
Abstract
Objective
The purpose of this meta-analysis was to evaluate the postoperative clinical outcomes of elderly patients who underwent the direct anterior approach (DAA) versus those who received posterolateral approach (PLA) for total hip arthroplasty (THA) in the treatment of femoral neck fractures.
Methods
An electronic search was conducted in databases including PubMed, Embase, Web of Science, the Cochrane Library, and CNKI from their inception to January 2022. We calculated the odds ratio (OR) and mean difference (MD) with 95% confidence intervals (CIs) to assess the effect of DAA compared to PLA for the management of total hip arthroplasty (THA) in elderly patients using the dichotomous or continuous method with a random or fixed-effect model.
Results
15 studies involving 1284 patients were included; 640 patients receiving DAA and 644 patients receiving PLA. DAA had a longer surgery duration than PLA [WMD = 9.41, 95% CI (4.64, 14.19), I2=95.5%]; The amount of postoperative drainage [WMD= −3.88, 95% CI (−5.59, −2.17), I2=98.3%], length of incision [WMD= −3.88, 95% CI (−5.59, −2.17), I2=98.3%], blood loss [WMD= −3.88, 95% CI (−5.59, −2.17), I2=98.3%], hospitalization time [WMD= −3.88, 95% CI (−5.59, −2.17), I2=98.3%], and postoperative bedtime [WMD = −5.56,95% CI (−7.11, −4.01), I2=99.0%], were similar between the two groups (p < 0.05). The HHS at 1 month, 12 months postoperatively [WMD = 7.58, 95%CI (5.70,9.46), I2=89.5%; WMD= 2.56, 95%CI 0.11,5.00, I2=93.2%] and the incidence of LFCN in patients were higher in the DAA group (OR = 2.91, 95% CI 1.26 to 6.71, I2=0.0%), while fewer patients in the DAA group suffered from postoperative dislocation than in the PLA group (OR = 0.26, 95% CI 0.11 to 0.60, I2=0.0%). No significant difference was observed in HHS at 1 week, 3 months, and 6 months postoperatively, VAS postoperatively at each time point, acetabular anteversion angle, acetabular abduction angle, wound infection, deep vein thrombosis, and intraoperative fracture (p > 0.05).
Conclusions
DAA offers a quicker functional recovery and is less invasive with an earlier return to daily activities in older THA patients than PLA. However, DAA was found to be associated with a high incidence of lateral femoral cutaneous nerve injury and a low incidence of postoperative dislocation.
The present study aims to evaluate the clinical outcomes in elderly patients receiving DAA versus PLA for THA in the treatment of femoral neck fractures by mate-analysis.
DAA offers a quicker functional recovery and is less invasive with an earlier return to daily activities in older THA patients. No significant difference was observed between the colchicine and comparators in terms of the need for HHS at 1 week, 3 months, and 6 months postoperatively, VAS postoperatively, acetabular anteversion angle, acetabular abduction angle, and complications (wound infection, deep vein thrombosis, and intraoperative fracture).
Key messages
Introduction
The treatment of patients suffering from hip problems aims to help patients recover from normal hip activities and functions [Citation1]. The hip replacement surgery performed on patients is affected by patients’ geographic area, socio-economic status, gender, race, and age [Citation2,Citation3]. Total hip arthroplasty (THA) increases the risk of health hazards in older patients, given their deteriorating health conditions [Citation4]. An appropriate surgery technique for THA can relieve pain, improve hip function, and shorten hospital stay and recovery time thus gaining patients’ satisfaction [Citation5,Citation6]. Generally, surgeons should weigh up the pros and cons before performing THA on elder patients with multimorbidity. Nevertheless, no precise guidelines are available to surgeons on selecting the most desirable approach. THA can be performed using a variety of surgical approaches, such as the direct anterior approach (DAA), the anterolateral approach, the lateral approach, and the posterolateral approach (PLA) [Citation7–9]. Several reviews have investigated different surgical methods for THA in patients of all ages [Citation10–14]. According to Elina Huerfano et al. [Citation15], there was no statistically significant difference in the incidence of dislocation related to surgical factors or cup positioning between the DAA and PLA groups. As a result, after primary THA, surgical techniques had minimal impact on prosthesis instability. Elina Huerfano et al. focused on prosthesis instability after primary THA for all ages, while we are more concerned about intraoperative and postoperative clinical investigations only for elder patients. Zhang Jiakai et al. [Citation16] compared the effects of DAA and other methods on patients regarding femoral neck fractures. They found that DAA for hemiarthroplasty was associated with decreased dislocation rate in comparison with the posterior capsular approach. However, the effects of DAA versus PLA for THA in elderly patients with hip problems were not investigated, as the methods used to be compared with DAA in their study did not include PLA, and only patients with femoral neck fractures were investigated. Sun Xuedong et al. [Citation17] compared DAA and PLA through a network meta-analysis and they discovered higher HHS in 6-month postoperative periods and shorter hospital stay in the DAA group compared with the PLA group, suggesting that DAA was more effective than the PLA regarding the postoperative early recovery of function. However, their study did not investigate the effects of DAA and PLA only on elder patients. Hence, the present study aims to evaluate the clinical outcomes in elder patients receiving DAA versus PLA for THA by meta-analysis.
