
Abstract
Purpose: The aim of this study was to examine the relationship of exercise cardiac power (ECP), defined as a ratio of directly measured maximal oxygen uptake with peak systolic blood pressure during exercise, with the risk of mortality from coronary heart diseases (CHD) and cardiovascular diseases (CVD).
Design: Population-based cohort study with an average follow-up of 25 years from eastern Finland. About 2358 men at baseline participated in exercise stress test and 182 CHD and 302 CVD deaths occurred.
Results: Men with low ECP (< 8.7 mL/mmHg, lowest quartile) had a 3.5-fold (95% CI 2.1–5.8, p < 0.0001) risk of CHD mortality as compared with men with high ECP (>16.4 mL/mmHg, highest quartile) after adjusting for age and examination year. Low ECP was associated with a 2.8-fold risk of CHD and 2.4-fold for CVD mortality after additional adjustment for conventional risk factors. After further adjustment for leisure time physical activity, the results hardly changed (HR 2.5, 95% CI 1.71–3.67, p < 0.001).
Conclusion: ECP provides non-invasive and easily available measure for the prediction of CHD and CVD mortality. One of the most potential explanation for the association between ECP and the risk of CHD and CVD mortality is an elevated afterload and peripheral resistance indicated by hypertension.
Index of exercise cardiac power defined as the ratio of directly measured maximal oxygen uptake (VO2max) with peak systolic blood pressure gives prognostic information in coronary heart disease (CHD) and CVD mortality risk stratification.
ECP provides non-invasive and easily available measure for the prediction of CHD and CVD mortality.
One of the most potential explanation for the association between ECP and the risk of CHD and CVD mortality is an elevated afterload and peripheral resistance indicated by hypertension.
Key messages
Introduction
The most important marker of cardiovascular risk yielded by the exercise test is the measure of exercise capacity (Citation1–3). Previous population-based studies have looked at the ability of indirectly defined functional capacity to predict total mortality and other cardiovascular events (Citation5–8). Good cardiorespiratory fitness (CRF) may predict the risk of acute myocardial infarction (AMI) by affecting modifiable risk factors including hypertension (Citation2), dyslipidemia (Citation3), and obesity (Citation4). It has been proposed that CRF, measured during exercise, has been shown to have a strong inverse relation to the risk of AMI (Citation9) and should be included when clinical decisions are being made in patients who are referred for evaluation of cardiovascular diseases (CVD) risk. Although CRF can be held as a predictive marker of cardiovascular capacity, it does not take into account the differences in cardiovascular resistance and cardiac afterload between the subjects. Our previous study has shown that systolic blood pressure (SBP) at rest is a risk factor for stroke (Citation10). In addition to resting SBP, exercise-induced elevation of SBP has been found to be an independent predictor of stroke (Citation10), hypertension (Citation7,Citation8), coronary heart disease (Citation9–12), cardiovascular disease (Citation13,Citation14), and sudden cardiac death (Citation15).
We hypothesized that an index of exercise cardiac power (ECP) defined as the ratio of directly measured maximal oxygen uptake (VO2max) with peak SBP gives prognostic information in coronary heart disease (CHD) and CVD mortality risk stratification. We, therefore, investigated the association of ECP by integrating surrogates of preload (VO2max) and afterload (SBP) during exercise with the risk of CHD and CVD mortality in a population-based sample of men from eastern Finland.
Methods
Subjects
Subjects were participants in the Kuopio Ischaemic Heart Disease Risk Factor Study (KIHD), designed to investigate risk factors for CVD, carotid atherosclerosis, and related outcomes in a population-based, randomly selected sample of men from eastern Finland (Citation16). Of the 3433 men aged 42, 48, 54, or 60 who resided in the city of Kuopio or its surrounding rural communities, 198 were excluded because of death, serious disease, or migration away from the area. At baseline, examinations were conducted on 2682 men (82.9% of the potential eligible) between March 1984 and December 1989. The KIHD study was approved by the Research Ethics Committee of the University of Kuopio, and each participant gave written informed consent. Complete data on ECP were available on 1798 subjects with no history coronary heart disease and cancer at baseline.
