
Abstract
A cross-sectional survey to investigate relationships between coronavirus anxiety, individual death attitudes, and personal worldview was conducted among 202 German-speaking adults in Central Europe. Results indicated that death anxiety significantly predicts coronavirus anxiety beyond sociodemographic variables. Women reported higher coronavirus anxiety than men. Against expectations, dimensions of personal worldview were hardly related to coronavirus anxiety. In contrast, we found evidence for a curvilinear relationship between religiosity as well as atheism and negative death attitudes. Our study contributes to recent discussions about death anxiety as a transdiagnostic factor in psychopathology and yields important implications for psychosocial support in the current pandemic.
In the year 2020, public life all over the world is dominated by one exceptional event: the global outbreak of the virus SARS-CoV-2. Unparalleled in its dimension—at least to our generation—this pandemic led and leads to drastic governmental interventions, such as the shut-down of large parts of cultural and economic life, the closing of schools and universities, or the implementation of rigorous border controls. Furthermore, through daily reports of new COVID-19 diseases and deaths in the media, and through diverse forms of infection control (e.g., the obligation to wear face masks in many public areas), most people are probably much more confronted with their own mortality now than they used to be. Besides the obvious medical, economic, and social aspects, this ubiquitous salience of one’s own mortality points to an additional, an existential dimension of the current coronavirus crisis—a dimension that received little attention in research so far.
Terror Management Theory (TMT; Solomon et al., Citation2004) provides a potential theoretical framework to examine this existential dimension of the pandemic. TMT in general deals with the unique human knowledge regarding one’s own mortality—which is in conflict with a universal desire to live—and its diverse effects on our social and cultural life. According to TMT, people draw on a set of evolutionarily developed strategies to alleviate anxiety resulting from a heightened (unconscious) awareness of one’s own mortality. One of these strategies is the creation and the belief in cultural worldviews. By upholding the standards and values of one’s own worldview, individuals are able to attain symbolic immortality: Through contributing to a valued community which outlasts oneself, someone is able to leave enduring traces in the world, and the ultimate destruction of the self after one’s demise can thereby be annulled. In contrast to secular worldviews, religious worldviews typically incorporate a belief in some form of life or existence after death. They offer not only symbolic, but also literal immortality, and thus are particularly appealing to many people as a way to cope with anxiety related to one’s own death. However, not only religious but also non-religious worldviews can serve as a protective buffer against deep-rooted existential fears (see Vail et al., Citation2010). Accordingly, a recent meta-analysis by Jong et al. (Citation2018) suggests that religiosity might not relate linearly to death anxiety, but rather curvilinearly in an inverted U-shaped manner; that is, highly religious as well as highly non-religious individuals are less fearful regarding their death than those who are only moderately religious. In this view, personal conviction and certainty concerning one’s own worldview are perhaps more decisive for its association with death anxiety than the particular content of the (religious or non-religious) belief system (see also Ellis & Wahab, Citation2013; Wink & Scott, Citation2005). Applied to the prevalent crisis, this means that a stable and convinced worldview, whether religious or not, might provide a protective buffer against the existential threat posed by the pandemic.
Death anxiety—as a dispositional trait—has recently been discussed as a transdiagnostic factor, involved in the development and maintenance of a wide range of mental disorders such as anxiety disorders, depression, and somatic symptom disorders (Iverach et al., Citation2014; Maxfield et al., Citation2014; Yalom, Citation2008). As Menzies and Menzies (Citation2020) articulate, this is highly relevant in the prevailing COVID-19 pandemic. Due to the current, ubiquitous salience of human mortality, individuals high in death anxiety are probably experiencing severe existential distress and are at a relatively higher risk of developing mental disorders. However, whereas anxiety—as well as avoidance—regarding one’s own death is seen as detrimental to human functioning, a more positive stance toward one’s own mortality (e.g., acceptance of death as a natural and integral part of life) is typically associated with higher mental well-being (Wong et al., Citation1994; Yalom, Citation2008). An individual’s attitudes toward death might therefore also explain potential impairments of mental health related to the COVID-19 pandemic.
Besides the indirect relationship between religiosity and mental disorders via death anxiety, one might also raise the question about the more general role of religiosity for mental health in times of COVID-19. Because pertinent evidence in this regard is largely absent so far (Dein et al., Citation2020), one might only speculate about the direction of the relationship—if any exists. Although religious communities provide several resources which may protect against mental distress (e.g., social support, positive affect, and a source of meaning in life; see Park & Slattery, Citation2013; Schnell, Citation2011), a crisis like the current pandemic can also lead to serious religious struggles, which relate to an impairment of mental health, as Dein et al. (Citation2020) discuss. Apart from the momentary situation, a meta-analysis on the relationship between measures of religiosity and mental health in German-speaking countries came to the conclusion that, on average, religiosity is significantly, but only slightly positively related to mental health (Hodapp & Zwingmann, Citation2019). The authors remarked that based on the available data no curvilinear relationship between the variables could be tested. However, because some previous studies, predominantly with US-American samples, found evidence for a curvilinear relationship between religiosity and psychological well-being (e.g., Eliassen et al., Citation2005; Galen & Kloet, Citation2011; Ross, Citation1990; Schnittker, Citation2001), mental distress due to COVID-19 might also be related curvilinearly to religiosity. As far as spirituality is concerned, there is increasing evidence that this, when understood as an idiosyncratic approach to transcendence, is more likely to be associated with negative mental health (King et al., Citation2013; Schnell, Citation2012; Schnell et al., Citation2020; Vittengl, Citation2018).
