
Abstract
High-tech communication aids are one form of augmentative and alternative communication (AAC) intervention offered to children following an assessment process to identify the most appropriate system based on their needs. Professional recommendations are likely to include consideration of child characteristics and communication aid attributes. Recommendations may be influenced by contextual factors related to the cultural work practices and service context of professionals involved, as well as by contextual factors from the child’s life including their family environment and wider settings. The aim of this study was to explore the influence of cultural and contextual factors on the real-time decision-making processes of specialized AAC professionals in the UK. A total of six teams were recruited to the study. Each team carried out an assessment appointment related to a communication aid recommendation for a child and family. Following the appointment, each team participated in a focus group examining their decision-making processes during the preceding assessment. Inductive coding was used to analyse the transcribed data, and three organizing themes emerged relating to the global theme of Cultural and Contextual Influencers on communication aid decision-making. An explanatory model was developed to illustrate the funnelling effect that contextual factors may have on decision-making, which can substantially alter the nature and timing of a communication aid recommendation. Implications for clinical practice and future research are discussed.
Communication aids provided to children have the potential to be life changing (Bryen, Chung, & Lever, Citation2010). These communication aids may augment spoken output, enhance language development opportunities, support communicative interaction, and ultimately open up opportunities for meaningful participation in society (Ryan et al., Citation2015). While communication aids have the potential to offer many benefits to children, these can only be realized when communication aids are appropriately recommended and implemented (Baxter, Enderby, Evans, & Judge, Citation2012). Identifying the most appropriate communication aid is a complex process involving the consideration of many factors related to the child and potential high-tech communication aids (Beukelman & Mirenda, Citation2013; Murray et al., Citation2019). However, there may also be factors outside the child and the communication aid that influence the recommendation process (Batorowicz & Shepherd Citation2011; Dietz, Quach, Lund, & McKelvey, Citation2012; Lindsay Citation2010). Environmental factors that may influence decision-making stem from the cultural work practices and context of the service provider and from the child’s home and wider context. Exploring how a service provider’s cultural work practices and contextual factors influence service delivery and simultaneously recognizing the cultural and context specific factors defining the child may enhance our understanding of communication aid recommendation processes.
How services are organized and delivered may potentially affect the recommendations made for individual children. Previous research has indicated that a number of service-related factors may influence decision-making in communication aid recommendations (Batorowicz, & Shepherd, Citation2011; Dietz et al., Citation2012; Lindsay, Citation2010) and the professionals’ experience level with AAC influences how the recommendation process is undertaken (Dietz et al., Citation2012). Service structures and processes may also affect the decisions professionals make; such that national or local policies may dictate who is involved in decision-making (Batorowicz, & Shepherd, Citation2011), when funding can be accessed, and how long a communication aid must last before a new aid can be recommended (Lindsay, Citation2010). Previous research has indicated these service-related factors influence the decisions made by professionals. In the UK, specialized and local AAC service structures vary considerably; and in England and Wales, AAC services are commissioned by the National Health Service (NHS) and are provided through a Hub and Spoke modelFootnote1. The majority of people who need AAC in England and Wales access services through the local Spoke services (NHS, Citation2018). Approximately 10% of individuals who need high-tech communication aids access services through specialized Hub provision. Children accessing specialized services must meet a range of referral criteria, including the presence of a receptive-expressive language gap, the ability to combine concepts, the need for graphic symbols to communicate through high-tech systems, or the need for a complex access solution to use high-tech (NHS, Citation2018). In other parts of the UK, AAC specialized services have referral criteria that enable local practitioners to refer any child with any type of AAC need.
As well as providing assessment and recommendation services, local providers may also deliver interventions critical for successful outcomes in aided AAC. Local AAC provision is typically managed within speech and language therapy services or may be provided by school-employed speech & language therapists (SLTs) in special education contexts. Local providers are often able to provide expertise to support a child’s full range of speech, language, and communication needs (e.g. supporting multimodal communication through interventions targeting speech and aided communication abilities concurrently). However, local professionals may have varying levels of AAC expertise, which typically ranges from highly expert to inexperienced; and variable access to continuing professional development opportunities (Gross, Citation2011; Matthews, Citation2001). They may have limited resources to provide AAC services (e.g. both AAC tools and service delivery time to provide appropriate support) and limited opportunities to collaborate with professionals with other relevant expertise (e.g. with specialist teachers or occupational therapists).
In contrast, UK specialized services mostly, but not exclusively, operate by offering local services access to a range of professional expertise for consultative support. Commonly, teams may include SLTs, occupational therapists (OTs), teachers, clinical scientists, and assistive technology specialists. Specialized service providers may be able to support a range of assistive technology needs (e.g. integration of powered mobility and high-tech AAC) and have access to a range of AAC resources. However, the expertise of some specialized providers is limited to (a) the small sub-set of children who meet their referral criteria; (b) making recommendations but not carrying out interventions; and (c) within England and Wales, addressing high-tech, but not low-tech or no-tech solutions (Gross, Citation2011). Recent changes in legislation across the UK have placed a lens over current and future AAC service organization and communication aid funding (e.g. Special Educational Needs and Disability Code of Practice, Citation2014). Thus far, the impact of these changes on service provision, and their potential influence on decision-making in communication aid recommendation, has not been documented. Given the impact of service structure, processes, and team composition on decision-making in other jurisdictions (Batorowicz, & Shepherd, Citation2011; Dietz et al., Citation2012; Lindsay, Citation2010), an exploration of the role of UK service structures and processes on decision-making in communication aid recommendations is timely.