Assessment of exercise cardiac power
A maximal symptom-limited exercise tolerance test was performed between 8:00 a.m. and 10:00 a.m. using an electrically braked cycle ergometer (Citation1). The standardized testing protocol composed of an increase in the workload of 20 W/min with the direct analyses of respiratory gases (Medical Graphics, St. Paul, MN). The VO2max was defined as the highest value for or the plateau of oxygen uptake. The VO2max was also expressed in metabolic equivalents (METs). Maximal exercise workload was defined as the highest workload achieved during the exercise test. Exercise workload was also divided by body weight in kilograms. For safety reasons, all tests were supervised by an experienced physician with the assistance of an experienced nurse. The electrocardiogram (ECG), blood pressure, and heart rate were registered during the exercise test (Citation5,Citation6). Electrocardiography was recorded continuously with the Kone 620 electrocardiograph (Kone, Turku, Finland).
Assessment of other covariates
Resting blood pressure was obtained using a random-zero sphygmomanometer after 5 and 10 min of rest in the seated position. The mean of these two values was used as resting blood pressure. Body mass index (BMI) was computed as the ratio of weight in kilograms to the square of height in meters. Information on the use of medications and diagnosis of diseases was collected at baseline examination by an internist (Citation1). Alcohol consumption was assessed with the use of the Nordic Alcohol Consumption Inventory. The collection of blood specimens and the measurement of serum lipids and lipoproteins, insulin, and the definition of type 2 diabetes have been described elsewhere (Citation5,Citation6). Serum C-reactive protein (CRP) was measured with an immunometric assay (Immulite High Sensitivity C-reactive protein Assay, DPC, Los Angeles, CA).
Ascertainment of outcome events
Every resident of Finland has a unique personal identifier (PID) that is used in registers. Follow-up for cardiovascular outcomes was carried out using the PIDs. Therefore, there were no losses to follow-up. Deaths were ascertained by computer linkage to the National Death Registry utilizing the Finnish social security number that is used by all registries. All deaths occurring between study entry (March 1984–December 1989) and 31 December 2011 were included. Cardiovascular causes of deaths were coded according to the International Classification of Diseases, 9th Revision, codes 390–459, and International Classification of Diseases, 10th Revision, codes I00–I99.
Statistical analysis
Descriptive data are presented as means and percentages. Risk factors for main outcomes were analyzed with a multivariate Cox model. ECP was entered into forced SPSS Cox proportional hazards models. Cox models were adjusted for age and other demographic and clinical factors previously reported to be predictive of CHD and CVD death by considering their clinical relevance. Hazards ratios (HRs) with 95% confidence intervals (CIs), adjusted for clinical risk factors, were estimated as antilogarithms of the coefficients from multivariable models. The fit of the proportional hazards models was examined by plotting the hazard functions in different categories of risk factors over time. The proportional hazards assumption was verified for all variables by inspection of the plots of Schoenfeld residuals for covariates. The linearity assumption was satisfied for all continuous variables, and it was assessed with Martingale residuals for each continuous variable against survival time. A p value of <0.05 was considered statistically significant. These statistical analyses were performed with the use of SPSS 21.0 (SPSS Inc., Chicago, IL) for Windows. Exercise cardiac power was divided into quintiles. Different sets of covariates were used: Model (Citation1) age and examination year; (Citation2) Model 1 + the use of antihypertensive medication, smoking, alcohol consumption, BMI, type 2 diabetes, CRP and serum HDL, and LDL cholesterol. The cumulative survival from AMI according to the presence of ECP was calculated using the Kaplan–Meier method ().
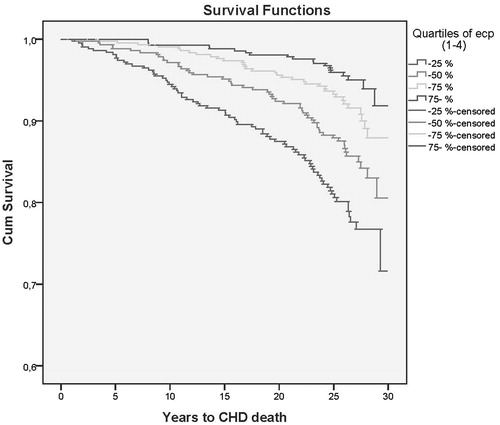
Figure 1. The age and examination adjusted survival curves of coronary heart disease mortality in men according to quarters of exercise cardiac power.