As several authors have discussed, unidimensional measures of religiosity or spirituality are not able to capture the full picture of a person’s individual worldview (e.g., Brewster et al., Citation2014; Hall et al., Citation2008; Schnell, Citation2015). In order to attain instructive insights into the role of an individual’s worldview for their mental health during the COVID-19 pandemic, personal worldview has thus to be treated multi-dimensionally, incorporating religious, secular, as well as non-religious-but-spiritual viewpoints. Because TMT suggests that the promise of literal immortality is one of the most powerful ways to diminish existential fears resulting from confrontations with one’s own mortality, worldview dimensions which deal with the question of vertical transcendence (i.e., belief in a god or supernatural power) are particularly interesting in this regard.
The present study
The present study aims to investigate how dysfunctional anxiety related to the new coronavirus (as a measure of mental health) is associated with an individual’s attitudes toward death and their personal worldview. Personal worldview is operationalized multi-dimensionally by assessing the degrees of religiosity (religious life and personal relationship with God), spirituality (a subjective approach to a higher reality), as well as atheism and agnosticism (as secular attitudes toward deity). Both convinced religiosity and atheism are considered stable worldviews: Religiosity is connected with a centuries-old tradition that is recognized and accepted in many parts of the world and thus offers high plausibility structures (Berger, Citation1967). Atheism is a decided denial of theism, shown to be associated with a negative attitude toward religion and a positive attitude toward science and technology (Schnell, Citation2015). Agnosticism is solely defined by the assumption that nothing can be known about the existence of a god or higher power. It does not imply any specific positive beliefs (Schnell, Citation2015). Spirituality has been shown to be a searching and open orientation (Saroglou & Muñoz-García, Citation2008; Schnell, Citation2012; Schnell et al., Citation2020) and thus represents a counterproposal to a firm and stable position. Death attitudes investigated in the present study are death anxiety, death avoidance, neutral acceptance (death as a natural and integral part of life), approach acceptance (the religious belief in a happy afterlife), and escape acceptance (death as a relief from pain and suffering; Wong et al., Citation1994).
Based on the theoretical and empirical background presented above, we anticipated that individuals with a stable personal worldview (either religious or atheistic) would be less prone to experiencing severe distress due to the COVID-19 pandemic than individuals with a more uncertain worldview. We, therefore, hypothesized curvilinear (inverted U-shaped) relationships between coronavirus anxiety and religiosity as well as atheism. Furthermore, we anticipated that individuals who showed high values in death anxiety would also tend to show high values in coronavirus anxiety. On the other hand, people who were able to accept their own death as a natural and integral part of life (neutral acceptance), should report less coronavirus anxiety. We further expected that religiosity and atheism would show curvilinear relationships with death anxiety and death avoidance. For agnosticism and spirituality, we expected either no association or positive relationships with coronavirus anxiety, death anxiety, and death avoidance. Finally, we tested exploratively whether worldview dimensions and death attitudes would statistically predict coronavirus anxiety beyond sociodemographics.
Method
The study was reviewed by the University of Innsbruck’s Board for Ethical Questions in Science and was granted ethical clearance.
Participants and procedure
Data from 202 adults were collected from May 20 to June 7, 2020, using the online survey tool Sosci Survey (Leiner, Citation2019). Participants were recruited via Facebook, Instagram, and the internal e-mail system of the University of Innsbruck. They were eligible for the study if they were at least 18 years of age, provided consent, completed the questionnaire, and checked a statement that all questions were answered honestly. The sample comprised 50 men, 150 women, and 2 “other”; mean age was 25.77 years (Mdn = 24, SD = 6.55); and about 72% were university students. Most of our participants were Austrian (47.5%), German (39.1%), or Italian (9.9%). In total, 103 reported to be currently in a romantic relationship (51.0%), the rest was not. The educational level was relatively high, with 45.5% (n = 92) of the partakers holding a bachelor’s degree or higher. Two-thirds of the participants (67.8%) reported to be a member of a religious community, most of them Roman-Catholics (80.3%) or Protestants (16.8%). Most of our participants had not been tested for COVID-19 previously (89.6%), none of them had been tested positively. Forty-four persons (21.8%) reported that a close person (friend or family member) had been infected with the coronavirus, two participants (1.0%) indicated that a close person had died from COVID-19.
Measures
Participants were asked to report their age, gender, nationality, education, and relationship status. They were also asked about membership in a religious community and, if yes, how strongly they felt to belong to their denominational group on a scale from (0) not at all to (5) very strongly. Three questions examined whether the participant had been previously tested for COVID-19, whether a close person had got infected with the coronavirus, and whether a close person had died due to an infection with COVID-19.
