
Abstract
Background: Birth weight percentiles by gestational age are important for assessing prenatal growth and predicting postnatal outcomes of newborns. Several countries have developed nation-specific birth weight references for twins, but China still lacks such references.
Methods and results: Birth weight data for twins born between October 2006 and September 2015 were abstracted from the China National Population-based Birth Defects Surveillance System. A total of 54,786 live twin births aged ≥28 weeks of gestation without birth defects were included in the analysis. The LMS method was adopted to generate gestational age-specific birth weight percentiles and curves for male and female twins separately. Significant differences were observed between the current reference and other references developed for Chinese or non-Chinese twins. The neonatal mortality rate in this cohort was 12.3‰, and much higher rates at very early gestation weeks were identified in small-for-gestational-age twins grouped by the newly developed reference cutoffs.
Conclusions: The established birth weight centiles represent the first birth weight norm for contemporary Chinese twins and can be a useful tool to assess growth of twins in clinical and research settings.
There have been no population-based birth weight percentiles for Chinese twins prior to this study. The established birth weight centiles for female and male twins are markedly lower than those for Chinese singletons. Twin-specific curves should be used for determining inappropriate for gestational age in twins rather than using existing singleton reference.
The birth weight percentiles for twins differed significantly from those for non-Chinese twins. In addition to ethnic influences, the observed differences could be ascribed to variations in prenatal care, fetal or maternal nutrition status or other environmental factors.
Neonatal mortality rates varied considerably among twins grouped by the newly developed reference percentiles. Small-for-gestational-age twins had much higher mortality than did appropriate-for-gestational-age twins, highlighting the need to reduce postnatal mortality by improving perinatal health care for twins.
Key Messages
Introduction
Birth weight remains the most commonly used indicator of fetal growth (Citation1,Citation2). Newborns can be classified as small, appropriate, and large for gestational age according to their birth weights, birth lengths, and/or head circumference. A weight below the 10th percentile for the gestational age is usually defined as small, while weight above the 90th percentile is referred as large (Citation1). Both small and large for gestational ages are associated with an increased risk of perinatal and infant mortality and morbidity, and with some long-term problems (Citation3–5). Therefore, correct classification of birth weights by using right references is very important in both clinic and research works for a more accurate risk prediction and more effective postnatal health care (Citation1,Citation2).
Recently, a number of nation-specific birth weight percentiles for gestational age have been developed. Most of them are created for singletons, a few for twins. Twins’ intrauterine growth pattern diverges from singletons’ in the third trimester (Citation6–8), and varies across racial groups (Citation6,Citation9). Twin pregnancies are more prone to perinatal and infant mortality than singletons (Citation10–13), which can be mainly attributed to the high proportion of preterm delivery, low birth weight, small for gestational age, and intrauterine growth restriction (Citation6,Citation14). Increasing evidence has indicated the need of establishing the plurality-specific birth weight norm in the growth evaluation of newborns (Citation3,Citation8).
Twins account for 2–4% of all births worldwide and the number continues to increase in developed countries (Citation15) as well as in some developing countries including China (Citation16). Due to their contribution to postnatal adverse outcomes, twin pregnancies and related issues have attracted more attention recently. Several countries, including Australia (Citation17), Argentina (Citation18), Canada (Citation19), Finland (Citation8), German (Citation20), Japan (Citation21), Norway (Citation22), and United States of America (Citation7), have developed population-based twin-specific birth weight references in order to accurately evaluate twin growth. The population in China accounts for one-fifth of the world population (Citation23), but there were no birth weight references for Chinese twins. Using data from the National Population-based Birth Defects Surveillance System (Citation23,Citation24), we constructed a national reference of gestational age-specific birth weight percentiles for Chinese twins born between 2006 and 2015.
Methods and materials
The data on twin births between October 2006 and September 2015 were obtained from the nation-wide birth defects surveillance system that covers 64 counties and districts in 30 provinces or municipalities in mainland China (Citation23,Citation24). In each province, one county in rural area and one district in a city were chosen as surveillance sites except for in Sichuan province (two rural sites) and in Tianjin city (six urban districts). Since the surveillance system did not collect data on fetuses or infants less than 28 weeks of gestation, live births and stillbirths of at least 28 weeks gestation who were born to women living in the defined surveillance areas for one year or more were recruited and followed till 42 d after birth. Data collected by surveillance staff include demographic features, birth date, sex, gravidity, parity, gestational age, birth weight, outcomes, and the identified birth defects (major malformations and chromosomal aberrations diagnosed within 42 d after birth and coded according to the International Classification of Diseases 10th edition). This surveillance database represented a wide array of geographical locations and socioeconomic status. More details on data collection and quality control in the surveillance system were described previously (Citation23,Citation24).
