
Abstract
Health-workers are more likely to die by suicide than their counterparts in other occupational groups. The suicide of a staff member can be widely felt by colleagues, leading to complex emotional and cognitive responses. Exposure to suicide heightens the risk of dying by suicide. We investigated the impact of a colleague suicide on National Health Service (NHS) staff. Twenty-nine staff were interviewed; all participants were white British, and so not representative of the ethnic make-up of the NHS. Data were analyzed using grounded theory methods. A theory, “filling in the gaps” was developed. Staff experiences gave rise to needs that were not always met. Staff endeavored to “fill in the gaps” in support; however, sometimes fell through those gaps. Organizational and professional contexts shaped their experiences and responses. Recommendations include skilled and targeted support and compassion for affected staff. Cultural change is needed to challenge suicide stigma and unhelpful narratives.
Introduction
Suicide is a leading cause of death globally, with more than 700,000 people dying by suicide every year (World Health Organization, Citation2021). UK healthcare professionals are at risk of suicide, with female nurses in particular being 23% more likely to die by suicide than their counterparts in the general population (NHS England, Citation2023). Suicide in healthcare workers is known to be elevated in other high-income countries (Milner et al., Citation2016). When someone dies by suicide, it is estimated that up to 135 people are impacted (Cerel et al., Citation2018). This includes work colleagues (Cerel et al., Citation2014).
Those who are affected by suicide experience a complex grief process that may include depression (Shields et al., Citation2015); shame (Törnblom et al., Citation2013); feelings of blame and emptiness (Cerel et al., Citation2017); intrusive thoughts and memories, hopelessness (Bellini et al., Citation2018); and burdensomeness (Talseth & Gilje, Citation2017). They may also experience physical symptoms such as increased pain and physical illnesses or poorer general health (Spillane et al., Citation2017). There is a risk of trauma for those who witness the death or discover the body (Knieper, Citation1999). There is also an association between suicide bereavement and occupational dropout (Pitman et al., Citation2018) and people exposed to suicide are at increased risk of dying by suicide themselves (Hill et al., Citation2020; Pitman et al., Citation2016). Thus, people who are impacted by a suicide require effective and timely support, often called postvention. Andriessen (Citation2009, p. 43) defines postvention as “activities developed by, with, or for suicide survivors, in order to facilitate recovery after suicide and prevent adverse outcomes including suicidal behavior.” Effective postvention support may lessen these risks (Jordan, Citation2017).
Work-related factors are one contributor to suicide in nurses (Groves et al., Citation2023). We do not know if this is the case for other healthcare professionals. However, we do know that needs following a colleague suicide differ across professional groups and are affected by professional identities and workplace cultures (Causer et al., Citation2022).
Previous researchers have explored the impact of patient or client suicide on a range of health professionals (Causer et al., Citation2019; Matandela & Matlakala, Citation2016; Saini et al., Citation2016; Wang et al., Citation2016), and the impact of colleague suicide across a range of job roles (Deheeger, Citation2008; Gulliver et al., Citation2016; Małecka, Citation2022; Sever & Ozdemir, Citation2022). The impact of patient or client suicide on health professionals may include emotional turmoil, stress reactions (Castelli Dransart et al., Citation2017), and severe distress (Wurst et al., Citation2013). Additionally, a perception of responsibility for the death (Gaffney et al., Citation2009), a sense of professional doubt, and fear of legal consequences may persist (Castelli Dransart et al., Citation2017). The experiences of healthcare staff who provide support to colleagues following the suicide of a coworker are reported in our sister paper (Spiers et al., Citation2024). However, there is no evidence globally on how a colleague suicide is experienced by healthcare workers nor what their support experiences or postvention needs are. An empirical evidence base to inform provision is lacking.
We asked, “how is the impact of colleague suicide experienced by NHS staff and what helps and/or hinders affected colleagues in seeking support?”
Methods
A qualitative approach was selected to gain understanding of participants’ experiences, perceptions, and meaning-making processes. We generated data using semi-structured interviews conducted via online video platforms or telephone calls, according to participants’ preferences. We applied a grounded theory analysis (Holton & Walsh, Citation2017), which can be applied within any philosophical paradigm (Holton & Walsh, Citation2017). In the case of this study, we adopted an inductive, exploratory inquiry. Grounded theory is particularly suited to exploring how people experience and resolve their problems, seeking to understand “what is going on” (Gibson & Hartman, Citation2014, p. 2). We used the consolidated criteria for reporting qualitative research (COREQ) checklist to inform our reporting of this study (Tong et al., Citation2007).
Ethics
Ethical approval was granted by the University of Birmingham (ERN_20-1566) and the Health Research Authority (IRAS 291050). Confidential therapeutic support was available to participants and researchers. We have de-identified all participant data.
Positionality statement
The researchers who undertook the interviews and led on analysis (HC, JS & RR) are all white British women none of whom are currently, nor have previously been, employed by the NHS.
Participants
Participants were recruited via a range of approaches, including NHS Trusts in England, our stakeholder networks e.g. NHS England and NHS Employers, social media posts on X (formally called Twitter) and Facebook groups for NHS staff, and practitioner journals such as the Nursing Standard.
The eligibility criteria were current employees of the NHS who had experienced and were affected by the suicide of a colleague between six months and ten years prior to data collection. Potential participants were sent an information leaflet; participants gave informed consent and completed a demographic questionnaire prior to interview. Despite our efforts to connect with NHS workers from diverse ethnic backgrounds, all participants in this study were white British. Given that minority ethnic people comprise almost a quarter of the NHS workforce (NHS England, Citation2023), we accept that our findings are unlikely to represent the experiences of all staff members.
