
Abstract
A randomized controlled trial was carried out to investigate effects of heightened mortality awareness on meaning in life and attitudes toward dying and death. An intervention group (n = 51) completed questionnaires and participated in interventions to increase mortality awareness; a control group (n = 47) only completed the questionnaires. Longitudinal analyses revealed a decrease in the intervention group’s fear of dying and an increase in their acceptance of dying, but no effects on attitudes toward death. Changes in meaningfulness were contingent on participants’ religiousness. Unexpected cross-sectional results and the study’s implications for theory and further empirical work are discussed.
According to the existentialist philosophies of Søren Kierkegaard and Martin Heidegger, human beings can adopt one of two different stances toward their own death: The first one, described as Mood by Kierkegaard (Citation1993) and as inauthentic Being-toward-Death by Heidegger (Citation1996), is a defensive, externally orientated, and basically unreflected attitude, which distracts us from the factum of our own mortality. This “way of being” is characterized by living one’s life along common opinions and customs, by repression and avoidance of death thoughts, and by hushing up one’s own mortality and its consequences for life. The other possible stance—Earnestness or authentic Being-toward-Death—can be described as a mindset in which one fully accepts one’s own finiteness by acknowledging that death is undetermined in its time, is not substitutable to someone else, and represents an irreversible event whose incidence has already been certain since birth. According to Kierkegaard and Heidegger, these insights throw the individual back upon itself and its existence and therefore can lead to a reevaluation of central values and goals in life.
Defense and growth
Both described ways of coping with death are represented by psychological theories. Terror Management Theory (TMT; for an overview, see Solomon et al., Citation2004) is a well-established theory, positing that people primarily react on the terror resulting from subtle reminders of our mortality (mortality salience, MS) by defensive, unconscious strategies. These manifest in an increased orientation toward culturally shared worldviews and in striving to boost one’s own self-esteem, which in turn is seen as generally related to social values and norms. Both strategies are hypothesized to serve as buffers and decrease existential anxiety arising from a confrontation with one’s own mortality.
Although advocates of TMT acknowledge the possibility of personal growth resulting from a confrontation with death (e.g., Pyszczynski et al., Citation2006), TMT has been criticized for reducing such processes to indications of self-esteem-boosting in order to buffer death anxiety. According to this critique, TMT interprets personal growth as merely defensive in its nature and not as an expression of pursuing intrinsic, basic human needs (Crocker et al., Citation2004; Ryan et al., Citation2004; Wong & Tomer, Citation2011). Two points might be mentioned in reaction to suchlike critical comments: First, the defensive terror management processes described by TMT need not always be negative (in a normative sense) in their (inter-)personal outcomes (e.g., devaluation of others holding divergent worldviews), but can lead to quite positive effects on, for example, social and health-related behavior (for an overview, see Vail et al., Citation2012). Second, the founders of TMT do not see the defensive and death-denying motives as the only or in any way superior driving force underlying human behavior, as some critics seem to imply. Rather, in an early TMT-article, Greenberg et al. (Citation1995) posit that defensive as well as growth-oriented motives both guide human lives and stand in a mutual, dialectical relationship. From a TMT perspective, however, defensive needs must first be addressed before growth can take place (Greenberg et al., Citation1995; Pyszczynski et al., Citation2006).
While research on TMT focuses on defensive processes, other authors and theories (e.g., Crocker et al., Citation2004; Martin et al., Citation2004; Wong, Citation2008) put more emphasis on growth-orientated motives. They argue that becoming aware of one’s own mortality may indeed induce anxiety and paralysis (and therefore the need for defensive actions) but can—at least under certain circumstances—also serve as a source of energy, resolve, and enthusiasm. Based on findings from research on post-traumatic growth (Tedeschi & Calhoun, Citation1995) and near-death experiences (Ring, Citation1984), Cozzolino (Citation2006) proposed a model of two existential systems. This model states that in contrast to the abstract MS-exercises typically used in TMT-studies (usually two short, open-ended questions concerning feelings and thoughts about one’s own death; see Rosenblatt et al., Citation1989), more specific, personalized, and intense forms of creating an awareness of mortality are likely to activate growth-oriented motivational states and self-regulatory processes (see also Cozzolino & Blackie, Citation2013). And indeed, as several empirical studies suggest, a conscious and vivid contemplation of one’s own death is able to promote personal growth, such as higher intrinsic goal orientation, less selfishness, enhanced identity integration, and an increased sense of authenticity (for an overview, see Rogers et al., Citation2019). From a Meaning Making Model perspective (Park, Citation2010), a serious confrontation with one’s own mortality can be regarded as a stressful event, which has the potential of challenging an individual’s global meaning system (e.g., central beliefs and goals), and therefore may lead to a reevaluation of and even changes in personal life orientations and values.
With his Meaning Management Theory (MMT), Wong (Citation2008) provides a complementary theoretical framework to TMT in which a non-defensive way of coping with one’s own finiteness is described as a tripartite interplay between death anxiety, death acceptance, and meaning in life (MIL): To seek and (re-)construct meaning in life is seen as a necessary foundation for establishing an attitude of death acceptance. Anxiety related to death should thus be reduced, which in turn is a basis for a fulfilled and happy life (see also Wong & Tomer, Citation2011). To view one’s life as meaningful, while at the same time acknowledging the factum of one’s own mortality, can be understood as a form of personal growth, as overcoming or at least attenuating defensiveness and therefore approaching a more authentic and autonomous orientation in life.
Although at present the relationship between death acceptance and meaning in life lacks empirical support, negative correlations of death anxiety and meaning in life have repeatedly been reported in the literature (e.g., Ardelt, Citation2008; Durlak, Citation1972; Rappaport et al., Citation1993). The same holds for the inverse relationship of death anxiety and death acceptance (e.g., Wittkowski, Citation1996; Wong et al., Citation1994).
Death education research
So-called “death-education” programs use didactic as well as experiential forms of intervention (for this distinction, see Durlak, Citation1994) to encourage participants to reflect on their own mortality. They are also based on the assumption that a conscious and longer-term confrontation with one’s own mortality can result in positive outcomes. Meta-analyses, however, yielded inconsistent results regarding the effectiveness of such programs in changing individual attitudes toward dying and death: While a study by Menzies et al. (Citation2018) came to the conclusion that death education had no significant effect on death anxiety, Maglio and Robinson (Citation1994) reported that, on average, death anxiety increased after such interventions, whereby didactic programs produced substantially higher increases in death anxiety than experiential interventions. Durlak and Riesenberg (Citation1991), on the other hand, concluded that experiential forms of death education were moderately effective in decreasing death anxiety and fear of death, whereas didactic programs rather led to an increase in these variables. Most studies on death education used death anxiety and fears related to death and/or dying as outcome measures. Few also included death acceptance, but up to now, to our best knowledge, no study investigated meaning in life as an outcome.