Methods
Search strategy and selection criteria
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. And the protocol was registered with the International Prospective Register of Systematic Reviews [Citation18].
Search strategy
The following databases were searched from their inception to January 2022, including Embase, PubMed, Cochrane library, Web of Science, and CNKI, with no restrictions on language. The following combined text and Medical Subject Headings (MeSH) terms were used: (Arthroplasty, Replacement, Hip[Mesh]); total hip replacement; total hip arthroplasty; direct anterior approach, posterolateral approach, THA, THR, DAA, and PLA, Aged[Mesh] OR Aged[Title/Abstract] OR Elderly[Title/Abstract]) OR old people[Title/Abstract]) OR elder[Title/Abstract]) OR Geriatric[Title/Abstract]. The search used for PubMed was: (Arthroplasty, Replacement, Hip[Mesh] OR Arthroplasty, Replacement[Title/Abstract] OR Arthroplasties, Replacement, Hip[Title/Abstract] OR Arthroplasty, Hip Replacement[Title/Abstract]) OR Hip Prosthesis Implantation[Title/Abstract]) OR Hip Prosthesis Implantations[Title/Abstract]) AND Direct anterior[Title/Abstract]) AND posterolateral[Title/Abstract] AND (Aged[Mesh] OR Aged[Title/Abstract] OR Elderly[Title/Abstract]) OR old people[Title/Abstract]) OR elder[Title/Abstract]) OR Geriatric[Title/Abstract]). All studies potentially eligible for review were considered, regardless of primary outcome or language.
Literature selection and data extraction
Studies were included in this meta-analysis if they were randomized clinical trials (RCTs) or controlled clinical trials which compared DAA and PLA for THA in elderly patients with a femoral neck fracture. We included elderly patients at age of over 60. We excluded studies if their full texts were not available, or their original research cannot be extracted. Excluded study types included animal experiments (such as pharmacological or pharmacokinetic studies), case reports, abstracts, editorial comments, conference papers, reviews, meta-analyses, etc. Duplicate publications were also excluded. The titles and abstracts were screened by two investigators independently to identify studies that met the inclusion criteria for full-text assessment. Two investigators analysed the selected studies and extracted data with an agreement value (κ) of 96·5%. Any disagreements were resolved by a third investigator. The extracted data included the name of the first author, publication year, country, general characteristics of patients (age, proportion of female patients, and BMI), outcomes, study and follow-up duration. The primary outcomes were Harris hip score (HHS) at 1 week, 1 month, 3 months, 6 months, and 12 months postoperatively; VAS at 3 days, 7 days, 1 month, and 6 months postoperatively; length of incision, duration of surgery, blood loss, length of hospital stay, postoperative drainage, acetabular abduction angle, acetabular anteversion angle, and complications (intraoperative fracture, postoperative dislocation, lateral femoral cutaneous nerve (LFCN) neurapraxia, wound infection, and deep vein thrombosis). Reference lists of relevant systematic reviews and identified articles also were reviewed to find additional eligible studies as completely as possible. No restriction was placed on the language or country of publication.
Statistical analysis
Continuous outcomes (Harris hip score at 1 week, 1 month, 3 months, 6 months, and 12 months postoperatively; VAS at 3 days, 7 days, 1 month, 6 months, and 12 months postoperatively; length of incision, duration of surgery, blood loss, length of hospital stay, postoperative drainage, duration of postoperative bed rest, acetabular abduction angle, acetabular anteversion angle) were reported as weighted mean differences (WMD) with 95% confidence intervals (CIs). As for the meta-analysis of dichotomous outcomes (intraoperative fracture, postoperative dislocation, lateral femoral cutaneous nerve (LFCN) neurapraxia, wound infection, and deep vein thrombosis), the odds ratio (OR) with 95% CIs was used. p < 0.05 was considered the threshold of significant difference. The funnel plot was adopted to assess publication bias (as shown in the Supplement) for the effect size against the standard error in each eligible study. Begg’s test was performed to examine the asymmetry of the funnel plot. with p < 0.05 suggesting publication bias [Citation19]. We performed the Chi-square test to evaluate heterogeneity between studies [Citation20] and the I2 test to assess the magnitude of the heterogeneity, with I2 value over 50% indicating high heterogeneity [Citation21]. Software Stata version 15.1 (Stata Corp, College Station, TX, USA) was utilized for all statistical analyses.
Funding source
This study was funded entirely by intramural funds without the involvement of any commercial entities. The funding source was not involved in the design of the study, data collection, data analysis, data interpretation, or report writing. The corresponding author had full access to all study data and was ultimately responsible for the decision to submit it for publication.