Coronavirus anxiety
The Coronavirus Anxiety Scale (CAS; Lee, Citation2020a) is a recently developed, brief mental-health screening instrument for dysfunctional anxiety associated with the COVID-19 crisis. It comprises five items related to different anxiety symptoms aroused by coronavirus related information and thoughts. On a 5-point Likert scale, ranging from (0) not at all to (4) nearly every day, participants rate how frequently they experienced each anxiety symptom in the last two weeks (sample item: “I felt dizzy, lightheaded, or faint, when I read or listened to news about the coronavirus”). First applications of the CAS indicated a stable factorial structure, sufficient internal consistency, as well as convergent and construct validity (Ahmed et al., Citation2020; Evren et al., Citation2020; Lee, Citation2020a, Citation2020b; Lee, Jobe, & Mathis, Citation2020; Lee, Mathis, et al., Citation2020). Because there was no validated German version of the CAS available at the time of study conceptualization, the scale was translated into German by the first author (see Appendix). Factorial validity of the German CAS was tested by conducting a confirmatory factor analysis. As in the English version, a sum score of the five translated CAS items was computed for statistical analyses.
Personal worldview
An individual’s worldview was assessed on four dimensions: religiosity, spirituality, atheism, and agnosticism. To operationalize religiosity and spirituality, the respective subscales of the German version of the SoMe questionnaire (Schnell & Becker, Citation2007; for the English version, see Schnell, Citation2014) were applied. In the present study, internal consistencies were α = .91 for religiosity (“Religion plays an important role in my life,” 3 items) and α = .72 for spirituality (“There are certain things in life I consider sacred,” 5 items). By employing the corresponding scales of the Dimensions of Secularity (DoS) inventory by Schnell (Citation2015), individual degrees of atheism and agnosticism were assessed. Cronbach’s alpha was .90 for atheism (“There is no such thing as a god/a higher power,” 5 items) and .89 for agnosticism (“There might be a higher power/a god, but we will never know for sure,” 5 items). The DoS as well as the SoMe use a 6-point Likert scale, from (0) do not agree at all to (5) agree completely, and items were averaged for each dimension.
Death attitudes
To assess different attitudes toward death, the Death Attitude Profile-Revised (Wong et al., Citation1994) was employed in its German translation (DAP-GR, Jansen et al., Citation2019). It consists of five subscales, assessing death anxiety (“The prospect of my own death arouses anxiety in me,” 7 items, α = .92), death avoidance (“I avoid death thoughts at all costs,” 5 items, α = .93), neutral acceptance (“Death should be viewed as a natural, undeniable, and unavoidable event,” 5 items, α = .64), approach acceptance (“I believe that I will be in heaven after I die,” 10 items, α = .93), and escape acceptance (“Death will bring an end to all my troubles,” 5 items, α = .84). The DAP-GR uses a 7-point Likert scale, ranging from (1) strongly disagree to (7) strongly agree, and items were averaged for each dimension.
Statistical analysis
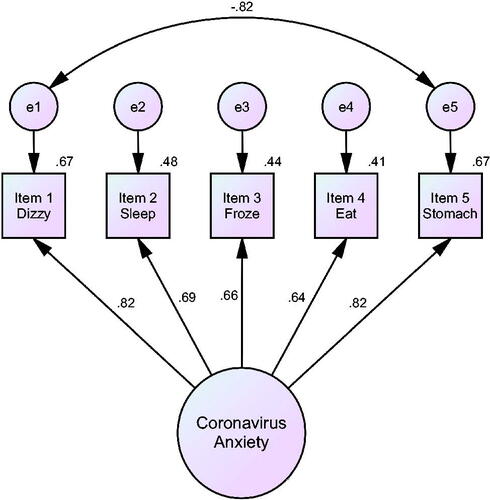
All statistical analyses were run with IBM SPSS Statistics Version 26 and IBM SPSS AMOS Version 24, respectively. All statistical significance tests were run two-sided. To evaluate the factorial validity of the CAS (German version)—that is, that all five items cohere to a single underlying factor of coronavirus anxiety—a confirmatory factor analysis (CFA) was carried out. In the first step, assumptions for factor analysis were tested. The five items met criteria for linearity, absence of multicollinearity and singularity, and factorability (Bartlett’s Test of Sphericity: χ2 = 371.71, df = 10, p < .001; KMO measure of sampling adequacy = .764; see Tabachnick & Fidell, Citation2013). However, there was a substantial deviation from univariate and multivariate normality; specifically, three items (2, 4, 5) showed univariate kurtosis values > 7.00 and normalized multivariate kurtosis was > 5.00 (see Byrne, Citation2016). Due to this non-normality of data, model fit was evaluated using a Bollen–Stine bootstrap procedure (Bollen & Stine, Citation1992) together with bootstrap-adjusted fit indices (Walker & Smith, Citation2017). In the following, the Bollen–Stine χ2 value equivalent statistic is denoted as χBS2, the Bollen–Stine bootstrapped p value as pBS, and fit indices are adjusted for non-normality. The statistical significance of model estimates was tested with bias-corrected 95% confidence intervals (number of bootstrap samples = 2000). An initial test of the original CAS measurement model (see Lee, Citation2020a) indicated an ambivalent model fit (χBS2 = 15.341, df = 5, pBS = .009, CFIAdjusted = .972, TLIAdjusted = .944, IFIAdjusted = .972, RMSEAAdjusted = .101) for our data, with the χBS2/df ratio, the Bollen–Stine p value as well as the RMSEA index indicating a poor model fit, while the CFI, TLI, and IFI indices were good to excellent. The examination of modification indices suggested that model fit could be increased by allowing a covariation between the error terms of item 1 and item 5 (MI = 16.33) and between item 4 and item 5 (MI = 15.07). Therefore, the model was respecified first by allowing the error terms of item 1 and item 5 to covary. This modification resulted in an excellent model fit: χBS2 = 4.356, df = 4, pBS = .360, CFIAdjusted = .999, TLIAdjusted = .998, IFIAdjusted = .999, RMSEAAdjusted = .021. Because the modified model fitted well, no further respecifications were made (Note. By allowing the error terms of item 4 and item 5 to covary first, the model fit remained ambivalent and the modification index for the covariation between error terms of item 1 and item 5 was still high. Therefore, the more parsimonious solution was chosen). The final model is depicted in . Internal consistency of the CAS was good with Cronbach’s α = .83. Due to small subsample-sizes, factorial invariance across demographics was not tested.
