
Abstract
Background
Clinical practice guidelines emphasize the importance of the prevention and treatment of non-specific back pain through exercise therapy and health education. However, it has not yet been confirmed that the combination of exercise plus education is more effective than usual medical care.
Objective
The aim of this study was to determine if the combination of exercise plus education is more effective for the prevention of non-specific back pain than usual medical care.
Materials and methods
A systematic search in PubMed, Scopus, Web of Science and Medline was conducted with the terms Back Pain, Neck Pain, Musculoskeletal Pain, Exercise, Exercise Therapy, Health Education, Cognitive Behavioral Therapy, Primary Prevention, Secondary Prevention and Clinical Trial. The inclusion criteria were: articles published from 2016 to 2021, the intervention included exercise and education, and the sample consisted of non-specific back pain patients.
Results
A total of 4 randomized controlled trials were selected (average PEDro score 6.5 points). The meta-analysis showed statistically significant differences in the pain intensity, standardized mean differences was found to be −0.75 (95% CI = −1.41 to −0.08; p = 0.03); and in disability, standardized mean differences was found to be −0.24 (95% CI = −0.38 to −0.1; p = 0.001).
Conclusions
Interventions combining exercise and education seem to have a greater preventive effect on non-specific back pain than usual medical care.
Exercise therapy and health education combination prevent better non-specific back pain than usual care.
Combining exercise with educational interventions has a higher improvement on disability and kinesophobia than usual care.
Key messages
Introduction
Back pain is a global problem and is a leading contributor to the increasing prevalence of disability over the past 30 years [Citation1]. The most common spinal disorder is non-specific back pain (NBP), as it cannot be attributed to a specific underlying disease such as cancer, infection, ankylosing spondylitis, or other inflammatory or infectious diseases [Citation2]. The prevalence of NBP worldwide is 14%, and it is increasing regardless of age, sex, ethnicity, socioeconomic status and geographic region [Citation3]. Specifically, non-specific low back pain is the second leading cause of medical care demand in developed countries, the third leading cause of surgery and functional disability and the fifth leading cause of hospitalization [Citation4,Citation5].
To avoid these serious socioeconomic problems, it is essential to prevent its progression and limiting consequences, such as loss of functionality or work capacity [Citation6,Citation7].
It is essential to know the risk factors associated with NBP in order to prevent it, with the aim of reducing the serious socioeconomic repercussions caused by NBP [Citation8]. This condition presents a multifactorial approach: sedentary lifestyle [Citation9], obesity [Citation10], lack of muscle strength [Citation11,Citation12], lack of flexibility [Citation13] and psychosocial [Citation14,Citation15] and work-related factors [Citation16,Citation17].
This complicates an accurate diagnosis, the definition of a prognosis and the design of effective interventions that reduce the use of invasive methods (surgical and opioid-based pharmacological interventions) [Citation18–20]. Clinical practice guidelines emphasize the importance of the prevention and treatment of NBP through exercise therapy (ET) (i.e. strengthening and stretching exercises and yoga) and health education (HE) (i.e. ergonomics, self-management techniques, pain neuroscience education and stress reduction techniques) [Citation2,Citation21–23].
Several systematic reviews have examined the benefits of ET in preventing pain, disability, loss of quality of life and kinesophobia related to non-specific low back [Citation24–27] and cervical pain [Citation28–33] and that ET is cost-effective versus usual medical care (UC) in the subacute and chronic treatment of NBP [Citation34]. Regarding HE, a meta-analysis published in 2021 concluded that counselling provides improvements in pain and disability, although the effects may be insufficient as monotherapy for patients with NBP [Citation35]. Moreover, no recent systematic reviews have attempted to determine whether the combination of ET plus HE is more effective for the prevention of NBP than UC. Therefore, the primary objective of the present systematic review and meta-analysis was to determine whether the combination of ET and HE is more effective than UC for the prevention of NBP. In addition, as secondary objectives, the effects on other related variables such as disability and kinesophobia were investigated.
Materials and methods
Data sources and searches
This study was prospectively registered on PROSPERO (ID: CRD42022311026) and followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) [Citation36] reporting guidelines in Exercise, Rehabilitation, Sport medicine and Sports (PERSIST) [Citation37] and the recommendations from the Cochrane Collaboration [Citation38]. The PICOS question was then chosen as follows: P – population (participants with NBP); I – intervention (ET plus HE); C – control (UC); O – outcome (characteristics of pain, disability and kinesophobia); S – study design (randomized controlled trial).