Results
Baseline characteristics
In the beginning of the follow-up, the mean age of the subjects was 52.2 years (range 42.0–61. 2 years). The mean ECP was 12.4 mL per mmHg (standard deviation (SD), 3.09 mL/mmHg, range 3.58–29.57 mL/mmHg). The mean follow-up time was 22.8 years (range 0.3–29.7 years). At baseline examination, men with low ECP were older, smoked more, and had higher serum LDL cholesterol, SBP, higher prevalence of diabetes, and were less physically active and consumed more alcohol as compared with those who had higher ECP ().
Table 1. Characteristics of men at baseline in the quarters of exercise cardiac power.
Risk predictors for coronary heart disease mortality
The strongest statistically significant risk factors for any CHD mortality were ECP (p < 0.001), BMI (p < 0.001), smoking (p < 0.001), and type 2 diabetes (p < 0.001) after adjustment for age and examination year. One SD increase in ECP (3.2 mL/mmHg) was associated with a decreased risk of CHD mortality by 40% (95% CI 51–30%).
Maximal cardiac power and risk for coronary heart disease mortality in men
ECP was associated to the risk of CHD mortality (). Men with low ECP (< 8.7 mL/mmHg, lowest quartile) had a 3.50-fold (95% CI 2.10–5.83, p < 0.001) risk of CHD mortality as compared with men with high ECP (>16.4 mL/mmHg, highest quartile) after adjusting for age and examination year. Low ECP was associated with a 2.80-fold risk of CHD mortality after additional adjustment for cigarette smoking, alcohol consumption, BMI, type 2 diabetes, CRP, serum LDL, and HDL-cholesterol (). Further adjustment for anti-hypertensive medication the results remained statistically significant (HR 2.76, 95% CI 1.64–4.65, p < 0.001). The multivariate adjusted cumulative Kaplan–Meier curves are shown in .
Table 2. The hazards ratio of coronary heart disease and cardiovascular deaths in the quartiles of exercise cardiac power in men at baselineTable Footnotea.
Exercise cardiac power, systolic blood pressure at rest and maximal oxygen uptake, and the risk of mortality
Among men with low ECP (<8.7 mL/mmHg) and the presence of elevated resting, SBP (≥132 mmHg, median) had a markedly increased risk of CHD mortality. Among men with low ECP and elevated resting, SBP was related to 2.5-fold (95% CI 1.45–4.44, p = 0.001) increased risk as compared with men with high ECP and low resting SBP.
Exercise cardiac power and risk of CVD mortality
One SD increase in ECP (3.2 mL/mmHg) was associated with a decreased risk of CHD mortality by 34% (95% CI 42–24%). Low ECP was also associated with an increased risk of CVD death. Men with low ECP had a 2.84-fold (95% CI 1.96–4.10, p < 0.001) risk of CVD death relative to those with high ECP after adjusting for age and examination years and with a 2.40-fold (95% CI 1.64–3.96, p < 0.001) risk of CVD death after further adjustment for the use of conventional risk factors. Further adjustment for anti-hypertensive medication among men with low ECP (<8.7 mL/mmHg) had increased risk of CVD death (HR 2.31, 95% CI 1.58–3.37, p < 0.001). The number of deaths per 1000 person years was 3.8 in the reference group (highest quartile) and 13.4/1000 person years in the lowest quartile, respectively.
Discussion
Exercise cardiac power, a novel marker of peak cardiac output during exercise, was associated with an increased risk of CHD and CVD mortality in a population-based study of men. The integration of afterload and preload with VO2max and peak SBP during exercise test, emphasising the role of ergospirometry in the risk prediction of CHD and CVD mortality, gives prognostic information in addition to that obtained by conventional methods.
To the best of our knowledge, this is the first population-based follow-up study showing an association between ECP and the risk for CHD and CVD death. This study shows that significant risk of mortality was observed among men with the lowest level of ECP. A continuous increase in ECP (3.2 mL/mmHg) corresponds to 34–40% decrease in the risk for mortality among these men. Our previous study showed that 1-MET increment in cardiorespiratory fitness reduced the risk of AMI by 22% (Citation9) and stroke risk by 17% (Citation15). On the basis of our studies, it seems that ECP may provide a more valuable tool for the risk prediction for mortality in high-risk subjects.