Findings from research on terror management theory
As for research on TMT, the effects of MS on meaning in life were investigated solely within experimental settings, showing significant differences in participants’ ratings of meaning in life after an MS-intervention. The results were contradictory, however: While some findings supported the hypothesis that MS increases the experience of meaning in life (Davis & McKearney, Citation2003; King et al., Citation2009), others actually indicated a decrease of meaning in life (Routledge et al., Citation2010; Taubman-Ben-Ari, Citation2011). The two latter studies identified dispositional self-esteem as an important moderator variable in this context: MS only led to a significant decrease in MIL for participants low in self-esteem, but not for participants with high self-esteem (thus supporting the assumption of self-esteem as a buffer against existential threats). Further results suggested that MS increases the search for meaning in life (again only for those low in self-esteem, Juhl & Routledge, Citation2014; see also McGregor et al., Citation2001). In an experiment by Routledge and Juhl (Citation2010), MS led to higher death anxiety for participants who rated their lives as less meaningful, in contrast to those who reported high meaning in life. The latter effect is interesting because it underlines the supposed protective function of meaning in life against death anxiety, as mentioned above. Irrespective of the different operationalizations of MS and meaning in life, these findings seem to suggest that a confrontation with one’s own mortality may at least raise existential questions. These, in turn, may consolidate or challenge a given meaning in life—or even motivate a person to start searching for meaning in life for the first time, depending on the individual starting point and the relationship to oneself (self-esteem). This line of reasoning would also be in accordance with the already mentioned Meaning Making Model by Park (Citation2010). It should be noted, though, that the cited findings are entirely based on experiments. They do not allow for conclusions regarding the longitudinal development of meaning in life after an MS-exposure.
The present study
The present study aims at expanding previous research on the interplay between an increased awareness of one’s own mortality, individual attitudes toward dying and death, and judging one’s life as meaningful. It is the first attempt to survey potential longer-term effects of a confrontation with one’s own mortality on evaluations of meaning in life. Therefore, the assumption of a threefold relationship between MIL, death anxiety, and death acceptance, as stated by Wong (Citation2008), can be tested longitudinally as well as cross-sectionally. In contrast to studies within the theoretical framework of TMT, which typically use short and subtle reminders of death, the present study operationalizes this confrontation as an intense, personalized, and longer-term intervention, designed to stimulate a conscious and comprehensive encounter with different facets of one’s own mortality. Hence, it is subsequently labeled as “mortality awareness” in order to distinguish it from typical MS-tasks.
Meaning in life and attitudes toward death are assessed by multidimensional measures, thus taking into account the possibility of differential relationships. Meaning in life is operationalized by both meaningfulness and crisis of meaning (which do not show a straight inverse relationship, see Schnell, Citation2009, Citation2010). The multidimensional nature of attitudes toward dying and death is represented by distinguishing the two qualities of fear and acceptance as well as by differentiating attitudes toward death from attitudes concerning the process of dying (Wittkowski, Citation1996). Because self-esteem has proven to be an important factor in how individuals cope with a confrontation with their own mortality (see above), it is included in our investigation as a potential moderator variable.
Drawing on theoretical assumptions which emphasize the potential of personal growth due to an honest and unbiased stance toward one’s own dying and death, it is hypothesized that participants whose mortality awareness is increased will show higher levels of meaningfulness, lower levels of crisis of meaning, higher levels of acceptance of their own dying/death, and lower levels of fear of their own dying/death at the end of the investigation period, compared to participants in the control group. Meaningfulness is expected to correlate negatively with fear of one’s own dying/death and positively with acceptance of one’s own dying/death, while the inverse is expected for crisis of meaning.
Method
The study was reviewed by the University of Innsbruck’s Board for Ethical Questions in Science and was granted ethical clearance.
Recruitment of participants
Participants were recruited via Facebook and the internal e-mail system of the University of Innsbruck. To minimize the risk of mental harm due to the personal and potentially frightening or disturbing interventions during the course of the study, participants were first screened for depression (PHQ-9; Spitzer et al., Citation1999) and anxiety symptoms (GAD-7; Spitzer et al., Citation2006) by means of an online survey. Participants were invited to the initial meeting of the study (T0) if their scale scores were below the recommended cutoff points (e.g., Kroenke et al., Citation2010). Of the 183 persons who completed the online survey, 145 met the criteria. They were invited and randomly assigned to either the intervention group (mortality awareness) or the control group. Of those who were invited, 98 attended the initial meeting. The mortality awareness group thus consisted of 51 (= n1) and the control group of 47 (= n2) participants at T0. Written informed consent was obtained at this point, prior to any measurement or intervention, and participants were told that they could quit their participation at any time without giving reasons. Students received course credit for their participation.
Participants
The participants’ age ranged from 18 to 58 (M = 25, SD = 8, Mdn = 22) and 70% were female. All the participants had graduated from high school and 87% were currently studying at university. The majority was born in Germany (60%) or Austria (36%). Forty-six percent self-described as Christian, 31% as atheistic, 16% as agnostic, and 3% as Buddhist (remaining: 1% other, 3% no response). Intervention and control group members did not differ significantly (p > .05) in demographics or baseline values of psychological measures (described in the next section). Randomized assignment can therefore be considered successful.
Materials
Mortality awareness
In contrast to often used single tasks to (unconsciously) activate death-related affects and/or cognitions, we employed a series of different interventions over a period of seven weeks. Thus, following an experiential rather than a didactic approach, participants were encouraged to (consciously) reflect upon their mortality in an intense and personal manner. The intervention group worked on mortality awareness (MA) tasks partly individually at home (MA2, MA3, MA5b), partly at the university lab, in groups of 10–20 persons (MA1, MA4, MA5a). In the end of the latter tasks, participants were encouraged to discuss and reflect their feelings, thoughts, personal impressions, and critique or unease concerning the specific exercise or the study in general (for the central role of group discussions in death education programs, see Durlak, Citation1994).
Mortality awareness was operationalized and implemented through five different tasks:
As first MA-task (MA1), participants completed the German SESTD-questionnaire by Klug (Citation1997), a series of twenty open-ended sentences related to dying, death, and “the afterwards.” Examples are “Regarding dying, I fear …,” “When I think of my death, I …” or “After death, I expect ….” (Session duration: ca. 15 min)
As second MA-exercise (MA2), a variant of the standard MS-induction in TMT-studies by Rogers (Citation2011) was used, which consisted of two open-ended questions concerning a personally meaningful/ideal death. (Session duration: ca. 15 min)
For the third MA-intervention (MA3), participants were asked to imagine they were diagnosed with a terminal disease during a medical routine screening, and that their remaining lifetime was restricted to a maximum of four weeks. Participants should then contemplate several questions under this premise, e.g., how they would evaluate their life and their priorities so far, if they felt any retrospective regrets, etc. They then had to express the results of this reflection in a short essay. (Session duration: ca. 60 min)
The fourth task (MA4) was a Buddhist meditation exercise based on a text by Halifax (n.Citationd.), which was translated into German. Themes of this meditation, which consists of nine tenets, cover the inevitableness of death, the uncertainty of its time and cause, the fundamental subjectivity of death, as well as consequences of these considerations for one’s personal way of life. The guided meditation was implemented using an audio-recording of the text and meditative background music. Participants were encouraged to sit on the floor, close their eyes during the exercise, or otherwise ensure a comfortable setting for the meditation (Session duration: ca. 60 min).
The fifth intervention consisted of two parts: During a group excursion to a local funeral home, participants became acquainted with different psychological, societal, and legal considerations in dealing with the dead (MA5a). The second part of the final MA-intervention (MA5b) was—again—the writing of an essay. This time, participants had to imagine their own funeral, draft a detailed plan of their mourning ceremony, and write about their preferred form of burial. (Session duration: ca. 120 + 60 min).