A systematic search of publications was conducted in December 2021 in the following databases: PubMed, Scopus, Web of Science and Medline. The search strategy included different combinations with the following Medical Subject Headings (MeSH) terms: Back Pain, Neck Pain, Musculoskeletal Pain, Exercise, Exercise Therapy, Health Education, Cognitive Behavioral Therapy, Primary Prevention, Secondary Prevention and Clinical Trial. The following word was used as a free term: Prevention. The search strategy according to the focused PICOS question is presented in .
Table 1. Search strategy according to the focused question (PICO).
Study selection
After removing duplicates, two reviewers (P.H.-L) and (J. L.-B.) independently screened articles for eligibility. In case of disagreement, both reviewers debated until an agreement was reached. The following inclusion criteria were applied for the selection of studies: (i) published in the last five years; (ii) ET plus HE was administered to the study sample; (iii) the sample consisted of participants with NBP; (iii) the research included a group that received UC, with neither exercise nor education. On the other hand, studies with the following characteristics were excluded from this review: (i) no quasi-experimental and observational studies; (ii) participants with specific causes of back pain; (iii) pregnant women; (iv) full text not available.
After screening the data, extracting, obtaining, and screening the titles and abstracts for inclusion criteria, the selected articles were obtained in full texts. Articles with titles and abstracts lacking sufficient information regarding the inclusion criteria were also obtained in full text. Full text articles were selected in case of compliance with inclusion criteria by the two reviewers using a data extraction form.
Data extraction and quality assessment
The two reviewers independently extracted data from the included studies using a customized data extraction table developed in Microsoft Excel. In case of disagreement, both reviewers debated until an agreement was reached.
The following data from the included articles were selected for further analysis: demographic information (title, authors, journal, and year), characteristics of the sample (age, gender, inclusion and exclusion criteria, and number of participants), study-specific parameters (duration of the intervention, adverse events, methods of ET and HE) and results obtained (variables analyzed, instruments used and time of follow-up). Tables were used to describe both the studies’ characteristics and the extracted data.
The Jadad scale and PEDRO scale were used to assess the quality of the studies.
Data synthesis and analysis
Tables were used to describe both the studies’ characteristics and the extracted data. When possible, the results were gathered based on type of intervention applied.
Standardized mean differences (SMD) and their 95% confidence interval (CI) were calculated as the between-group difference in means divided by the pooled standard deviation (SD) [Citation39]. SMDs were interpreted using the following cut-off values: 0–0.2 (very small); 0.2–0.5 (small); 0.5–0.8 (moderate); and >0.8 (large) [Citation40]. The same increments were used for negative values. The significance level was set to p < 0.05. The I2 statistic was used to determine the degree of heterogeneity, where the percentages quantified the magnitude of heterogeneity: 25% = low; 50% = medium; and 75% = high heterogeneity [Citation41]. The analyses were performed with Comprehensive Meta-Analysis (CMA) V2 software (Biostat, NJ, USA).
Results
Study selection
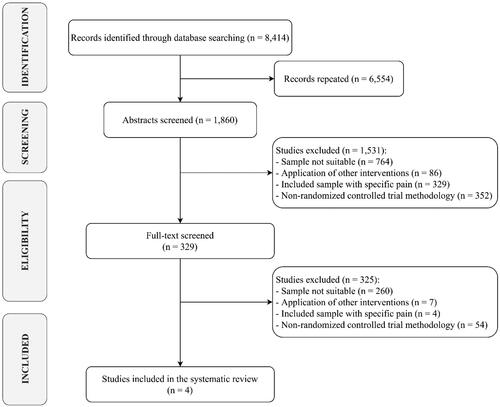
Out of 8414 search results, 1832 studies were considered eligible for inclusion after removing duplicates. Among the 1860 papers screened, 1531 were excluded after abstract and title screening. After the first reading of all candidate full texts, the Kappa score of reviewers 1 and 2 was 0.85 (i.e. almost perfect) [Citation42]. All four full-text articles assessed for eligibility were finally included in the synthesis, as depicted by the PRISMA flowchart in .
Figure 1. PRISMA flow diagram.