It has been suggested that VO2max is a non-invasive measure of cardiac output during physical stress and reflects cardiac preload whereas SBP is a mere indicator of afterload during exercise as cardiac output is dependent both on preload and on afterload. In subjects with elevated adrenergic tone and inappropriately constricted arterial bed, cardiac output can be lowered in the presence of disproportionately elevated SBP (i.e., afterload) (Citation17). Consequently, VO2max may be reduced considerably over the years and thus it may underestimate cardiac pumping capacity in subjects. Cardiac output is a non-invasive descriptor of cardiac function derived from preload, blood pressure, and cardiac output (Citation18) and ECP takes into consideration not only the preload but also afterload that potentially increases its value as a prognostic marker for CHD and CVD death.
It is probable that the incidence of CHD and CVD death can be reduced by a combination of several approaches and hence preventing its occurrence. VO2max may be preserved among subjects with medications lowering afterload despite the reduced pumping capacity. Anti-hypertensive medications may decrease the afterload and increase cardiac output to a higher level during progressive exercise. This was not the case in our study as we adjusted for anti-hypertensive medications. VO2max is determined by several physiological, environmental, and genetic factors such as age, sex, physical activity, and prevalent diseases. Cardiorespiratory fitness can be improved by increasing physical activity which ultimately confers long-term benefits on the cardiovascular system.
Our previous study has shown that low VO2max was associated with accelerated progression of carotid atherosclerosis (Citation1). The impairment of coronary blood flow and cardiac function during exercise may be caused by dynamic coronary artery stenosis as a result of vessel constriction, endothelial dysfunction, spasm, and thrombosis (Citation17–19). A high intraluminal pressure will lead to extensive change in endothelium and smooth muscle function in the arteries. In subjects with preclinical atherosclerotic changes and elevated SBP at rest or during exercise, the increased stress on the vessel wall can increase the risk of endothelial injury and permeability and result in local or multi-focal oedema (Citation16,Citation20). The damage to endothelium and change in blood cell–endothelium interaction can lead to local thrombi formation and ischemic lesions increasing the risk of CHD and CVD death. However, in our study, adjustment for known risk factors did not markedly change the association between ECP and risk for CHD and CVD death, although the adjustment for resting SBP somewhat slightly weakened the observed relationship between ECP and risk for mortality. This is consistent with the role of resting SBP as a documented risk factor for mortality (Citation21).
As ECP is a function of cardiac output (VO2max) and peripheral resistance (SBP), it may improve the predictive value of VO2max alone. Previous studies have suggested that low cardiorespiratory fitness is comparable with other conventional risk factors for CVD (Citation5,Citation14,Citation22,Citation23). Our findings suggest that it may be useful to assess the level of ECP although further studies are needed showing the exact value of ECP as a prognostic measure. The role of ECP can be considered as a modifiable risk factor by increasing cardiorespiratory fitness and a decrease in blood pressure will help in the prevention of mortality.
The strengths of this study are that we have a representative population-based sample of middle-aged men with a high participation rate. There were no losses during follow-up and reliable assessments of CHD and CVD deaths. Other strengths of our study include the definitive diagnosis of mortality. ECP remained as a risk factor, even after taking into account resting blood pressure and left ventricular hypertrophy in a multivariate model. A limitation of this study is that it is based on an ethnically homogenic and middle-aged male population that may limit the generalization of our results. Therefore, more studies are needed in different study populations including elderly and in women to confirm our findings.
This prospective population-based study provides the evidence that ECP is associated with an increased risk of CHD and CVD mortality. Exercise cardiac power during exercise may provide additional valuable information on risk staratification of mortality from CHD and CVD.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- Lakka TA, Laukkanen JA, Rauramaa R, Salonen R, Lakka HM, Kaplan GA, et al. Cardiorespiratory fitness and progression of carotid atherosclerosis in middle-aged men. Ann Intern Med. 2001;134:12–20.
- Fagard RH. Physical fitness and hypertension. J Hypertension Suppl. 1993;11:47–52.
- Stefanick ML, Mackey S, Sheehan M, Ellsworth N, Haskell WL, Wood PD. Effects of diet and exercise in men and postmenopausal women with low levels of HDL cholesterol and high levels of LDL cholesterol. N Engl J Med. 1998;339:12–20.
- Hill JO, Drougas HJ, Peters JC. Physical activity, fitness and moderate obesity. In: Bouchard C, Shepard RJ, Stephens T, eds. Physical activity, fitness and health campaign, 111, pp. 684–95. Champaign, Illinois: Human Kinetics Publishers, 1994.