Additional contextual aspects that potentially influence communication-aid decision-making are the child’s educational and home environments, which constitute extrinsic factors contributing to AAC uptake and achievement. Children who use AAC live within family systems and the recommendation of a high-tech communication aid is likely to resonate across the whole family (Angelo, Citation2000; Smith, Murray, von Tetzchner, & Langan, Citation2010). Existing literature indicates that a host of factors related to the family and the child’s wider context have the potential to act as facilitators or barriers to using AAC (Lindsay, Citation2010). Contextual factors likely to affect the outcome of aided interventions include family attitudes to technology, time available for communication aid customization, family and teacher expectations of the child, and the priority given to AAC by the family (Angelo, Citation2000; Goldbart & Marshall, Citation2004; Johnson, Inglebret, Jones, & Ray, Citation2006; Lindsay, Citation2010). Previously, these factors have been identified by research participants reflecting on what they perceive as contributing to outcomes for children who need or use AAC (Lindsay, Citation2010). However, little research has focused on how these factors influence the decisions made within the recommendation process.
This study examined the views of professionals regarding child, communication aid, and other factors influencing their high-tech communication aid recommendations. Due to the breadth of the findings from this study, a companion paper in this issue (see Murray et al., Citation2019) addresses the child characteristics, access features, and communication aid attributes considered in communication aid recommendations for children in the UK. The aim of this study was to understand the cultural and contextual aspects of communication aid recommendations; specifically, how these factors influence the team’s communication aid recommendation decisions. The research question addressed was: What factors, besides the child, access, and the communication aid, influence how professionals make decisions in communication aid recommendations?
Method
Design
This exploratory study used an ethnographic qualitative approach to examine the recurring cultural work practices and contextual influencers on decision-making in communication aid recommendations by professional teams. This study forms part of a more extensive research project examining decision-making in communication aid recommendation in the UK. Ethical approval was obtained from Manchester Metropolitan University and the relevant NHS Research Ethics Committee (REC reference 6/NW/0165).
Participants
Professionals
Teams of professionals from centres providing communication aid recommendations to children from across the UK were invited to participate. Purposive sampling of teams (n = 6) was undertaken to ensure that participants had relevant expertise and that the sample reflected the range of different service providers in the UK (e.g. government-funded public services and charitable organizations). Participants were eligible to take part if they were (a) professional team members (e.g. SLTs, OTs) involved in making a communication aid recommendation for an identified child aged 0–18 years referred to a specialized service, and (b) employed directly by the specialized service or by local services supporting the individual child. All professional team members involved in the clinical decision-making for a particular child were invited to participate in one focus group, and all provided written consent.
Six focus groups were completed. The focus groups ranged in size from two to 13 participants, with a mean of five. Participants were grouped in their teams and, therefore, focus group size was determined by the number of professionals involved in decision-making for each child and varied according to service structures and delivery processes. Participants in each focus group had a range of professional backgrounds (see ). Each focus group discussed the decision-making processes for one child who attended for an assessment episode immediately before the focus group.
Table 1. Focus group demographics.
Child and families
Children and their families who facilitated this study were also recruited using purposive sampling. This procedure ensured the children represented a range of profiles regarding age, sex, medical diagnosis, abilities and challenges, and stage of communication aid use that are typically referred to UK specialized services (see ). Each team identified a family due to attend for an assessment appointment and invited them to be facilitators of the research. The families were provided with research aim information and asked to provide written consent to their child's communication aid recommendation being discussed by the professional team members in a focus group. To avoid the research having any influence on the clinical decision-making related to each child’s assessment, families were not invited to participate in this study.
Table 2. Demographics of the children discussed by focus group participants (all names are pseudonyms).
Procedure
One appointment within a communication aid assessment acted as the starting point for each focus group discussion. Two researchers travelled to the assessment location. The researchers were not present for the assessment to avoid any assumptions formed while observing the process from influencing the data. It also ensured that the research did not impact on the assessment appointment, including any discussion of decisions made with the family. Following the appointment, participants were convened in a focus group facilitated by the two researchers. Open-ended questions and follow-up probes were used to explore the decision-making processes within the appointment and in their practice more generally (see Supplementary Appendix).
Data analysis
Focus group transcripts were imported into NVIVO10™ software for data management purposes. To identify the salient and recurrent themes in the dataset, an inductive thematic analysis approach was used (Braun & Clarke, Citation2006). Using this approach, two researchers who were specialist AAC SLTs with more than 20 years’ experience each in AAC clinical practice and research read and re-read the transcripts to obtain an overall sense of the data and to develop their initial impressions. An initial coding process was then undertaken to identify meaningful data segments related to early codes. The two researchers discussed initial coding recognizing commonalities and discrepancies that were further discussed to inform the coding development, undertaking an iterative process of coding refinement. Independent coding reviews were conducted by two external researchers to ensure credibility and transferability (Braun & Clarke, Citation2006). In addition, a peer review process was undertaken by a co-researcher with lived experience of AAC and an AAC researcher/specialist SLT in AAC. The purpose of this review was to ensure trustworthiness of the qualitative process. The co-researcher and specialist SLT reviewed portions of coding against the operational coding definitions and asked questions about the overall procedure, meanings, and interpretations. The NVIVO10™ software provided an audit trail and supported credibility. All basic codes were themed from focus group transcripts with 5–83 references per basic code recorded. Content was in many instances assigned to more than one basic code; however, it appears here in the basic code where it was considered most salient. A thematic network was drawn up to reflect the relationships between themes identified from the dataset. Further sense checking was carried out with the wider research team using quotes to illustrate the identified themes.
Results
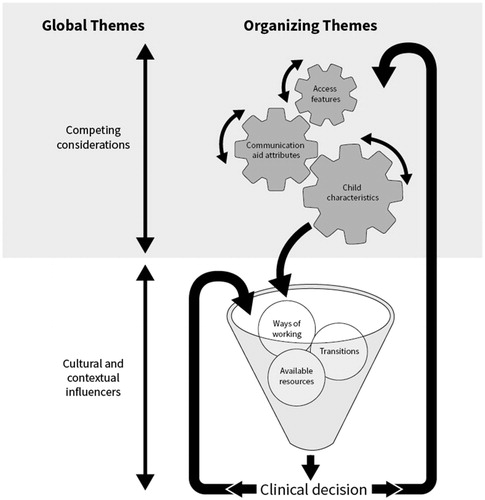
Data analysis resulted in the development of a thematic network (see ). The thematic network comprised two Global Themes. The first, Competing Considerations, encompasses the child and communication aid factors that influence decision-making. This has been extensively addressed in a companion paper in this issue (see Murray et al., Citation2019) and, therefore, is not considered further in the current study. The second Global Theme, Cultural and Contextual Influencers, is considered here in detail. The results from the second global theme draw together the cultural and the contextual influences on decision-making within communication aid recommendations for the professionals, the child, and their family.