Results
Eligible studies and their characteristics
The literature retrieval and selection process is presented in . A total of 105 studies were initially identified from databases (Web of Science = 20, Embase = 34, PubMed = 31, Cochrane Library = 5, CNKI =15). Endnote X8 (Thomson Reuters Corp, USA) software was utilized to remove duplicate publications, with 77 studies left. After screening the titles and abstracts, 28 studies were removed. Finally, 15 studies with 1,284 patients (DAA group = 640, PLA group = 644) that met the inclusion criteria were included in the meta-analysis [Citation22–36], and the basic characteristics of included studies are summarized in . The publication year was from 2015 to 2021. Follow-up duration ranged from 1 week to 1 year.
Figure 1. The flow diagram of study selection.
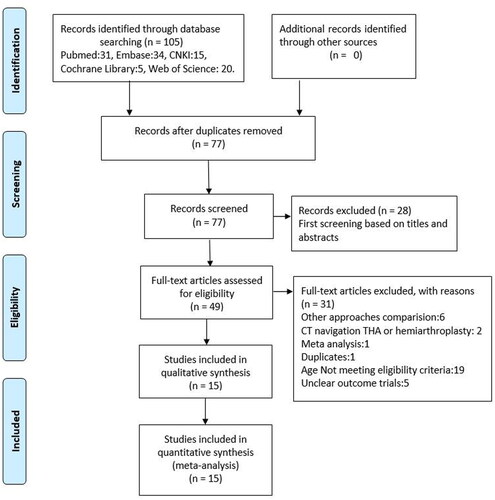
Table 1. General characteristics of included studies.
Risk of bias
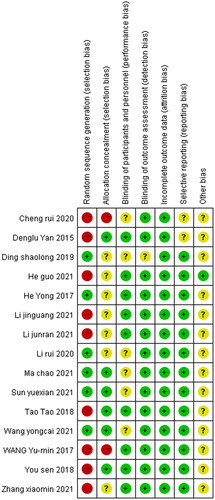
The risk of bias graph and summary across included studies are presented in and Citation3 respectively. Among 15 eligible studies, 2 were rated with a low risk of bias (selection bias), and 5 were judged with unclear risk of bias (selection bias). The risk of bias about allocation concealment was low in 4 studies but high in the other 2 studies. The risk of bias about the blinding of participants was high across all eligible studies. The risk of bias regarding attrition was unclear in 6 studies. The risk of bias from other sources was high in 1 study and unclear in 2 studies.
Figure 2. Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.
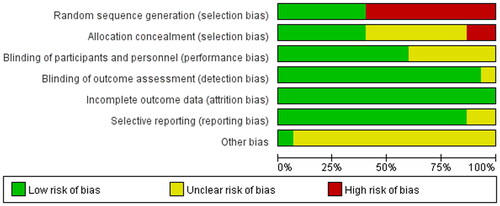
Figure 3. Risk of bias summary for included studies. +, no bias; −, bias; ?, bias unknown.
Meta-analysis
Harris hip score at 1 week, 1 month, 3 months, 6 months, and 12 months postoperatively
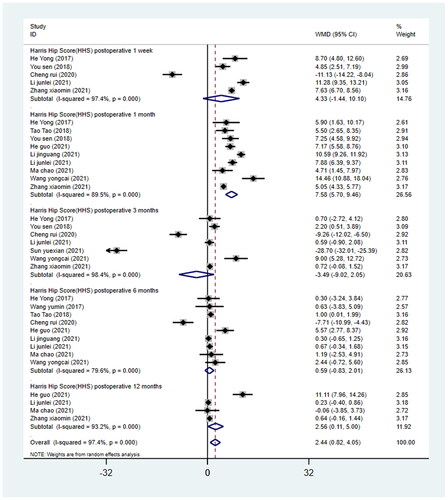
Among the 15 studies, 5 studies [Citation23,Citation26,Citation28,Citation32,Citation36] reported HHS at 1 week postoperatively, 9 studies [Citation23,Citation25,Citation26,Citation30–33,Citation35,Citation36] reported HHS at 1 month postoperatively, 7 studies [Citation23,Citation26,Citation28,Citation32,Citation34–36] reported HHS at 3 months postoperatively, 9 studies [Citation23–25,Citation28,Citation30–33,Citation35] reported HHS at 6 months postoperatively, and 4 studies [Citation20,Citation28,Citation29,Citation32] reported HHS at 12 months postoperatively. A total of 1,284 patients who received THA were involved in 15 eligible studies (640 in the DAA group and 644 in the PLA group). We conducted the meta-analysis in subgroups based on different follow-up time points. The results showed that HHS at 1 month and 12 months postoperatively were higher in the DAA group than that in the PLA group (1 month, WMD = 7.58, 95%CI 5.70 to 9.46, p = 0.000, I2=89.5%; 12 months, WMD= 2.56, 95%CI 0.11 to 5.00, p = 0.040, I2=93.2%; ). No statistically significant difference was observed between the two surgical approaches in HHS at 1 week, 3 months, and 6 months postoperatively (1 week, WMD = 4.33, 95%CI − 1.44 to 10.10, p = 0.142, I2=97.4%; 3 months, WMD = −3.49, 95%CI −9.02 to 2.05, p = 0.217, I2=98.4%; 6 months, WMD = 0.59, 95%CI −0.83 to 2.01, p = 0.415, I2=79.6%; ).