Measures
To operationalize the two qualities of meaning in life, meaningfulness and crisis of meaning, the respective subscales of the German version of the SoMe questionnaire (LeBe, Schnell & Becker, Citation2007; for the English version, see Schnell, Citation2014) were applied. Both scales consist of five items and use a 6-point Likert scale, from (0) strongly disagree to (5) strongly agree. They show good internal consistencies as well as high short-term stability. Test-retest stability was found to be still high after six months for meaningfulness, but lower for crisis of meaning (Schnell, Citation2009). Validity of the SoMe has been demonstrated in numerous studies (for an overview, see Schnell, Citation2014). In the present study, internal consistencies were .70–.80 for meaningfulness (sample item: “I lead a fulfilled life.”) and .86–.93 for crisis of meaning (sample item: “My life seems meaningless.”).
For the assessment of attitudes toward dying and death, the FIMEST-R by Wittkowski (Citation1996) was employed. It allows for assessment of the following death-related constructs: Fear of one’s own dying (10 items; observed α’s = .87–.88; “The possibility of losing my personal dignity when I am dying appalls me.”), fear of one’s own death (12 items; α’s = .94–.95; “I am frightened by the idea that all my thoughts and feelings will stop when I am dead.”), acceptance of one’s own dying (8 items; α’s = .84–.86; “The dying process contributes toward rounding off my life.”), and acceptance of one’s own death (11 items; α’s = .94–.95; “Somehow, the knowledge of my death is a part of my life that I view positively.”). The FIMEST-R uses a 4-point Likert scale, from (0) agree not at all to (3) agree almost totally.
Several demographics were assessed: gender, age, nationality, family status, highest educational degree, current employment status, and religion. In the demographic questionnaire (DemQ), participants were also asked how intensely they had given thought to their own dying and death so far (1 item, 7-point Likert scale: (0) not at all to (6) very intensely). Additionally, dispositional self-esteem was assessed using the revised German version of the well-established Rosenberg-scale (RSES; Von Collani & Herzberg, Citation2003; observed α = .82). The 10 items of the RSES are scored using a 4-point Likert scale, from (0) strongly disagree to (3) strongly agree.
Procedure and preliminary analyses
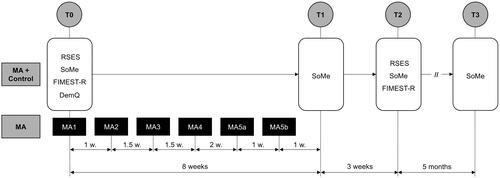
At the initial meeting (T0), members of both groups completed the RSES, the SoMe-scales, the FIMEST-R, and the demographic questionnaire. The control group then left, while the mortality awareness group worked on the first MA-task (MA1). For the next seven weeks, the same participants completed the remaining MA-exercises, either at home or on-site. One week after MA5b a first, very short interim survey (T1; N = 90, n1 = 45, n2 = 45) was administered online, assessing the degrees of meaningfulness and crisis of meaning in all participants. Three weeks later the main outcome measurement (T2; N = 87, n1 = 46, n2 = 41) took place in the university lab, again employing the SoMe as well as the FIMEST-R (note that one participant in the MA-condition attended T0 and T2, but not T1). At the end of T2, the primary investigation ended, and all participants were fully debriefed and thanked for their participation. Five months later an additional and optional ad-hoc assessment (T3; N = 67, n1 = 36, n2 = 31) was conducted to control for possible longer-term changes in the MIL-dimensions meaningfulness and crisis of meaning.
It seemed plausible to us that changes in meaning in life following mortality awareness might occur in a complex sequential manner, e.g., crisis of meaning could increase initially and diminish again after meaning structures had been adapted, whereas meaningfulness might behave inversely. Therefore, the meaning qualities were tracked more thoroughly in comparison to the mortality-related outcome dimensions, i.e., an additional interim measurement (T1) as well as a follow-up survey (T3) were carried out for meaningfulness and crisis of meaning, but not for the other measures (see ).
Figure 1. Study protocol.
Data were screened for univariate and multivariate outliers prior to further analyses. In sum, three univariate outliers were detected and their impact was reduced by winsorization (see Tabachnick & Fidell, Citation2013). No multivariate outliers were detected. Following the recommendations by Dumville et al. (Citation2006), attrition rates were analyzed. The analyses did not indicate any structural biases. The effect size measure for independent samples t-tests (gs, an unbiased estimate of Cohen’s d) was chosen and labeled following Lakens (Citation2013) and calculated—with 95% CIs—using an online software application by Uanhoro (Citation2017). For the hierarchical linear models (see below), an estimate of effect size (d incl. 95% CI) is given following the recommendations of Feingold (Citation2015).
As for demographics, several noteworthy group differences were found: Women (n = 69) reported higher rates of fear of their own death (t(73.59) = −3.19, p = .002, gs = −0.60, 95% CI [−1.05, −0.16]) than men (n = 28). Participants in a relationship (n = 55) were lower in crisis of meaning than singles (n = 43; t(75.73) = 2.11, p = .038, gs = 0.44, 95% CI [0.04, 0.85]). Religious persons (n = 49; denominations combined) showed higher values in meaningfulness (t(93) = 2.28, p = .025, gs = 0.46, 95% CI [0.06, 0.88]), acceptance of their own dying (t(93) = 2.26, p = .026, gs = 0.46, 95% CI [0.05, 0.87]), as well as self-esteem (t(93) = 2.02, p = .046, gs = 0.41, 95% CI [0.01, 0.82]), and lower values in crisis of meaning (t(93) = −2.09, p = .039, gs = −0.43, 95% CI [−0.84, −0.02]) than secular participants (n = 46; atheists and agnostics combined due to the small number of each).
Age as well as the intensity with which participants had previously given thought to their own dying/death did not correlate significantly with any of the other measures. Self-esteem was positively associated with meaningfulness and acceptance of one’s own dying, and negatively with crisis of meaning and fear of one’s own death (see ).
Table 1. Correlation matrix and descriptive statistics for continuous variables at T0 (N = 98).
Results
Cross-sectional results
To test the cross-sectional hypotheses, Pearson correlations were computed (see ). Of all FIMEST-R dimensions, only acceptance of one’s own dying was significantly related to meaning in life: r = .23 for meaningfulness, r = −.25 for crisis of meaning.
Longitudinal analyses
Model building
To examine potential effects of our MA-treatment on the six outcome measures, hierarchical linear models (HLM) were computed using the statistical software R (R Core Team, Citation2019) and the nlme-package (Pinheiro et al., Citation2019). Each outcome variable was examined in a separate two-level model (time points nested within participants); model estimates were obtained using maximum likelihood estimation (ML). The first step of any analysis was to build a null model containing a random intercept but no other predictors. For all outcomes, the null model fitted the data significantly better than a model with a fixed intercept only (using χ2 likelihood-ratio tests, all p’s < .001; see Tabachnick & Fidell, Citation2013). Intraclass correlations were high, between .72 and .91, underpinning the adequacy of a multi-level analysis (see Tabachnick & Fidell, Citation2013). In a second step, the level-1-predictor “time” was included as a fixed effect in the model. To account for the longitudinal design of our study, we tested whether a first-order autoregressive covariance structure improved the model (using corCAR1() due to unequally spaced time points; see Field et al., Citation2012). For meaningfulness (χ2(1) = 4.59, p = .032) and crisis of meaning (χ2(1) = 8.30, p = .004), a model that allowed for autocorrelation fitted the data significantly better than the previous model, which assumed no autocorrelation. For the dying- and death-variables, including autocorrelation did not improve the model (χ2(1)’s = 0.00, p’s > .999); therefore, the default covariance structure of lme was maintained for these outcomes. As a final step, the level-2-predictor “group” was included in the models. displays the results of the final models. In , estimated marginal means (time × group) for the final models, calculated with the emmeans-package (Lenth, Citation2019), are reported.
