
Abstract
The Dual Process Model of Coping with Bereavement (DPM) proposes that there is an adaptive oscillation between loss-oriented (LO) and restorative-oriented (RO) coping processes. Empirical data supports these processes, but the oscillation process is not well-understood. This study explored the correspondence between the DPM and lived experience of bereaved people, with an additional investigation of perceived changes in grief over time. Using a cooperative inquiry inspired participatory research design, nine bereaved adults and three researchers met nine times to discuss experiences of grief. Knowledge production took place through ongoing sharing, exploration, and reflection upon personal experiences and grief theory. Support was found for the LO and RO processes, but they were perceived to overlap. Support was also found for the oscillation process, which was found to hold learning properties. Time off from grief was not supported. Perspectives on how and why grief experiences change over time emerged, emphasizing the importance of acceptance, learning, time, and contextual factors.
Introduction
Most bereaved adults experience an adaptive, yet often painful, grieving process following the loss of a person with whom they had a close relationship (Bonanno & Malgaroli, Citation2020; O’Connor, Citation2010). The intensity of the grief symptoms typically declines over the first 6 months following bereavement (Lundorff et al., Citation2019; Nielsen et al., Citation2019) without requiring specialized professional intervention (Bonanno & Kaltman, Citation2001; Prigerson et al., Citation2009). The Dual Process Model of Coping with Bereavement (DPM; Stroebe & Schut, Citation1999, Citation2010) provides a current theoretical framework for understanding the process of adapting to bereavement and was the topic of investigation in the present study.
The dual process model of coping with bereavement
The DPM proposes that, in response to the death of a other, a bereaved person engages in loss-oriented (LO) and restoration-oriented (RO) coping to manage feelings of grief and stressors of everyday life following the loss (Stroebe & Schut, Citation1999, Citation2010). LO coping consists of traditional grief work, including yearning for the deceased, ruminating about the death, reappraising the meaning of the loss, adjusting the relational bond to the fact that the deceased is dead, and confronting expected and unexpected grief-related feelings and reactions (Stroebe & Schut, Citation1999, Citation2010). LO coping is thought to dominate early in the grief process, i.e., during acute grief (Fiore, Citation2021). In addition, the bereaved person may be preoccupied with thoughts about events leading up to and following the death, and trying to understand and come to terms with the loss (Eisma et al., Citation2022; Lundorff et al., Citation2019). RO coping is activated as the bereaved person deals with loss-related secondary stressors (Stroebe & Schut, Citation1999, Citation2010). In adjusting to a life without the deceased, the bereaved person may face considerable challenges. Some challenges surface immediately, such as making funeral arrangements, handling legal issues, and perhaps responding to financial concerns. Others are can be more long-term, such as having to take on new roles and responsibilities and rethink plans and goals in life. These challenges and changes may be associated with additional emotional distress (Eisma et al., Citation2022).
An adaptive approach to loss is believed to consist of a flexible oscillation between LO and RO coping (Stroebe & Schut, Citation1999, Citation2010). It is presumed that one cannot simultaneously attend to both LO and RO stressors (Eisma et al., Citation2022; Stroebe & Schut, Citation1999), but rather one alters between confronting and avoiding each of the processes. Consequently, stressors are confronted in manageable doses (Lundorff et al., Citation2019; Stroebe & Schut, Citation1999). This dosing mechanism helps ensure that the demands of the loss do not greatly exceed and overwhelm the person’s resources for coping death (Stroebe & Schut, Citation1999, Citation2016). The DPM model also incorporates necessary periods of time off from grief, where the bereaved person “simply relaxes and recuperates” while engaging in non-bereavement activities (Stroebe & Schut, Citation2016, p. 99). Bereaved persons who fail to flexibly oscillate between the LO and RO coping processes, and who do not experience necessary breaks, are at risk for developing grief complications. For example, complications can occur when a person exclusively struggles with the painful experiences of grief (loss-oriented focus) and fails to attend to, or actively avoids dealing with, the associated more practical consequences. Or when a person attempts to ignore the reality of death and the associated negative emotions, while instead focusing exclusively on addressing the secondary consequences and getting on with life (restoration-oriented focus). In 2016, Strobe and Schut introduced another obstacle to an adaptive grieving process. They wrote about the idea of “overload”, which happens when the bereaved person’s coping resources are outmatched by the demands of grief and the loss-related consequences. This, in turn, can lead to additional feelings of pressure, distress, anxiety, or exhaustion. In conclusion, the DPM offers ideas for how to think about both adaptive and complicated grief processes.
The DPM is an influential and well supported theoretical model (Fiore, Citation2021). It is widely used to inform grief interventions (see Lund et al., Citation2010; Shear et al., Citation2005; Zuckoff et al., Citation2006) and public education about grief, as evidenced by grief-related websites (e.g., @Compass_Resource_Group, n.d.; Applebury, Citation2021; Williams, Citation2014). However, there are elements of the DPM which remain not fully understood. For example, the oscillation process remains difficult to comprehend and measure. Further, the DPM says little about how the experience of grief changes over time. Additional empirical exploration and validation of the DPM model could help advance our understanding of grief as a natural healing process following loss.
Exploring grief through participatory research
Participatory research within healthcare settings has become widespread in diverse fields of research. It involves conducting research with people with lived experiences rather than about or for them. It represents the idea that multiple perspectives will enhance the quality and relevance of the research (Kothari et al., Citation2022). This participatory approach challenges scientific communities to rethink research processes and democratize knowledge production by creating space for co-researchers with lived experiences to partner with academic researchers in research endeavors (Sangill et al., Citation2019).