Figure 4. Forest plot for comparing DAA versus PLA in terms of Harris hip score postoperative at 1 week, 1 month, 3 months, 6 months and 12 months.
Visual analogue scale at 3 days, 7 days, 1 month, 6 months, and 12 months postoperatively
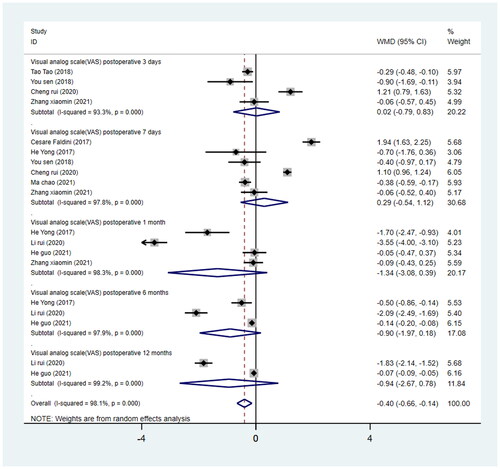
Compared with the PLA group, the DAA group was not associated with the VAS at each time point postoperatively in comparison with the PLA group (3 days, WMD = 0.02, 95%CI −0.79 to 0.83, p = 0.96; 7 days, WMD = 0.05, 95%CI −0.918 to 0.817, p = 0.909; 1 month, WMD = −1.34, 95%CI −3.08 to −0.39, p = 0.130; 6 months, WMD = −0.90, 95%CI −1.97 to −0.18, p = 0.101; 12 months, WMD = −0.94, 95%CI −0.56 to −0.02, p = 0.284; ).
Figure 5. Forest plot for comparing DAA versus PLA in terms of Visual Analogue Scale at 3 days, 7 days, 1 month, 6 months, and 12 months.
Length of incision
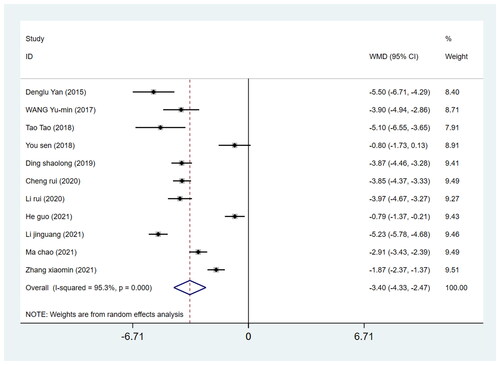
Eleven studies reported incision length involving 909 patients undergoing THA (449 in the DAA group and 460 in the PLA group). By pooling the data on the length of incision from these studies, the incision length in the DAA group was found to be 3.40 cm shorter than that in the PLA group. (WMD = −3.40, 95%CI −4.33 to −2.47, I2=95.3%, p = 0.000, ).
Figure 6. Forest plot for comparing DAA versus PLA in terms of skin incision length.
Duration of surgery
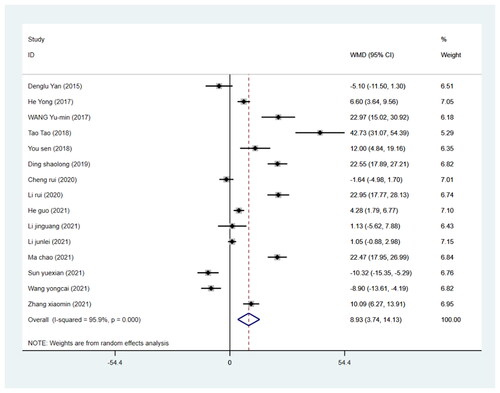
The duration of surgery was reported in all 15 included studies involving 1284 patients (640 in the DAA group and 644 in the PLA group). We pooled the data on surgery duration from these studies and found that compared with the PLA group, the increase in the surgery duration was not related to the DAA approach (WMD= 8.93, 95%CI 3.74 to 14.127, p = 0.001, I2=95.9% ).
Figure 7. Forest plot for comparing DAA versus PLA in terms of operation time.
Blood loss
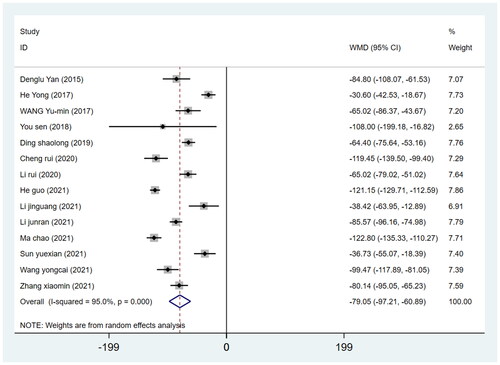
Fourteen studies reported blood loss involving 1204 patients (605 in the DAA group and 599 in the PLA group). We pooled the data on blood loss from these studies and discovered that the postoperative blood loss in the DAA group was less than that in the PLA group (WMD = −79.05, 95%CI −97.21 to −60.89, I2=95.0%, p = 0.000, ).