Data generation
Semi-structured interviews commenced in November 2021 and were completed in January 2023. Dates and times were set at the participants’ convenience. Interviews were undertaken by HC (n = 15), JS (n = 12), and RR (n = 2). A topic guide was used which contained 16 questions about participants’ relationship with the colleague who died; participants’ accounts of their experiences in relation to their colleague’s suicide; experiences of support; and opportunities for learning (Appendix A, supplementary material). The topic guide was informed by and developed in response to, a scoping review of the literature; input from our patient and public involvement and engagement (PPIE) group; a consultation exercise conducted with NHS managers; and the lived experiences of study co-applicants. Interviews were recorded via encrypted audio recorders and were transcribed and de-identified by professional transcribers.
Data analysis
The methodological aim of analysis was to uncover any patterns in reported participant behaviors that explained their main concern (Holton & Walsh, Citation2017). Coding was done by HC alongside ongoing discussion with JS. Data saturation was informed by the quality of the data collected, and depth and rigor of the analytic process (Low, Citation2019). Therefore, the data analysis was considered complete when there was nothing further to add to the categories that had been developed. The analytic process included three stages of coding and category building, the development of a core category, and theoretical conceptualization of the relationships between the core and other categories. At all stages of analysis, constant comparison (Glaser & Strauss, Citation1967), analytic memoing, memo sorting (Holton & Walsh, Citation2017), and diagraming (Saldaňa, Citation2016) were used. Engaging these tools promoted an ongoing iterative and reflective process of comparing and checking as codes, categories, and the relationships across and between them were developed. The full analytic process is described in Appendix B, supplementary material.
Findings
Twenty-nine NHS employees gave consent to participate in the study. Interviews lasted in a range from 45–90 min (mean: 1 hr 7 min). Participant characteristics are presented in .
Table 1. Participant characteristics.
We present the developed grounded theory below, followed by each of the categories with illustrative verbatim quotes. Findings about “the workplace” and “professional identities” are reported within other category sections to reflect the integration that was evident throughout our analysis.
A grounded theory
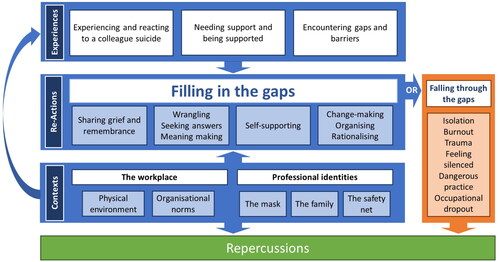
Analysis resulted in the development of a grounded theory, “filling in the gaps” (). The theory combines seven categories and one core category. illustrates the relationships between and across the categories. Participants experiences included the event of their colleague’s suicide, their experiences of needing support and being supported and their encountering of gaps and barriers to the support that they required. In response to these gaps and barriers, participants acted, and reacted in a range of ways, to “fill in the gaps.” The prevalence of participant reactions in their accounts, and the emotional vehemence with which participants spoke about them, illustrated the centrality of this aspect to their experience. As such, they are captured in the core category, “filling in the gaps” which describes the many ways that participants sought to support themselves and their colleagues in the absence or failure of formal provision of acknowledgment, information, and support. For some participants, however, the experience was more akin to “falling through the gaps,” which resulted in a range of challenging outcomes. Participant accounts evidenced how their experiences and reactions throughout were shaped by their work environments, the physical and cultural environment of the workplace, and the multiple aspects of their professional identities. For all participants, there were repercussions to their experiences, that for some, continue to impact on their professional or personal lives.
Figure 1. Filling in the gaps: A grounded theory of the NHS staff experiences following a colleague death by suicide.
Experiencing and reacting to a colleague suicide
Some participants’ experiences began with the discovery of a colleague’s body and active attempts to save a colleague’s life.
my brain went just full paramedic mode […] like didn’t think. Erm so yeah then we started CPR [cardiopulmonary resuscitation] and when [the ambulance arrived] I ran to warn them who it was cause I just didn’t want my colleagues to have the shock that I’ve had. Like I, it’s gonna be awful for them anyway, but I wanted [to warn them]. (Paramedic)
However, most participants heard the news of their colleague’s suicide either via an online or in-person meeting, telephone call, by word of mouth from other colleagues, or through less formal channels: “we all found out through social media” (Nurse).
I got a text message from a colleague saying “is it true that one of your juniors has killed themselves?”[…] and I was like oh crikey, you know I was really shocked because I hadn’t [been informed] […] I kind of found out about it in a less than ideal way and then spent a bit of time erm trying to establish you know what had happened and what we needed to do. (Consultant)
The way in which participants received the news was affected by the physical and cultural contexts of the workplace, and the behavioral norms of their professional identities. Some heard the news via an online meeting and were advised to turn off their cameras and mute themselves so that their responses remained “private.” Participants reported mixed feelings about this privatizing of their grief/shock responses: some believed it was sensitive, others found it disrupted the shared experience and was isolating and harmful: “I was left alone with my thoughts and feelings” (Administrative Assistant). One participant was haunted by the memory of hearing a colleague crying because they hadn’t muted their microphone, but not knowing who it was.
Initial reactions described included shock, emotional and grief responses. Some felt anger toward their deceased colleague and found it difficult to express this:
it would have been hard for me just to … say “actually I’m not sad, I’m fucking pissed off.” Cause it’s not what a lot of the other people were saying. (Therapist)
The professional mask was used as a means of conforming to the dominant narrative of invulnerability and expectations about carrying on. However, professional identities, where healing was central, led some to doubt their professionalism.
I’ve had a real wobble myself […] not feeling suicidal, but really, a crisis of confidence in terms of am I doing a good job? You know? Am I ok as a nurse? What’s it all about? All those sorts of questions, you know, if you can’t protect your own what [are] we doing? Are we doing this the right way? (Nurse manager)
The conceptualization of and sense of belonging to the “professional family” magnified some participants’ sense of loss, grief, guilt, or anger.
it’s what a family would go through […] we spend more time in our workplaces with the people we work with, than sometimes our own family and it does feel like family, so that loss was as deep, as hurtful as a family member. (Nurse)
Such emotional responses were still present, for some, years after the event.