Table 3. Global themes, organizing themes, and basic codes.
Global theme 2: Cultural and contextual influencers
The data suggest that, in addition to the detailed consideration given to Child characteristics, Access features, and Communication aid attributes (Murray et al., Citation2019), decisions are further influenced by a host of cultural and contextual influencers. Cultural influencers originate from the context-specific work processes of the services provided and also from the child’s social, environmental, and support networks. The global theme was divided into three organizing themes: Ways of working, Transitions, and Available resources. Ways of working highlighted influencers from the service providers’ context, including family involvement in the team. Transitions related to the child’s journey as well as technology change in the wider context. Available resources reflected influencers related to the supports available to the child across home and service settings. In the following section, basic codes are presented alphabetically (i.e. ordering does not imply a hierarchy of importance), with example quotes illustrating responses from across the data. All names are pseudonyms, and all commercial products have been anonymized.
Ways of working
This organizing theme defines a range of service structures and team processes that potentially influenced the way decisions were made.
Balancing decisions
Participants reported that contextual factors sometimes meant that they had to make tradeoffs within their recommendations for individual children. For example, in recommending a new communication aid for Owen, the team considered how those in his support environment had managed the development and use of his previous communication aid. While they felt the language package on his first aid was best suited to his needs, they chose a different language system as a replacement based on the support available in his educational setting, as his specialist SLT described:
There has been a huge roll-through of different people around Owen in that time and the thread of using [named system] just got lost. Although it might have provided the best language opportunities at the time when we prescribed it, it didn’t end up [offering] the best language opportunities because it didn’t make a lot of sense to the people around him, especially in his [mainstream] school.
Contextual factors also led to tradeoffs in terms of how recommendation processes were carried out and the professionals’ expectations of children. For example, Noel’s team recognized his challenges in using a high-tech communication aid when his younger sister was present:
I’m quite glad his sister wasn’t there today but his sister is part of the family. I think it is important to do the assessment in the environment the person is in. If it means he can only use his system when his sister is at Granny’s house that would influence my recommendation. I would still be recommending it, but I know the opportunities for using it would be restricted (specialist SLT).
The data suggest that, in addition to making tradeoffs across child characteristics, access features, and communication aid attributes, professionals also had to consider the child in context. Considering context within communication aid recommendations resulted in compromises to ensure the aid was best aligned to the child in the context of his or her family and wider social network.
Basis for the referral
Participants indicated that the reason for referral often shaped the direction of the recommendation process. For example, Owen was referred for assessment as his current communication aid was very old and was no longer functioning as it should. The participants indicated that his referral information enabled a straightforward assessment recommendation process due to the family and young person’s existing understanding of AAC. However, sometimes the referral information suggested one type of process, but, in reality, a different process was needed. For example, Naraah’s specialized team considered that a referral indicated an equipment-only process was needed (i.e. where the local team identify the communication aid and the specialized team review and approve the local team’s decision): “On paper I think it looked almost like an equipment-only referral”. Instead, it turned out to be a fully specialized recommendation process (i.e. where the specialized team goes through the process of choosing a communication aid with the family). In another example, the referral information indicated that the child was at an early stage of communicative function, and the team prepared for the assessment accordingly. On meeting the child, they determined that she had a different profile of abilities that required a different preparation process: “So, from the referral, it sounded like Valerie was low level with language, so, we weren’t really expecting her to be as able” (specialist SLT). This suggests, in some instances, current referral information practices may not optimally support the team’s preparation for recommendation appointments. Another participant noted that the reason for referral may also influence the family’s expectations from the recommendation process. As some specialized services only provide technology-based solutions, the service structure may create expectations that it was inevitable that technology would be recommended: “When I first got involved with Noel’s family I felt, from the family, under pressure to come up with a high-tech solution. I suppose maybe that is also part of the referral too” (specialist SLT). Finally, specialist-led assessment teams discussed the need for children to be able to show them what they could do during their appointments. This was done so that they could confirm that the child reached the specialized service referral criteria for recommendation and provision of communication aid equipment: “These are the criteria. We need to [be certain that] Paul can do these things” (specialist SLT). For example, specialized teams described needing referral information in advance, but also needed to see the children perform similarly during the recommendation process in order for the professionals to sanction communication aid funding: “We’re just going to see Naraah today using this [aid] just so that we’ve seen it and can [rubber] stamp it” (specialist OT). Within the data, perspectives on the usefulness or otherwise of referral information and on the constraints of stated criteria for communication aid recommendation were pervasive and highlighted challenges within the decision-making and recommendation processes.
Extraneous factors
Extraneous factors referred to unconnected factors from within the context that influenced the decision-making. A key aspect that emerged was the role of luck in decisions. Luck was referenced regarding geographic location relative to the regional availability of the specialized service and regarding school placement: “I don’t think that Noel really needs it [sign support] that much now, which is fortunate because he’s not going to a school that signs” (local SLT). Sometimes, luck also played a role within the recommendation process itself. One professional described how they trialled Naraah with the equipment they had rather than what they would have chosen for her based on their clinical judgement. This chance occurrence informed their final choice of vocabulary layout: “I think, fortuitously, more by luck than judgement that it turned out to be quite enlightening to look at a slightly pared down vocabulary package” (specialist healthcare scientist).