Figure 8. Forest plot for comparing DAA versus PLA in terms of blood loss.
Length of stay in hospital
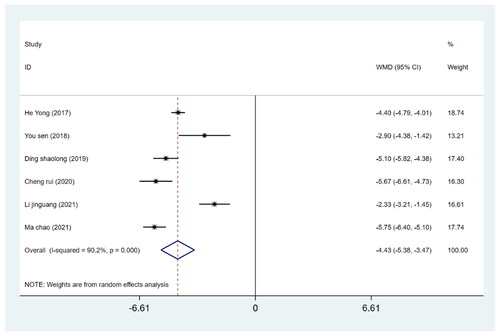
The length of hospital stay was reported in six studies involving 482 patients (241 in the DAA group and 241 in the PLA group). A random-effects model was utilized for meta-analysis due to significant heterogeneity across eligible studies (I2 > 50%) which could not be eliminated by either sensitivity analysis or subgroup analysis. The results revealed no significant difference between the two groups regarding the hospital length of stay (WMD= −4.43, 95%CI −5.38 to −3.47, p = 0.000, ).
Figure 9. Forest plot for comparing DAA versus PLA in terms of hospitalization time.
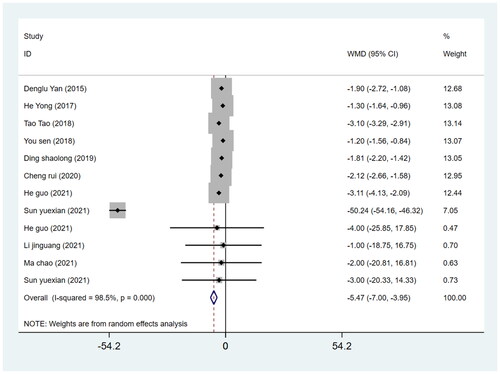
Postoperative bed rest duration
The WMD of the duration of postoperative bed rest for the DAA group which was −5.47 (p = 0.000; 95%CI −7.00 to −3.95), was lower than that for the PLA group, with a significant difference between the two groups (p < 0.05) ().
Figure 10. Forest plot for comparing DAA versus PLA in terms of the duration of postoperative bed rest.
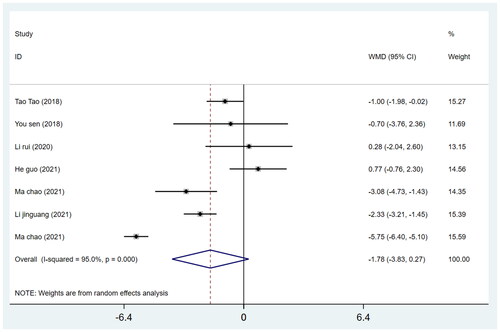
Acetabular abduction angle
We pooled data from 7 studies on 436 patients (215 in the DAA group and 221 in the PLA group) regarding the acetabular abduction angle of THA. The WMD of the inclination angle through DAA was −1.78 (p = 0.088; I2=95.0%,95%CI − 3.83 to −0.27), while between the two approaches, there was no significant difference in the acetabular abduction angle (p > 0.05) ().
Figure 11. Forest plot for comparing DAA versus PLA in terms of acetabular abduction angle.
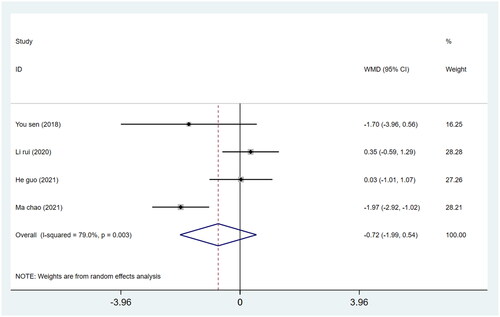
Acetabular anteversion angle
We pooled data on 356 patients (180 in the DAA group and 176 in the PLA group) from 7 studies regarding the acetabular abduction angle of THA. For the DAA method, the WMD of the anteversion angle was −0.72 (p = 0.263; 95%CI −1.99 to 0.54), with no significant difference in the acetabular abduction angle between the two groups (p > 0.05) ().
Figure 12. Forest plot for comparing DAA versus PLA in terms of acetabular anteversion angle.