Figure 1. Single-factor CFA model. All of the standardized coefficients are significant at the .05 level.
Prior to further analyses, skewness and kurtosis values of all outcome variables were inspected to identify possible deviations from normality. By using a cutoff of ±2 for skewness as well as kurtosis (George & Mallery, Citation2016), age (positively skewed, positively kurtotic) and coronavirus anxiety (positively skewed, positively kurtotic) showed substantial deviations. Therefore, age was dichotomized with “0” = 18 to 29 years, and “1” = 30 years and older, and CAS scores were log-transformed (y = lg[x + 1]), resulting in acceptable distributional characteristics. Multivariate outliers were identified by applying a significant (p < .001) Mahalanobis distance as a criterion (Tabachnick & Fidell, Citation2013). One case fulfilled this criterion and was deleted. Thus, the effective sample size for all analyses below is N = 201.
Results
Correlates and predictors of coronavirus anxiety
The examination of bivariate correlations (see ) revealed that women reported higher values in coronavirus anxiety (r = .24, p = .001) than men. CAS scores were not related to age, education, or relationship status (p’s > .05). A one-way ANOVA indicated that there was no significant difference in coronavirus anxiety between German, Austrian, and Italian participants, F(2, 191) = 0.30, p = .745, ηP2 = .003. Membership in a religious community was positively related to coronavirus anxiety (r = .17, p = .019). However, the sense of belonging to this group (n = 137) did not correlate with coronavirus anxiety (r = −.05, p = .553). Furthermore, a close person’s infection with the virus (n = 44) was not related to CAS scores (r = .05, p = .481). (None of the participants themselves had been tested positively.)
Table 1. Correlation matrix and descriptive statistics for the outcome variables (N = 201).
From the four worldview dimensions, only agnosticism correlated significantly with coronavirus anxiety (r = .16, p = .024). To uncover potential quadratic relationships between worldview and coronavirus anxiety, regression models were computed. In these models, coronavirus anxiety served as the criterion and a linear, as well as a quadratic term of the respective worldview dimension (mean centered), were entered consecutively as predictors. None of the quadratic models was significant (see for detailed statistics).
Table 2. Regression statistics for quadratic relationships between worldview dimensions and coronavirus anxiety, death anxiety, and death avoidance.
Coronavirus anxiety was related positively to death anxiety (r = .31, p < .001) and death avoidance (r = .14, p = .046), and negatively to neutral acceptance (r = −.21, p = .003). CAS scores did not correlate significantly with approach or escape acceptance.
To investigate whether worldview dimensions and death attitudes accounted for variability in CAS scores beyond sociodemographics, a hierarchical multiple regression model was computed. Predictors were chosen based on significant zero-order correlations with the dependent variable coronavirus anxiety. At first, assumptions for multiple regression were checked. Following the recommendations of CitationTabachnick and Fidell (2013), no issues regarding multivariate outliers, multicollinearity and singularity, independence of errors, linearity, normality, and homoscedasticity were detected. The regression analysis then was carried out in three steps: In the first step, gender and worldview group were entered as predictors. The second step added agnosticism (the only worldview dimension significantly related to coronavirus anxiety). In the last step, death anxiety, death avoidance, and neutral acceptance were entered in the regression model (results are presented in ).
Table 3. Hierarchical multiple regression model for coronavirus anxiety (CAS).
In step 1, gender (β = 0.24, p = .001) and membership in a religious community (β = 0.18, p = .008) predicted coronavirus anxiety significantly (F(2, 197) = 9.68, p < .001, R2 = .09). In the second step, gender (β = 0.23, p = .001) and membership in a religious community (β = 0.15, p = .036) were significant predictor variables, but not agnosticism (β = 0.11, p = .124). Although the entire model was significant (F(3, 196) = 7.29, p < .001, R2 = .10), the change in F was not: ΔR2 = .01, ΔF(1, 196) = 2.38, p = .124. In the last step of the regression analysis, death anxiety, death avoidance, and neutral acceptance were added as predictors. In this model (F(6, 193) = 6.53, p < .001, R2 = .17), which differed significantly from the model of step 2 (ΔR2 = .07, ΔF(3, 193) = 5.28, p = .002), gender (β = 0.18, p = .007) and death anxiety (β = 0.29, p = .001) were significant predictors of coronavirus anxiety.