How decisions are made
The theme of how decisions are made summarized the processes used by specialized teams that underpinned their decision-making during the assessment episodes. The specialized service structure was predicated on making recommendations based on information already gathered by the child’s local team. For example, Naraah’s specialized assessment team reported: “We didn’t do any assessment, language assessment per se because it’s already been done, which is an expectation” (specialist SLT). Instead of child-focused language and communication assessment tasks, the specialized recommendation episodes often involved discussion of available information to tease out the pros and cons of different communication aid choices: “We did talk around different [hardware] systems, with different purposes, (…) we’ve discussed everything we can think of over time” (local SLT). Also, team discussion was used to make a final communication aid decision where a shortlist of possible aids had been identified: “We had a lot of round the table discussion about, well are we going to go with this [named system], or with that [named system]” (local SLT). Another work process used to support decision-making was technology trials. During specialized assessment episodes, and in technology trials, teams provided children with the opportunity to engage with technology and gauged their response as a means to making decisions: “Sometimes you get something out (of) the cupboard, and you think, ‘Right, okay. We’ll give it a go’, and it works, or it doesn’t work, and then you try and work from there” (specialist clinical scientist). A range of technology trial formats were available, including activity-based trials within the appointment, 1–2 week-long loans, and extended trial periods of 6 months or more. Selection of equipment for the trial was informed by the referral information and available resources: “What I’d want to do is have some sessions with Mark on the other system, just playing around with it and seeing how he seems with it. I guess how fluid he seems with it” (specialist SLT). Longer trial periods were viewed as beneficial in that they allowed teams to evaluate future potential to “give Paul the experience of getting something from communication” (specialist clinical scientist).
Information brokering
A number of participants indicated that, within their service model, accessing all the desired information to make a recommendation could sometimes be challenging. Participants indicated that, in many instances, they were constrained by an inability to access all relevant information. Sometimes they made recommendations based on the available information with acknowledgment of the information gaps. There were different reasons for information gaps. For example, sometimes it was not possible to collaborate with those holding the relevant information, as one specialist SLT explained:
It was a shame that the therapist wasn’t able to make it, because we didn’t have a feel for what they are going to be using at that college and how they are going to be using it, and that’s almost an element of [the] unknown.
Similarly, the service structure precluded the team’s detailed assessment of the child’s abilities, as this function was the remit of the local service. As a result, teams were reliant on referral information and what was observable during the appointment. Her specialist SLT said:
It’s not always clear what Naraah communicates about at the moment. You know, from a linguistic point of view like her combinations and how she operates something, I don’t know what she talks about. So, it’d be really helpful to explore that a little bit more.
Some teams reported that service pressures at both local and specialized levels prevented information-sharing and collaboration at the time of the appointment: “It’s supposed to be a partnership, but in terms of time constraints from our service and also from a community point of view, we can’t say you have to come” (specialist SLT).
Despite the challenges reported in obtaining necessary information, teams also referenced work practices that they felt were supportive of effective information gathering. For example, one team described the benefits of the local professional attending the specialized appointment to share information on the assessment that had taken place at a local level: “And she also brought with her a report from their service on the trial that they’d written up which was extremely helpful” (specialist clinical scientist). Another described extensive information gathering in advance of the specialized appointment through phone calls: “It’s a lot of gentle questioning to parents and the local team, to find out what it is that’s difficult? What is not working? Why isn’t it working” (specialist OT).
Inheriting decisions
Another contextual factor raised by participants related to the recommendation processes for a second or subsequent communication aid. Comments from some participants highlighted the influence of the choice made for the child’s first communication aid in shaping the decision for their next communication aid: “It was another reason to pick the same machine from the same [communication aid] family that displays the letters with the same sort of size and shape and font” (specialist SLT). Participants indicated a desire to retain learning that has been invested in one type of system, suggesting that extra care is needed in these early decisions, as they may have ramifications over many years in the future.
Policy
One focus group highlighted how the wider policy context had the potential to influence the recommendation and change the decisions made by professionals. Participants identified a particular type of graphic representation that they felt best suited the child’s needs. However, they subsequently chose a different type of symbol as they felt there were too many potential challenges in obtaining support from the child’s school due to the local policy that was in place: “The local area has a policy where they’ve ranked all the symbol communication [language representation] systems in order of iconicity, and they’ve put [named symbols] at the bottom, and for that reason, they won’t use it in schools” (specialist SLT).
Roles and responsibilities
Participants reported a lack of role clarity in relation to making communication aid recommendations. Service structures and processes at times appeared to be barriers to effective collaborative working across all those involved in choosing communication aids for children. For example, one specialist SLT commented on the working relationships between specialized and local providers: “We’re not often seeing enough engagement from the local professionals. So we’re seeing a kind of referral [that suggests] over to us”. A local service provider reported a similar lack of shared responsibility beyond SLT for supporting children in her setting: “I think the flipside of being on staff means that [AAC] communication is just for us [SLT responsibility]” (local SLT). These perceptions and contextual realities highlight the challenges that lack of role clarity may have on collaborative working in communication aid recommendations.
Service delivery model
The particular service delivery model governing how the team operated had a considerable influence on the recommendation process. Two service delivery model factors that arose in the data were (a) the setting used for the recommendation evaluation, and (b) the timeframe available to the specialized team to make the recommendation. Recommendations were made in different settings across each focus group. Taking children out of their typical settings for the recommendation process was discussed as a limiting factor in some service delivery models. There was consensus across focus groups that observing children in their typical environments was important; however, it was not always practicable for all teams: “It is important to do the assessment in the environment that the person is in because it has to work in that environment” (specialist SLT). Participants reported that assessment in a clinical setting had variable impacts on children (i.e. affecting some children more than others), but that this location had benefits regarding access to a range of AAC resources during the process.
The time available to make a recommendation also differed across teams, ranging from a single appointment to a supported trial period of 18–24 months. These appointments appeared to be driven by contractual service delivery obligations, rather than informed by specific client needs. For example, one participant described the model she worked in: “On average, it’s about three times. It is a pure sort of diagnostic assessment service” (specialist SLT). Professionals discussed these different models and their influence on decision-making. For single appointments there appeared to be a greater emphasis on prior information gathering to maximize the appointment. In contrast, long trial periods appeared to defer decisions as teams waited to see how a child responded to experiences with a system: “I can potentially see this being like 18 months–2 years before we get to that point with provision” (specialist SLT). In some focus groups, recommendations made were not necessarily final decisions, but allowed for later changes, particularly where these longer assessment processes were used. Some participants indicated that their service model had flexibility so that they had the ability to change a recommendation at a later stage: “Actually if we get this wrong, and I’m not sure, wrong is probably a bit harsh, but if this needs changing, it can be” (specialist OT).