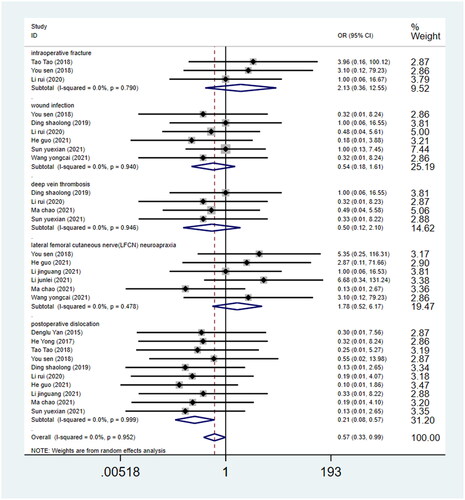
Complications
No significant difference emerged between the DAA and the PLA group in terms of intraoperative fracture (OR = 2.20, 95%CI 0.398 to 12.191, p = 0.366, ), wound infection (OR = 0.51, 95%CI 0.18 to 1.45, p = 0.204, ), and deep vein thrombosis (OR = 0.49, 95%CI 0.12 to 2.00, p = 0.320, ). During the follow-up period, the incidence of the lateral femoral cutaneous nerve (LFCN) neurapraxia was found to be higher in the DAA group than that in the PLA group (OR = 1.78; 95%CI 0.52 to 6.17, p = 0.358, ). However, complete recovery was recorded respectively at 3- and 6-month followup. Moreover, The DAA group was also related to a higher incidence of postoperative dislocation compared with the PLA group (OR = 0.201; 95%CI 0.08 to 0.53, p = 0.001, ) [Citation17,Citation33,Citation37,Citation38].
Figure 13. Forest plot for comparing DAA versus PLA in terms of complications.
Discussion
It has been a hot topic for researchers to determine the most effective surgical approach for THA elderly patients that has the most satisfying therapeutic effect with a low likelihood of postoperative problems.
In the present study, we conducted a meta-analysis to compare the DAA and the PLA approach to THA in elderly patients. Our analysis revealed that DAA reduced postoperative drainage, incision length, and blood loss and improved postoperative bed rest duration, length of stay in the hospital, and surgery duration. Since DAA is less invasive than PLA for THA in elderly patients with lower surgical stress, the results demonstrated a statistically significant difference in favour of DAA. In contrast, the meta-analyses by N. Ramadanov et al. [Citation39] found similarly prolonged operation times in THA through DAA. DAA had a shorter incision length than CAs; DAA had similar results compared to CAs for blood loss. To further validate our conclusion, a sensitivity analysis was performed. The evidence quality of most of our analyses was low to middle.
Our meta-analysis targeted elderly patients and is comprehensive considering analyzing the following outcomes: HHS at 1 week, 1 month, 3 months, 6 months, and 12 months postoperatively; VAS at 3 days, 7 days, 1 month, 6 months, and 12 months postoperatively; incision length, duration of surgery, blood loss, length of hospital stay, postoperative drainage, duration of postoperative bed rest, acetabular abduction angle, and acetabular anteversion angle. To the best of our knowledge, this study involves the most comprehensive meta-analysis to evaluate DAA and PLA for THA in elderly patients.
HHS was used to assess the function of the hip joint, and our analysis results revealed significant differences between the two approaches in terms of HHS score at 1 month and 12 months postoperatively. The network meta-analysis conducted by Putananon et al. [Citation8] conducted a network meta-analysis to compare DAA and PLA in THA and found that DAA was a preferable approach for improving postoperative VAS and HHS, but they only compared the VAS and HHS at the final follow-up. The meta-analysis by N. Ramadanov et al. [Citation39] showed no difference in HHS 3, 6 and 12 months postoperatively in THA through DAA compared to THA through CAs. In our study, the VAS and HHS were classified at several time points postoperatively. According to our meta-analysis, DAA was better than PLA considering the HHS at 1 month and 12 months postoperatively, while no significant differences were observed between the two approaches regarding the HHS at 1 week, 3 months, and 6 months postoperatively. It was found that DAA was not related to the VAS score at 3 days, 7 days, 1 month, 6 months, and 12 months postoperatively in comparison with PLA. The overall results showed a tendency towards a better outcome in THA through DAA compared to THA through PLA. The improved functional outcome found in THA through DAA follows the lower tissue and muscle damage, presumably because of operating in a muscle-sparing anatomical plane. The improvement of HHS and relief of pain severity by DAA may be attributed to its muscle-sparing nature and less damage to soft tissue, compared with PLA [Citation40].
In the present meta-analysis, these studies reported less mean hospitalization time, shorter operative time, and earlier duration of postoperative bed rest. Nevertheless, the PLA group generally required longer skin incision length and reported more blood loss and postoperative drainage during surgery. This indicates that PLA does more harm to the soft tissue than DAA, suggesting that the minimal invasion of DAA is attributed to less soft tissue injury and less amount of blood transfusion which is important to older patients.
The comparison of DAA and PLA for THA in terms of complications (postoperative dislocation, intraoperative fracture, lateral femoral cutaneous nerve (LFCN) neurapraxia, wound infection, and deep vein thrombosis) revealed that no significant differences emerged between the two approaches regarding intraoperative fracture, wound infection, and deep vein thrombosis (p > 0.05). However, DAA was found to be associated with a lower risk of postoperative dislocation, while the incidence of LFCN injury was higher in the DAA group than that in the PLA group with a significant difference. Only one study [Citation38] involving 96 patients (48 in the DAA group and 48 in the PLA group) reported the rate of aseptic loosening at 2.08% in the PLA group.