Relationships between death attitudes and personal worldview
Death anxiety as well as death avoidance were not significantly related to any worldview dimension, except for agnosticism (death anxiety: r = .23, p = .001; death avoidance: r = .14, p = .044). Neutral acceptance was negatively related to religiosity (r = −.20, p = .005) as well as spirituality (r = −.27, p < .001), and positively related to atheism (r = .27, p < .001). Approach acceptance related positively to religiosity (r = .68, p < .001), spirituality (r = .62, p < .001), and agnosticism (r = .17, p = .016), and negatively to atheism (r = −.74, p < .001). Escape acceptance only correlated with agnosticism: r = −.15, p = .031.
Similar to the analyses for coronavirus anxiety, regression models were computed to test for quadratic relationships between worldview dimensions and death anxiety as well as death avoidance (statistics are presented in ). For death anxiety, the quadratic models for religiosity as well as for atheism were significant. Although the quadratic regression model was also significant for agnosticism, only the linear term significantly predicted death anxiety, but not the quadratic term. The quadratic model for spirituality was not significant. For death avoidance, the quadratic models were significant for religiosity and atheism, but not for spirituality and agnosticism.
Discussion
The present study was carried out to investigate associations between personal worldview, individual death attitudes, and dysfunctional anxiety related to the coronavirus crisis. Contrary to our expectations, coronavirus anxiety was not related, linearly or curvilinearly, to any of the worldview dimensions when sociodemographic variables were accounted for. This finding seems to contradict a number of previous studies on relationships between mental well-being and religiosity (Eliassen et al., Citation2005; Galen & Kloet, Citation2011; Hodapp & Zwingmann, Citation2019; Ross, Citation1990; Schnittker, Citation2001) as well as spirituality (King et al., Citation2013; Schnell, Citation2012; Schnell et al., Citation2020; Vittengl, Citation2018). However, our results might be related to the exceptional and unprecedented situation that the coronavirus pandemic poses and in which contextual variables might be more predictive for mental well-being than one’s personal worldview.
In contrast to personal worldview, the extent of coronavirus anxiety turned out to be related to an individual’s attitudes toward death. Specifically, death anxiety and death avoidance were positively associated with coronavirus anxiety, whereas neutral acceptance related negatively to it. As the hierarchical regression analysis revealed, death avoidance and neutral acceptance could not predict the CAS score beyond the other variables already entered. However, death anxiety was a significant predictor of coronavirus anxiety and exhibited the highest beta value in the model. This finding fits well in the growing body of research on death anxiety as a transdiagnostic factor involved in the development and maintenance of a wide array of mental disorders (Iverach et al., Citation2014; Menzies & Menzies, Citation2020). We acknowledge that other authors (Lee, Jobe, Mathis, et al., Citation2020) view death anxiety more as a consequence of coronavirus anxiety rather than a predisposition to it. However, given the operationalization of death anxiety as a relatively stable personality trait (see Wong et al., Citation1994) as well as its theoretical foundation in existential psychology (Maxfield et al., Citation2014; Yalom, Citation2008), we found it more convincing to treat death anxiety as the predictor and coronavirus anxiety as the criterion. In the light of this interpretative context, death anxiety can be regarded as a potential therapeutic target in the psychological support of individuals suffering from mental distress related to the COVID-19 pandemic. Several therapeutic avenues for mitigating death anxiety were previously discussed (see Iverach et al., Citation2014; Menzies & Menzies, Citation2020; Yalom, Citation2008). One of them, the cultivation of an attitude which sees death as a natural and integral part of life, is supported by our study, given the negative relationship between neutral acceptance and death anxiety as well as coronavirus anxiety.
Our analyses revealed further that women reported higher degrees of coronavirus anxiety than men. This result is in line with previous findings on the CAS in Turkey and Bangladesh (Evren et al., Citation2020; Ahmed et al., Citation2020). In US samples (Lee, Citation2020a; Lee, Jobe, Mathis, et al., Citation2020; Lee, Mathis, et al., Citation2020), however, analyses of gender differences with respect to coronavirus anxiety yielded conflicting results, thus questioning the presence of a universal gender effect for this newly defined construct. Further research is needed to clarify this issue. We also found that membership in a religious community was positively correlated with coronavirus anxiety, albeit this relationship missed statistical significance in the last step of the hierarchical regression analysis. Because coronavirus anxiety was not related to any worldview dimension or to members’ sense of belonging to their community, this correlation does probably not originate from dogmatic factors. Perhaps, the closing of churches and a suspension of worship services increased the salience of the crisis for those who are at least formally connected to an institutionalized religion, and therefore intensified potential negative impacts on their mental well-being.