In the present study, we explored the experience of grief through cooperative inquiry (Heron, Citation1996; Heron & Reason, Citation2001), a method of participatory research where people with different experiences and expertise (e.g., lived or academic experience and expertise) work together toward a common goal. As co-researchers, the participants seek to make sense of experiences and produce new knowledge in a creative, dynamic process, consisting of repeated dynamic cycles of reflection and action within a workgroup. That is, a topic is explored and critically evaluated by all co-researchers, and then a course of action is agreed upon (Heron & Reason, Citation2001). The present study deviated from a traditional cooperative inquiry approach in that the goals for the inquiry were pre-determined by the academic researchers. The aim was not to change a particular practice, but rather to describe and explain a domain of experience, akin to an informative cooperative inquiry, which might yield future transformative implications (Heron, Citation1996). The cooperative inquiry approach was seen as a useful method to explore and evaluate the applicability of the DPM as it relates to the lived experience of bereaved people.
The aim of the present study was to investigate the DPM’s applicability to bereaved people’s lived experience with grief in general, and to learn more about two aspects of the DPM not currently well-understood or described, namely the oscillation process and potential changes in the experience of grief over time. With this aim, we sought to further explore the validity and applicability of the DPM to lived experience.
Methods
Design
As mentioned above, the study design consisted of a participatory research approach, inspired by the cooperative inquiry method (Heron, Citation1996; Heron & Reason, Citation2001). In an informative cooperative inquiry, propositions concerning the nature of the domain of interest are explored and revealed from a lived experience perspective (Heron, Citation1996). Data production and evaluation (analysis) was achieved through dialogue among the group’s participants with the study aims in mind (Tsoukas, Citation2009). Data sources consisted of the meeting dialogue, participant-approved minutes, written participant-completed assignments, and the development of an expanded version of the DPM (the project’s outcome output). The study is presented in line with the Consolidated Criteria for Reporting Qualitative Research (Tong et al. Citation2007) with the checklist presented as an online supplemental document.
Participants
Participants were recruited through grief support organizations within the greater Copenhagen area, Denmark. Those interested in participating were asked to contact the study coordinator (LHL). Inclusion criteria were: (1) being at least 28 years old, (2) having lost a close other at least one year prior, (3) generally functioning well in day-to-day life but still experiencing grief, and (4) being interested in sharing one’s lived experience with grief. The lower limit of 28 years was chosen due to our interest in studying grief in adults, who were relatively settled in life. That is, we wanted to limit the degree of potential added stress associated with developmental tasks of young adulthood (e.g., transition from school to work, moving away from home and settling into independent living, establishing a family etc.), potentially interfering with or interacting with grief experiences and processes. During the initial phone conversation with potential participants, eligibility was assessed and information about the project and expectations for participation were addressed. A diverse group of bereaved participants was selected, representing different types of loss experiences. Variation among the participants was sought in terms of age, gender, kinship to the deceased, time since the death, and causes of death. The final selection, made from the available pool of possible participants, consisted of nine bereaved adults, ranging in age from 33 to 79 years (see ). While some participants had experienced a sudden loss due to suicide or after a short course of illness, e.g., 3 weeks, it should be mentioned that recruitment efforts did not lead to enrollment of participants with a sudden non-illness related loss, such as following an accident or natural disaster, although such losses were within the inclusion criteria. All who were invited to participate in the study accepted the invitation, and there were no dropouts over the course of the study. The cooperative inquiry group also included two clinical Ph.D. research psychologists (LHL and MOC) and a Ph.D. research nurse (LH). An anthropologist/visual artist participated in two meetings focusing on creativity and grief. A research assistant was present during the meetings to help with practical matters and take minutes. None of the bereaved participants were known to the researchers prior to the study. The bereaved participants received a gift certificate in an amount equivalent to $70 per meeting as compensation for their time and participation.
Table 1. Bereaved workgroup participants.
Procedure and knowledge production
Knowledge about the applicability of the DPM to lived experience was generated during nine meetings of three hours each, held at the offices of the Danish National Center for Grief in Copenhagen, Denmark in the spring of 2022. Authors LHL and LH co-facilitated seven of the meetings. Two meetings were led by an anthropologist/artist. The meetings were facilitated to engage the participants in dialogue, fostering an interplay between experiences, reflection, and sense-making (Heron, Citation1996). Each meeting had an overall structure, consisting of a brief welcome/introduction, review of the meeting agenda, approval of the meeting minutes from the prior meeting, a presentation and discussion of a theme, and a wrap-up of the meeting, including review of home assignments. The theme varied from meeting to meeting and included sharing personal experiences, discussing grief theories, and developing a method and questionnaire to assess changes in grief over time. Two meetings explored the potential role of creative processes in grieving and coping. At the final meeting, an open feedback evaluation (Christiansen & Rosenkvist, Citation2008) was conducted to assess the participants’ thoughts on the cooperative inquiry process, their satisfaction with the final outcomes, and any personal benefits or challenges experienced due to their participation.
The approval of minutes at each meeting served to ensure that experiences, opinions, and explanations were accurately perceived and recorded by the researchers. Between meetings, the bereaved participants completed assignments to encourage personal reflection and idea-generation in preparation for the following meeting. The academic researchers reviewed, organized, and condensed information from the preceding meeting where relevant. The assignments and condensed information were then presented, discussed, and elaborated upon at the subsequent meeting. Several themes ended up being discussed multiple times (e.g., grief reactions, the importance of time, and changes over time). Knowledge was produced in an ongoing dialogical process of sharing experiences, interpersonal reflection, and joint meaning-making across multiple voices (i.e., reflecting participant’s lived experiences, values, and thoughts). There was a tension between the centripetal tendency toward unity (e.g., seeking consensus) and the centrifugal tendency toward difference (e.g., expressing diverse experience and options; see Phillips et al., Citation2022).