Table 2. Results of the HLM analyses (final models).
Table 3. Estimated marginal means for final models.
HLM main results
As can be seen in , the expected time × group-interaction was only significant for acceptance of dying (p = .002), nearly significant for fear of dying (p = .072), but not for the other DVs (all p’s > .251). For acceptance of dying, the significant interaction was broken down by conducting a simple slope analysis using the reghelper-Package (Hughes, Citation2018). The analysis showed that in the mortality awareness group the time-effect was significant (b = 0.18, SEb = 0.03, t(85) = 5.85, p < .001, d = 0.25, 95% CI [0.16, 0.34]), whereas in the control group it was not (b = 0.04, SEb = 0.03, t(85) = 1.19, p = .239, d = 0.06, 95% CI [−0.04, 0.16]). For fear of dying, where the interaction-effect approached significance (p < .10), the simple slope analysis yielded an almost significant effect of time in the mortality awareness group (b = −0.06, SEb = 0.03, t(85) = −1.77, p = .081, d = −0.09, 95% CI [−0.19, 0.01]), but not in the control group (b = 0.03, SEb = 0.04, t(85) = 0.84, p = .403, d = 0.05, 95% CI [−0.07, 0.17]).
HLM further analyses
Because previous research suggests that individuals’ reactions to death-related stimuli depend in part on their level of dispositional self-esteem (see above), we conducted moderation analyses by including self-esteem (grand-mean centered) as a fixed predictor (incl. all two-way- and the three-way-interaction) in the models. First, the inclusion of self-esteem did not alter the main results of the preceding section: The treatment-effect of mortality awareness (two-way interaction time × group) was still significant for acceptance of dying (b = 0.15, SEb = 0.05, t(83) = 3.26, p = .002, d = 0.22, 95% CI [0.09, 0.35]), nearly significant for fear of dying (b = −0.10, SEb = 0.05, t(83) = −1.95, p = .054, d = −0.15, 95% CI [−0.30, −0.00]), but not for any other outcome (p’s > .204). The three-way interaction between time, group, and self-esteem was non-significant for all dependent variables, although it approached significance (p < .10) in the case of fear of death (b = 0.02, SEb = 0.01, t(83) = 1.83, p = .071, d = 0.02, 95% CI [−0.00, 0.05]). Dispositional self-esteem did thus not moderate the effect of mortality awareness on the measured outcomes.
Apart from self-esteem, also participants’ religiosity could be hypothesized as a moderator regarding the effects of mortality awareness (see, e.g., Vail et al., Citation2010; Vail & Soenke, Citation2018). Thus, we tested whether our demographic variable religion (dichotomous: religious/secular) moderated the time × group-interaction in the HLM models, similarly to the analyses described for self-esteem. By including religion in the model, the time × group-interaction was still significant for acceptance of dying (b = 0.17, SEb = 0.07, t(80) = 2.61, p = .011, d = 0.26, 95% CI [0.07, 0.45]), but did not reach significance for fear of dying (b = −0.02, SEb = 0.07, t(80) = −0.25, p = .800, d = −0.03, 95% CI [−0.25, 0.19]) or any other outcome (p’s > .107). The time × group × religion-interaction was solely significant in the case of meaningfulness: b = −0.17, SEb = 0.08, t(232) = −2.03, p = .044, d = −0.59, 95% CI [−1.16, −0.02]. To unpack this three-way-interaction, a simple-slope analysis for the time-effect, depending on group and religion, was conducted. As can be seen in and , there was no significant time-effect in the control group, neither for religious nor for secular participants. However, in the mortality awareness group there was a significant decrease in meaningfulness over time for the secular, but not for the religious participants, for whom meaningfulness rather increased (albeit not significantly).
Figure 2. Three-way interaction between time, group, and religion in predicting meaningfulness (estimated marginal means are displayed).
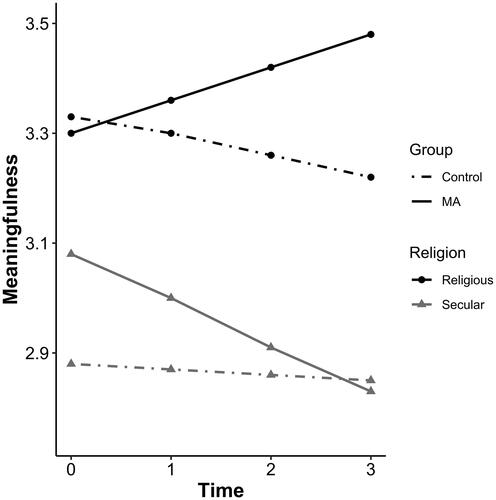
Table 4. Results for the time-effect on meaningfulness, depending on group and religion (three-way-interaction).
Previous investigations as well as the present study suggest that acceptance and fear of one’s own mortality are mutually related. Regarding the causal sequence, it seems conceivable that to reduce fear, one might have to establish an attitude of accepting one’s own mortality first. Concerning the present study, this would be the case if the effect of mortality awareness on fear was mediated by acceptance (i.e., due to an increase in acceptance, fear would decrease). Because we did not find any treatment-effect for fear and acceptance of death, we tested this hypothesis for fear and acceptance of dying. As reported, the direct effect of our MA-treatment (time × group-interaction) on fear of dying was almost significant (path c, p = .072), whereas the effect on acceptance of dying (the potential mediator in question) was significant (path a, p = .002). To test the indirect effect of mortality awareness (operationalized as time × group-interaction) on fear of dying via the mediator, we included acceptance of dying as a fixed predictor in the model for fear of dying. CIs for the indirect effect were computed using the RMediation-package (Tofighi & MacKinnon, Citation2011). The effect of acceptance of dying on fear of dying was significant (path b, p < .001). Accounting for this significant mediation, the direct effect of MA on fear of dying was not significant (path c’, p = .399). The indirect effect of MA (path ab, p = .013) accounted for roughly half of the total effect, PM = .51. The results of the mediation analysis are displayed in and .
Figure 3. Results of the mediation analysis for fear of dying. Unstandardized regression coefficients are given. The direct effect controlled for the mediation (bc’) is presented in parentheses. Mortality awareness represents the time × group-interaction here. Significance levels: †p < .10, **p < .01, ***p < .001.
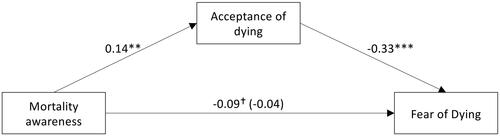
Table 5. Mediation analysis for fear of dying, predicted by MA via acceptance of dying.