Besides the results concerning coronavirus anxiety, our study also investigated relationships between personal worldview and death attitudes. As expected, we found that individuals with an unsecure and uncertain worldview, i.e., persons who were only moderately religious or atheistic suffered from death anxiety. They also reported more avoidance behavior regarding the issue of death, which is itself strongly positively associated with death anxiety. These findings complement previous empirical evidence of a curvilinear relationship between religiosity and death anxiety (Ellis & Wahab, Citation2013; Jong et al., Citation2018; Wink & Scott, Citation2005). However, to our best knowledge, our study is the first which expands this finding to death avoidance as well as to atheism, measured independently of religiosity. Moreover, we found that agnosticism, which is based on skepticism and therefore may imply existential uncertainty, also exhibited a positive relationship to death anxiety and death avoidance. Spirituality was not at all related to both, perhaps due to the great variety of beliefs covered by this umbrella concept (Schnell, Citation2019). In sum, our results underline the importance to take clients’ personal worldviews into account when working on their stance toward death in psychological treatment and psychotherapy.
Limitations and future directions
Our study is subject to several limitations. First, our participants were relatively young, highly educated, and mainly sampled from German-speaking countries in Central Europe. Those who indicated to be members of a religious community were all Christian, except one Buddhist. Therefore, our results cannot be readily generalized to other age groups or to different societal, cultural, and religious backgrounds. We would like to encourage other researchers to investigate the relationships between personal worldview and mental well-being in times of COVID-19 especially with samples drawn from non-Western, non-Christian and/or more religious societies in order to qualify our (non-)results in this regard.
Data collection took place after the first peak in COVID-19 infection rates in Austria and Germany. Several of the governmental interventions regarding infection control were thus already repealed or relaxed. Furthermore, none of our participants reported having tested positively for COVID-19, only 22% reported that a close person had been infected, and two participants reported a death among their family and friends. This context might explain why CAS scores in our sample were highly positively skewed: About 59% (n = 120) of our participants had a sum score of 0 on the scale, and only three persons (1.5%) reached the recommended cutoff point of ≥9 for a clinically significant level of functional impairment (Lee, Citation2020a; Lee, Mathis, et al., Citation2020). Although this is in general a very positive finding regarding mental health in times of COVID-19, it is probably based on the relatively favorable circumstances in Austria and Germany at the time of data gathering. Future research will show whether our findings on correlates of coronavirus anxiety will hold in areas or samples which were more severely affected by the pandemic.
Additionally, another limitation of our study concerns the factorial validity of the CAS scale (German version). Our analysis indicated the need for a modification of the original measurement model, i.e., a covariation term between errors of item 1 (“I felt dizzy, lightheaded, or faint, when I read or listened to news about the coronavirus”) and item 5 (“I felt nauseous or had stomach problems when I thought about or was exposed to information about the coronavirus”). Similar adaptations, although for different item pairings, were reported by Ahmed et al. (Citation2020) for the Bangla version and by Choi et al. (Citation2020) for the Korean version of the CAS. The inclusion of covariance between two error terms resulted in an excellent model fit. However, previous validations of the English CAS did not report a need to include this covariation term. Further studies with larger samples are needed to secure the factorial validity of the CAS (German version) as well as to conduct multigroup analysis to test for factorial invariance across demographic groups, an analysis that could not be run in the present study due to the small sample size. Nevertheless, we assume that the validity of the scale is not fundamentally called into question by this correlation of two error terms.
Due to the cross-sectional nature of our data, no conclusions regarding the causal direction of the statistical relationships we found can be drawn. A longitudinal study design, preferably combined with the employment of other measures for mental health than coronavirus anxiety, would yield further and stronger evidence for the role of death anxiety for psychological well-being during the prevailing crisis.
Conclusion
The present study sought to provide the first evidence on how coronavirus anxiety relates to an individual’s personal worldview and their attitudes toward death. We found that coronavirus anxiety was hardly associated with personal worldview but related positively to death anxiety. The latter fits well with a growing body of theory and empirical research in existential psychology on death anxiety as a transdiagnostic factor underlying the development and maintenance of a wide range of mental disorders. In addition, we found a gender effect for coronavirus anxiety in that women reported higher degrees of dysfunctional anxiety related to the new coronavirus than men. Besides findings related to coronavirus anxiety, our study provides evidence of a curvilinear relationship between religiosity and atheism on one side, and death anxiety and death avoidance on the other.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Ahmed, O., Faisal, R. A., Sharker, T., Lee, S. A., & Jobe, M. C. (2020). Adaptation of the Bangla version of the COVID-19 Anxiety Scale. International Journal of Mental Health and Addiction, 1–12. https://doi.org/https://doi.org/10.1007/s11469-020-00357-2
- Berger, P. L. (1967). The sacred canopy: Elements of a sociological theory of religion. Doubleday.
- Bollen, K. A., & Stine, R. A. (1992). Bootstrapping goodness-of-fit measures in structural equation models. Sociological Methods & Research, 21(2), 205–229. https://doi.org/https://doi.org/10.1177/0049124192021002004
- Brewster, M. E., Robinson, M. A., Sandil, R., Esposito, J., & Geiger, E. (2014). Arrantly absent: Atheism in psychological science from 2001 to 2012. The Counseling Psychologist, 42(5), 628–663. https://doi.org/https://doi.org/10.1177/0011000014528051
- Byrne, B. M. (2016). Structural equation modeling with Amos: Basic concepts, applications, and programming (3rd ed.). Routledge, Taylor & Francis Group.