The gestational age was calculated as the number of completed weeks from the first day of the last menstrual period to the day of birth. In the surveillance areas, women with suspected pregnancy had an ultrasound examination for confirmation in the first trimester according to obstetric clinical guidelines. For women with irregular menses and those who could not remember the last menstrual date, gestational ages were estimated based on sonography examination. The birth weight of each neonate was measured and recorded to the nearest 5 g by a trained midwife within 1 h after birth. All the information of maternal and infant characteristics was included in hospital delivery records and abstracted by surveillance staff using uniformed datasheet (Citation23,Citation24). From October 2006 to September 2015, a total of 28,670 pairs of twins (57,340 individuals) were identified among 2,981,630 newborns by the surveillance system, of which male–male, male–female, and female–female pairs accounted for 38.2% (10,949), 34.9% (10,018), and 26.9% (7703), respectively. Infants of foreign origin (n = 14), stillbirths (n = 773, 1.35‰), and infants affected by congenital anomalies (n = 1630, 2.84%, including100 stillbirths), were first excluded from the analysis. Among the rest of 55,023 records, 126 records (0.23%) were subsequently excluded due to missing gestational age or birth weight. Finally, Tukey’s methodology (Citation25) was adopted to screen implausible combinations of gestational age and birth weight in infants of ≤34 weeks gestation. Birth weights for each gestational age and sex combinations that were beyond the range of median ±2 × (interquartile range) were considered as outliers and were excluded. Meanwhile, the obviously erroneous records with gestational age above 34 weeks were eliminated by using pediatrician's professional judgment. Following this procedure, 111 records (0.20%, including 108 outliers and three errors) were removed from downstream analysis, yielding a final sample size of 54,786 for this study.
According to the geographical location of the surveillance sites, all the subjects were divided into three groups (costal, inner land, and remote areas). Infants born to women who lived in urban districts were classified into urban group, while newborns whose mothers lived in rural counties fell into rural group (Citation24). Univariate analysis was used to examine the birth weight distributions and to calculate the interquartile range for each gestational age and sex. Standard Chi-square test was adopted to compare differences in categorical variables between different groups, while linear Chi-square test was used to examine time trends in preterm births, low birth weight, and adverse outcomes. The LMS method, which adopts a Box–Cox transformation based semiparametric technique and solves penalized likelihood equation, was utilized to generate birth weight centiles (Citation26). The analysis was carried out by using R package VGAM (Citation27).
Results
shows the maternal and infant characteristics of the study subjects. The final sample for analysis included 51.5% male and 48.5% female births. Urban and rural births accounted for 54.5% and 45.5% of the cohort, respectively; while newborns whose mothers lived in coastal regions, inland, and remote areas accounted for 50.6%, 26.4%, and 23.1% of all births, respectively. The vast majority (92.8%) of the mothers were Han Chinese, and the rest (7.2%) were minorities. Most (87.1%) mothers aged 20–34 years at the time of delivery, with few (1.1%) aged ≤20 years and aged ≥35 years (11.8%). More than 70% of infants were born to primiparous women. Both maternal (age, ethnicity, parity, birth area, and geographic region) and infant (gestational age and sex) characteristics were associated with birth weight (Supplementary Table 1).
Table 1. Maternal and infant characteristics of live twin births in this study.
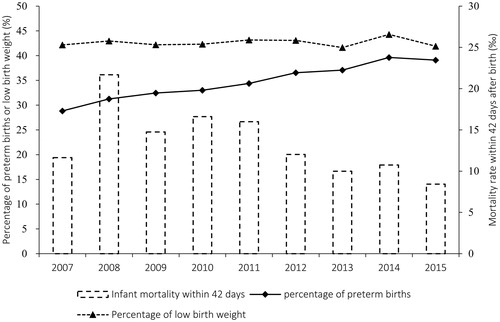
The overall percentage of low birth weight was 42.7%, and females tended to have a higher rate than males (46.9% versus 38.7%). Preterm births accounted for 35.5% of total twins. The annual preterm delivery rates varied between 28.8% and 39.7%, and presented an upward trend. About 1.3% of twins died within 42 days after birth, whereas the postnatal mortality rates declined from 21.7‰ in 2008 to 8.4‰ in 2015 ( and ).