Needing support and being supported
Participants reported needing support to manage and validate their emotional responses, processing, and ability to continue working. Additionally, they needed permission and protected spaces to talk, a confirmed point of contact who would regularly check in with them, and clear signposting to other resources.
Experiences of being supported included structured, informal, and self-generated support, which was delivered within the workplace as well as through peer and personal networks. Support, if provided, came from team leaders or managers, staff wellbeing/liaison services, or an NHS chaplain. When staff could share memories of their colleague, they felt supported and able to process events and feelings.
and [my manager] said “I want you all to go into the office […] I need you as a team to be together and supporting one another” so, we did […] we all got together and just sat and laughed and cried and laughed and cried. And, you know it was nice to be together, support one another. (Nurse)
Many participants described being together with colleagues, sharing space, and talking as vital. Disconnection from colleagues, however, due to different job roles or ways of working, generated feelings of being “othered,” or overlooked for some.
Finance departments are sort of notoriously erm … I think we get the reputation of being the grey robot people so the - one would expect that that you know signposting probably wouldn’t have been that great, erm we probably couldn’t get any further away from clinical services. Had I worked in the clinical team I guess that I would have had erm probably better support and signposting probably would have been there straight away but, but that’s not something we had. (Accountant)
So, while the “professional family” can feel safe, supportive, and inclusive to some, it can feel remote, exclusive, and discriminatory to others.
Overall, support did not meet most participants’ needs. Some reported offers of support that never materialized, while others chose not to engage with the available support. Some felt that managers needed training to be able to offer empathic, compassionate support. Several felt that an impartial/external person to provide support would be beneficial and would avoid placing the burden of support on a manager who was also affected by the suicide. Participants felt they were expected to “reach out” and ask for support rather than supporters “reaching in” to ask what they needed.
The managers are there, we know they’re there, but they never initiated anything like “are you all okay” um, “are you all alright, do you need five minutes to chat with me about anything?” That never occurred. (Support worker)
Encountering gaps and barriers
Most participants reported gaps in support provision or barriers to accessing support. They described miscommunications or insensitivities; pre-conceptions of professional identities such as invulnerability; and cultures of silence and secrecy around the suicide, where everything was felt by staff to be “brushed under the carpet” (Nurse manager).
Participants who were informed of the death whilst working faced the challenge of having to continue to perform. A stoic “carry on” narrative appeared to be woven through the culture of teams and organizations which, when combined with a “patient-first” value-base, created a barrier to staff feeling “allowed” to attend to their own needs.
In many instances, participants reported a complete absence of support, where both the death of their colleague and the impact on staff went unacknowledged.
there’s, there’s been nothing to remember [our colleague] from the NHS. Nothing at all. Erm, you see where other people died of cancer or something, then they have a lot of recognition. Erm, but there’s been nothing for [our colleague] […] and [they] must have worked in the NHS for about 20-odd years. (Support worker)
The lack of staff-only spaces or meeting rooms posed challenges to participants who needed private or shared spaces in which to express their feelings.
Some participants reported that their professional identity prevented the release of difficult feelings, slowed down processing, and acted as a barrier to accessing support: “we’re terrible at going to the doctors or seeking any – any sort of support. So, we don’t practise what we preach” (Nurse). There was a sense of challenge around crossing the line from perceptions of being the “healer” to the “patient.”
Coming up against these gaps and barriers led to secondary impacts such as perceptions of being dismissed or ignored or feeling invisible. There were additional hurdles to overcome and feelings to process, such as the task of self-care to make up for lack of support or the risk of continuing to work without support or safeguards in place. These experiences gave rise to intense frustration, anger, or bitterness, emotions which disrupted participants’ ability to process thoughts and feelings.
The anger about how the lack of support from the organization was getting in the way of us grieving and thinking about [our colleague]. (Allied health worker)
Participants, including those who worked with suicidal patients, reported a lack of process to check if they were safe to practice following the suicide of their colleague.
in [my] role, you’re by yourself. A lot of that time I was on my own and then, nobody said, nobody thought that could be really horrible, knowing what’s just happened […] [It was] just unsafe for everybody really. (Associate practitioner)
Filling in the gaps
Participants’ main concern was the gaps in their support. This core category describes the diverse ways participants responded to those failings and absences. The work of responding became a prominent focus, disrupting the work of loss and grief. This dominated accounts and greatly influenced participants’ experiences.
we supported ourselves as a team. I think that’s how we got through it really, rather than the managers being at the forefront of it, if I’m being honest. (Support worker)
Filling in the gaps was a necessity for several reasons: so that staff could process their feelings and thoughts about what had happened; so that they could remember and honor their colleague in ways that felt appropriate and compassionate; and to enable them to continue to work safely. The work entailed in filling in the gaps happened both within and beyond the workplace and alongside participants’ need to process their grief. One recalled the efforts required to ask for time off to attend their colleague’s funeral.
I remember having to build myself up for […] the conversation, why I want [the day of the funeral] off, and it being a case of, I’ll see what I can do as opposed to yeah, we’ll get it sorted, and so I just remember thinking, I’m not gonna get this. And it was very, [last minute] only that day that I got confirmation. (Nurse)
The strategies that participants engaged in response to these gaps included sharing grief and remembrance with peers; self-supporting, change-making, organizing, and rationalizing; wrangling processes, such as meaning-making; going into professional mode; not speaking and self-protection; and doing things differently.
Sharing grief and remembrance
The loss of a colleague is a shared experience; having the time to talk about that loss collectively appeared crucial for some participants through the earliest days following the death. The importance of talking, remembering, and crying together came through in several accounts, but more important was being physically present with each other.