Team theory
Team theory is the final theme in Ways of working and references the theory used by teams to support decision-making. Many specialist participants described using implicit internal frameworks to underpin their decision making. Developed over time, their implicit frameworks drew on their professional education, recognized AAC and assistive technology models, and clinical experience. Different models were reported in each focus group with no common model identified. Participants indicated personal preferences for the named models: “ICF, we always use it. It’s kind of our template around [which] we will try really hard to look at participation activities and also thinking about (…) those personal environmental factors as well” (specialist SLT). Participants reported that these models guided their internal frameworks rather than being followed in a formalized way: “It’s something we all do consciously or unconsciously as a guiding principle. You start at the human and you work towards the technology and not the other way around” (specialist healthcare scientist). Profession-specific education also shaped their processes: “like my core skills as an OT, I don’t know about technology, but my core skills, my OT skills about physical skills, my knowledge about perception. You bring all those” (specialist OT).
Finally, clinical AAC experience also informed participants’ internal frameworks: “I personally use my own kind of internal framework that has kind of evolved with me because I have been in this service for a long time” (specialist SLT). Implicit, internal frameworks were supportive of decision-making, but were described as being very varied and posing a potential barrier to sharing knowledge. Frameworks that are inaccessible to others are potentially limiting to how others understand the decision-making processes, as one participant observed: “I don’t know if I am very good at being explicit. I think I have it more in my head, (…). But that’s not very helpful for passing onto people is it” (specialist SLT). Participants reported making their processes explicit when working with students or less experienced colleagues or clinicians. However, decision-making processes remain implicit when all professional members were experienced: “We have worked with Alison a lot, you know if it was a different therapist, you might have been explaining more, but we’ve known Alison for years” (specialist OT). Furthermore, implicit decision-making may make the process opaque to families limiting their opportunities to take on active roles: “It’s also not very good maybe at explaining to the families or to the relatives why it is you’re doing certain things. I think probably it does need to become a little bit more explicit” (specialist SLT).
Transitions
The organizing theme Transitions encompassed future planning for predicted changes as well as the broader change in technology in both commercial development and in a greater awareness and familiarity with technology from the public.
Future planning
Expected change in the child or young person’s future influenced decision-making. Such changes included planned or usual transitions in the child’s life (e.g. starting or leaving school) as well as unplanned changes (e.g. in services or setting). Impending transitions sometimes created a sense of pressure in making a timely recommendation: “So I am really keen to see some sort of decision being made on how she can go forward into the next setting” (Local SLT). Thinking about the future also affected decision-making related to the future role of the communication aid: “We were talking about giving Naraah some more opportunities to integrate within a mainstream school to give her that opportunity to participate in conversations with peers” (specialist OT). It was also important to consider with whom the communication aid would be used:
She’s also going to be in residential, [and] that’s a huge step. So, Mum is conscious that, at the minute, she comes home at ten past three, and she’s got this wonderful supportive, self-sufficient home set up and she isn’t going to have that for a while (specialist SLT).
Technology change
Another contextual factor discussed was the rapid development in technology and how the pace of technology change impacted on recommendations. Participants aimed to recommend the best available equipment, but felt their choices were often quickly superseded by better options on the market: “When we got him that communication aid the first time around, it was the best on the market. What is available on the market now is very different” (specialist SLT). To combat this challenge of keeping up with the latest available technology, participants described how they considered delaying their recommendation if they felt an enhanced option was likely to come onto the market: “The fact that technology is changing so quickly, that certainly is in there (as part of the decision-making)” (local SLT). Participants indicated that new technology features were important for some children as a means to obtain their buy-in: “We found him using the new communication aid a lot more, he was very much more eager to use it” (specialist SLT).
In summary, participants reported that expected changes in the child’s life sometimes created a sense of urgency in the recommendation process and, in other instances, decisions were influenced by predicted future needs and the potential role of the communication aid. The rapid change in technology also had potential to influence the timing of recommendations.
Available resources
The final organizing theme, Available resources, included: attitudinal support, financial resources, intervention input, general practical support, team-around-the child knowledge and skills, and on-going training available to support the communication aid recommendation.
Attitude
One intangible resource that influenced how teams made decisions was the attitudinal support of those around the child: “You don’t perhaps have that level of family buy-in either because they’re not at a level where they’ve accepted the idea of their child using AAC. That sometimes happens” (specialist clinical scientist). Where attitudinal support was missing, teams identified addressing attitudinal change through education as part of their communication aid recommendation process: “So gently helping parents to open that door to the value of having [a] communication aid [to enhance] the richness of their interaction with their child” (specialist OT). Participants indicated that more extended timeframes for recommendation processes might be advantageous to allow time for acceptance of AAC: “And I think his parents have come [on] a journey too” (specialist SLT). Furthermore, participants reported that a lack of buy-in across the child’s contexts would not prevent a communication aid being recommended, but it may limit their expectations of how it might be used, as one participant said: “We would prefer the device to be used across all situations and contexts. But we do get a lot of parents who just go, ‘Even if you send it home, I’m not going to use it’” (specialist healthcare scientist).
Cost
Discussion of the financial cost of purchasing communication aids was notably absent from most of the focus groups. This absence may reflect recent funding changes in parts of the UK, specifically England and Wales, where specialized services now have dedicated funding streams. These services can make recommendations based on clinical need within their referral criteria to access upfront funding. There was limited discussion of the financial cost of communication aids in two focus groups. One specialist SLT considered that financial cost was a deciding factor between communication aids that were perceived to function similarly, and they selected “the cheapest system that is sufficiently reliable” (specialist SLT).