The survival rate of artificial implants can be affected by the placement of femoral components [Citation41]. The meta-analysis results revelated no significant differences in acetabular anteversion angle and abduction angle between the DAA and PLA groups [Citation39]. What’s more, the mean cup inclination and anteversion angle of the DAA and PLA groups were almost within Lewinnek’s safe zone [Citation42]. Therefore, we think that both DAA and PLA are effective for THA from the radiography perspective.
Conclusion
Compared with PLA, DAA is related to earlier functional recovery and less invasion to help elderly THA patients return to normal activities. It was discovered that postoperative dislocation was uncommon for DAA. High-quality RCTs with large sample sizes that take account of complications, including lateral femoral cutaneous nerve injury and incidence of postoperative dislocation, during a long-term follow-up are required to verify these findings.
Limitation
Our study has some limitations. First, more high-quality RCTs are needed to further investigate the effects of DAA on THA patients. Second, the inclusion of retrospective studies for meta-analysis inevitably resulted in selection bias. Third, differences in postoperative rehabilitation may lead to heterogeneity in the outcome. Four, we searched four English databases without limiting the language of the search. After screening strictly, irrelevant studies were excluded, and most of the included literature were from China. We respect the objective facts of the screened results. However, for the sake of the rigour and reliability of the results, we evaluated the quality of the literature strictly by the Cochrane bias risk assessment tool, and the results suggested that the overall literature quality was good. Although Chinese literature does not affect the results and conclusions, the results of a single language have certain limitations. We look forward to more studies from all over the world to verify and enrich our results in the future. Besides, the high risk of bias in participant blinding affects the accuracy of the results.
Author contributions
All authors have made substantial contributions to this work and have approved the final version of the manuscript. Concept and design: ZQJ. Acquisition of data: ZQJ, LGW, QJW. Statistical analysis: ZQJ, JQ, HH. Interpretation of data: ZQJ, LGW, JQ, HH. Writing original draft: ZQJ, QJW. Writing review and editing: all authors.
Disclosure statement
The authors declare that the research was conducted without any commercial or financial relationships that might be regarded as a potential conflict of interest.
Data availability Statement
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.
Additional information
Funding
References
- Souder CD, Brennan ML, Brennan KL, et al. The rate of contralateral proximal femoral fracture following closed reduction and percutaneous pinning compared with arthroplasty for the treatment of femoral neck fractures. J Bone Joint Surg Am. 2012;94(5):418–425.
- Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–785.
- Mota RE, Tarricone R, Ciani O, et al. Determinants of demand for total hip and knee arthroplasty: a systematic literature review. BMC Health Serv Res. 2012;12(1):225.
- Ferguson R, Prieto-Alhambra D, Peat G, et al. Does pre-existing morbidity influences risks and benefits of total hip replacement for osteoarthritis: a prospective study of 6682 patients from linked national datasets in England. BMJ Open. 2021;11(9):e046712.
- Husted H, Holm G. Fast track in total hip and knee arthroplasty–experiences from hvidovre university hospital. Denmark Injury. 2006;37(Suppl 5):S31–S35.
- Sculco PK, Pagnano MW. Perioperative solutions for rapid recovery joint arthroplasty: get ahead and stay ahead. J Arthroplasty. 2015;30(4):518–520.
- Yang XT, Huang HF, Sun L, et al. Direct anterior approach versus posterolateral approach in total hip arthroplasty: a systematic review and meta-analysis of randomized controlled studies. Orthop Surg. 2020;12(4):1065–1073.
- Putananon C, Tuchinda H, Arirachakaran A, et al. Comparison of direct anterior, lateral, posterior and posterior-2 approaches in total hip arthroplasty: network meta-analysis. Eur J Orthop Surg Traumatol. 2018;28(2):255–267.
- Pituckanotai K, Arirachakaran A, Tuchinda H, et al. Risk of revision and dislocation in single, dual mobility and large femoral head total hip arthroplasty: systematic review and network meta-analysis. Eur J Orthop Surg Traumatol. 2018;28(3):445–455.
- Meermans G, Konan S, Das R, et al. The direct anterior approach in total hip arthroplasty: a systematic review of the literature. Bone Joint J. 2017;99-b(6):732–740.
- Yoo JI, Cha YH, Kim KJ, et al. Gait analysis after total hip arthroplasty using direct anterior approach versus anterolateral approach: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2019;20(1):63.
- Yue C, Kang P, Pei F. Comparison of direct anterior and lateral approaches in total hip arthroplasty: a systematic review and Meta-Analysis (PRISMA). Medicine. 2015;94(50):e2126.
- Cha Y, Yoo JI, Kim JT, et al. Disadvantage during perioperative period of total hip arthroplasty using the direct anterior approach: a network Meta-Analysis. J Korean Med Sci. 2020;35(19):e111.
- Chen W, Sun JN, Zhang Y, et al. Direct anterior versus posterolateral approaches for clinical outcomes after total hip arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res. 2020;15(1):231.
- Huerfano E, Bautista M, Huerfano M, et al. Use of surgical approach is not associated with instability after primary total hip arthroplasty: a meta-analysis comparing direct anterior and posterolateral approaches. J Am Acad Orthop Surg. 2021;29(22):e1126–e1140.