Participants felt that sharing helped them to process, release difficult feelings, and reconcile with what had happened. Those who were able to be together found this helpful. “And so people just shared stories, expressed their sadness, um, might have been a little bit of ventilation, it helped” (Nurse).
Due to COVID-19 restrictions, some participants were unable to meet. They spoke of the difficulty of being apart: “it feels hard to see someone upset and not be able to put an arm around them or comfort them in a physical way” (Therapist).
There was a felt need by participants to remember their colleague. If facilitation of remembrance was absent, participants created ways to do so informally, like a chat in the workplace, formally, through activities such as visiting their colleague’s grave, or through actions like creating a space in honor of their colleague.
there was a tree right in the corner of the car park, and we, we made it [our colleague’s] tree, and we went and planted things and put flowers in the tree. You know, just made it really beautiful. (Therapist)
Some reported a culture where their colleague was often spoken of in their workspaces.
every new member of the team, that comes into the team, you know I’ll say “You know we used to have a colleague called [name] and we talk about her so you know so if we are laughing about her and talking about her that’s who she is, and this is what happened.” (Support worker)
Self-supporting, change-making, organizing, rationalizing
Staff employed a range of proactive behaviors to support themselves and their colleagues. They made requests for counseling, accessed their GPs, found information online, drew on personal support networks, and found support via other organizations. Sometimes, these actions were underpinned by uncertainty and a lack of guidance alongside the realization that action was needed in the absence of formal provision. For instance, one nurse recalled arranging a get-together with colleagues.
There wasn’t any, you know, manualized OK, let’s just go to the “colleague who’s just died by suicide” book, you know, and, and structure it in this way. There’s nothing like that, it was […] just an acknowledgment that we, that we’ve lost [our colleague] and my sense of speaking to people is that there’s a lot of pain and heartache out there. And um, people might benefit from having an opportunity to get together […] I wasn’t sure whether I had permission to do this. (Nurse)
By employing this range of proactive behaviors, participants created the space and time they needed to attend to tasks such as checking in on each other, organizing memorials, and working through their ideas and understanding about the death.
We helped each other. We’d meet, we’d meet for a coffee somewhere and chat and say how we was feeling. I think we got more comfort from that. (Support worker)
Wrangling, seeking answers, and meaning-making
All participants shared experiences of cognitive “wrangling” with the death as they struggled to find resolution or answers and to fill in the gaps in their understanding. Some described going round in circles with unanswerable questions, which felt excruciating. This wrangling impacted all participants, often remaining unresolved.
Sometimes you wonder, I wonder if she, you know, that’s a stupid question ‘cause she’s done it – but if she’d regret it [laughs]. It’s a stupid question. But actually, it’s like – yeah, so it, it’s those bits of just trying to make sense of something that – that – it’s difficult. (Clinical manager)
It seemed that being a healthcare professional led participants to self-scrutiny, questioning why they didn’t notice, and why they couldn’t save their colleague, “did [we] really know them?” (Nurse); “were we complicit?” (Therapist).
we’re a mental health team – we work a lot with suicidal patients, and then you start questioning yourself, like, well why didn’t we notice it? Like, what could we have done, like why couldn’t we help her? Like, this is our job, and she’s one of us, and and we’ve lost her. (Assistant practitioner)
These processes seemed to be shaped by the shared professional identity. Participants often spoke collectively, saying “we” when they spoke about seeking answers or understanding around their colleague’s death. In framing these thought processes as being collective, there emerged a shared sense of responsibility.
Additionally, some participants asked if systemic structures, cultural expectations and behaviors, institutional narratives, and discourses had contributed to their colleague’s death. Participants experienced cognitive wrangling, their thoughts jumping from one line of questioning to another, as they tried to find answers.
And this ongoing bad management I think is what upsets me. Because it was, I feel like all these failings affected [my colleague] to the extent that [pause] I don’t think that’s why she did it. I don’t think so. And I don’t think that even with the greatest management in the world it would have [pause] changed what she did that day? Because I fully accept that it was her mental health. It was so much more complex than just [mental health]. (Paramedic)
Falling through the gaps
Some participants were left with unresolved, complex feelings and thoughts about their experience due to insufficient or absent support. This could result in stress and burnout.
I just completely burnt out and had to have some time off, yeah, everything just kind of piled up. Erm, and yeah, I definitely became depressed and I just, well my tank was empty, that’s how it felt […] Like I’d be sat at my laptop but physically couldn’t do anything. So yeah I had to take [some time] off. (Assistant therapist)
The lack of acknowledgment, support, and safeguarding of staff working with suicidal patients led to increased anxieties around this aspect of their work.
you have your patients that are suicidal and so you you’re listening to them, and so it does put you on edge. You’re frightened of you know [when] you can’t be there, you you’re going in for 45 minutes to talk to somebody. You know and then you’re closing the door and leaving them and it’s, yeah it’s frightening. (Support worker)
Repercussions
Most participants described some form of impact or legacy following the event. These “repercussions” were not only about recovery, healing, or “getting over it”; but also about ongoing effects. As they continued to work, they did so alongside the impact of their experiences, which shaped their approach to work and sense of self.
there’s a little part of me that worries maybe I’ve just kind of shut down or just become that’s my way of protecting myself or yeah distancing it a bit. (Therapist)
This impact meant that others experience of work was compromised or harmed.