Intervention
Professionals viewed that the intervention supports available to the child were likely to influence their choice of communication aid. Professionals perceived that some communication aids needed more implementation support than others, and they would not recommend these aids without access to a high level of intervention support: “Do you go through all that battle of teaching [named system]? Getting the staff on board would take a good year of our time” (Clinical Scientist). Others reported that they were less concerned about specific vocabulary features contained in their recommendation, as they considered that, if the recommendation was supported well with intervention, the particular language features were not especially important:
We could literally give her anything, and as long as it was administered, for want of a better word, in the right way, then, she would make as good a job with one thing as she would another (specialist SLT).
Support
Parental support was valued by participants and had an impact on the choice of communication aid. The available support from people in the environment influenced their recommendations: “Looking at my decisions around it, who went on [named system], who didn’t go on [named system], where they ended up, I think I probably put a lot more weight on the people around the child” (specialist SLT).
Team knowledge and skill
The knowledge and skills in team members around the child—including their family, were important considerations in choosing a communication aid for a child. Participants reported that teams viewed these systems more favourably in decision-making if the people around a child were familiar and confident with particular systems, as this enabled them to draw on existing knowledge and skill:
We know the local team are confident in using the software, that Naraah’s support needs are going to be handled mainly in-house, and that her team’s training needs are going to be relatively minimal (specialist healthcare scientist).
The fore-fronting of familiar communication aids in decision-making suggests that careful consideration needs to be given to the initial selection of communication aids in contexts like schools. Once a system is used by some school students, it may be more likely to be recommended to other students because of staff familiarity and experience. Participants emphasized that, while familiarity was taken into account, they would choose a less familiar system if there was good clinical reasoning to do so: “If we saw a child and the software was completely inappropriate, we’d never hesitate to talk with them about changing it. But if you’ve got those skills there already, it’s often easier to integrate” (specialist healthcare scientist).
Another aspect of team knowledge and skill that influenced the recommendation process was the shift towards democratization of AAC knowledge in people around the child. Participants reported that the internet and proliferation of information technology offered benefits in terms of all team members being able to share ideas and problem-solve creatively in identifying aids for children, as a specialist SLT explained:
Because we do get blinkered. You’re under pressure, and one has a huge caseload, you’re kind of frantically trying to do, so it sometimes is refreshing to have somebody saying what about x, y, z for this child? And, you think, actually ‘what about it? I wish I’d thought of that myself”.
Greater awareness of technology and AAC may be helping to reduce the fear of the use of communication technology. Participants viewed that learning how to edit or support a communication aid may be less daunting than it was in the past: “I wonder whether people’s familiarity with technology means that they aren’t so scared” (specialist SLT). However, discussion in the focus groups also reflected that this greater awareness of technology in those around the child may have its downsides. Participants commented on the portrayal of AAC in the media that might create false expectations of the technology being more advanced than it is in reality: “People have a perception of it as being something other than reality, because in the TV and films when you see someone using the system, it is very speedy” (specialist SLT). Similarly, easy access to information online can also create false expectations: “by a tap of a few buttons on a computer you can find everything on the devices out there, and you probably think look how easy it is to use, let’s go with that one” (specialist SLT). This dilemma highlights the need to openly discuss and develop a shared understanding of what communication aids might be able to achieve for a child within the recommendation process.
Participants expressed a preference for working with informed families, but also considered that the information gathered by families in advance can skew expectations and may result in too much focus on particular tools: “I am probably more being pushed into fitting people into existing systems on demand from somebody. It might not be the family, it might be the school” (specialist SLT).
Increased general awareness was also reported as an influence on referral patterns. Participants reported growth in families self-referring, specifically for high-tech communication aids and often for particular systems: “That’s new to us that pressure from someone for something specific. That’s a completely different ballgame for us, seeing that awareness” (Local SLT). Consequently, one specialized team was generating online resources to support families to have a realistic understanding and expectation of aided communication technology, to offer a balance to commonly available but potentially misleading information.
Training
Providing training for those around the child was an important consideration within the communication aid recommendation process. Training was often planned for as part of the communication aid set-up regime: “We’ve got to plan that and how much we can support and how much school can get skilled up to do what’s needed” (specialist SLT). Training for people around the child was also seen as essential to support everyone to feel comfortable with the communication aid recommendation:
A day a week gives you the opportunity to spend a bit of time every week with him, or with his team, or with the team at home to support that. To make sure everybody is feeling a little bit more comfortable even if he’s just comfortable getting lost [in navigating the aided system] (specialist OT).
In summary, these results suggest that there are multiple influencers impacting on decision-making processes for communication aid recommendations. These factors are external to the child, access, and communication aid features, and reflect the cultural perspectives and contexts in which AAC may be used by the child and young person.
Discussion
This study, the first in the UK to examine real-time decision -making in communication aid recommendations, reveals the inherent complexity in making those decisions. As previously demonstrated (Murray et al., Citation2019), communication aid recommendations are a product of a process where child characteristics, access features, and communication aid attributes are weighed up with consideration given to various permutations to identify the most appropriate communication aid for each child. However, this study confirms that these decisions are shaped by and distilled through cultural work practices, contextual influencers from the service provider, and contextual influencers from the child’s environment. The analytic framework suggests that some contextual influencers have an unduly large impact on the final decision and can consequently overturn the most appropriate communication aid as determined by feature-matching procedures. To illustrate this complex and dynamic interplay of characteristics and influencers, an explanatory model was developed (see ). The current findings as depicted in the model suggest that cultural and contextual influencers may have a considerable impact on the decisions made for children.
Figure 1. An explanatory model of specialist professional AAC decision-making.