Samples and risk of bias of included studies
The methodological quality of the studies was five or more points on the PEDRO scale and the average score was 6.5 points (). According to the PEDRO scale, the studies have a good methodological quality [Citation43]. At the same time, on the JADAD scale, two works [Citation44,Citation45] were rated with tree points and the other two works [Citation46,Citation47] received four points. The most common methodological shortcoming was the absence of blinding [Citation44,Citation45] ().
Table 2. Risk of bias assessment using the Physiotherapy Evidence Database (PEDro) scale.
Table 3. Baseline characteristic of patients and Jadad scale risk of bias.
Baseline characteristic of patients
A total of 1,235 patients took part in the included studies [Citation44–47] (65.9% of whom are women). The mean age of the participants was 46 years. For more details, see . The participants only experienced adverse effects in one study [Citation46], and these were discomfort, pain, or harm caused by the intervention. In two articles [Citation44,Citation45], the authors do not refer to the adverse effect.
Interventions applied
The average number of sessions was 12, with 60–120 min being the most common range of session time [Citation44–46]. Antúnez et al. [Citation45] completed five sessions per week, while other two studies [Citation44,Citation46] attended one session per week. Sandal et al. [Citation47] did not report the duration and number of sessions per week.
The ET performed in the four selected studies were yoga [Citation44,Citation46] and strengthening and stretching exercises [Citation45,Citation47]. On the other hand, the HE was focused on ergonomics [Citation45], pain neuroscience education [Citation47], and mindfulness and stress reduction techniques [Citation44,Citation46]. These interventions were supervised by physiotherapists [Citation45], physicians [Citation47] and psychologists [Citation44,Citation46] ().
Table 4. Characteristics of the included trials.
Meta-analysis results
Four studies included in this systematic review analyzed the pain variable, with a total sample size of 1,235 participants [Citation44–47]. Three studies [Citation45–47] were included in the meta-analysis. (p < 0.001, I2 = 93.6%). SMD effect size was found to be −0.75 (p = 0.03), with a variance of 0.115 (95% CI = −1.41 to −0.08). The forest plot is shown in .
Figure 2. Forest plots of meta-analysis results. (A) Meta-analysis results for PAIN; (B) Meta-analysis results for DISABILITY. ET: Exercise Therapy; HE: Health Education; UC: Usual Medical Care.
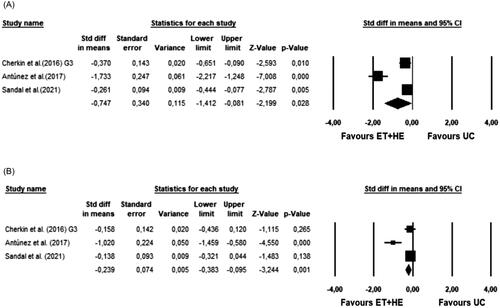
Three articles [Citation36–38] with a total sample of 751 participants analysed the variable disability. All three studies were included in the meta-analysis (). The Q-test established heterogeneity across the studies and was high (p = 0.001, I2 = 85.3%). SMD effect size was found to be −0.24 (p = 0.001), with a variance of 0.005 (95% CI = −0.38 to −0.1).
Turner et al. [Citation44] research is the only one that indirectly assesses kinesophobia. With a sample of 342 participants, they analyzed this variable. A significant post-intervention improvement was observed (p < 0.01), with a mean difference between groups of −3.3 and (95% CI −5.11 to −1.5).
Discussion
The aim of this study was to determine whether the combination of ET and HE is more effective for the prevention of NBP than UC. The results suggest that there is a positive effect of combining ET and HE in the prevention of NBP. In addition, improvements were observed in other variables, such as disability and kinesophobia.
In the studies analyzed [Citation45–47], the combination of ET plus HE obtained significant improvements on NBP compared to UC. Although it should be mentioned that the effect found in the meta-analysis is moderate. Different reviews confirm the benefits of exercise in non-specific low back pain [Citation24–27] and in non-specific cervical pain [Citation28–30,Citation33]. In addition, two of these reviews compare the effect of ET versus UC [Citation24,Citation25], including several articles in which yoga is used, as in two of the studies [Citation44,Citation46] included in this review, or strengthening and flexibility exercises, as also occurs in these works [Citation45,Citation47].