Which makes it hard […] going back to work, you want to do your best, [describes new job-role] like it’s an amazing [opportunity] and I can’t make the most of it. And that gets on your mental health too. Yeah, it’s all [a] spiral. (Paramedic)
Participants described career impact, with some leaving their jobs:
we’re working with high levels of risk on a daily basis […] I’ve found it really difficult, I’m, I’m actually, I’m leaving the team in the near future. So I’m I’m, moving out of mental health services. (Allied health practitioner)
I think what [their] death did, did do, as [my colleague] said is that it changed our personal culture of you know how we are with each, how we look after each other on the unit. How we, we check in with each other a lot more. (Doctor)
what I found comforting was to imagine err [my colleague] as like a little fairy godmother, a cartoon. Erm and she swore a lot. So I was imagining her as this little fairy godmother, waving her wand and swearing as she goes. And err yeah so I wrote that to one of my colleagues and they said “yes yes, that’s exactly it!” […] And so that’s comforting and happy and makes me smile. (Administrator)
Discussion
We asked, “how is the impact of colleague suicide experienced by NHS staff and what helps and/or hinders affected colleagues in seeking support?” Our findings demonstrated that participants experienced diverse impacts and that their experiences of seeking support where hindered when they encountered a range of gaps in, and barriers to, provision.
When NHS staff are affected by the suicide of a colleague, they experience a complicated emotional response ranging from shock, despair, and grief to guilt, anger, and fear. Their experiences and reactions give rise to a range of support needs. In seeking to have those needs met, they encounter diverse gaps and barriers to provision. Their subsequent actions and reactions take the form of filling in those gaps for themselves and their colleagues. Some colleagues fall through the gaps entirely. Workers’ experiences, needs, actions, and reactions are informed by two contexts: workplace norms, narratives, and cultures; and individual and shared professional identities. Throughout these experiences, staff employ emotional labor (in addition to that already employed in their work) to manage their complex responses which impact their emotional and psychological health. The efforts that they engage to overcome and fill the gaps in support lead to difficulties and disruptions in processing their feelings; perceptions of isolation; consequences for patient-facing work, particularly when working with patients who display suicidal behaviors; and occupational dropout.
Participants spoke of colleague relationships as reaching beyond the professional and becoming friendships. These relational aspects shaped responses to the suicide. Such stories of closeness align with those told by Colbert et al. (Citation2016), who evidence a range of “functions” within workplace relationships that include friendship and the opportunity to give to others. Indeed, perceptions of closeness (Cerel et al., Citation2017) are of greater relevance than familial relationships in informing the extent of impact following a suicide. Thus, it is likely that the suicide of a close colleague will leave coworkers in need of support, for which workplaces must be prepared.
The perception of being part of a workplace “family” was a key factor in shaping the shared professional identities of study participants. Many used the collective “we,” when describing experiences, responses, or reactions following their colleague’s suicide, suggesting a strong sense of shared experience. Connection with colleagues and experiences of support from them and from leadership figures are protective factors for health workers (West, Citation2021). This phenomenon may not be exclusive to healthcare professionals; staff in UK universities found that perceptions of belongingness and community nurtured a sense of closeness to a student following their death by suicide (Causer et al., Citation2021). Belonging to a “workplace family” and experiencing coworker support is associated with better worker health and less exhaustion (Maben et al., Citation2012; Treiber & Davis, Citation2012) and may serve as a protective factor against workplace stresses and challenges (Riley et al., Citation2021). So, it appears that the concept of “family” in the workplace may serve to heighten responses to a colleague death, but also provide protective factors in managing personal responses. This sense of a shared experience contrasts with the reported experiences of healthcare professionals who perceived themselves as isolated following the death by suicide of a patient or client (Causer et al., Citation2019). This raises the question of whether it is the perception of losing a “family” member, as opposed to a patient, that generates this difference.
There was a dominant narrative of professionalism across participant accounts. References to the “professional mask” highlighted how participants put their emotions aside to manage the demands of their roles. Employees may suppress or regulate emotions following a stressful event to deliver an appropriate emotional presentation for the workplace (Grandey, Citation2000). Emotional management of this kind has been conceptualized as emotional labor (Hochschild, Citation1983). This cognitive dissonance leads to stress, which can lead to burnout (Zapf & Holz, Citation2006). Participants in this study employed the “professional mask” as performativity associated with emotional labor (Riley & Weiss, Citation2016). The suppression of felt emotions, whilst presenting the self in a “preferred,” or “approved of” manner may lead to emotional dissonance and internal tension (Morris & Feldman, Citation1996), which they needed time and space to resolve.
Our findings suggest that participants needed safe, protected time and spaces to be together, talk, process, share memories, and make plans for memorializing their colleague. These spaces were often not available. A lack of training and resources for supporting staff after a suicide was detrimental to people’s ability to cope, process, and move forward. This aligns with the experiences of doctors and nurses following a patient death by suicide, who have reported a lack of postvention support (Malik et al., Citation2022). Creating safe, protected time and space for processing and healing may prevent mid- and long-term harm such as extended periods of sick leave or people choosing to change/leave profession (Uys et al., Citation2023). Our findings suggest that such short-term investment could garner long-term economic and workforce benefits. The need for time and space challenged participants’ embedded perceptions of invulnerability, within the context of organizational narratives about “carrying on.” They faced a duality of experience as their need to share and be together impinged on the work culture that prizes invulnerability both organizationally and individually (Maben et al., Citation2021).
Participants found themselves with nowhere to go in a culture that stigmatized and silenced the topic of suicide, they were left to take care of themselves and their colleagues by “filling in” the gaps in support. Our findings evidenced a lack of acknowledgment by senior leaders and organizations of a colleague suicide. Participant experiences of the “minimization” of their colleague’s suicide and their own responses left them bewildered and angry. When the life of someone who died by suicide goes unacknowledged, there is a sense that the individual becomes objectified by the means of their death (Yue, Citation2022). Such de-personalization contributes to the perpetuation of stigmatized conceptions of suicide in the workplace (McGrath et al., Citation2023).
An absence of support, alongside the “carry on” narrative and culture of silence, generates a sense of invisibility. Staff perceive this as a message that their organization does not want to acknowledge their distress. This prompted us to query what impact this may have on perceptions of trust between staff and employers. Organizational failure to respond to staff suicide renders it a “non-event”; thus, it is invisible and staff needs are overlooked. Effective support might include compassionate, supportive leadership that normalizes vulnerability, and access to therapeutic interventions (Riley et al., Citation2021).