- Choi, E., Lee, J., & Lee, S. A. (2020). Validation of the Korean version of the obsession with COVID-19 scale and the Coronavirus anxiety scale. Death Studies, 1–7. https://doi.org/https://doi.org/10.1080/07481187.2020.1833383
- Dein, S., Loewenthal, K., Lewis, C. A., & Pargament, K. I. (2020). COVID-19, mental health and religion: An agenda for future research. Mental Health, Religion & Culture, 23(1), 1–9. https://doi.org/https://doi.org/10.1080/13674676.2020.1768725
- Eliassen, A. H., Taylor, J., & Lloyd, D. A. (2005). Subjective religiosity and depression in the transition to adulthood. Journal for the Scientific Study of Religion, 44(2), 187–199. https://doi.org/https://doi.org/10.1111/j.1468-5906.2005.00275.x
- Ellis, L., & Wahab, E. A. (2013). Religiosity and fear of death: A theory-oriented review of the empirical literature. Review of Religious Research, 55(1), 149–189. https://doi.org/https://doi.org/10.1007/s13644-012-0064-3
- Evren, C., Evren, B., Dalbudak, E., Topcu, M., & Kutlu, N. (2020). Measuring anxiety related to COVID-19: A Turkish validation study of the Coronavirus Anxiety Scale. Death Studies, 1–7. https://doi.org/https://doi.org/10.1080/07481187.2020.1774969
- Galen, L. W., & Kloet, J. D. (2011). Mental well-being in the religious and the non-religious: Evidence for a curvilinear relationship. Mental Health, Religion & Culture, 14(7), 673–689. https://doi.org/https://doi.org/10.1080/13674676.2010.510829
- George, D., & Mallery, P. (2016). IBM SPSS statistics 23 step by step. A simple guide and reference (14th ed.). Routledge.
- Hall, D. E., Koenig, H. G., & Meador, K. G. (2008). Hitting the target: Why existing measures of “religiousness” are really reverse-scored measures of “secularism”. Explore, 4(6), 368–373. https://doi.org/https://doi.org/10.1016/j.explore.2008.08.002
- Hodapp, B., & Zwingmann, C. (2019). Religiosity/spirituality and mental health: A meta-analysis of studies from the German-speaking area. Journal of Religion and Health, 58(6), 1970–1998. https://doi.org/https://doi.org/10.1007/s10943-019-00759-0
- Iverach, L., Menzies, R. G., & Menzies, R. E. (2014). Death anxiety and its role in psychopathology: Reviewing the status of a transdiagnostic construct. Clinical Psychology Review, 34(7), 580–593. https://doi.org/https://doi.org/10.1016/j.cpr.2014.09.002
- Jansen, J., Schulz-Quach, C., Eisenbeck, N., Carreno, D. F., Schmitz, A., Fountain, R., Franz, M., Schäfer, R., Wong, P. T. P., & Fetz, K. (2019). German version of the Death Attitudes Profile-Revised (DAP-GR) – Translation and validation of a multidimensional measurement of attitudes towards death. BMC Psychology, 7(1), 61. https://doi.org/https://doi.org/10.1186/s40359-019-0336-6
- Jong, J., Ross, R., Philip, T., Chang, S.-H., Simons, N., & Halberstadt, J. (2018). The religious correlates of death anxiety: A systematic review and meta-analysis. Religion, Brain & Behavior, 8(1), 4–20. https://doi.org/https://doi.org/10.1080/2153599X.2016.1238844
- King, M., Marston, L., McManus, S., Brugha, T., Meltzer, H., & Bebbington, P. (2013). Religion, spirituality and mental health: Results from a national study of English households. British Journal of Psychiatry, 202(1), 68–73. https://doi.org/https://doi.org/10.1192/bjp.bp.112.112003
- Lee, S. A. (2020a). Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety. Death Studies, 44(7), 393–401. https://doi.org/https://doi.org/10.1080/07481187.2020.1748481
- Lee, S. A. (2020b). Replication analysis of the Coronavirus Anxiety Scale. Dusunen Adam: The Journal of Psychiatry and Neurological Sciences, 33, 203–205. https://doi.org/https://doi.org/10.14744/DAJPNS.2020.00079
- Lee, S. A., Jobe, M. C., & Mathis, A. A. (2020). Mental health characteristics associated with dysfunctional coronavirus anxiety. Psychological Medicine, 1–2. https://doi.org/https://doi.org/10.1017/S003329172000121X
- Lee, S. A., Jobe, M. C., Mathis, A. A., & Gibbons, J. A. (2020). Incremental validity of coronaphobia: Coronavirus anxiety explains depression, generalized anxiety, and death anxiety. Journal of Anxiety Disorders, 74, 102268. https://doi.org/https://doi.org/10.1016/j.janxdis.2020.102268
- Lee, S. A., Mathis, A. A., Jobe, M. C., & Pappalardo, E. A. (2020). Clinically significant fear and anxiety of COVID-19: A psychometric examination of the Coronavirus Anxiety Scale. Psychiatry Research, 290, 113112. https://doi.org/https://doi.org/10.1016/j.psychres.2020.113112
- Leiner, D. J. (2019). SoSci Survey (Version 3.1.06). https://www.soscisurvey.de
- Maxfield, M., John, S., & Pyszczynski, T. (2014). A terror management perspective on the role of death-related anxiety in psychological dysfunction. The Humanistic Psychologist, 42(1), 35–53. https://doi.org/https://doi.org/10.1080/08873267.2012.732155
- Menzies, R. E., & Menzies, R. G. (2020). Death anxiety in the time of COVID-19: Theoretical explanations and clinical implications. The Cognitive Behaviour Therapist, 13, e19. https://doi.org/https://doi.org/10.1017/S1754470X20000215
- Park, C. L., & Slattery, J. M. (2013). Religion, spirituality, and mental health. In R. F. Paloutzian & C. L. Park (Eds.), Handbook of the psychology of religion and spirituality (2nd ed., pp. 540–559). The Guilford Press.