Ethical consideration
The study design and protocol were reviewed and approved by the Research Ethics Committee at Aarhus University, Denmark (Journal no.: 2021-0302497) and submitted to the Center for Open Science (Larsen et al., Citation2022).
Sharing experiences of grief and bearing witness to those of others can be emotionally taxing. Consequently, the study participants were offered the opportunity to talk to a psychologist during the study period, should they become overwhelmed by grief or negative feelings due to their participation. None of the participants requested such support.
Results
An expanded dual process model of coping with bereavement
The bereaved group participants found the DPM to accurately reflect lived experiences with some notable exceptions. The group discussed how the model might be modified to better reflect their experiences. Over the course of many meetings and extensive group discussions, several drafts of an expanded version of the DPM were developed. The final version is presented in and also includes added descriptions of the participants’ perceived changes in grief over time.
Figure 1. Changes in grief expereinces over time.
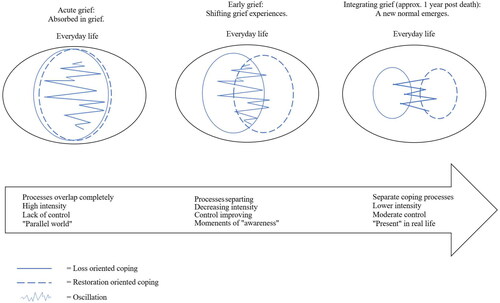
The expanded model shows the LO and RO coping processes overlapping initially but then gradually becoming more separate over time. Time off is not included, as the bereaved participants did not feel it was possible to take breaks from their grief. The expanded model further shows the participants’ experiences with changes in the intensity of their grief, in the sense of control they experienced, and in the degree to which they felt connected to other people and reality. The participants found time to be an important factor in the progression of their grief experience but were unable to pinpoint an exact timeline for when changes had occurred. The first several months had been particularly difficult, followed by a period of adjusting. After about one year following the loss, they felt something had changed. They somehow felt more settled in their new reality. At this point, having to cope with grief had become less dominant (as indicated by smaller circles in ), and they could turn their attention to more typical (none-grief-related) everyday life activities. However, their loss and grief had not disappeared, but rather had become integrated into their lives and identities.
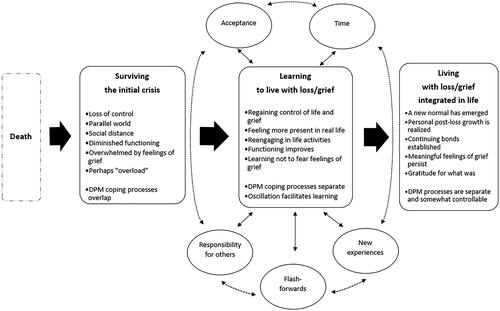
A conceptual map of changes in grief over time
To capture both the expanded model of the DPM and the additional content of the group discussions, the academic researchers subsequently developed a conceptual map (see ). Below we discuss the map’s components.
Figure 2. Conceptual map of perceived changes in grief as discussed by the work group participants.
Surviving the initial crisis
Overlapping coping responses
When learning about the DPM (Stroebe & Schut, Citation1999), the bereaved group members immediately recognized the LO and RO coping processes and the oscillation between the two from their own grief experiences. In the presented visual representation of the model, LO and RO were depicted as separate processes, which did not entirely match the participants’ experience. The bereaved workgroup participants were unanimous, when they noted that, in the initial acute grief, they experienced almost complete overlap between the two processes. They were overwhelmed by multiple stressors, which prevented a flexible oscillation in their coping responses—akin to what Stroebe and Schut has described as overload (Stroebe & Schut, Citation2016). One participant noted: “You are in one process that contains elements of both processes” (P7). Another explained: “The processes are not 100% separate. They become more separated over time. But in the beginning, you are in both processes at the same time” (P6). When asked to provide examples of being in both processes, one participant said: “The squeezing of the heart, does not disappear just because I go to work” (P7), suggesting that the physical pain and sadness of the loss was present, when he was trying to resume going to work. Another example was provided, when a member talked about going to the grocery store—attempting to restore an everyday task—and then falling apart with debilitating feelings of grief while standing in line to pay. In general, the bereaved group members felt that the DPM failed to take in account the physical pain and cognitive challenges experienced concurrently with the emotional pain.
Existing in a parallel world
Another grief reaction not reflected in the DMP had to do with a change in the bereaved persons’ experience of being present in the real world. The bereaved participants initially discussed feeling disconnected from the world, as if they existed in what they termed a “parallel world”. During the first several months following the loss, their experiences of being in the world seemed unreal and uncontrollable. They felt as if they were on “autopilot”, in a “zombie-like state” or in “another dimension” compared to those around them. They described somehow being able to take care of what they needed to but doing so without truly feeling present in the moment. One participant described it as “a paradox of life stopping and continuing at the same time” (P2). Gradually, once the acute crisis had begun to ease, the participants felt more in control of their lives, becoming more aware of living in the real world. They described that they started making proactive decisions, rather than merely reacting. They began to make choices based on their own needs and wants. They started feeling more like themselves, present in their own bodies. One participant described the experience this way: “It was as if I had been shot out into space, and I was circling the earth in my own little orbit, far away. I could see the earth, but I was not a part of it. Gradually, my trajectory would get closer and closer to earth, until I eventually found myself back there” (P8).