Our findings further evidenced an absence of attention given to staff members who work with patients or clients who experience suicidality. Participants spoke of their distress at having to deal with suicidal patients in different settings around the time of their colleague’s suicide. None reported safe practice conversations with supervisors or assessments to ensure their fitness to practice following the suicide of their colleague. They spoke of feeling unsafe, and of their concerns for patient safety. This reported failure to recognize affected staff members’ needs may increase the likelihood of staff operating below their usual capacity, increase risk of professional errors or lead to reduced patient safety.
Strengths and limitations
This is the first study to investigate the experiences and needs of NHS staff following a colleague death by suicide. The novel findings add to knowledge of the impact of suicide in the workplace, specifically in healthcare settings. The findings are pertinent to senior leaders and policymakers, within and beyond NHS Trusts and Integrated Care Boards who wish to understand the postvention needs of staff in healthcare settings. The developed grounded theory provides an empirical evidence base that will contribute to the development of much-needed postvention guidance for the NHS. We aimed to build theory based on an inductive understanding of participants’ experiences, perceptions, and needs; qualitative methods are best suited to such aims. Grounded theory is suited to un-researched topics and populations (Holton & Walsh, Citation2017).
We made efforts during our participant recruitment period to establish connections with ethnically diverse populations of NHS workers. Despite this, our sample was solely white British. Given that Black and minority ethnic people comprise almost a quarter of the NHS workforce (NHS England, Citation2023), our findings are unlikely to represent the experiences of all staff members.
Most participants talked about deaths which ranged from less than a year ago to four years ago. However, four participants were talking about deaths which had occurred nine to ten years ago, meaning their memories of that time may have been impacted.
Recommendations
In line with our published guidelines (Riley et al., Citation2023), we make the following recommendations:
Staff need to hear the news of their colleague’s death in a timely and sensitive manner.
Staff need safe and private spaces in which they can come together to talk, process, share memories, and make plans for remembrance of their colleague.
Psychological support should be available, clearly signposted, and offered repeatedly over the first weeks and months.
A culture that challenges stigma around mental health and suicide and that validates difficult feelings (such as anger) is essential for giving staff permission to process their responses to their colleague’s suicide.
Staff may need robust permission to “step out of role,” put their own needs first, and look after themselves as they see fit.
All staff affected by a colleague suicide should be consulted and their ability to return to full duty discussed with them. A wellbeing assessment should be undertaken with affected staff who work with patients at risk of suicide.
Staff who do not engage with support should be followed up to find out if specific support is required.
Memorialization activities chosen by colleagues should be encouraged by senior leads and trusts.
Trusts should acknowledge the suicide of a colleague and pay respect to the colleague as they would if they had died by any other means.
Future research is needed to explore the experiences of minority ethnic healthcare workers following a colleague death by suicide. In addition, we suggest that evaluation of the implementation of our recommendations would increase understanding of what works in practice.
Conclusion
Our data suggest the needs of staff affected by the suicide of a colleague were rarely met, with some falling through the gaps and suicide stigma and unhelpful narratives prevalent. Work is required to challenge such stigma and narratives and to ensure culture change to better support the psychological wellbeing of healthcare staff affected.
Supplemental Material
Download MS Word (22.8 KB)Acknowledgments
We are grateful to our study participants who generously shared their experiences and stories with us.
Disclosure statement
The authors declare no conflict of interest. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NIHR, NHS or the Department of Health.
Data availability statement
Data is not available. The sharing of qualitative data would violate the privacy and consent of study participants.
Additional information
Funding
References
- Andriessen, K. (2009). Can postvention be prevention? Crisis, 30(1), 43–47. https://doi.org/10.1027/0227-5910.30.1.43
- Bellini, S., Erbuto, D., Andriessen, K., Milelli, M., Innamorati, M., Lester, D., Sampogna, G., Fiorillo, A., & Pompili, M. (2018). Depression, hopelessness, and complicated grief in survivors of suicide. Frontiers in Psychology, 9, 198. https://doi.org/10.3389/fpsyg.2018.00198
- Castelli Dransart, D. A., Treven, M., Grad, O. T., & Andriessen, K. (2017). Impact of client suicide on health and mental health professionals. In K. Andriessen, K. Krysinska, & O. T. Grad (Eds.), Postvention in action: The international handbook of suicide bereavement support (pp. 245–254). Hogrefe. https://doi.org/10.1027/00493-000
- Causer, H., Bradley, E., Muse, K., & Smith, J. (2021). Bearing witness: A grounded theory of the experiences of staff at two United Kingdom higher education institutions following a student death by suicide. PLoS One, 16(5), e0251369. https://doi.org/10.1371/journal.pone.0251369
- Causer, H., Muse, K., Smith, J., & Bradley, E. (2019). What is the experience of practitioners in health, education or social care roles following a death by suicide? A qualitative research synthesis. International Journal of Environmental Research and Public Health, 16(18), 3293. https://doi.org/10.3390/ijerph16183293
- Causer, H., Spiers, J., Efstathiou, N., Aston, S., Chew-Graham, C. A., Gopfert, A., Grayling, K., Maben, J., van Hove, M., & Riley, R. (2022). The impact of colleague suicide and the current state of postvention guidance for affected co-workers: A critical integrative review. International Journal of Environmental Research and Public Health, 19(18), 11565. https://doi.org/10.3390/ijerph191811565
- Cerel, J., Brown, M. M., Maple, M., Singleton, M., van de Venne, J., Moore, M., & Flaherty, C. (2018). How many people are exposed to suicide? Not six. Suicide & Life-Threatening Behavior, 49(2), 529–534. https://doi.org/10.1111/sltb.12450
- Cerel, J., Maple, M., van de Venne, J., Brown, M., Moore, M., & Flaherty, C. (2017). Suicide exposure in the population: Perceptions of impact and closeness. Suicide & Life-Threatening Behavior, 47(6), 696–708. https://doi.org/10.1111/sltb.12333
- Cerel, J., McIntosh, J. L., Neimeyer, R. A., Maple, M., & Marshall, D. (2014). The continuum of “survivorship”: Definitional issues in the aftermath of suicide. Suicide & Life-Threatening Behavior, 44(6), 591–600. https://doi.org/10.1111/sltb.12093
- Colbert, A. E., Bono, J. E., & Purvanova, R. K. (2016). Flourishing via workplace relationships: Moving beyond instrumental support. Academy of Management Journal, 59(4), 1199–1223. https://doi.org/10.5465/amj.2014.0506
- Deheeger, J. (2008). Suicide of a service member: How to organize support for the bereaved service members in the emotional aftermath. In B. K. Wiederhold (Ed.), Lowering suicide risk in returning troops: Wounds of war (pp. 149–161). Ios Press.