In addition, Miyamoto et al. [Citation34] conclude that exercise is cost efficient versus UC in the subacute and chronic treatment of non-specific low back pain. The results seem to indicate that theoretical-practical interventions have better results in the prevention of NBP than totally passive interventions included within UC [Citation45–Citation47], suggesting that exercise is cost efficient versus UC in the subacute and chronic treatment of low back NBP. This effect could be due to the multifactorial origin of NBP: some risk factors for NBP have a biophysical origin, such as a lack of strength or flexibility of the spinal musculature [Citation12,Citation48]. Other risk factors have a psychological origin, such as fear or stress, or even social factors such as false beliefs about NBP or work-related factors [Citation17,Citation49]. Therefore, the latest clinical guidelines on acute and chronic low back pain highlight exercise and education as key elements in clinical interventions [Citation22].
The disability variable also showed a positive result in the meta-analysis [Citation45–47]. These results are coherent, since disability is strongly related to pain, due to the close relationship between the physical and psychosocial components [Citation50]. In the same line, two reviews conclude that ET produces an improvement in function in the lumbar [Citation26] and cervical regions [Citation28]. Kinesiophobia and catastrophism are two prognostic factors of clinical results in low back pain that are associated with disability [Citation51]. Other authors have also found significant relationships between catastrophizing and the anxiety reaction to pain [Citation52], as well as with the perception of pain intensity [Citation53]. Turner et al. [Citation44] observed that the combination of ET and HE is more effective than UC in reducing catastrophizing, and they also observed improvements in Pain Self-Efficacy. The International Association for the Study of Pain also establishes a relationship between fear-pain-knowledge, as they state that pain represents not only the sensation of physical harm, but also an emotional experience that can be influenced by other emotions, such as anxiety or fear of the unknown [Citation54]. For all these reasons, the biopsychosocial approach is the current paradigm in the treatment and prevention of NBP [Citation55].
Currently, there are reviews that analyse the effects of exercise applied in isolation in which a larger number of articles are analysed [Citation25,Citation33]. However, the novel objective of this review makes the inclusion of articles more demanding since only those interventions that combine HE and ET were included. Despite this, all the articles included in this review are randomized controlled trials with a high methodological quality and with a large number of participants overall. This makes it possible to draw a first conclusion while awaiting new studies that provide greater strength to this novel meta-analysis.
Limitations
Among the limitations of the present investigation, the authors must acknowledge that they have not taken into account differentiated analyses by gender and age subgroups, nor have they included studies comparing the combination of ET and HE with UC in pregnant women. It is worth mentioning that, due to the high heterogeneity in the analyzed studies, it was not possible to establish which ET and HE interventions are the most effective, as well as the most appropriate frequency and duration of sessions. However, this is the first meta-analysis that analyzes the effects of the combination of exercise therapy, and HE compared to usual medical care in the prevention of LBP. In view of the above, further research is needed to compare the effects of different interventions with the aim of developing specific protocols for NBP prevention.
Conclusions
Interventions combining ET and HE seem to have a greater preventive effect on NBP than UC. In addition, combining exercise with educational interventions has a higher improvement on disability and kinesophobia than UC.
The obtained results may help healthcare professionals to increase the effectiveness of their clinical interventions and thus reduce the severe socioeconomic impact caused by NBP worldwide.
Author contributions
P. H.-L., R. L.-R., J. L.-B., J. L. G.-S. conceptualized and designed the study, drafted the initial manuscript, designed the data collection instruments, collected data, carried out the initial analyses, and critically reviewed the manuscript for important intellectual content. All authors have read and agreed to the published version of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The dataset used and analyzed during the current study are available from the corresponding author.
References
- James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858.
- Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8–20.
- Wu A, March L, Zheng X, et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the global burden of disease study 2017. Ann Transl Med. 2020;8(6):299.
- Gómez-Conesa A, Valbuena S. Lumbalgia crónica y discapacidad laboral [chronic low back pain and disability at work. ]. Fisioterapia. 2005;27(5):255–265.
- Borenstein DG. Epidemiology, etiology, diagnostic evaluation, and treatment of low back pain. Curr Opin Rheumatol. 2001;13(2):128–134.
- Bartys S, Frederiksen P, Bendix T, et al. System influences on work disability due to low back pain: an international evidence synthesis. Health Policy. 2017;121(8):903–912.
- Foster NE, Anema JR, Cherkin D, Lancet Low Back Pain Series Working Group, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383.
- Cholewicki J, Pathak P, Reeves NP, et al. Simulation of multifactorial causes of low back pain. Spine J. 2016;16(10):277.