Discussion
The present study was designed to examine effects of a longer-term mortality awareness intervention on dimensions of meaning in life and attitudes toward dying and death, as well as cross-sectional relations between these variables. As the longitudinal analyses suggest, mortality awareness led to an increase in participants’ acceptance of their own dying. Also, their fear of their own dying decreased over time, albeit not significantly. No MA-effects were found for the respective death-related dimensions. A possible explanation for this differential impact of mortality awareness on attitudes toward dying versus those toward death could lie in the respective base levels of these variables: In the entire sample, fear of death was low, thus leaving much less room for changes than fear of dying, which was more marked. The same was true for acceptance of dying and death, with acceptance of death being quite high from the start. Such differences between attitudes toward dying and death are in line with previous findings by Wittkowski (Citation1978, Citation1996) who reported that people usually fear dying more than death, and that they are able to accept their death more easily than their dying. The differential effects of MA on attitudes toward dying vs. death may therefore be caused by the more positive view on death at baseline. This finding might indicate a floor effect for fear of one’s own death and a ceiling effect for acceptance of one’s own death, respectively—an interpretation which is supported by the actual distributions of the variables, as can be seen in . From another perspective, these distributions might also be interpreted as an indication of death denial (i.e., understating anxiety and exaggerating acceptance). This reading would question the possibility of measuring death-related constructs explicitly. Future studies could circumvent potential biases through death denial processes by employing implicit measures of death attitudes.
Whatever the explanation for this finding, it might be the reason for contradictory results of meta-analyses on the effectiveness of death education programs: Previous studies might either have focused solely on fear of death, confounded fear of death with fear of dying, or investigated fear of dying rather than death anxiety. Special attention should thus be paid to labeling, distinguishing, and defining psychological constructs concerning dying and death to improve comparability.
When analyzing the results related to attitudes toward one’s own dying in more detail, we found that fear of dying was affected by mortality awareness more indirectly than directly via an altered level of acceptance toward one’s own dying. It seems, in line with assumptions by Wong (Citation2008) and others, that we must first establish an attitude of acceptance toward our own mortality to decrease fears and anxieties related to it. However, this sequential relationship was only present for attitudes toward dying, not for attitudes toward one’s own death, where no changes over time were observed.
Probably the most unexpected result of this investigation is the absent correlation between experiencing one’s life as meaningful and not fearing dying/death. No combination of meaningfulness/crisis of meaning and fear of one’s own dying/death yielded significant correlations, which contrasts previous research that repeatedly showed inverse relationships between meaning in life and death anxiety. Furthermore, associations between the acceptance variables and meaning in life qualities turned out to be relatively weak, although statistically significant in the case of acceptance of one’s own dying.
One explanation for these small to non-existent correlations might be our differentiated approach to measure the psychological constructs in question: Beside the multidimensional assessment of attitudes toward dying and death, meaning in life was also measured in a more differentiated way than in former research. Throughout the studies concerning the correlation of meaning in life and death anxiety cited earlier, meaning was assessed with the Purpose in Life Test (Crumbaugh & Maholick, Citation1964), which is, according to Schnell (Citation2009) and Steger et al. (Citation2006), confounded with variables like depression and satisfaction with life, and also not designed to distinguish adequately between the two qualities of meaningfulness and crisis of meaning. Therefore, the present results cannot be directly compared to the respective previous studies.
Perhaps our finding is also attributable to an age effect hypothesized by Hui and Fung (Citation2009), who investigated relationships of religiosity, death anxiety, and meaning in life in a sample of college students and found that the negative correlation of death anxiety and MIL vanished when intrinsic religiosity was taken into account. Discussing their results, the authors argue that young people are typically less concerned with their own death, which is still far away, and view their life time more as “time since birth” than “time left to live” (see also Gesser et al., Citation1988), compared to older individuals. Hence, death is probably not a central motive in their life yet and may therefore be not (so strongly) related to their conceptualization of meaning in life. This explanation might also apply to the present, relatively young study sample. Nevertheless, because TMT and related empirical research suggest that death is a universal motivational force—also for young adults with which most of the existing studies were conducted—this finding still appears surprising. It could be that the aforementioned lifetime perspective of the young serves as a form of proximal defense (Pyszczynski et al., Citation1999) against the threat of mortality, which enables them to push the problem of death out of conscious awareness and into a distant future during everyday life. Older adults may not have this resource due to their undeniably increased proximity to death and a higher frequency of already made experiences with bereavement due to their age (Pyszczynski et al., Citation2015). However, this issue needs a more thorough and direct examination. Future research intended to clarify the nexus of meaning, death, and dying should consider the question whether relationships between meaning in life and attitudes toward death and dying vary across the life span.
The finding that attitudes toward dying/death and MIL were largely unrelated in the present sample was also supported by longitudinal results: Mortality awareness led to changes in attitudes toward dying, but these effects were apparently not accompanied by changes in evaluations of meaning in life. Although a floor effect might also account for the non-effect of MA on crisis of meaning, there is no indication for a ceiling effect regarding meaningfulness (see ). Here, the mean score was relatively close to the scale’s theoretical mean, and comparable to the reported mean in a representative sample (see Schnell & Becker, Citation2007). This speaks against the possibility of biases through specific sample characteristics (i.e., an unexpectedly high level of meaningfulness).
Research on TMT has yielded significant effects of mortality salience on measures of MIL, though these changes were not tracked longitudinally so far. In the present study, the latency between the last MA-intervention and the assessment of dependent variables (one week, four weeks and six months later) ensured that only longer-term effects would be measured. It hence contrasted the typical short-term analysis in TMT-experiments. Because no longer-term changes could be observed, it is conceivable that MS-effects on MIL are simply very short-termed consequences of a (subtle and brief) mortality confrontation, which fade away soon afterwards—or get “managed” in the sense of TMT—and entail no persistent, existential shifts. These fluctuations in experiencing one’s life as meaningful could probably be interpreted in terms of the context dependency of meaningfulness (see King et al., Citation2006; Schnell, Citation2020), which is contrasted by its relative stability over longer periods (Schnell, Citation2009, Citation2014; Schnell & Becker, Citation2007). In any case, the specific interventions applied in the present study have not evoked such far-reaching, existential reflections which would be capable of shaking up an individual’s evaluation of their life’s meaning. Another reason for this non-effect of MA could be seen in the fact that the present sample mainly participated out of an extrinsic motivation. It is likely that they did not feel an intrinsic need to evaluate or even change their core values and beliefs. In contrast, in cases where existential reflections are undertaken on one’s own initiative or based on a need for clarification in life, such as in contemporary pilgrimage rituals, radical and enduring changes in meaning in life have been observed (see Schnell & Pali, Citation2013).
There was one instructive exception to the observation that MA did not yield any effects on individuals’ sense of meaning in life: Secular participants—in comparison to religious ones—exhibited a slight decrease in meaningfulness as effect of our treatment (and thus paralleling the experimental results of Vail & Soenke, Citation2018). From a TMT-perspective, one might conclude that a secular, worldly oriented view on life is presumably less protecting against existential threats than a religious view, which typically promises some kind of continued existence after death (i.e., literal immortality), and therefore serves as a source of meaning that transcends mortality (see Vail & Soenke, Citation2018). It should be noted though, that this decrease of meaningfulness was not accompanied by an increase in crisis of meaning. Because we assessed religiousness by asking respondents to identify their worldview (options: Buddhism, Christianity, Hinduism, Islam, Judaism, atheism, agnosticism, other), we only have a superficial insight regarding our participants’ religiousness and thus refrain from drawing too far-reaching conclusions from this finding. Further research, employing a more differentiated operationalization of (a)religiousness, is needed to qualify our results.