- Gaffney, P., Russell, V., Collins, K., Bergin, A., Halligan, P., Carey, C., & Coyle, S. (2009). Impact of patient suicide on front-line staff in Ireland. Death Studies, 33(7), 639–656. https://doi.org/10.1080/07481180903011990
- Gibson, B., & Hartman, J. (2014). Rediscovering grounded theory. Sage.
- Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory: Strategies for qualitative research. Aldine Transaction.
- Grandey, A. A. (2000). Emotional regulation in the workplace: A new way to conceptualize emotional labor. Journal of Occupational Health Psychology, 5(1), 95–110. https://doi.org/10.1037/1076-8998.5.1.95
- Groves, S., Lascelles, K., & Hawton, K. (2023). Suicide, self-harm, and suicide ideation in nurses and midwives: A systematic review of prevalence, contributory factors, and interventions. Journal of Affective Disorders, 331, 393–404. https://doi.org/10.1016/j.jad.2023.03.027
- Gulliver, S. B., Pennington, M. L., Leto, F., Cammarata, C., Ostiguy, W., Zavodny, C., Kimbrel, N. A., & Flynn, E. J. (2016). In the wake of suicide: Developing guidelines for suicide postvention in fire service. Death Studies, 40(2), 121–128. https://doi.org/10.1080/07481187.2015.1077357
- Hill, N. T. M., Robinson, J., Pirkis, J., Andriessen, K., Krysinska, K., Payne, A., Boland, A., Clarke, A., Milner, A., Witt, K., Krohn, S., & Lampit, A. (2020). Association of suicidal behavior with exposure to suicide and suicide attempt: A systematic review and multilevel meta-analysis. PLoS Medicine, 17(3), e1003074. PMID: 32231381 32. https://doi.org/10.1371/journal.pmed.1003074
- Hochschild, A. R. (1983). The managed heart: Commercialization of human feeling. University California Press.
- Holton, J. A., & Walsh, I. (2017). Classic grounded theory: Applications with qualitative and quantitative data. Sage.
- Jordan, J. R. (2017). Postvention is prevention: The case for suicide prostvention. Death Studies, 41(10), 614–621. https://doi.org/10.1080/07481187.2017.1335544
- Knieper, A. J. (1999). The suicide survivor’s grief and recovery. Suicide & Life-Threatening Behavior, 29(4), 353–364. https://doi.org/10.1111/j.1943-278X.1999.tb00530.x
- Low, J. (2019). A pragmatic definition of the concept of theoretical saturation. Sociological Focus, 52(2), 131–139. https://doi.org/10.1080/00380237.2018.1544514
- Maben, J., Adams, M., Peccei, R., Murrells, T., & Robert, G. (2012). ‘Poppets and parcels’: The links between staff experience of work and acutely ill older peoples’ experience of hospital care. International Journal of Older People Nursing, 7(2), 83–94. https://doi.org/10.1111/j.1748-3743.2012.00326.x
- Maben, J., Taylor, C., Reynolds, E., McCarthy, I., & Leamy, M. (2021). Realist evaluation of Schwartz rounds® for enhancing the delivery of compassionate healthcare: Understanding how they work, for whom, and in what contexts. BMC Health Services Research, 21(1), 709. https://doi.org/10.1186/s12913-021-06483-4
- Małecka, K. A. (2022). “Have you heard about X?”: (Mis) management of mortality in academia. Death Studies, 46(7), 1678–1688. https://doi.org/10.1080/07481187.2020.1830888
- Malik, S., Gunn, S., & Robertson, N. (2022). The impact of patient suicide on doctors and nurses: A critical interpretive meta-synthesis. Archives of Suicide Research: official Journal of the International Academy for Suicide Research, 26(3), 1266–1285. https://doi.org/10.1080/13811118.2021.1885533
- Matandela, M., & Matlakala, M. C. (2016). Nurses’ experiences of inpatients suicide in a general hospital. Health SA Gesondheid (Online), 21(1), 54–59. https://doi.org/10.1016/j.hsag.2015.10.001
- McGrath, M. O., Krysinska, K., Reavley, N. J., Andriessen, K., & Pirkis, J. (2023). Disclosure of mental health problems or suicidality at work: A systematic review. International Journal of Environmental Research and Public Health, 20(8), 5548. https://doi.org/10.3390/ijerph20085548
- Milner, A. J., Maheen, H., Bismark, M. M., & Spittal, M. J. (2016). Suicide by health professionals: A retrospective mortality study in Australia, 2001-2012. The Medical Journal of Australia, 205(6), 260–265. https://doi.org/10.5694/mja15.01044
- Morris, J. A., & Feldman, D. C. (1996). The dimensions, antecedents, and consequences of emotional labor. The Academy of Management Review, 21(4), 986–1010. https://doi.org/10.5465/amr.1996.9704071861
- NHS England. (2023). Working together to prevent suicide in the NHS workforce. Retrieved November 14, 2023, from https://www.england.nhs.uk/long-read/working-together-to-prevent-suicide-in-the-nhs-workforce/
- Pitman, A., Putri, A. K., De Souza, T., Stevenson, F., King, M., Osborn, D., & Morant, N. (2018). The impact of suicide bereavement on educational and occupational functioning: A qualitative study of 460 bereaved adults. International Journal of Environmental Research and Public Health, 15(4), 643. https://doi.org/10.3390/ijerph15040643