- Sitthipornvorakul E, Janwantanakul P, Lohsoonthorn V. The effect of daily walking steps on preventing neck and low back pain in sedentary workers: a 1-year prospective cohort study. Eur Spine J. 2015;24(3):417–424.
- Smuck M, Kao MCJ, Brar N, et al. Does physical activity influence the relationship between low back pain and obesity? Spine J. 2014;14(2):209–216.
- Lindstrøm R, Schomacher J, Farina D, et al. Association between neck muscle coactivation, pain, and strength in women with neck pain. Man Ther. 2011;16(1):80–86.
- Behennah J, Conway R, Fisher J, et al. The relationship between balance performance, lumbar extension strength, trunk extension endurance, and pain in participants with chronic low back pain, and those without. Clin Biomech (Bristol, Avon). 2018;53:22–30.
- Mistry GS, Vyas NJ, Sheth MS. Comparison of hamstrings flexibility in subjects with chronic low back pain versus normal individuals. J Clin Exp Res. 2014;2(1):85.
- Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148–1156.
- Ortego G, Villafañe JH, Doménech-García V, et al. Is there a relationship between psychological stress or anxiety and chronic nonspecific neck-arm pain in adults? A systematic review and meta-analysis. J Psychosom Res. 2016;90:70–81.
- Mork R, Falkenberg HK, Fostervold KI, et al. Discomfort glare and psychological stress during computer work: subjective responses and associations between neck pain and trapezius muscle blood flow. Int Arch Occup Environ Health. 2020;93(1):29–42.
- Shiri R, Falah‐Hassani K, Heliövaara M, et al. Risk factors for low back pain: a population‐based longitudinal study. Arthritis Care Res (Hoboken). 2019;71(2):290–299.
- Chou R, Qaseem A, Snow V, American Pain Society Low Back Pain Guidelines Panel, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American college of physicians and the American pain society. Ann Intern Med. 2007;147(7):478–491.
- George SZ, Lentz TA, Beneciuk JM, et al. Framework for improving outcome prediction for acute to chronic low back pain transitions. Pain Rep. 2020;5(2):e809.
- Manogharan S, Kongsted A, Ferreira M, et al. Do older adults with chronic low back pain differ from younger adults in regards to baseline characteristics and prognosis? Eur J Pain. 2017;21(5):866–873.
- Hurwitz EL, Randhawa K, Yu H, et al. The global spine care initiative: a summary of the global burden of low back and neck pain studies. Eur Spine J. 2018;27(Suppl 6):796–801.
- George SZ, Fritz JM, Silfies SP, et al. Interventions for the management of acute and chronic low back pain: Revision 2021: Clinical practice guidelines linked to the international classification of functioning, disability and health from the academy of orthopaedic physical therapy of the American physical therapy association. J Orthop Sports Phys Ther. 2021;51(11):CPG1–CPG60.
- Corp N, Mansell G, Stynes S, et al. Evidence‐based treatment recommendations for neck and low back pain across Europe: a systematic review of guidelines. Eur J Pain. 2021;25(2):275–295.
- Hayden JA, Wilson MN, Stewart S, Chronic Low Back Pain IPD Meta-Analysis Group, et al. Exercise treatment effect modifiers in persistent low back pain: an individual participant data meta-analysis of 3514 participants from 27 randomised controlled trials. Br J Sports Med. 2020;54(21):1277–1278.
- Hayden JA, Ellis J, Ogilvie R, et al. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev. 2021;9(9) CD009790.
- Frizziero A, Pellizzon G, Vittadini F, et al. Efficacy of core stability in non-specific chronic low back pain. JFMK. 2021;6(2):37.
- Domingues C, Costa DA, Junior NC, et al. Effects of the pilates method on kinesiophobia associated with chronic non-specific low back pain: Systematic review and meta-analysis. J Bodyw Mov Ther. 2020;24(3):300–306.
- O'Riordan C, Clifford A, Van De Ven P, et al. Chronic neck pain and exercise interventions: Frequency, intensity, time, and type principle. Arch Phys Med Rehabil. 2014;95(4):770–783.
- Arimi SA, Bandpei MAM, Javanshir K, et al. The effect of different exercise programs on size and function of deep cervical flexor muscles in patients with chronic nonspecific neck pain: a systematic review of randomized controlled trials. Am J Phys Med Rehabil. 2017;96(8):582–588.
- Sihawong R, Janwantanakul P, Sitthipornvorakul E, et al. Exercise therapy for office workers with nonspecific neck pain: a systematic review. J Manipulative Physiol Ther. 2011;34(1):62–71.