Figure 1. Time trends in the rates of preterm births, low birth weight, and infant deaths within 42 d after birth during the study period (statistical year was defined as the period from the last October to this September).
By using LMS method, the smooth-estimated percentile values were generated for male and female twins, respectively ( and LMS parameters were presented in Supplementary Table 2) and smoothed growth curves for the 1st, 3rd, 5th, 10th, 25th, 50th, 75th, 90th, 95th, 97th, and 99th percentiles were constructed (). The corrected median birth weights for boys at 28–42 weeks were 1.1–6.0% heavier than for girls. The sex differences in the 10th and 90th percentiles varied between 1.2–6.7% and 0.9–6.1%, respectively. Greater sex differences were observed in the birth weight percentiles for preterm births. For example, the differences could be as great as 8.3%, 7.5%, 7.2%, and 6.7% in the 1st, 3rd, 5th, and 10th percentiles at very early gestations (less than 33 gestation weeks), respectively.
Figure 2. Percentile charts for Chinese newborn twins. P1, P3 to P99 denote the 1st, 3rd to 99th percentile curves, respectively.
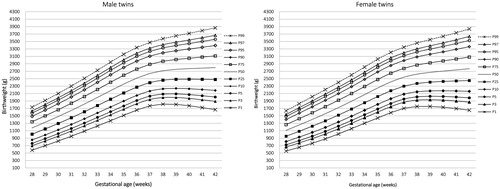
Table 2. Smoothed birth weight percentiles for Chinese twin boys and girls.
When comparing with the latest charts for Chinese singletons (Citation24), the current 10th and 50th percentiles for twins were significantly smaller at almost all gestational weeks except at very early gestations (). The differences in the 10th percentiles could be reached 36.9% and 32.6% for term males and females, respectively, while the differences in median birth weights for term infants varied between 14.3% and 26.1% ().
Table 3. Relative differences at 10th and 50th percentile between the current charts and previously published references.
There were significant differences between the current curves and previously published charts for twins. Moderate differences were found between ours and those based on samples from Taiwan (Citation28) and the United States of America (Citation7), whereas greater differences were observed as compared with Australian (Citation17), German (Citation20), and Japanese references (Citation21). Interestingly, the 10th percentile values for Australian preterm male twins were lower (Citation17), but such values for female twins were higher than current centile values at almost all gestation weeks except at 30 weeks of gestation. Taking our percentiles as reference, the degree of differences could be as great as 23.3% for 10th percentiles and 11.0% for medium birth weight ().
Finally, we analyzed the postnatal outcomes in twin groups categorized by current reference centiles. As shown in , the overall neonatal and postnatal mortality rates in the surveillance period (from birth to 42 d) were 12.3‰ and 12.9‰, nearly six-fold greater than the counterparts in non-malformed singleton cohorts (2.1‰ and 2.2‰) in the same areas. The neonatal and postnatal mortality rates of preterm twins (30.7‰ and 32.1‰) were considerably higher than those of term twins (2.2‰ and 2.4‰), but slightly lower than the rates of preterm singletons (33.9‰ and 34.8‰). Notably, the gestational-age specific mortality rates of very early preterm twins (<32 weeks gestation) were far greater than 100‰. Almost at all gestational weeks the mortality rates in small-for-gestational-age groups were higher than rates in large- and appropriate-for-gestational-age groups except for at 28 weeks’ gestation. The overall neonatal and postnatal mortality rates of small-for-gestational-age twins can be as high as 33.1‰ and 33.7‰, respectively ().
Table 4. Neonatal mortality and infant mortality within first 42 d of life by birth weight percentiles for gestational age.
Discussion
Population-based birth weight references by sex and gestational age are essential for prenatal growth evaluation, postnatal care, and the risk prediction of long-term outcomes. However, there were no published percentiles for twins in China. For the first time, we developed a population-based, gestational age-specific birth weight reference for Chinese twins based on a large and nationally representative database, which could be of great value in evaluating contemporary Chinese twins.