Clinical implications
The results of this study suggest that service-related influencers substantially shape the decisions made. Despite the recent publication of service guidance for many parts of the UK (e.g. Scottish Government, Citation2018; SEN-DCP, Citation2014), which set out the vision for communication aid recommendations to be made in a child-centred way, current services offered to children appear to be determined by existing service structures and local service delivery models. The recommendation processes apparent in this study show that local service structures and delivery processes affect many facets of the recommendation, this includes the time available to make a recommendation, who is involved, what is done, and the funding that is available. In particular, the teams participating in the study varied in terms of size, professional backgrounds, service delivery models, and recommendation timeframes. The findings suggest that these variations in team composition appeared to be determined by service provision models rather than by children’s needs. For example, in one service, two children with the most significant physical impairments and access considerations were seen by an SLT but not by an OT. In another service, a specialist OT saw a young adult without a physical impairment and with minimal access considerations. This study supports prior research demonstrating that local service delivery models influence decision-making (Batorowicz & Shepherd Citation2011, Lindsay Citation2010). It is acknowledged that delivering communication aid recommendations will inevitably be influenced by service-related factors. However, it is important that service structure parameters should not unduly influence decisions over and above child need.
Furthermore, in the UK, the service delivery models have, in many instances, separated the assessment of child capabilities from the communication aid recommendation process. As an example, participants responsible for making recommendations took decisions, even while recognizing that they did not always have all the information they needed to make a fully informed recommendation. The data suggests a need (a) to build capacity for assessment at local level for children with complex communication needs, and (b) for more robust information-gathering processes at a specialized level to ensure recommendation processes are conducted with sufficient knowledge of child capabilities. Moreover, the split in service responsibilities (i.e. local and specialized) resulted in an undermining of collaborative working practices for professionals. For example, service structures and delivery processes inhibited collaborative working, whereby those local practitioners holding relevant information related to children being unable to be present for recommendation discussions. In addition, collaboration to support the recommendation process was more challenging for children who lived further away from specialized services. Collectively, these findings suggest a need for enhanced referral information-gathering processes. Effective collaboration may be enhanced by adopting novel service delivery models such as telehealth that would mitigate the need for travel yet allow those supporting children to be involved in recommendation discussions (Anderson et al., Citation2012). The use of telehealth may also reduce the inequity identified based on postal address (Anderson et al., Citation2012). Indeed, some specialized providers in the UK have used this practice for a number of years.
The findings also indicate UK professionals tend to make a recommendation for a communication aid, even when the contextual factors are not supportive of that decision. Participants indicated that unfavourable contextual factors would not prevent them making a recommendation, even though it sometimes changed the nature of the recommendation or their expectations for the child. This reflects a similar finding from a Canadian study (Lindsay, Citation2010). It raises questions as to whether contextual factors are given, or are having too much influence on communication aid recommendation processes. It is possible that professionals need to do more to identify, understand, and quantify contextual factors that have the potential to alter or limit aid recommendations.
Our findings suggest professionals may draw on implicit frameworks informed by theoretical knowledge and practical experience to manage the many considerations in decision-making. These internal decision-making processes may preclude the inclusion of, and participation in decisions by children, families, and professionals with less AAC experience. Implicit processes facilitated decision-making in communication aid recommendations, but also potentially masked the complexity involved in the recommendation by obscuring the key decision points for the child and their family. Previous research has indicated that families may be excluded or marginalized within decision-making (Batorowicz, & Shepherd, Citation2011) and may not be empowered to undertake a decision-making role (Serpentine, Tarnai, Drager, & Finke, Citation2011). There is a need for tools and supports to make decision-making processes more transparent and inclusive in the communication aid recommendation process.
A further contextual influencer that merits consideration from a service perspective is the rapid change in technology and how it impacts decision-making. Concerns about technology obsolescence related to the rapid rate of change in technology development did at times delay aid recommendations. It is recognized that children need access to aided language as early as possible (Cress & Marvin, Citation2003), and it is concerning that professionals might consider delaying a recommendation for a communication aid due to the pace of technology change. This finding suggests a need for collaboration between professionals making recommendations and suppliers of communication aids, to ensure future changes in technology are managed in a way that does not unduly interfere with recommendation processes.
Findings support existing literature that contextual factors from the child’s home and wider settings impact upon the nature of decisions made in recommendations (Batorowicz, & Shepherd Citation2011; Dietz et al., Citation2012; Lindsay Citation2010). The finding that a lack of attitudinal support from those in the environment might limit professionals’ expectations for the child’s communication aid use echoes the findings of previous research on aid abandonment, which also identified attitude and support as critical factors in successful outcomes (Johnson et al., Citation2006). A greater focus is needed on addressing external influencing factors during the recommendation process, in addition to goals for the child’s linguistic and communication development so that these do not contribute to device abandonment.
Finally, the findings indicate that decisions made for the child’s first high-tech communication aid may have potential ramifications for future communication aid recommendations. Participants indicated a desire to build on existing knowledge and skills and showed preferences for choosing communication aids within the same ‘family’ or of the same type as the first communication aid for subsequent recommendations. Given the potential long-term impact that those decisions may have, decision-making around the first communication aid needs to be carefully managed and include recognition of any unconscious bias towards technology of one type or another, and specifically how that relates to graphic language representation systems on offer within that technology.
Limitations and future directions
The present study has a number of limitations. While the study design reduced the potential for the research to impact on the child’s service, the exclusion of parents did not enable family perspectives to be included in understanding of decision-making processes. Furthermore, while the thematic network and explanatory model were developed from a relatively small but robust sample, the focus group results on cultural and contextual influences might not apply to children in other settings. Context-specific factors exerted considerable influence on decision-making processes, and, therefore, it could be expected that different influencers to the communication aid recommendation process may appear in other service structures. Researchers did not collect data on the professionals’ or children’s cultural background, age, or years of experience; or on the children’s socioeconomic status or family education. It was, therefore, beyond the scope of this research to identify any potential influence of these factors on decision-making processes. Future research could include consideration of these factors, and be inclusive of parents, to develop further the explanatory model proposed.