Last but not least, and against our expectation, dispositional self-esteem did not moderate participants’ reactions to the mortality awareness treatment, an observation frequently made in TMT-experiments (e.g., Juhl & Routledge, Citation2014; Routledge et al., Citation2010; Taubman-Ben-Ari, Citation2011). The buffer function of self-esteem against existential threats, as proposed by TMT, is possibly effective only in the short term (e.g., by moderating defensive processes resulting from mortality salience), but seems to be less central for a longer-term and more conscious reflection on one’s own mortality. Through contemplating one’s own mortality intensely, central values, motives, and goals in life can be called into question. Established sources of self-worth and previous accomplishments might thus be less important in such situations and their protective function might be neutralized.
The present study has several limitations. First, the sample under investigation consisted of Western European students, mainly between 20 and 30 years of age. Thus, the results presented in this article cannot be generalized to older (or also younger) populations (as also discussed above), to different social subgroups in the same age cohort, or to other cultural and societal backgrounds.
A second limitation concerns the sensitivity of the applied outcome measures for growth processes induced by heightened mortality awareness. Because the investigated constructs of meaningfulness and crisis of meaning represent the most abstract level of personal meaning construction processes (“hierarchic model of meaning,” see Schnell, Citation2009, Citation2014), it is conceivable that changes on lower levels (e.g., sources of meaning or individual life goals, which might have occurred without affecting evaluations of meaning in life) remained undetected due to the applied methodology. Similarly, the items of the FIMEST-R are very specific and certainly insensitive to changes in attitudes outside the primary scope of the questionnaire. Indeed, (unsystematic) qualitative feedback from participants collected subsequently to the primary investigation suggested that—at least some—participants experienced changes like living more consciously and mindfully, taking their own mortality more into account when making important decisions, being able to talk more openly about topics related to dying and death, or taking notice of own repression mechanisms regarding such issues. Further research targeting potential growth processes on lower levels of meaning construction and facets of one’s stance toward mortality other than fear and acceptance would therefore be fruitful.
A third limitation of our study lies in the fact that the control and mortality awareness groups might not have been directly comparable. Whereas participants in the MA-condition spent a lot of time reflecting on their own mortality, individuals in the control setting were relatively unrelated to the study and did not solve any “neutral” tasks in the meantime. Their involvement in the study may have affected MA-participants’ motivation to complete the questionnaires in a biased way. In addition, the design was not double-blinded (i.e., the experimenter was aware of the rationale behind the study), which opens the possibility of various experimenter biases.
Fourth, the effectiveness of the MA-tasks was not controlled in our study (e.g., by assessing “death-thought accessibility”; see Greenberg et al., Citation1994). However, participants reported various experiences related to reflections on their own death and expressed their interest for the issue in an unsystematic qualitative survey after T2 (see above) as well as during the group discussions. We are therefore confident that mortality awareness was effectively increased by our interventions.
Finally, statistical power might have been too low to detect small effects of our treatment. To target this issue, we conducted power analyses using the RMASS-3-software (Center for Health Statistics, Citation2015; Hedeker et al., Citation1999). The program estimates the necessary entire sample size in two-group repeated-measurement designs for detecting a linear time × group-interaction, allowing for attrition (settings used: two-sided test, α = .05, (1−β) = .80, attrition rate of 10% for each time interval). Based on the parameters of our HLM-models and an expected effect size of d = 0.30, chosen with respect to findings from previous meta-analyses on death education programs (Durlak & Riesenberg, Citation1991; Maglio & Robinson, Citation1994), the calculations yielded an averaged necessary sample size of 139 for the death attitudes (two timepoints). For d = 0.50, the analysis resulted in N = 50. Necessary sample sizes of 231 (if d = 0.30) and 83 (if d = .50), respectively, were obtained for the meaning variables (four timepoints). These calculations, albeit rather rough estimates, suggest that our design was underpowered for detecting true effects of d = 0.30. However, for an effect of d = 0.50 our achieved sample size was high enough to conduct tests with a power of at least .80. Given these results, we conclude that there were—with sufficient probability—no moderate or large effects of our treatment on our outcome variables. This conclusion is also deducible from the confidence intervals of our treatment effects (see ), which indicate that, irrespective of whether an effect was significant or not, effect sizes in excess of approximately |d| = 0.30 are not very likely, given our observed data (see Hoenig & Heisey, Citation2001). However, we cannot rule out the possibility that there might have been smaller effects in addition to those we have found which we couldn’t detect given our limited sample size. Unfortunately, because of the elaborate study design and a lack of further time resources, our (initial) sample size of N = 98 could not be exceeded. Further studies are thus needed to replicate the present findings. The calculations from above can be used as a starting point for determining necessary sample sizes for future research in this regard.
Conclusions
The present study suggests that positive changes in attitudes toward one’s own mortality can be stimulated by adequately designed interventions on mortality awareness. However, these effects—if present—seem to be small, and a clear differentiation within such attitudes turned out to be crucial. Moreover, the absence of correlations between dimensions of meaning in life and dying-/death-attitudes questions the validity of previous research, in which less-specific measures of meaning- and death-related constructs were applied. Finally, the present work suggests that—at least for religious individuals—existential foundations seem to be stable and generally highly resilient against an intense (but fictional) confrontation with one’s own mortality.
Acknowledgments
We would like to thank our anonymous reviewers for their insightful and helpful comments, from which this article benefitted considerably. Our reliable participants also deserve a big thank you. Without their commitment, this study would not have been possible.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Ardelt, M. (2008). Wisdom, religiosity, purpose in life, and death attitudes of aging adults. In A. Tomer, G. T. Eliason, & P. T. P. Wong (Eds.), Existential and spiritual issues in death attitudes (pp. 139–158). Lawrence Erlbaum Associates.
- Center for Health Statistics. (2015). RMASS-3 [Online software application]. http://www.rmass.org
- Cozzolino, P. J. (2006). Death contemplation, growth, and defense: Converging evidence of dual-existential systems? Psychological Inquiry, 17(4), 278–287. https://doi.org/https://doi.org/10.1080/10478400701366944
- Cozzolino, P. J., & Blackie, L. E. R. (2013). I die, therefore I am: The pursuit of meaning in the light of death. In J. A. Hicks & C. Routledge (Eds.), The experience of meaning in life: Classical perspectives, emerging themes, and controversies (pp. 31–45). Springer.
- Crocker, J., & Nuer, N. (2004). Do people need self-esteem? Comment on Pyszczynski et al. (2004). Psychological Bulletin, 130(3), 469–472. https://doi.org/https://doi.org/10.1037/0033-2909.130.3.469
- Crumbaugh, J. C., & Maholick, L. T. (1964). An experimental study in existentialism: The psychometric approach to Frankl’s concept of noogenic neurosis. Journal of Clinical Psychology, 20(2), 200–207. https://doi.org/https://doi.org/10.1002/1097-4679(196404)20:2<200::AID-JCLP2270200203>3.0.CO;2-U
- Davis, C. G., & McKearney, J. M. (2003). How do people grow from their experience with trauma or loss? Journal of Social and Clinical Psychology, 22(5), 477–492. https://doi.org/https://doi.org/10.1521/jscp.22.5.477.22928
- Dumville, J. C., Torgerson, D. J., & Hewitt, C. E. (2006). Reporting attrition in randomised controlled trials. BMJ (Clinical Research ed.), 332(7547), 969–971. https://doi.org/https://doi.org/10.1136/bmj.332.7547.969
- Durlak, J. A. (1972). Relationship between individual attitudes toward life and death. Journal of Consulting and Clinical Psychology, 38(3), 463–463. https://doi.org/https://doi.org/10.1037/h0032854
- Durlak, J. A. (1994). Changing death attitudes through death education. In R. A. Neimeyer (Ed.), Death anxiety handbook: Research, instrumentation, and application (pp. 243–260). Taylor & Francis.