Due to the lack of appropriate reference tools, birth weight percentiles for singletons are commonly used in clinical practice in China (Citation29), which might cause a large portion of misclassification in twin birth weights. The current medium birth weight and 10th percentiles are smaller for term and moderate preterm births as compared to the newly updated Chinese singleton reference which is also based on data from the surveillance system (Citation24) (). From around 30 gestational weeks onwards, birth weight of both twin boys and girls diverged progressively from singletons in similar pattern as observed in previous studies (Citation6–8,Citation22). For instance, the relative differences in median weights at 30 weeks’ gestation between singletons and twins were 0.9% and 0.1% for male and female newborns, respectively. Notably, the corresponding differences in the 50th percentiles at 37 weeks’ gestation increased to 14.3% and 15.4% for males and females, respectively. The large divergences clearly indicate that twin-specific curves should be used for determining inappropriate for gestational age of twins rather than using existing singleton reference.
Consistent with previous studies, this research found that birth weight patterns of twins differed significantly among populations. The smoothed median birth weights for gestational age of Chinese term twins were smaller, but the median weights of preterm twins were larger than those counterparts in Argentina (Citation18), Japan (Citation21), Taiwan (Citation28), and the United States (Citation7). For twins born between 33 and 42 gestational weeks, the current median weights are markedly lighter than those of non-Asian twins such as Australian (Citation17), Canadian (Citation19), Finnish (Citation8), German (Citation20), and Norwegian (Citation22). Remarkably, the 10th percentiles at 33 gestation weeks onwards were consistently smaller than such references for Finnish and German twins (Citation8,Citation20), whereas the 10th centiles at gestation <37 weeks were larger than those for Argentinians (Citation18) and Japanese twins (Citation21), and for Australian twin boys (Citation17). These findings suggest that racial disparities are apparent in twins as in singletons although the underlying mechanisms are still unknown. In addition to ethnic influences, the observed differences in nation-specific percentiles could be associated with variations in perinatal care, maternal nutrition status, or other environmental factors. Smaller percentile values at very early gestations in developed countries might be correlated with a higher live birth rate for fetuses prone to be premature, which is usually attributed to better maternal nutrition status and improved prenatal health care. Similarly, improvements in perinatal care for preterm births might contribute to the downward trend in twin mortality in our study ().
It is well known that both environmental factors and genetic backgrounds contribute to birth weight patterns (Citation30,Citation31). In the current study, twin birth weight varied by socio-demographic, maternal, and infant characteristics. Twins in urban area or in coastal region who generally had better socioeconomic conditions were heavier than those in rural area, or in inner land and remote area. Older women tended to give birth to heavier babies than younger women, and twins born to primiparous women were lighter than those born to multiparous women. In our study, the difference of mean birth weight between maternal–parity groups was relatively smaller, 1.4% (38 g) and 1.1% (29 g) in boys and girls at 40 gestation weeks. There is still some controversy about whether maternal parity should be included in evaluating twin growth (Citation8). Only a few of studies constructed parity-specific birth weight percentiles for twins (Citation8,Citation20). Considering the small difference in observed mean birth weight and small sample size at some gestation weeks, we did not create percentile curves by maternal parity for each sex. Other factors like maternal cigarette smoking, obesity, and mode of delivery may affect birth weight distributions, but the effects on centiles cannot be assessed due to limited data.
Birth weight for gestational age not only reflects intrauterine growth but also correlates postnatal outcomes. The neonatal mortality rate in this study (12.3‰) was greater than the latest rates in general Chinese population (i.e. 5.9‰ in 2014) (Citation32) and in singleton cohort in the same areas (2.1‰). We identified an overall postnatal mortality rate of 33.7‰ for small-for-gestational-age twins (). Given the short-time period for surveillance (from 28 weeks of gestation to 42 d after birth), the actual infant mortality of small-for-gestational-age twins as well as of the whole twin population might be even higher. Although there was a substantial decline (61.1%) in the postnatal mortality during the study period (), the high mortality rates indicated an urgent need to improve the perinatal health care for twins, particularly for small and premature twins (). It is obvious that the newly established birth weight reference can provide more accurate risk prediction for early intervention for twins.