Learning to live with loss and grief
Following a period of crisis and disbelief, the reality of what had happened began to set in, as did a period of adjusting. The bereaved group members reported experiencing a growing ability to control their grief and lives. The DPM coping processes began to separate. Previously, empirical studies have found a similar increase in perceived control over the oscillation process developing over time (Lundorff et al., Citation2019). The participants noted that learning about grief, seeking information to help understand the process of grief and their experiences, and meeting others in similar situations were helpful activities. Gradually, they became able to better concentrate and focus on restorative activities. For example, they returned to work and school, accepted invitations to social gatherings, started to find enjoyment in activities again (e.g., reading for pleasure, listening to music), and they established new everyday routines. One participant described the experience as “going from being a spectator to being an active participant” (P8). In addition, they began to develop the ability to reengage in LO coping at will and to experience feelings of gratitude in addition to the pain.
Oscillation promotes learning
The bereaved group members found that the DPM did not sufficiently capture how the oscillation process involves an accumulation of learning that facilitates an ongoing momentum in the adaptation process. For example, LO activities of remembering and missing the deceased and thinking about, what he or she would have wanted for the bereaved person, could serve as a motivator or “internal force” which helped the bereaved person handle issues in the RO process. Missing a deceased partner, remembering his values and approaches to things, inspired and encouraged a bereaved participant to try to handle parenting responsibilities like he had. One participant noted: “What you learn in one process is useful and helpful in the other process, in the new life you are adapting to” (P6). The bereaved person is thereby shaped by their grief experience in helpful ways. Another participant described this learning process as carrying a backpack which gets filled with experiences and lessons learned along the way. In RO coping, the bereaved person is learning to manage in a new everyday life, which helps promote a new sense of self-reliance, which, in turn, can help in the LO process when strong feelings of grief hit. Over time, especially after the first year, the bereaved person learns that the challenges brought on by the death can be managed.
External and internal causes had contributed to the oscillation. For example, the bereaved group members noted that stopping engaging in LO coping could be motivated by external demands, such as caretaking responsibility, social demands, practical issues, work or educational responsibilities. It could also be caused by internal demands, such as feeling hungry or tired, feeling bored or emotionally exhausted, or experiencing a desire to do somethings else. Stopping engaging in RO coping could likewise be motivated by external cues, e.g., situations, places or people that triggered grief-related feelings. Internal cues could also trigger a change away from RO coping, for example when feeling a need to be close to the deceased, to connect with one’s grief, or to express bottled-up feelings. Other internal triggers could be spontaneous physical sensations of grief, when feeling frustrated and helplessness when facing difficult practical problems, when finding life meaningless without the deceased, and following an intrusive memory. Feelings of grief could also appear for no apparent reason. While the oscillation process initially was perceived as automatic and involuntary, the bereaved participants gradually felt more in control. They became able to, in a sense, control the dosing of their RO or LO coping activities based on their immediate needs.
The importance of time
The participants agreed that the passing of time played a significant role in adapting to their losses. There was a sense that time afforded new learning experiences and opportunities, which helped them figure out how to live without the deceased. One participant talked about feeling like a tilting doll, rounded at the bottom, allowing it to tilt over on its side only to automatically right itself again. With time she had learned that when she felt knocked over and overwhelmed by grief, it was not a permanent state. Rather, she would recover and feel okay again. This lesson taught her not to fear her grief. Stroebe and Schut (Citation1999) also pointed to time playing a role in coping with a loss. They seemed to suggest that the active ingredient is that time affords habituation. They noted that “In the course of time, after sufficient, perhaps repeated exposure and confrontation, there may no longer be a need to think about certain aspect of the loss. Habituation has taken place” (Stroebe & Schut (Citation1999, p. 216). In this study, however, learning how to navigate, not merely getting used to, new life circumstances was the key. This is exemplified by the backpack and tilting doll metaphors described earlier.
While the participants could not specify how much time was needed to learn how to cope with a difficult loss, they agreed that the one year mark held significance. For some, it was then they began to realize that they had made significant gains in their adjustment (e.g., they could focus on other things than the loss or feel joy again), and therefore felt more hopeful that they would be okay in the future. One participant described how he, after one year of being consumed by grief, made a conscious decision to “pull [himself] up by the bootstraps “(P9) and start focusing on moving on in life. He had trouble explaining what led to that decision, and how he was able to act on it. He offered one possible reason: “Having lived through one year without her…the holidays, birthdays. That helped us understand that we could manage without her “(P9). Another group member said:” All I know is that it took a year, before I could feel happiness without feeling an underlying feeling of grief at the same time “(P5). Another participant noted: “It took one year before spontaneous experiences of happiness started to happen again” (P2).
The importance of acceptance
Stroebe and Schut (Citation1999) did not address the issue of acceptance at great length. They did note that “In our framework, it is also necessary to accept the reality of the changed world” (p. 215). The participants in the present study agreed and discussed how reaching a form of acceptance was an essential milestone in the grieving process. One participant said: “Time plays a role, but it is really about accepting your situation. The realization that the person is dead. It just takes time to understand” (P5). Some took issue with the word accept, preferring to refer to a need to “recognize” or “acknowledge” what had happened. There was agreement, though, that this notion of acceptance or acknowledgement of the death was necessary for moving from focusing on who and what was lost to a more present- and future-oriented focus. It also made it possible to appreciate the past and experience feelings of gratitude.
