (2021). On the decomposition of rank-dependent indicator of socio-economic inequalities in child malnutrition: Some empirical findings. Socio-Economic Planning Sciences, 77, 101025. https://doi.org/10.1016/j.seps.2021.101025
- Bandura, A. (1977). Social learning theory. Prentice-Hall.
- Bell, K. M., & Naugle, A. E. (2008). Intimate partner violence theoretical considerations: Moving towards a contextual framework. Clinical Psychology Review, 28(7), 1096–1107. https://doi.org/10.1016/j.cpr.2008.03.003
- Bhowmik, J., & Biswas, R. K. (2022). Married women’s attitude toward intimate partner violence is influenced by exposure to media: A population-based spatial study in Bangladesh. International Journal of Environmental Research and Public Health, 19(6), 3447. https://doi.org/10.3390/ijerph19063447
- Bhowmik, J., Biswas, R. K., & Ananna, N. (2020). Women’s education and coverage of skilled birth attendance: An assessment of Sustainable Development Goal 3.1 in the South and Southeast Asian Region. PloS One, 15(4), e0231489. https://doi.org/10.1371/journal.pone.0231489
- Bhowmik, J., Biswas, R. K., & Hossain, S. (2021). Child marriage and adolescent motherhood: A nationwide vulnerability for women in Bangladesh. International Journal of Environmental Research Public Health, 18(8), 4030. https://doi.org/10.3390/ijerph18084030
- Biswas, R. K., Rahman, N., Kabir, E., & Raihan, F. (2017). Women’s opinion on the justification of physical spousal violence: A quantitative approach to model the most vulnerable households in Bangladesh. PloS One, 12(11), e0187884. https://doi.org/10.1371/journal.pone.0187884
- Burelomova, A., Gulina, M., & Tikhomandritskaya, O. (2018). Intimate partner violence: An overview of the existing teories, conceptual frameworks, and defnitions. Psychology in Russia: State of the Art, 11(3), 128–144. https://doi.org/10.11621/pir.2018.0309
- Coll, C. V. N., Ewerling, F., García-Moreno, C., Hellwig, F., & Barros, A. J. D. (2020). Intimate partner violence in 46 low-income and middle-income countries: An appraisal of the most vulnerable groups of women using national health surveys. BMJ Global Health, 5(1), e002208. https://doi.org/10.1136/bmjgh-2019-002208
- Cools, S., & Kotsadam, A. (2017). Resources and intimate partner violence in sub-Saharan Africa. World Development, 95, 211–230. https://doi.org/10.1016/j.worlddev.2017.02.027
- Copp, J. E., Giordano, P. C., Longmore, M. A., & Manning, W. D. (2019). The development of attitudes toward intimate partner violence: An examination of key correlates among a sample of young adults. Journal of Interpersonal Violence, 34(7), 1357–1387. https://doi.org/10.1177/0886260516651311
- Dalal, K., Lee, M. S., & Gifford, M. (2012). Male adolescents’ attitudes toward wife beating: A multi-country study in South Asia. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 50(5), 437–442. https://doi.org/10.1016/j.jadohealth.2011.09.012
- Fageeh, W. M. K. (2014). Factors associated with domestic violence: A cross-sectional survey among women in Jeddah, Saudi Arabia. BMJ Open, 4(2), e004242. https://doi.org/10.1136/bmjopen-2013-004242
- Forsyth, S., & Ward, K. P. (2022). Media use and men’s approval of intimate partner violence in honduras. Journal of Interpersonal Violence, 37(13-14), Np11541–Np11556. https://doi.org/10.1177/0886260521993926
- Foshee, V. A., Bauman, K. E., & Linder, G. F. (1999). Family violence and the perpetration of adolescent dating violence: Examining social learning and social control processes. Journal of Marriage and the Family, 61(2), 331–342. https://doi.org/10.2307/353752