As ethnicity and other socio-demographic factors correlate with birth weight distributions, researchers have suggested that the birth weight references should be updated every 5–10 years (Citation28). In the past three decades in China, marked changes have occurred in socioeconomic, maternal, and infant characteristics along with the fast economic development, such as increased family income, improved education level of the parents, increments in infant weight and length, as well as improvements in prenatal nutritional status (Citation33,Citation34). In this study, the use of a large, nationally representative population-based sample of twins ensures a more representative and accurate estimate of percentiles. The ethnic and urban–rural distributions are in proportion to those from the National Census 2010 (http://www.stats.gov.cn/tjgb/rkpcgb/). The minorities and urban births accounted for 7.2% and 54.5%, respectively, highly comparable with 8.5% and 49.7% in the Census 2010. Although the male–male, male–female, and female–female twin pairs distribute unequally in our cohort, the sample size is large enough to generate sex-specific percentiles. Based on the experience in previous studies (Citation22,Citation35), we used Tukey’s methodology to screen outliers at 28–34 weeks of gestation, and removed erroneous measurements at 35–42 weeks by clinical judge. The careful exclusion of subjects with missing key variables or outlier values also reduces errors in the estimated percentiles.
Our study has several limitations. First, discrepancies in birth weight measurement could influence the accuracy of percentiles, whereas the effects were likely minimal due to systemically trained professionals in surveillance sites. Second, we could not develop percentiles for newborns below 28 weeks of gestational age, nor adjust reference centiles for maternal cigarette smoking, obesity, diabetes, in vitro fertilization treatment, and caesarean delivery, because these data were not collected. Third, birth weight alone is insufficient for a complete evaluation of fetal and neonatal growth, we were not able to create birth length and head circumference reference charts for twins due to limits of data. Future studies are warranted to develop references for other anthropometric measurements for Chinese twins as well as for singletons.
In summary, our newly developed gestational age-specific birth weight percentiles for Chinese twins are based on up-to-date data from the largest national registry. They can provide clinicians and researchers with a valuable reference of identifying high-risk twins in China.
B20170104-Supplementary_Tables.docx
Download MS Word (17.1 KB)Acknowledgements
The authors thank the obstetricians, pediatricians, and other staff members involved in data collection. The opinions expressed in this manuscript are the views of the authors. They do not reflect the official position of the National Center for Birth Defects Monitoring, P.R. China.
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Additional information
Funding
Related Research Data
Reference
- Wilcox AJ. On the importance-and the unimportance-of birthweight. Int J Epidemiol. 2001;30:1233–41.
- Resnik R. One size does not fit all. Am J Obstet Gynecol. 2007;197:221–2.
- Joseph KS, Fahey J, Platt RW, Liston RM, Lee SK, Sauve R, et al. An outcome-based approach for the creation of fetal growth standards: do singletons and twins need separate standards? Am J Epidemiol. 2009;169:616–24.
- Curhan GC, Willett WC, Rimm EB, Spiegelman D, Ascherio AL, Stampfer MJ. Birth weight and adult hypertension, diabetes mellitus, and obesity in US men. Circulation 1996;94:3246–50.
- Boney CM, Verma A, Tucker R, Vohr BR. Metabolic syndrome in childhood: association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 2005;115:e290–6.
- Alexander GR, Kogan M, Martin J, Papiernik E. What are the fetal growth patterns of singletons, twins, and triplets in the United States? Clin Obstet Gynecol. 1998;41:114–25.
- Min SJ, Luke B, Gillespie B, Min L, Newman RB, Mauldin JG, et al. Birth weight references for twins. Am J Obstet Gynecol. 2000;182:1250–7.
- Sankilampi U, Hannila ML, Saari A, Gissler M, Dunkel L. New population-based references for birth weight, length, and head circumference in singletons and twins from 23 to 43 gestation weeks. Ann Med. 2013;45:446–54.
- Hur YM, Luciano M, Martin NG, Boomsma DI, Iacono WG, McGue M, et al. A comparison of twin birthweight data from Australia, the Netherlands, the United States, Japan, and South Korea: are genetic and environmental variations in birthweight similar in Caucasians and East Asians? Twin Res Hum Genet. 2005;8:638–48.
- Kiely JL. The epidemiology of perinatal mortality in multiple births. Bull N Y Acad Med. 1990;66:618–37.