- Durlak, J. A., & Riesenberg, L. A. (1991). The impact of death education. Death Studies, 15(1), 39–58. https://doi.org/https://doi.org/10.1080/07481189108252408
- Feingold, A. (2015). Confidence interval estimation for standardized effect sizes in multilevel and latent growth modeling. Journal of Consulting and Clinical Psychology, 83(1), 157–168. https://doi.org/https://doi.org/10.1037/a0037721
- Field, A. P., Miles, J., & Field, Z. (2012). Discovering statistics using R. Sage.
- Gesser, G., Wong, P. T. P., & Reker, G. T. (1988). Death attitudes across the life-span: The development and validation of the Death Attitude Profile (DAP). OMEGA - Journal of Death and Dying, 18(2), 113–128. https://doi.org/https://doi.org/10.2190/0DQB-7Q1E-2BER-H6YC
- Greenberg, J., Pyszczynski, T., & Solomon, S. (1995). Toward a dual-motive depth psychology of self and social behavior. In M. H. Kernis (Ed.), Efficacy, agency, and self-esteem (pp. 73–99). Springer.
- Greenberg, J., Pyszczynski, T., Solomon, S., Simon, L., & Breus, M. (1994). Role of consciousness and accessibility of death-related thoughts in mortality salience effects. Journal of Personality and Social Psychology, 67(4), 627–637. https://doi.org/https://doi.org/10.1037/0022-3514.67.4.627
- Halifax, J., (n.d.). The nine contemplations of Atisha. https://www.upaya.org/dox/Contemplations.pdf
- Hedeker, D., Gibbons, R. D., & Waternaux, C. (1999). Sample size estimation for longitudinal designs with attrition: Comparing time-related contrasts between two groups. Journal of Educational and Behavioral Statistics, 24(1), 70–93. https://doi.org/https://doi.org/10.2307/1165262
- Heidegger, M. (1996). Being and Time. A translation of Sein und Zeit (J. Stambaugh, Trans.). State University of New York Press.
- Hoenig, J. M., & Heisey, D. M. (2001). The abuse of power: The pervasive fallacy of power calculations for data analysis. The American Statistician, 55(1), 19–24. https://doi.org/https://doi.org/10.1198/000313001300339897
- Hughes, J. (2018). reghelper: Helper functions for regression analysis (Version 0.3.4) [R package]. https://CRAN.R-project.org/package=reghelper
- Hui, V. K.-Y., & Fung, H. H. (2009). Mortality anxiety as a function of intrinsic religiosity and perceived purpose in life. Death Studies, 33(1), 30–50. https://doi.org/https://doi.org/10.1080/07481180802494099
- Juhl, J., & Routledge, C. (2014). The effects of trait self-esteem and death cognitions on worldview defense and search for meaning. Death Studies, 38(1–5), 62–68. https://doi.org/https://doi.org/10.1080/07481187.2012.718038
- Kierkegaard, S. (1993). At a graveside. In S. Kierkegaard, H. V. Hong & E. H. Hong (Trans.), Three discourses on imagined occasions (Kierkegaard’s Writings X) (pp. 69–102). Princeton University Press.
- King, L. A., Hicks, J. A., & Abdelkhalik, J. (2009). Death, life, scarcity, and value: An alternative perspective on the meaning of death. Psychological Science, 20(12), 1459–1462. https://doi.org/https://doi.org/10.1111/j.1467-9280.2009.02466.x
- King, L. A., Hicks, J. A., Krull, J. L., & Del Gaiso, A. K. (2006). Positive affect and the experience of meaning in life. Journal of Personality and Social Psychology, 90(1), 179–196. https://doi.org/https://doi.org/10.1037/0022-3514.90.1.179
- Klug, A. (1997). Fragebogen zum Sterben, zum Tod und zum “Danach” (SESTD). https://www.zpid.de/pub/tests/PT_9003495_SESTD_Fragebogen.pdf
- Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Löwe, B. (2010). The Patient Health Questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. General Hospital Psychiatry, 32(4), 345–359. https://doi.org/https://doi.org/10.1016/j.genhosppsych.2010.03.006
- Lakens, D. (2013). Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Frontiers in Psychology, 4, 863. https://doi.org/https://doi.org/10.3389/fpsyg.2013.00863
- Lenth, R. (2019). emmeans: Estimated marginal means, aka least-squares means (Version 1.4.2) [R package]. https://CRAN.R-project.org/package=emmeans
- Maglio, C. J., & Robinson, S. E. (1994). The effects of death education on death anxiety: A meta-analysis. OMEGA - Journal of Death and Dying, 29(4), 319–335. https://doi.org/https://doi.org/10.2190/KEA9-2G73-AMJM-MNP6
- Martin, L. L., Campbell, W. K., & Henry, C. D. (2004). The roar of awakening: Mortality acknowledgment as a call to authentic living. In J. Greenberg, S. L. Koole, & T. Pyszczynksi (Eds.), Handbook of experimental existential psychology (pp. 431–448). Guilford.
- McGregor, I., Zanna, M. P., Holmes, J. G., & Spencer, S. J. (2001). Compensatory conviction in the face of personal uncertainty: Going to extremes and being oneself. Journal of Personality and Social Psychology, 80(3), 472–488. https://doi.org/https://doi.org/10.1037/0022-3514.80.3.472
- Menzies, R. E., Zuccala, M., Sharpe, L., & Dar-Nimrod, I. (2018). The effects of psychosocial interventions on death anxiety: A meta-analysis and systematic review of randomised controlled trials. Journal of Anxiety Disorders, 59, 64–73. https://doi.org/https://doi.org/10.1016/j.janxdis.2018.09.004
- Park, C. L. (2010). Making sense of the meaning literature: An integrative review of meaning making and its effects on adjustment to stressful life events. Psychological Bulletin, 136(2), 257–301. https://doi.org/https://doi.org/10.1037/a0018301
- Pinheiro, J. C., Bates, D. M., DebRoy, S., Sarkar, D., R Core Team. (2019). nlme: Linear and nonlinear mixed effects models (Version 3.1-140) [R package]. https://CRAN.R-project.org/package=nlme
- Pyszczynski, T., Greenberg, J., & Solomon, S. (1999). A dual-process model of defense against conscious and unconscious death-related thoughts: An extension of terror management theory. Psychological Review, 106(4), 835–845. https://doi.org/https://doi.org/10.1037/0033-295X.106.4.835
- Pyszczynski, T., Greenberg, J., Solomon, S., & Maxfield, M. (2006). On the unique psychological import of the human awareness of mortality: Theme and variations. Psychological Inquiry, 17(4), 328–356. https://doi.org/https://doi.org/10.1080/10478400701369542
- Pyszczynski, T., Solomon, S., & Greenberg, J. (2015). Thirty years of terror management theory: From genesis to revelation. Advances in Experimental Social Psychology, 52, 1–70.