- Ross, C. E. (1990). Religion and psychological distress. Journal for the Scientific Study of Religion, 29(2), 236–245. https://doi.org/https://doi.org/10.2307/1387431
- Saroglou, V., & Muñoz-García, A. (2008). Individual differences in religion and spirituality: An issue of personality traits and/or values. Journal for the Scientific Study of Religion, 47(1), 83–101. https://doi.org/https://doi.org/10.1111/j.1468-5906.2008.00393.x
- Schnell, T., & Becker, P. (2007). Fragebogen zu Lebensbedeutungen und Lebenssinn: LEBE. Hogrefe.
- Schnell, T. (2011). Religiosität und Spiritualität als Quellen der Sinnerfüllung. In C. Klein, H. Berth, & F. Balck (Eds.), Gesundheit—Religion—Spiritualität: Konzepte, Befunde und Erklärungsansätze (pp. 259–271). Juventa.
- Schnell, T. (2012). Spirituality with and without religion—Differential relationships with personality. Archive for the Psychology of Religion, 34(1), 33–61. https://doi.org/https://doi.org/10.1163/157361212X644495
- Schnell, T. (2014). Meaning in life operationalized: An empirical approach to existential psychology. In S. Kreitler & T. Urbánek (Eds.), Conceptions of meaning (pp. 173–194). Nova Science.
- Schnell, T. (2015). Dimensions of Secularity (DoS): An open inventory to measure facets of secular identities. The International Journal for the Psychology of Religion, 25(4), 272–292. https://doi.org/https://doi.org/10.1080/10508619.2014.967541
- Schnell, T. (2019). Spirituality. In V. Zeigler-Hill & T. K. Shackelford (Eds.), Encyclopedia of personality and individual differences. Springer.
- Schnell, T., Fuchs, D., & Hefti, R. (2020). Worldview under stress: Preliminary findings on cardiovascular and cortisol stress responses predicted by secularity, religiosity, spirituality, and existential search. Journal of Religion and Health. https://doi.org/https://doi.org/10.1007/s10943-020-01008-5
- Schnittker, J. (2001). When is faith enough? The effects of religious involvement on depression. Journal for the Scientific Study of Religion, 40(3), 393–411.
- Solomon, S., Greenberg, J., & Pyszczynksi, T. (2004). The cultural animal: Twenty years of terror management theory and research. In J. Greenberg, S. L. Koole, & T. Pyszczynksi (Eds.), Handbook of experimental existential psychology (pp. 13–34). Guilford.
- Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed., international edition). Pearson.
- Vail, K. E., Rothschild, Z. K., Weise, D. R., Solomon, S., Pyszczynski, T., & Greenberg, J. (2010). A Terror Management analysis of the psychological functions of religion. Personality and Social Psychology Review, 14(1), 84–94. https://doi.org/https://doi.org/10.1177/1088868309351165
- Vittengl, J. R. (2018). A lonely search?: Risk for depression when spirituality exceeds religiosity. The Journal of Nervous and Mental Disease, 206(5), 386–389. https://doi.org/https://doi.org/10.1097/NMD.0000000000000815
- Walker, D. A., & Smith, T. J. (2017). Computing robust, bootstrap-adjusted fit indices for use with nonnormal data. Measurement and Evaluation in Counseling and Development, 50(1-2), 131–137. https://doi.org/https://doi.org/10.1080/07481756.2017.1326748
- Wink, P., & Scott, J. (2005). Does religiousness buffer against the fear of death and dying in late adulthood? Findings from a longitudinal study. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 60(4), P207–P214. https://doi.org/https://doi.org/10.1093/geronb/60.4.p207
- Wong, P. T. P., Reker, G. T., & Gesser, G. (1994). The Death Attitude Profile-Revised: A multidimensional measure of attitudes towards death. In R. A. Neimeyer (Ed.), Death anxiety handbook: Research, instrumentation, and application (pp. 121–148). Taylor & Francis.
- Yalom, I. D. (2008). Staring at the sun: Overcoming the terror of death. Jossey-Bass.