- Luke B, Keith LG. The contribution of singletons, twins and triplets to low birth weight, infant mortality and handicap in the United States. J Reprod Med. 1992;37:661–6.
- Imaizumi Y. Perinatal mortality in single and multiple births in Japan, 1980–1991. Paediatr Perinat Epidemiol. 1994;8:205–15.
- Powers WF, Kiely JL. The risks confronting twins: a national perspective. Am J Obstet Gynecol. 1994;170:456–61.
- Tobe RG, Mori R, Shinozuka N, Kubo T, Itabashi K. A nationwide investigation on gestational age specific birthweight and mortality among Japanese twins. Paediatr Perinat Epidemiol. 2011;25:228–35.
- Ananth CV, Chauhan SP. Epidemiology of twinning in developed countries. Semin Perinatol. 2012;36:156–61.
- Cui L, Zhou X, Cui Y, Guo H. Twinning rates in Zhengzhou during the period of 1996 to 2005. Chinese Rural Health Service Admin 2007;27:142–3.
- Li Z, Umstad MP, Hilder L, Xu F, Sullivan EA. Australian national birthweight percentiles by sex and gestational age for twins, 2001–2010. BMC Pediatr. 2015;15:148.
- Urquia ML, Alazraqui M, Spinelli HG, Frank JW. Reference birthweights for the Argentine population by multiplicity of birth, sex, and gestational age. Rev Panam Salud Publica 2012;29:108–19.
- Arbuckle TE, Wilkins R, Sherman GJ. Birth weight percentiles by gestational age in Canada. Obstet Gynecol. 1993;81:39–48.
- Voigt M, Rochow N, Schneider KT, Hagenah HP, Straube S, Scholz R, et al. New percentile values for the anthropometric dimensions of twin neonates: analysis of perinatal survey data of 2007–2011 from all 16 states of Germany. Z Geburtshilfe Neonatol. 2014;218:254–60.
- Ooki S, Yokoyama Y. Reference birth weight, length, chest circumference, and head circumference by gestational age in Japanese twins. J Epidemiol. 2003;13:333–41.
- Glinianaia SV, Skjaerven R, Magnus P. Birthweight percentiles by gestational age in multiple births. A population-based study of Norwegian twins and triplets. Acta Obstet Gynecol Scand. 2000;79:450–8.
- Dai L, Zhu J, Liang J, Wang YP, Wang H, Mao M. Birth defects surveillance in China. World J Pediatr. 2011;7:302–10.
- Dai L, Deng C, Li Y, Zhu J, Mu Y, Deng Y, et al. Birth weight reference percentiles for Chinese. PLoS One 2014;9:e104779.
- Tukey JW. Exploratory data analysis. Don Mills, Ontario: Addison-Wesley, 1977.
- Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. 1992;11:1305–19.
- Yee TW. The VGAM package. R News 2008;8:28–39.
- Hu IJ, Hsieh CJ, Jeng SF, Wu HC, Chen CY, Chou HC, et al. Nationwide twin birth weight percentiles by gestational age in Taiwan. Pediatr Neonatol. 2015;56:294–300.
- Zhang J, Mikolajczyk R, Lei X, Sun L, Yu H, Cheng W. An adjustable fetal weight standard for twins: a statistical modeling study. BMC Med. 2015;13:159.
- Bakketeig LS. Current growth standards, definitions, diagnosis and classification of fetal growth retardation. Eur J Clin Nutr. 1998;52:S1–S4.
- Kramer MS. Socioeconomic determinants of intrauterine growth retardation. Eur J Clin Nutr. 1998;52:S29–S32. Discussion S-3.
- National Health and Family Planning Commission of the People's Republic of China. China health and family planning yearbook (2015). Beijing: Peking Union Medical College Press, 2015.
- Zheng X, Pang L, Tellier S, Tan L, Zhang L, Hu Y, et al. The changing patterns of abortion among married women in China, 1984–2005. Eur J Obstet Gynecol Reprod Biol. 2013;166:70–5.
- Li H, Zhu Z, Zhang D. A national survey on growth of children under 7 years of age in nine cities of China, 2005. Zhonghua Er Ke Za Zhi. 2007;45:609–14.
- Skjaerven R, Gjessing HK, Bakketeig LS. Birthweight by gestational age in Norway. Acta Obstet Gynecol Scand. 2000;79:440–9.