- Gage, A. J., & Thomas, N. J. (2017). Women’s work, gender roles, and intimate partner violence in Nigeria. Archives of Sexual Behavior, 46(7), 1923–1938. https://doi.org/10.1007/s10508-017-1023-4
- Gamage, S., Biswas, R. K., & Bhowmik, J. (2022). Health awareness and skilled birth attendance: An assessment of sustainable development goal 3.1 in south and south-east Asia. Midwifery, 115, 103480. https://doi.org/10.1016/j.midw.2022.103480
- Gracia, E., Marco, M., López-Quílez, A., & Lila, M. (2021). Chronic high risk of intimate partner violence against women in disadvantaged neighborhoods: An eight-year space-time analysis. Preventive Medicine, 148, 106550. https://doi.org/10.1016/j.ypmed.2021.106550
- Heron, R. L., & Eisma, M. C. (2021). Barriers and facilitators of disclosing domestic violence to the healthcare service: A systematic review of qualitative research. Health & Social Care in the Community, 29(3), 612–630. https://doi.org/10.1111/hsc.13282
- Ibrahim, Z., Ahmed, W. S., El-Hamid, S., & Hagras, A. (2015). Intimate partner violence among Egyptian pregnant women: Incidence, risk factors, and adverse maternal and fetal outcomes. Clinical and Experimental Obstetrics & Gynecology, 42(2), 212–219. https://doi.org/10.12891/ceog1829.2015
- Islam, M. M., Khan, M. N., & Rahman, M. M. (2021). Attitudes to and experiences of intimate partner violence among Rohingya women who married before eighteen years of age. Global Health Action, 14(1), 1943852. https://doi.org/10.1080/16549716.2021.1943852
- Jesmin, S. S. (2015). Social determinants of married women’s attitudinal acceptance of intimate partner violence. Journal of Interpersonal Violence, 32(21), 3226–3244. https://doi.org/10.1177/0886260515597436
- John, N. A., Kapungu, C., Sebany, M., & Tadesse, S. (2022). Do gender-based pathways influence mental health? Examining the linkages between early child marriage, intimate partner violence, and psychological well-being among young Ethiopian women (18–24 years Old) [Article]. Youth and Society, 55(6), 1155–1172. https://doi.org/10.1177/0044118X221079375
- Kelly, J., & Payton, E. (2019). A content analysis of local media framing of intimate partner violence. Violence and Gender, 6(1), 47–52. https://doi.org/10.1089/vio.2018.0019
- Krause, K. H., Haardörfer, R., & Yount, K. M. (2017). Individual schooling and women’s community-level media exposure: A multilevel analysis of normative influences associated with women’s justification of wife beating in Bangladesh. Journal of Epidemiology and Community Health, 71(2), 122–128. https://doi.org/10.1136/jech-2015-206693
- Krug, E. G., Mercy, J. A., Dahlberg, L. L., & Zwi, A. B. (2002). The world report on violence and health. Lancet (London, England), 360(9339), 1083–1088. https://doi.org/10.1016/s0140-6736(02)11133-0
- Melnikas, A. J., Ainul, S., Ehsan, I., Haque, E., & Amin, S. (2020). Child marriage practices among the Rohingya in Bangladesh. Conflict and Health, 14(1), 28. https://doi.org/10.1186/s13031-020-00274-0
- Memiah, P., Ah Mu, T., Prevot, K., Cook, C. K., Mwangi, M. M., Mwangi, E. W., Owuor, K., & Biadgilign, S. (2021). The prevalence of intimate partner violence, associated risk factors, and other moderating effects: Findings from the Kenya national health demographic survey [Article]. Journal of Interpersonal Violence, 36(11–12), 5297–5317. https://doi.org/10.1177/0886260518804177
- Miller, M., Okoth, V., Prigmore, H. L., Ressler, D. J., Mbeya, J., Rogers, A., Moon, T. D., & Audet, C. M. (2022). The Prevalence of Interpersonal Violence (IPV) against women and its associated variables: An exploratory study in the Rongo sub-county of Migori County, Kenya. Journal of Interpersonal Violence, 37(5–6), 2083–2101.