- R Core Team. (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing. http://www.R-project.org/
- Rappaport, H., Fossler, R. J., Bross, L. S., & Gilden, D. (1993). Future time, death anxiety, and life purpose among older adults. Death Studies, 17(4), 369–379. https://doi.org/https://doi.org/10.1080/07481189308252631
- Ring, K. (1984). Heading toward omega: In search of the meaning of the near-death experience. William Morrow.
- Rogers, R. (2011). Conceptualizing death in a worldview consistent, meaningful way and its effects on worldview defense. Death Studies, 35(2), 107–123. https://doi.org/https://doi.org/10.1080/07481187.2011.535379
- Rogers, R., Sanders, C. S., & Vess, M. (2019). The terror management of meaning and growth: How mortality salience affects growth-oriented processes and the meaningfulness of life. In C. Routledge & M. Vess (Eds.), Handbook of terror management theory (pp. 325–345). Academic Press.
- Rosenblatt, A., Greenberg, J., Solomon, S., Pyszczynski, T., & Lyon, D. (1989). Evidence for terror management theory: I. The effects of mortality salience on reactions to those who violate or uphold cultural values. Journal of Personality and Social Psychology, 57(4), 681–690. https://doi.org/https://doi.org/10.1037//0022-3514.57.4.681
- Routledge, C., & Juhl, J. (2010). When death thoughts lead to death fears: Mortality salience increases death anxiety for individuals who lack meaning in life. Cognition & Emotion, 24(5), 848–854. https://doi.org/https://doi.org/10.1080/02699930902847144
- Routledge, C., Ostafin, B., Juhl, J., Sedikides, C., Cathey, C., & Liao, J. (2010). Adjusting to death: The effects of mortality salience and self-esteem on psychological well-being, growth motivation, and maladaptive behavior. Journal of Personality and Social Psychology, 99(6), 897–916. https://doi.org/https://doi.org/10.1037/a0021431
- Ryan, R. M., & Deci, E. L. (2004). Avoiding death or engaging life as accounts of meaning and culture: Comment on Pyszczynski et al. (2004). Psychological Bulletin, 130(3), 473–477. https://doi.org/https://doi.org/10.1037/0033-2909.130.3.473
- Schnell, T. (2009). The sources of meaning and meaning in life questionnaire (SoMe): Relations to demographics and well-being. The Journal of Positive Psychology, 4(6), 483–499. https://doi.org/https://doi.org/10.1080/17439760903271074
- Schnell, T. (2010). Existential indifference: Another quality of meaning in life. Journal of Humanistic Psychology, 50(3), 351–373. https://doi.org/https://doi.org/10.1177/0022167809360259
- Schnell, T. (2014). Meaning in life operationalized: An empirical approach to existential psychology. In S. Kreitler & T. Urbánek (Eds.), Conceptions of meaning (pp. 173–194). Nova Science.
- Schnell, T. (2020). The psychology of meaning in life. Routledge.
- Schnell, T., & Becker, P. (2007). Fragebogen zu Lebensbedeutungen und Lebenssinn: LEBE. Hogrefe.
- Schnell, T., & Pali, S. (2013). Pilgrimage today: The meaning-making potential of ritual. Mental Health, Religion & Culture, 16(9), 887–902. https://doi.org/https://doi.org/10.1080/13674676.2013.766449
- Solomon, S., Greenberg, J., & Pyszczynksi, T. (2004). The cultural animal: Twenty years of terror management theory and research. In J. Greenberg, S. L. Koole, & T. Pyszczynksi (Eds.), Handbook of experimental existential psychology (pp. 13–34). Guilford.
- Spitzer, R. L., Kroenke, K., & Williams, J. B. (1999). Validation and utility of a self-report version of PRIME-MD: The PHQ Primary Care Study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA, 282(18), 1737–1744. https://doi.org/https://doi.org/10.1001/jama.282.18.1737
- Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing Generalized Anxiety Disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/https://doi.org/10.1001/archinte.166.10.1092
- Steger, M. F., Frazier, P., Oishi, S., & Kaler, M. (2006). The Meaning in Life Questionnaire: Assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53(1), 80–93. https://doi.org/https://doi.org/10.1037/0022-0167.53.1.80
- Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th International Edition). Pearson.
- Taubman-Ben-Ari, O. (2011). Is the meaning of life also the meaning of death? A terror management perspective reply. Journal of Happiness Studies, 12(3), 385–399. https://doi.org/https://doi.org/10.1007/s10902-010-9201-2
- Tedeschi, R. G., & Calhoun, L. G. (1995). Trauma & transformation: Growing in the aftermath of suffering. Sage.
- Tofighi, D., & MacKinnon, D. P. (2011). RMediation: An R package for mediation analysis confidence intervals. Behavior Research Methods, 43(3), 692–700. https://doi.org/https://doi.org/10.3758/s13428-011-0076-x
- Uanhoro, J. O. (2017). Effect size calculators [Online software application]. https://effect-size-calculator.herokuapp.com
- Vail, K. E., Juhl, J., Arndt, J., Vess, M., Routledge, C., & Rutjens, B. T. (2012). When death is good for life: Considering the positive trajectories of terror management. Personality and Social Psychology Review: An Official Journal of the Society for Personality and Social Psychology, Inc, 16(4), 303–329. https://doi.org/https://doi.org/10.1177/1088868312440046
- Vail, K. E., Rothschild, Z. K., Weise, D. R., Solomon, S., Pyszczynski, T., & Greenberg, J. (2010). A Terror management analysis of the psychological functions of religion. Personality and Social Psychology Review: An Official Journal of the Society for Personality and Social Psychology, Inc, 14(1), 84–94. https://doi.org/https://doi.org/10.1177/1088868309351165
- Vail, K. E., & Soenke, M. (2018). The impact of mortality awareness on meaning in life among Christians and Atheists. Religion, Brain & Behavior, 8(1), 44–56. https://doi.org/https://doi.org/10.1080/2153599X.2016.1238845
- Von Collani, G., & Herzberg, P. Y. (2003). Eine revidierte Fassung der deutschsprachigen Skala zum Selbstwertgefühl von Rosenberg. Zeitschrift für differentielle und diagnostische Psychologie, 24(1), 3–7. https://doi.org/https://doi.org/10.1024//0170-1789.24.1.3
- Wittkowski, J. (1978). Tod und Sterben: Ergebnisse der Thanatopsychologie. Quelle und Meyer.
- Wittkowski, J. (1996). Fragebogeninventar zur mehrdimensionalen Erfassung des Erlebens gegenüber Sterben und Tod (FIMEST). Hogrefe.
- Wong, P. T. P. (2008). Meaning management theory and death acceptance. In A. Tomer, G. T. Eliason, & P. T. P. Wong (Eds.), Existential and spiritual issues in death attitudes (pp. 65–87). Lawrence Erlbaum Associates.
- Wong, P. T. P., Reker, G. T., & Gesser, G. (1994). The Death Attitude Profile-Revised: A multidimensional measure of attitudes towards death. In R. A. Neimeyer (Ed.), Death anxiety handbook: Research, instrumentation, and application (pp. 121–148). Taylor and Francis.
- Wong, P. T. P., & Tomer, A. (2011). Beyond terror and denial: The positive psychology of death acceptance. Death Studies, 35(2), 99–106. https://doi.org/https://doi.org/10.1080/07481187.2011.535377