Being responsible for others promoted coping
The complex and important role of the external context when adapting to loss was addressed by Stroebe and Schut in their article on family matters (Stroebe & Schut, Citation2015). Within the workgroup, the bereaved participants also recognized the external context as an important factor, affecting their grief trajectories in important ways. Those with responsibility for family members or pets, and those who needed to return to work- or school-related responsibilities, found this to be helpful in many ways. For example, it provided a helpful structure to everyday life in an otherwise chaotic life circumstance; it helped restore a sense of meaning and purpose; it required action when one lacked motivation to do things; and it provided an external focus, requiring attention to be pulled away from one’s internal emotional distress. Having responsibility for others was perceived as a driving force in progressing in one’s grieving process, by providing a reason to get up in the morning and keeping a momentum going when life otherwise felt at a standstill. Having responsibilities was also seen to help promote meaningful ways of maintaining a bond with the deceased, for example when taking on tasks that used to be done by the deceased, thinking about the deceased, and emulating his or her approach. A mother reported initially having felt angry that her deceased husband had left her to take care of their children on her own, but she came to see parenting responsibilities as an important catalyst for her grief process. One young man, reflecting on his grief process, noted that the lack of responsibility for others might have contributed to him “getting stuck” in the LO process. He wondered if he had spent more time and personal resources on the internal emotional toll of grief, because he lacked an external pull back to “real life.”
On the other hand, too many external responsibilities might be a hindrance, when little time and emotional energy is left for LO coping, including paying attention to one’s feelings and needs. This was the experience of a woman who suddenly became responsible for running and selling a large property. Her attention and energy had to be directed at dealing with the property, at the expense of paying attention to her feelings and processing her mother’s death. She seemed to have experienced an overload of external stressor, much in line with what Stroebe and Schut addressed in their 2016 publication on overload. The group concluded that having a manageable amount of external responsibility did not necessarily reduce grief, but provided motivation, meaning, and purpose, and might have facilitated overall adaptation.
No timeouts but moments of awareness
The workgroup discussed the DPM’s proposed timeouts, i.e., moments in the adaptation process without experiences of grief, at great length. According to Stroebe and Schut (Citation1999, p. 216), “[t]he person may choose to take ‘time out,’ be distracted, or need to attend to new things, or at times it may be too painful to confront some aspect, leading to voluntary suppression or more involuntary repression.” The participants in the present study did not experience that it was possible to take a break from their grief. In the first months after the loss, the participants described trying to distract themselves from their grief, but they never truly felt able to ignore or avoid it—it had become part of their existence. One participant tried to reconnect with old friends following her husband’s death, but she was unable to ignore the absence of her husband and a physical sensation of grief. Going on trips and binge-watching TV shows were mentioned as activities meant to distract from grief; to some degree they did, but not completely. The loss was described as ever-present, impossible to escape, as if life now was experienced through a new lens which incorporated grief. The closest they came to what seemed like a break, were brief experiences of increased awareness of being present in real life. The group came to think of those as spontaneous “flash-forwards.” They were described as glimpses of “normalcy”—a more recognizable sense of existence. These flash-forwards were only recognizable after-the-fact and gradually increased in frequency and duration, as greater integration of and adjustment to life after the loss took place. Flash-forwards were experienced as positive, holding the promise that life would get better. One participant noted: “It is as if life grabs a hold of you again” (P6).
Living with loss and grief integrated in life
At some point after about one year had passed since the death, a new normal had set in for the bereaved participants. Grief was still present, but it had become more manageable and an integrated, meaningful part of life. Having learned to better manage one’s thoughts and feelings related to the loss, it had become possible to reengage in LO coping at will. For example, when wanting to feel closer to the deceased or when experiencing physical discomfort perceived to be loss-related, the bereaved person could reconnect with feelings of grief and for example seek relief through crying. Part of the restoration process included finding ways the deceased could continue to play a role in the bereaved person’s life, i.e., ways to continue the bond (Klass et al., Citation1996). This could occur when engaging in activities the deceased had enjoyed (e.g., listening to music), taking over responsibilities from the deceased (e.g., making a certain dish for family birthday parties), or continuing a tradition in honor of the deceased. Maintaining an ongoing relationship with the deceased was seen as a source of contentment and as a helpful internal force. Although the participants reported a greater sense of control over their experiences of grief over time, they agreed that they never felt fully in control of it. Even several years following the loss, waves of grief could hit at any time, seemingly out of the blue. On the other hand, they also noted that the nature or quality of their grief changed from being primarily painful and debilitating, to also containing feeling close to the deceased and feeling gratitude for what was. One participant noted, “…grief is not just ‘over-and-done’ but a lifelong condition. And that is okay” (P1).
When looking back on their experiences with grief, the discussion often returned to how grief had changed them as a people, often promoting personal growth. Examples of personal changes included a) shifts in self-perception, i.e., identity, purpose, and presence in the world; b) feeling greater clarity around priorities, values, and life goals c) experiencing life more intensely; and d) developing greater tolerance of differences among people. Thus, looking back, the participants recognized that the loss, in the long run, was associated with not only negative and painful feelings but also with positive experiences, feelings, and personal changes.
Additional observations on the DPM
The DPM may be more relevant for some than for others
An observation made by the group was that the two coping processes may vary in their relevance depending on the type of loss experienced. For some group members, the death of their loved one had had a profound impact on their everyday life, sense of identity, and future. For others this was not the case. For example, losing a parent as an adult did not necessitate drastic changes in routines and responsibilities, though the experience of grief could be quite profound. So, for several bereaved group members some elements of the RO process seemed less relevant. Thus, the group members wondered if the DPM was more reflective of some grieving processes than others.