- Pitman, A. L., Osborn, D. P. J., Rantell, K., & King, M. B. (2016). Bereavement by suicide as a risk factor for suicide attempt: A cross-sectional national UK-wide study of 3432 young bereaved adults. BMJ Open, 6(1), e009948. https://doi.org/10.1136/bmjopen-2015-009948
- Riley, R., Causer, H., Spiers, J., Chew-Graham, C. A., Efstathiou, N., Gopfert, A., Grayling, K., Maben, J., & van Hove, M. (2023). Postvention guidance: Supporting NHS staff after the death by suicide of a colleague. University of Surrey. uos-suicide-postvention-brochure.pdf (surrey.ac.uk)
- Riley, R., Kokab, F., Buszewicz, M., Gopfert, A., Van Hove, M., Taylor, A. K., Teoh, K., Martin, J., Appleby, L., & Chew-Graham, C. (2021). Protective factors and sources of support in the workplace as experienced by UK foundation and junior doctors: A qualitative study. BMJ Open, 11(6), e045588. https://doi.org/10.1136/bmjopen-2020-045588
- Riley, R., & Weiss, M. C. (2016). A qualitative thematic review: Emotional labour in healthcare settings. Journal of Advanced Nursing, 72(1), 6–17. https://doi.org/10.1111/jan.12738
- Saini, P., Chantler, K., While, D., & Kapur, N. (2016). Do GPs want or need formal support following a patient suicide?: A mixed methods study. Family Practice, 33(4), 414–420. https://doi.org/10.1093/fampra/cmw040
- Saldaňa, J. (2016). The coding manual for qualitative researchers. Sage.
- Sever, M., & Ozdemir, S. (2022). How an academic’s death by suicide impacts coworkers and an organization. Death Studies, 46(2), 323–328. https://doi.org/10.1080/07481187.2019.1700572
- Shields, C., Kavanagh, M., & Russo, K. (2015). A qualitative systematic review of the bereavement process following suicide. Omega, 74(4), 426–454. https://doi.org/10.1177/0030222815612281
- Spiers, J., Causer, H., Chew-Graham, C. A., Efstathiou, N., Gopfert, A., Grayling, K., Maben, J., van Hove, M., & Riley, R. (2024). Negotiating the postvention situation: A grounded theory of NHS staff experiences when supporting their co-workers following a colleague’s suicide. Death Studies, 1–11. https://doi.org/10.1080/07481187.2023.2297056
- Spillane, A., Larkin, C., Corcoran, P., Matvienko-Sikar, K., Riordan, F., & Arensman, E. (2017). Physical and psychosomatic health outcomes in people bereaved by suicide compared to people bereaved by other modes of death: A systematic review. BMC Public Health, 17(1), 939. https://doi.org/10.1186/s12889-017-4930-3
- Talseth, A. G., & Gilje, F. L. (2017). Liberating burdensomeness of suicide survivorship loss: A critical interpretive synthesis. Journal of Clinical Nursing, 26(23-24), 3843–3858. https://doi.org/10.1111/jocn.13797
- Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care: journal of the International Society for Quality in Health Care, 19(6), 349–357. https://doi.org/10.1093/intqhc/mzm042
- Törnblom, A. W., Werbart, A., & Rydelius, P. A. (2013). Shame behind the masks: The parents’ perspective on their sons’ suicide. Archives of Suicide Research: official Journal of the International Academy for Suicide Research, 17(3), 242–261. https://doi.org/10.1080/13811118.2013.805644
- Treiber, L. A., & Davis, S. N. (2012). The role of ‘workplace family’ support on worker health, exhaustion and pain. Community, Work & Family, 15(1), 1–27. https://doi.org/10.1080/13668803.2011.580123
- Uys, C., Carrieri, D., & Mattick, K. (2023). The impact of shared social spaces on the wellness and learning of junior doctors: A scoping review. Medical Education, 57(4), 315–330. https://doi.org/10.1111/medu.14946
- Wang, S., Ding, X., Hu, D., Zhang, K., & Huang, D. (2016). A qualitative study on nurses’ reactions to inpatient suicide in a general hospital. International Journal of Nursing Sciences, 3(4), 354–361. https://doi.org/10.1016/j.ijnss.2016.07.007
- West, M. A. (2021). Compassionate leadership: Sustaining wisdom, humanity and presence in health and social care. Swirling Leaf Press.
- World Health Organization. (2021). One in 100 deaths is by Suicide. Retrieved August 30, 2022, from https://www.who.int/news/item/17-06-2021-one-in-100-deaths-is-by-suicide
- Wurst, F. M., Kunz, I., Skipper, G., Wolfersdorf, M., Beine, K. H., Vogel, R., Müller, S., Petitjean, S., & Thon, N. (2013). How therapists react to patient’s suicide: Findings and consequences for health care professionals’ wellbeing. General Hospital Psychiatry, 35(5), 565–570. https://doi.org/10.1016/j.genhosppsych.2013.05.003
- Yue, E. (2022). Comment made in response to: ‘Weaponizing time in the war on welfare: Slow violence and welfare-related deaths [Paper presentation]. Suicide Cultures Seminar, University of Edinburgh.
- Zapf, D., & Holz, M. (2006). On the positive and negative effects of emotion work in organizations. European Journal of Work and Organizational Psychology, 15(1), 1–28. https://doi.org/10.1080/13594320500412199