Conclusion
Cultural and contextual influencers may have a substantial impact on decision-making about communication aid recommendations. Existing research suggests that children and their families should be central to decisions affecting their future AAC outcomes (Parette, VanBiervliet, & Hourcade, Citation1999). Yet, the findings presented here indicate cultural and contextual influencers may prevent these key players having active roles in decision-making. Furthermore, these influencers, that have little to do with the child, may alter final communication aid recommendations, even to the extent of taking priority over feature matching processes (Murray et al., Citation2019). The impact of these influencers on decision-making should not go unrecognized if we are to better understand successful and less successful implementation of high-tech communication aid recommendations. Moreover, the findings suggest innovative and enhanced AAC service delivery practices are required to ensure the individual child’s needs remains at the heart of decision-making in communication aid recommendations.
2018-0069_Appendix_for_T_F_March_20.docx
Download MS Word (16.9 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Notes
1 The Hub and Spoke model of AAC service provision was commissioned by NHS England. The “Hubs” are specialized high-tech AAC assessment services whose personnel provide consultative services to children and adults who have especially complex requirements. The Hubs also have a responsibility to support service development for local, or “Spoke”, services that provide assessment and intervention to the majority of people who need AAC. This model does not exist in other parts of the UK.
References
- Anderson, K., Boisvert, M., Doneski-Nicol, J., Gutmann, M., Hall, N., Morelock, C., … Cohen, E. (2012). Tele-AAC resolution. International Journal of Telerehabilitation, 4, 79–82. doi:10.5195/ijt.2012.6106
- Angelo, D. (2000). Impact of augmentative and alternative communication devices on families. Augmentative and Alternative Communication, 16, 37–47. doi:10.1080/07434610012331278894
- Batorowicz, B., & Shepherd, T. (2011). Teamwork in AAC: Examining clinical perceptions. Augmentative and Alternative Communication, 27, 16–25. doi:10.3109/07434618.2010.546809
- Baxter, S., Enderby, P., Evans, P., & Judge, S. (2012). Barriers and facilitators to the use of high-technology augmentative and alternative communication devices: A systematic review and qualitative synthesis. International Journal of Language & Communication Disorders, 47, 115–129. doi:10.1111/j.1460-6984.2011.00090.x
- Beukelman, D., & Mirenda, P. (Eds.). (2013). Augmentative and alternative communication: Supporting children and adults with complex communication needs (4th ed.). Baltimore, MD: Brookes.
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3, 77–101. doi:10.1191/1478088706qp063oa
- Bryen, D., Chung, Y., & Lever, S. (2010). What you might not find in a typical transition plan! Some important lessons from adults who rely on augmentative and alternative communication. Perspectives on Augmentative and Alternative Communication, 19, 32–40. doi:10.1044/aac19.2.32
- Cress, C., & Marvin, C.A. (2003). Common questions about AAC services in early intervention. Augmentative and Alternative Communication, 19, 254–272. doi:10.1080/07434610310001598242
- Dietz, A., Quach, W., Lund, S.K., & McKelvey, M. (2012). AAC assessment and clinical decision-making: The impact of experience. Augmentative and Alternative Communication, 28, 148–159. doi:10.3109/07434618.2012.704521
- Goldbart, J., & Marshall, J. (2004). "Pushes and pulls" on the parents of children who use AAC. Augmentative and Alternative Communication, 20, 194–208. doi:10.1080/07434610400010960
- Gross, J. (2011). Two years on: Final report of the communication champion for children. https://www.rcslt.org/speechand
- Johnson, J., Inglebret, E., Jones, C., & Ray, J. (2006). Perspectives of speech language pathologists regarding success versus abandonment of AAC. Augmentative and Alternative Communication, 22, 85–99. doi:10.1080/07434610500483588
- Lindsay, S. (2010). Perceptions of health care workers prescribing augmentative and alternative communication devices to children. Disability and Rehabilitation: Assistive Technology, 5, 209–222. doi:10.3109/17483101003718195
- Matthews, R. (2001). A survey to identify therapists' high-tech AAC knowledge, application and training. International Journal of Language & Communication Disorders, 36, 64–69. doi:10.3109/13682820109177860
- Murray, J., Lynch, Y., Meredith, S., Moulam, L., Goldbart, G., Smith, M., … Judge, S. (2019). Professionals’ decision making in recommending communication aids in the UK: Competing considerations. Augmentative and Alternative Communication.
- National Health Service (NHS). (2018). Service specifications for complex disability equipment: Communication aids (specialised augmentative and alternative communication (AAC) services). Retrieved from www.england.nhs.uk/commissioning/spec-services/npc-crg/group-d/d01/
- Parette, P., VanBiervliet, A., & Hourcade, J. (1999). Family centered decision making in assistive technology. Journal of Special Education Technology, 15, 45–55. doi:10.1177/016264340001500104
- Ryan, S., Shepherd, T., Renzoni, A., Anderson, C., Barber, M., Kingsnorth, S., & Ward, K. (2015). Towards advancing knowledge translation of AAC outcomes research for children and youth with complex communication needs. Augmentative and Alternative Communication, 31, 137–147. doi:10.3109/07434618.2015.1030038
- Scottish Government. (2018) Guidance of the provision of communication equipment and support in using that equipment. https://beta.gov.scot/binaries/content/documents/govscot/publications/guidance/2018/05/guidance-provision-communication-equipment-support-using-equipment/documents/00535995-pdf/00535995-pdf/govscot:document/
- Serpentine, E., Tarnai, B., Drager, K., & Finke, E. (2011). Decision making of parents of children with autism spectrum disorder concerning augmentative and alternative communication in Hungary. Communication Disorders Quarterly, 32, 221–231. doi:10.1177/1525740109353938
- Smith, M., Murray, J., von Tetzchner, S., & Langan, P. (2010). A tale of transitions: The challenges of integrating speech synthesis in aided communication. In J. Mullennix & S. Stern (Eds.), Computer synthesized speech technologies: Tools for aiding impairment (pp. 234–256). New York, USA: Medical Information Science Reference: IGI Global.
- Special Educational Needs and Disability Code of Practice: 0-25 years. (2014). Statutory guidance for organisations which work with and support children an young people who have special educational needs or disabilities. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/398815/SEND_Code_of_Practice_January_2015.pdf