It was also noted that those, who had lost a person with whom they had had a conflictual or ambivalent relationship, did not feel the DPM captured the complexities of their loss. They suggested that rather than grieving the loss of the person, they were grieving what they never had and over having lost the possibility that the relationship might improve in the future. The group members felt it was unreasonable to expect the DPM to account for all grief experiences, but wanted to point out that there can be unique circumstances and losses, which are relevant to keep in mind when trying to understand the experience of bereaved people.
The DPM overlooks some secondary losses
The group members discussed how their loss of a particular person (e.g., husband, mother, child) was associated with other related losses. For example, they spoke of grieving the loss of the support and comfort which the deceased person used to provide; grieving that their children would not have a grandparent; grieving the lost ability to share important future milestones; and feeling grief associated with the loss of future dreams and plans. In addition, some reported feeling grief associated with the loss of one’s naively perceived belief that life is safe, predictable, and controllable—this illusion vanished with the death of their important others. These types of secondary losses seemed qualitatively different from those described in the DPM. The workgroup seemed to be describing secondary losses associated with the attachment bond and the interpersonal relationship, whereas the DPM seems to focus on secondary consequences related to more practical everyday life circumstances as well as changes in the bereaved person’s identity and social/familial roles.
Discussion
We set out to investigate concordance between the DPM and lived experience of bereaved adults. Indeed, the bereaved participants in the study reported seeing their grief process reflected in the DPM to a large extent. They recognized the LO and RO coping processes but did not perceive them as two entirely separate processes. Rather, they were perceived to overlap, particularly in the beginning. Gradually over time they had become more separate (see ). The idea of overlapping coping processes has been discussed previously. For example, when exploring adaptive and maladaptive use of avoidance during acute grief, Shear (Citation2010) proposed that LO and RO coping might better be shown visually as overlapping, concurrent processes, where it is the private experiences of thoughts and emotions that oscillate (Shear, Citation2010). Shear also hypothesized that restoration-related activities facilitate processing of the loss. For example, when bereaved people work to cope with new life circumstances without the deceased being present, they must simultaneously work to accept and process the loss. In the present study, when the bereaved father started listening to music and attending concerts again, he did that without his son and had to simultaneously process feelings of grief brought on by this restorative activity. Shear further suggested that successful coping with restoration-related stressors can make the acceptance of the finality of the loss (i.e., LO coping) less frightening and signal that is might be possible to find satisfaction and pleasure in the new life (Shear, Citation2010). A study examining the subjective experiences of bereaved spouses and the DPM found that most participants recognized the LO, RO and oscillation processes, and found them to have been relevant to their subjective grief experiences (Fasse & Zech, Citation2016). However, they also reported that the LO and RO processes were interdependent and indistinguishable from each other early in the grief experience. In sum, the theoretical conceptualization of two clearly separate coping processes does not seem to capture the complexity of lived experience, as least not early in the grief process.
In the present study, the bereaved participants also recognized the experience of oscillating between LO and RO coping processes. They did not perceive it as merely a shifting from one form of coping to the other, or as an attempt to escape from one to the other. Rather they saw the oscillation process as representing an ongoing accumulation of learning and adaptive coping experiences. What they learned in one process, helped inform coping with challenges in the other.
As the oscillation process is not well-understood (Fiore, Citation2021), we aimed to shed additional light on this phenomenon by asking the bereaved participants to reflect upon what might be causing the shifting between the LO and RO coping processes. We were interested in knowing more about when and how oscillation occurs. The participants noted that the shifting could be motivated by internal factors (e.g., emotional, cognitive, or physical) and external demands and cues (e.g., responsibilities or interruptions). Further, oscillation could happen spontaneously (e.g., initiated by known or unknown triggers) or be deliberate (i.e., intentionally initiated by the person). They described that they were unable to control of the oscillation process in the beginning of their grief experience, but over time they became better able to purposefully switch between the two coping processes. Similarly, Fasse and Zech (Citation2016) found that engaging in the LO an RO coping processes could be automatic, by chance, or purposeful.
The DPM proposes that moments of respite (time off) from grief occur in the adaptation process (Stroebe & Schut, Citation1999, Citation2010). This idea seemed foreign to the bereaved members of the workgroup. They described their grief as constant, ever-present, and indistinguishable from who they had become as people. They explained that they might engage in non-grieving activities (such as going to the movies) which could be seen as distractions from grief, but the sense of loss and grief did not disappear; some described it as a constant physical sensation. Over time, the permanent changes created by the loss, such as new rituals and reengagement in activities, would still carry markers of the loss and grief. For example, going to concerts would again be enjoyable, but would also bring back bittersweet memories of attending concerts with the deceased. Traveling to new places would be exciting, but also remind the bereaved person that the deceased person was missing. Finishing school felt like a great accomplishment, but the deceased person was missed at the graduation ceremony. It seemed impossible to return to a lived experience without some form of felt presence of grief.
While not endorsing grief-free timeouts, the participants did report what they came to call flash-forwards. These were brief moments of feeling a sense of normalcy or awareness of being present in the moment. They occurred later in the adjustment process and tended to become more frequent as the loss was becoming integrated in the bereaved person’s life and lived experience. They could perhaps be seen as a type of timeout from actively engaging in the process of grieving but occurring later in the grief process. Some participants in the study by Fasse and Zech (Citation2016) did report of achieving respite from their grief during their grieving process, though these breaks were not consciously undertaken as distractions from their grief, for example engaging with others in non-bereavement related activities. In conclusion, the notion of timeouts from grief during the active grieving process remains complex and poorly understood across studies. It requires additional investigation.