- Mootz, J. J., Basaraba, C. N., Corbeil, T., Johnson, K., Kubanga, K. P., Wainberg, M. L., & Khoshnood, K. (2021). Armed conflict, HIV, and syndemic risk markers of mental distress, alcohol misuse, and intimate partner violence among couples in Uganda. Journal of Traumatic Stress, 34(5), 1016–1026. https://doi.org/10.1002/jts.22740
- Okenwa-Emegwa, L., Lawoko, S., & Jansson, B. (2016). Attitudes toward physical intimate partner violence against women in Nigeria. SAGE Open, 6(4), 215824401666799. https://doi.org/10.1177/2158244016667993
- Oseni, T. I. A., Salam, T. O., Ilori, T., & Momoh, M. O. (2022). Prevalence and pattern of intimate partner violence among men and women in Edo State, Southern Nigeria. African Journal of Primary Health Care & Family Medicine, 14(1), e1–e7. https://doi.org/10.4102/phcfm.v14i1.3147
- Sabri, B., Renner, L. M., Stockman, J. K., Mittal, M., & Decker, M. R. (2014). Risk factors for severe intimate partner violence and violence-related injuries among women in India. Women & Health, 54(4), 281–300. https://doi.org/10.1080/03630242.2014.896445
- Sagrestano, L. M., Heavey, C. L., & Christensen, A. (1999). Perceived power and physical violence in marital conflict. Journal of Social Issues, 55(1), 65–79. https://doi.org/10.1111/0022-4537.00105
- Sanni, Y., Hudani, A., Buh, A., & Ghose, B. (2021). Prevalence and predictors of intimate partner violence among married women in Egypt. Journal of Interpersonal Violence, 36(21–22), 10686–10704.
- Sayem, A. M., Begum, H. A., & Moneesha, S. S. (2012). Attitudes towards justifying intimate partner violence among married women in Bangladesh. Journal of Biosocial Science, 44(6), 641–660. https://doi.org/10.1017/s0021932012000223
- Sellers, C. S., Cochran, J. K., & Branch, K. A. (2005). Social learning theory and partner violence: A research note. Deviant Behavior, 26(4), 379–395. https://doi.org/10.1080/016396290931669
- Serrano-Montilla, C., Lozano, L. M., Bender, M., & Padilla, J. L. (2020). Individual and societal risk factors of attitudes justifying intimate partner violence against women: A multilevel cross-sectional study. BMJ Open, 10(12), e037993. https://doi.org/10.1136/bmjopen-2020-037993
- Shimamoto, K., & Gipson, J. D. (2019). Investigating pathways linking women’s status and empowerment to skilled attendance at birth in Tanzania: A structural equation modeling approach. PloS One, 14(2), e0212038. https://doi.org/10.1371/journal.pone.0212038
- Short Fabic, M., Choi, Y., & Bird, S. (2012). A systematic review of demographic and health surveys: Data availability and utilization for research. Bulletin of the World Health Organization, 90(8), 604–612. https://doi.org/10.2471/BLT.11.095513
- Speizer, I. S. (2010). Intimate partner violence attitudes and experience among women and men in Uganda. Journal of Interpersonal Violence, 25(7), 1224–1241. https://doi.org/10.1177/0886260509340550
- Tran, T. D., Nguyen, H., & Fisher, J. (2016). Attitudes towards intimate partner violence against women among women and men in 39 low- and middle-income countries. PloS One, 11(11), e0167438. https://doi.org/10.1371/journal.pone.0167438
- Upadhyay, U. D., Gipson, J. D., Withers, M., Lewis, S., Ciaraldi, E. J., Fraser, A., Huchko, M. J., & Prata, N. (2014). Women’s empowerment and fertility: A review of the literature. Social Science & Medicine (1982), 115, 111–120. https://doi.org/10.1016/j.socscimed.2014.06.014
- Uthman, O. A., Lawoko, S., & Moradi, T. (2009). Factors associated with attitudes towards intimate partner violence against women: A comparative analysis of 17 sub-Saharan countries. BMC International Health and Human Rights, 9(1), 14. https://doi.org/10.1186/1472-698X-9-14
- Waltermaurer, E. (2012). Public justification of intimate partner violence: A review of the literature. Trauma, Violence & Abuse, 13(3), 167–175. https://doi.org/10.1177/1524838012447699
- Wang, L. (2016). Factors influencing attitude toward intimate partner violence. Aggression and Violent Behavior, 29, 72–78. https://doi.org/10.1016/j.avb.2016.06.005
- Weiman, Y., & Hesketh, T. (2021). Intimate partner violence and depression in women in China. Journal of Interpersonal Violence, 36(21–22), NP12016–NP12040. https://doi.org/10.1177/0886260519888538
- Weitzman, A. (2018). Does increasing women’s education reduce their risk of intimate partner violence? Evidence from an education policy reform. Criminology: An Interdisciplinary Journal, 56(3), 574–607. https://doi.org/10.1111/1745-9125.12181
- World Health Organization. (2021). Violence against women. https://www.who.int/news-room/fact-sheets/detail/violence-against-women