- Cheng CH, Su HT, Yen LW, et al. Long-term effects of therapeutic exercise on nonspecific chronic neck pain: a literature review. J Phys Ther Sci. 2015;27(4):1271–1276.
- Kay TM, Gross A, Goldsmith CH, et al. Exercises for mechanical neck disorders. Cochrane Database Syst Rev. 2012;8.
- Gross A, Paquin JP, Dupont G, Cervical Overview Group, et al. Exercises for mechanical neck disorders: a cochrane review update. Man Ther. 2016;24:25–45.
- Miyamoto GC, Lin CWC, Cabral CMN, et al. Cost-effectiveness of exercise therapy in the treatment of non-specific neck pain and low back pain: a systematic review with meta-analysis. Br J Sports Med. 2019;53(3):172–181.
- Jones CM, Shaheed CA, Ferreira GE, et al. Advice and education provide small short-term improvements in pain and disability in people with non-specific spinal pain: a systematic review. J Physiother. 2021;67(4):263–270.
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
- Ardern CL, Büttner F, Andrade R, et al. Implementing the 27 PRISMA 2020 statement items for systematic reviews in the sport and exercise medicine, musculoskeletal rehabilitation and sports science fields: the PERSiST (implementing prisma in exercise, rehabilitation, sport medicine and SporTs science) guidance. Br J Sports Med. 2022;56(4):175–195.
- Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. 2019. 10:ED000142.
- Higgins JP, Thomas J, Chandler J, et al. Handbook for systematic reviews of interventions version 6.2. Chichester: Cochrane; 2021. www.training.cochrane.org/handbook
- Ferguson CJ. An effect size primer: a guide for clinicians and researchers. Prof Psychol Res Pract. 2009;40(5):532–538.
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558.
- Cicchetti DV. Assessing inter-rater reliability for rating scales: Resolving some basic issues. Br J Psychiatry. 1976;129(5):452–456.
- Maher CG, Sherrington C, Herbert RD, et al. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721.
- Turner JA, Anderson ML, Balderson BH, et al. Mindfulness-based stress reduction and cognitive behavioral therapy for chronic low back pain: similar effects on mindfulness, catastrophizing, self-efficacy, and acceptance in a randomized controlled trial. Pain. 2016;157(11):2434–2444.
- Antúnez S, Almeida MC, Roldán R, et al. Effectiveness of an individualised physiotherapy program versus group therapy on neck pain and disability in patients with acute and subacute mechanical neck pain. Aten Primaria. 2017;49(7):417–425.
- Cherkin DC, Sherman KJ, Balderson BH, et al. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: a randomized clinical trial. JAMA. 2016;315(12):1240–1249.
- Sandal LF, Bach K, Øverås CK, et al. Effectiveness of app-delivered, tailored self-management support for adults with lower back pain–related disability: a selfBACK randomized clinical trial. JAMA Intern Med. 2021;181(10):1288–1296.
- França FR, Burke TN, Caffaro RR, et al. Effects of muscular stretching and segmental stabilization on functional disability and pain in patients with chronic low back pain: a randomized, controlled trial. J Manipulative Physiol Ther. 2012;35(4):279–285.
- Pincus T, Burton AK, Vogel S, et al. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine (Phila Pa 1976). 2002;27(5):E109–E120. E109E20
- Arnstein P, Caudill M, Mandle CL, et al. Self efficacy as a mediator of the relationship between pain intensity, disability and depression in chronic pain patients. Pain. 1999;80(3):483–491.
- Picavet HSJ, Vlaeyen JW, Schouten JS. Pain catastrophizing and kinesiophobia: predictors of chronic low back pain. Am J Epidemiol. 2002;156(11):1028–1034.
- Buenaver LF, Edwards RR, Haythornthwaite JA. Pain-related catastrophizing and perceived social responses: Inter-relationships in the context of chronic pain. Pain. 2007;127(3):234–242.
- Esteve R, Ramírez-Maestre C, López-Marínez AE. Adjustment to chronic pain: the role of pain acceptance, coping strategies, and pain-related cognitions. Ann Behav Med. 2007;33(2):179–188.
- Raja SN, Carr DB, Cohen M, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982.
- Knezevic NN, Candido KD, Vlaeyen JWS, et al. Low back pain. Lancet. 2021;398(10294):78–92.