In the present study, we were interested in exploring changes in the grief experience over time, as the DPM does not offer much detail about that. The bereaved participants described a progression through grief, reflecting several changes. There was a perceived gradual decrease in grief intensity, an increase in perceived control over one’s grief and life, improved connectedness with others and the world, strengthening of a continuing bond with the deceased, and the emergence of personal growth. The participants could not pinpoint why or how these changes happened, other than noting that they happened over time, concurrent with their learning to live without the deceased. Overall, the changes they described could be mapped into three-step process involving (1) a period of chaos, focused on surviving the initial crisis; (2) a middle period consisting of learning to accept and live with the loss and grief; and (3) a third period of living a changed life, with the loss and grief integrated into it (see ). The steps were sequential but were overlapping in the transition phases, as learning and adapting gradually solidified. This progression was facilitated by adaptive learning through experiences and the passage of time. Reaching a degree of acceptance of the death and its consequences, having responsibility for others, and experiences moments of normalcy were perceived to be important factors.
Time and learning through experience are important in coping with loss. Stroebe and Schut (Citation2016, p. 100) noted that “Life goes on, and this, in and of itself, can at times be quite beneficial and healing”. They also emphasized that coping with loss is facilitated by exposure and extinction of behaviors and thought, through confrontation and avoidance, resulting in new habits and social reengagement (Stroebe & Schut, Citation2016). Thus the grieving process involves learning new habits and behavioral patterns. Mary Frances O’Connor, a neuroscientist, also conceptualizes grief as a form of learning and describes the process in detail. O’Connor notes that adjusting to a loss, learning to live with it and its consequences, requires time and feedback based on new experiences (O’Connor, Citation2022; O’Connor & Seeley, Citation2022). According to O’Connor, loss of a close other is disorienting. It results in the removal of markers and routines which the bereaved person had come to rely on. Previous predictions and expectations no longer match the new life circumstance. The brain must gather information about this new environment without the deceased and adapt to be able to again make accurate predictions of events in life. In the current study, the adult son who had lost his mother needed to experience many holidays without her, for his brain to learn not to expect her to be there, and for him to learn that he would be able to handle these days. The widow, who had been waking up next to her husband nearly every morning for decades, needed time (and many painful reminders of her loss) for her brain to learn not to expect him to be there. Shear (Citation2010) also emphasizes the role of learning in adapting to loss. She proposed that healing is associated with not only restoration of functioning but also learning to integrate the grief experience into the new life. The participants of the present study gave numerous examples of how they had learned to integrate their grief and the deceased in meaningful ways into the new life. They talked to and about the deceased, remembered them on important days, kept their values and intentions alive, and so on.
Fasse and Zech (Citation2016, p. 231) note that “coping with bereavement takes place in everyday life” and we would add coping happens through a learning process. That is, coping reflects learning, by “filling the backpack” with experiences and feedback from navigating in a new reality without the deceased, resulting in a return to adaptive functioning. The participants in our study exemplified this as they gradually learned not to fear strong feelings grief, because they knew they would subside. They realized that gratitude and positive memories, could replace painful feelings of loss. They learned that activities that seem impossible early on, such as going to work, again became possible. With time it became possible to experience joy without feeling guilty and reconnect with other people. And, as the sense of chaos and lack of control gradually subsided, it became possible to feel normal again.
Limitations
This study had limitations which could limit the generalizability of the findings. For example, the workgroup consisted of a small number of bereaved adults. It was noteworthy though that their lived experiences as they related to the DPM were quite similar to those of others as reported in another study with a similar focus (Fasse & Zech, Citation2016). Two-thirds of the bereaved workgroup members were females. While differences in lived experience based on gender were not observed in the group discussion, a more even distribution of females to males would have been preferable. The study provided interesting information about how grief changes over time, but the time since death was relatively short. Most of the bereaved persons had experienced the loss between 2 to 6 years prior, which limits what we can learn about how grief changes in the long-term. To learn about the process and change of grief over the long-term, a larger time-since-death range would be needed.
Supplemental Material
Download MS Word (38.8 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- @Compass_Resource_Group. (n.d). Grief theory: Dual process model. https://griefcompass.com/dualprocess
- Applebury, G. (2021). The dual process model of grief in simple terms. https://www.lovetoknow.com/life/grief-loss/dual-process-model-grief-simple-terms
- Bonanno, G. A., & Kaltman, S. (2001). The varieties of grief experience. Clinical Psychology Review, 21(5), 705–734. https://doi.org/10.1016/S0272-7358(00)00062-3
- Bonanno, G. A., & Malgaroli, M. (2020). Trajectories of grief: Comparing symptoms from the DSM-5 and ICD-11 diagnoses. Depression and Anxiety, 37(1), 17–25. https://doi.org/10.1002/da.22902
- Christiansen, M., & Rosenkvist, G. (2008). Voksenundervisning—Formidling i praksis. Gyldendal.
- Eisma, M. C., de Lang, T. A., & Stroebe, M. S. (2022). Restoration-oriented stressors of bereavement. Anxiety, Stress, and Coping, 35(3), 339–353. https://doi.org/10.1080/10615806.2021.1957849
- Fasse, L., & Zech, E. (2016). Dual process model of coping with bereavement in the test of the subjective experiences of bereaved spouses: An interpretative phenomenological analysis. OMEGA—Journal of Death and Dying, 74(2), 212–238. https://doi.org/10.1177/0030222815598668
- Fiore, J. (2021). A systematic review of the dual process model of coping with bereavement (1999-2016). Omega, 84(2), 414–458. https://doi.org/10.1177/0030222819893139
- Heron, J. (1996). Cooperative inquiry: Research into the human condition. SAGE.