- Zhang JK, Wu JL, Zheng XG[, et al. Meta-analysis of direct anterior approach and other approaches for hemiarthroplasty in elderly patients with femoral neck fracture. Zhongguo Gu Shang. 2020;33(8):776–783.
- Sun X, Zhao X, Zhou L, et al. Direct anterior approach versus posterolateral approach in total hip arthroplasty: a meta-analysis of results on early post-operative period. J Orthop Surg Res. 2021;16(1):69.
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
- Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–463.
- Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560.
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Statist Med. 2002;21(11):1539–1558.
- Yan D, Song Y, Pei F. Minimally invasive direct anterior approach for total hip arthroplasty in the management of femoral neck fractures in older patients. Curr Orthopaed Pract. 2015;26(1):27–31.
- Yong H, Liu XW, Zhang JD, et al. Clinical efficacy of total hip arthroplasty through direct anterior approach for the treatment of elderly femoral neck fracture. China Clin Pract Med. 2017;8(3):5.
- Wang YM, Li X. Minimally invasive direct anterior approach used in total hip arthroplasty for the treatment of femoral neck fracture in the elderly. Orthoped J China. 2017;25(18):5.
- Tao T. Comparison of early clinical effects between minimally invasive direct anterior approach and posterolateral approach for total hip arthroplasty in the treatment of femoral neck fractures. Soochow Univ. 2020;4:53.
- You S. The anatomy and clinical efficacy of total hip arthroplasty through direct anterior approach for the treatment of elderly femoral neck fracture. Fujian Med Univ. 2019;9:1–47.
- Ding S. Short and medium term effect of total hip arthroplasty with direct anterior approach in the treatment of senile femoral neck fracture. J Changzhi Med Coll. 2019;1(33):4.
- Chen R. Effect analysis of total hip arthroplasty with direct anterior approach for femoral neck fracture in elderly patients. Med Theory Pract. 2020;3(11):3.
- Li R, Song DC, Sun L. Clinical effect of minimally invasive total hip arthroplasty with direct forward approach for femoral neck fracture in elderly patients. Beijing Med. 2020;7(42):4.
- He G, Wang H, Bi Y, et al. Efficacy of different approaches of hip arthroplasty in treatment of senile femoral neck fracture complicated with parkinson’s disease. J Reg Anatomy Operat Surg. 2021;7(30):5.
- Li JG, Zhang JJ, Enhamujiang BY, et al. Comparison of effects of total hip arthroplasty through direct anterior approach and posterolateral approach in treatment of elderly patients with femoral neck fractures. Med J Chin People’s Health. 2021;19(33):3.
- Li JR, Li LG, Zhai JX, et al. Comparison of early functional recovery between direct anterior minimally invasive surgery and posterolateral approach for total hip arthroplasty in the treatment of femoral neck fracture in the elderly. Chin J Anat Clin. 2022;2(26):6.
- Ma C, Tang HY. Clinical effect of total hip arthroplasty via direct anterior approach and posterolateral approach in the treatment of femoral neck fractures in the elderly. J Traum Surg. 2021;2:5.
- Sun YX, Yu J, Zhuang TW, et al. Observation on rehabilitation efficacy of total hip arthroplasty via direct anterior approach in elderly patients with femoral neck fracture. China Med Pharm. 2021;2:4.
- Wang YC, Huang Q, Liu K. The effects of the direct anterior approach and the posterolateral approach on the short term function of balance and proprioception in elderly patients with femoral neck fracture after to- tal hip arthroplasty. Pract J Clin Med. 2021;18(4):120–123.
- Zhang XM, Yan TS, Li GQ, et al. Comparison of early effects of total hip arthroplasty with direct anterior approach and posterolateral approach in the treatment of elderly femoral neck fractures. Clin Res Pract. 2021;23:4.
- Faldini C, Perna F, Mazzotti A, et al. Direct anterior approach versus posterolateral approach in total hip arthroplasty: effects on early post-operative rehabilitation period. J Biol Regul Homeost Agents. 2017;31(4 suppl 1):75–81.
- Bon G, Kacem EB, Lepretre PM, et al. Does the direct anterior approach allow earlier recovery of walking following total hip arthroplasty? A randomized prospective trial using accelerometry. Orthop Traumatol Surg Res. 2019;105(3):445–452.
- Ramadanov N, Bueschges S, Lazaru P, et al. A meta-analysis on RCTs of direct anterior and conventional approaches in total hip arthroplasty. Sci Rep. 2021;11(1):20991.
- Zhao HY, Kang PD, Xia YY, et al. Comparison of early functional recovery after total hip arthroplasty using a direct anterior or posterolateral approach: a randomized controlled trial. J Arthroplasty. 2017;32(11):3421–3428.
- Harrison CL, Thomson AI, Cutts S, et al. Research synthesis of recommended acetabular cup orientations for total hip arthroplasty. J Arthroplasty. 2014;29(2):377–382.
- Lewinnek GE, Lewis JL, Tarr R, et al. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60(2):217–220.