- Laukkanen JA, Mäkikallio TH, Rauramaa R, Kiviniemi V, Ronkainen K, Kurl S. Cardiorespiratory fitness is related to the risk of sudden cardiac death: a population-based follow-up study. J Am Coll Cardiol. 2010;56:1476–83.
- Kurl S, Laukkanen JA, Rauramaa R, Lakka TA, Sivenius J, Salonen JT. Systolic blood pressure response to exercise stress test and risk of stroke. Stroke 2001;32:2036–41.
- Kannel WB, Wolf PA, McGee DL, Dawber TR, McNamara P, Castelli WP. Systolic blood pressure, arterial rigidity, and risk of stroke. The Framingham study. JAMA. 1981;245:1225–9.
- Singh JP, Larson MG, Manolio TA, O'Donnell CJ, Lauer M, Evans JC, et al. Blood pressure response during treadmill testing as a risk factor for new-onset hypertension. The Framingham Heart study. Circulation. 1999;99:1831–6.
- Lakka TA, Venäläinen JM, Rauramaa R, Salonen R, Tuomilehto J, Salonen JT. Relation of leisure-time physical activity and cardiorespiratory fitness to the risk of acute myocardial infarction. N Engl J Med. 1994;330:1549–54.
- Kurl S, Laukkanen JA, Niskanen L, Rauramaa R, Tuomainen TP, Sivenius J, et al. Cardiac power during exercise and the risk of stroke in men. Stroke. 2005;36:820–4.
- Laukkanen JA, Kurl S, Salonen R, Rauramaa R, Salonen J. The predictive value of cardiorespiratory fitness for cardiovascular events in men with various risk profiles: a prospective population-based cohort study. Eur Heart J. 2004;25:1428–37.
- Laukkanen JA, Kurl S, Rauramaa R, Lakka TA, Venäläinen JM, Salonen JT. Systolic blood pressure response to exercise testing is related to the risk of acute myocardial infarction in middle-aged men. Eur J Cardiovasc Prev Rehabil. 2006;13:421–8.
- McHam SA, Marwick TH, Pashkow FJ, Lauer MS. Delayed systolic blood pressure recovery after graded exercise: an independent correlate of angiographic coronary disease. J Am Coll Cardiol. 1999;34:754–9.
- Mundal R, Kjeldsen SE, Sandvik L, Erikssen G, Thaulow E, Erikssen J. Exercise blood pressure predicts mortality from myocardial infarction. Hypertension. 1996;27:324–9.
- Kurl S, Laukkanen J, Rauramaa R, Lakka TA, Sivenius J, Salonen JT. Cardiorespiratory fitness and the risk for stroke in men. Arch Intern Med. 2003;163:1682–8.
- Fagard RH. Exercise characteristics and the blood pressure response to dynamic physical training. Med Sci Sports Exerc. 2001;33:S484–S92.
- Zelis R, Flain SF. Alterations in vasomotor tone in congestive heart failure. Prog Cardiovasc Dis. 1982;24:437–59.
- Bain RJ, Tan LB, Murray RG, Davies MK, Littler WA. The correlation of cardiac power output to exercise capacity in chronic heart failure. WA Eur J Appl Physiol Occup Physiol. 1990;61:112–18.
- Saxon LA, Stevenson WG, Middlekauff HR, Fonarow G, Woo M, Moser D, et al. Predicting death from progressive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol. 1993;72:62–5.
- Palatini P. Exaggerated blood pressure response to exercise: pathophysiologic mechanisms and clinical relevance. J Sports Med Phys Fitness. 1998;38:1–9.
- Laukkanen JA, Jennings JR, Kauhanen J, Mäkikallio TH, Ronkainen K, Kurl S. Relation of systemic blood pressure to sudden cardiac death. Am J Cardiol. 2012;110:378–82.
- Laukkanen JA, Kurl S, Salonen JT. Cardiorespiratory fitness and physical activity as risk predictors of future atherosclerotic cardiovascular diseases. Curr Atheroscler Rep. 2002;4:468–76.
- Kurl S, Jae SY, Kauhanen J, Ronkainen K, Rauramaa R, Laukkanen JA. Exercise cardiac power and the risk of sudden cardiac death in a long-term prospective study. Int J Cardiol. 2015;181:155–9.