- Heron, J., & Reason, P. (2001). The practise of co-operative inquiry: Research with rather than on people. In P. Reason & H. Bradbury (Eds.), Handbook of action research. Participate inquiry and practice (pp. 179–188). London: Sage.
- Klass, D., Silverman, P. R., & Nickman, S. L. (1996). Continuing bonds: New understandings of grief. Taylor & Francis.
- Kothari, A., Rycroft-Malone, J., McCutcheon, C., & Graham, I. D. (2022). Introduction. In I. D. Graham, J. Rycroft-Malone, A. Kothari, & C. McCutcheon (Eds.), Research co‐production in healthcare. (pp. 1–13). Wiley-Blackwell. https://doi.org/10.1002/9781119757269.ch1
- Larsen, L. H., O’Connor, M., Hybholt, L., & Schierff, L. H. (2022). An exploration of the processes of grief in the dual process model: A co-operative inquiry-based study. https://doi.org/10.17605/OSF.IO/NG58T
- Lund, D., Caserta, M., Utz, R., & De Vries, B. (2010). Experiences and early coping of bereaved spouses/partners in an intervention based on the dual process model (DPM). Omega, 61(4), 291–313. https://doi.org/10.2190/OM.61.4.c
- Lundorff, M., Thomsen, D. K., Damkier, A., & O’Connor, M. (2019). How do loss- and restoration-oriented coping change across time? A prospective study on adjustment following spousal bereavement. Anxiety, Stress, and Coping, 32(3), 270–285. https://doi.org/10.1080/10615806.2019.1587751
- Nielsen, M. K., Carlsen, A. H., Neergaard, M. A., Bidstrup, P. E., & Guldin, M. B. (2019). Looking beyond the mean in grief trajectories: A prospective, population-based cohort study. Social Science & Medicine, 232, 460–469. https://doi.org/10.1016/j.socscimed.2018.10.007
- O’Connor, M. (2010). A longitudinal study of PTSD in the elderly bereaved: Prevalence and predictors: Erratum. Aging & Mental Health, 14(5), 3–3.
- O’Connor, M. F. (2022). The grieving brain—The surprising science of how we learn from love and loss. Harpercollins Publishers Inc.
- O’Connor, M. F., & Seeley, S. H. (2022). Grieving as a form of learning: Insights from neuroscience applied to grief and loss. Current Opinion in Psychology, 43, 317–322. https://doi.org/10.1016/j.copsyc.2021.08.019
- Phillips, L., Christensen-Strynø, M., & Frølunde, L. (2022). Arts-based co-production in participatory research: Harnessing creativity in the tension between process and product. Evidence & Policy, 18(2), 391–411. https://doi.org/10.1332/174426421X16445103995426
- Prigerson, H. G., Horowitz, M. J., Jacobs, S. C., Parkes, C. M., Aslan, M., Goodkin, K., Raphael, B., Marwit, S. J., Wortman, C., Neimeyer, R. A., Bonanno, G., Block, S. D., Kissane, D., Boelen, P., Maercker, A., Litz, B. T., Johnson, J. G., First, M. B., & Maciejewski, P. K. (2009). Prolonged grief disorder: Psychometric validation of criteria proposed for DSM-V and ICD-11. PLoS Medicine, 6(8), e1000121. https://doi.org/10.1371/journal.pmed.1000121
- Sangill, C., Buus, N., Hybholt, L., & Berring, L. L. (2019). Service user’s actual involvement in mental health research practices: A scoping review. International Journal of Mental Health Nursing, 28(4), 798–815. https://doi.org/10.1111/inm.12594
- Shear, K., Frank, E., Houck, P. R., & Reynolds, C. F. (2005). Treatment of complicated grief: A randomized controlled trial. JAMA, 293(21), 2601–2608. https://doi.org/10.1001/jama.293.21.2601
- Shear, M. K. (2010). Exploring the role of experiential avoidance from the perspective of attachment theory and the dual process model. Omega, 61(4), 357–369. https://doi.org/10.2190/OM.61.4.f
- Stroebe, M., & Schut, H. (1999). The dual process model of coping with bereavement: Rationale and description. Death Studies, 23(3), 197–224. https://doi.org/10.1080/074811899201046
- Stroebe, M., & Schut, H. (2010). The dual process model of coping with bereavement: A decade on. Omega, 61(4), 273–289. https://doi.org/10.2190/OM.61.4.b
- Stroebe, M., & Schut, H. (2015). Family matters in bereavement: Toward an integrative intra-interpersonal coping model. Perspectives on Psychological Science, 10(6), 873–879. https://doi.org/10.1177/1745691615598517
- Stroebe, M., & Schut, H. (2016). Overload: A missing link in the dual process model? OMEGA—Journal of Death and Dying, 74(1), 96–109. https://doi.org/10.1177/0030222816666540
- Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19(6), 349–357.
- Tsoukas, H. (2009). A dialogical approach to the creation of new knowledge in organizations. Organization Science, 20(6), 941–957. https://doi.org/10.1287/orsc.1090.0435
- Williams, L. (2014, September 23, 2014). Grief theory 101: The dual process model of grief. https://whatsyourgrief.com/dual-process-model-of-grief/
- Zuckoff, A., Shear, K., Frank, E., Daley, D. C., Seligman, K., & Silowash, R. (2006). Treating complicated grief and substance use disorders: A pilot study. Journal of Substance Abuse Treatment, 30(3), 205–211. https://doi.org/10.1016/j.jsat.2005.12.001
