
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objective
The varicella vaccine is not included in the national childhood immunization schedules in China. Varicella epidemics and outbreaks are frequently reported, and the evidence for the effectiveness of the varicella vaccine remains unclear. The aim of this study was to investigate varicella vaccine effectiveness in Wuxi, China.
Methods
Varicella surveillance data were extracted from the China Information System for Disease Control and Prevention, and vaccination data were obtained from the Vaccination Integrated Service Management Information System of Jiangsu Province, China. Time-series analysis approaches were used to estimate varicella vaccine effectiveness.
Results
A total of 16,093 varicella cases among children aged 1–6 years between January 2016 and December 2020 were analysed. A total of 217,297 children completed a two-dose varicella vaccination series. Compared with districts with lower vaccination rates, districts in Wuxi with higher varicella vaccination rates had a lower proportion of cases (p < 0.001). In the time-series approach, 0.8% fewer varicella cases were associated with a 1% increase in the two-dose varicella vaccination rate (p < 0.001), and similar effects were found in both the male and female populations.
Conclusions
Two-dose varicella vaccination was recommended as an effective health intervention to prevent varicella in Wuxi, China. Varicella vaccination is urgently needed in routine childhood immunisation programs.
KEY MESSAGES
The introduction of two-dose varicella vaccination was an effective intervention to prevent varicella in Wuxi, China.
Varicella vaccination is urgently needed in routine childhood immunization programmes.
Introduction
Varicella is an acute and highly contagious respiratory disease caused by varicella zoster virus (VZV)[Citation1]. Children aged below 14 years are more susceptible to VZV, which usually causes outbreaks in school settings [Citation2]. Varicella has gradually become a considerable preventable disease burden in the population, and the global annual varicella disease burden includes 4.2 million severe complications leading to hospitalization and 4200 deaths [Citation3]. The prevalence of varicella in China ranks first among vaccine-preventable infectious diseases, with an average annual incidence of 55.05/100,000 people in 2016–2019 [Citation4,Citation5]. The varicella live attenuated vaccine (VarV) has been recommended in routine childhood immunization programs by the World Health Organization (WHO) to reduce the incidence of varicella among children[Citation6]. Currently, the VarV is included in routine childhood immunization programs in multiple countries[Citation7,Citation8]. Since 2000, an immunization program that includes a single dose of the VarV has been introduced for children aged 1–6 years in Wuxi, Jiangsu, China. However, on the basis of being well-informed, signing up voluntarily, self-funded, the coverage rate of one-dose varicella vaccine was still low[Citation9]. Currently, a two-dose schedule (at ages 12–15 months and 4–6 years) has been recommended since 2018, which is free of charge. Most recently, attacks and several outbreaks of varicella in Wuxi have continued to occur, it is increasingly being viewed as a serious public health problem [Citation10]. In addition, the immunization schedule is not widely recommended nationwide, and investigations assessing the effectiveness of the VarV are limited. There were also some doubts about the protection against varicella between the one-dose and two-dose schedules [Citation11].
In Jiangsu Province, since 1 January 2023, cities incorporated the two-dose varicella vaccine schedule into the Expanded Programme on Immunization. To gain a comprehensive understanding of the vaccination coverage rate of the VarV among children in Wuxi and to describe the effectiveness of the two-dose varicella vaccine schedule, our study assessed varicella vaccine effectiveness for preventing varicella in children 6 years or younger in Wuxi, China, following the introduction of the VarV in December 2018. We hypothesized that varicella vaccine, especially the two-dose vaccine, would decrease the incidence of varicella, which could help optimize immunization programs in China.
Materials and methods
Study site
Wuxi, located 31°07′ to 32°02′ N and 119°31′ to 120°36′ E in southern China, is a low latitude, mild temperature and high humidity area with a population of approximately 7 million. Wuxi is divided into 7 districts (i.e. Liangxi, Binhu, Xishan, Huishan, Xinwu, Jiangyin, and Yixing).
Definition of varicella and data collection
A case of varicella was defined as an acute maculopapulovesicular rash without other apparent cause, with laboratory confirmation of varicella or an epidemiological link to a confirmed case. In general, varicella is clinically diagnosed by paediatricians. Presently, in Wuxi, varicella is reported as a statutorily notifiable infectious disease through clinical diagnoses or laboratory confirmation. The data on varicella cases from 1 January 2016, to 31 December 2020 were extracted from the China Information System for Disease Control and Prevention according to the date of onset and the patient’s current address and information including name, sex, age, and birth date. Wuxi Centre for Disease Control and Prevention is responsible for reviewing and managing the national notifiable disease reported in Wuxi legally, and we had authority to obtain and analyze the data. All varicella cases aged 1–6 years in Wuxi were included in the current analysis.
VarV immunization program in Wuxi
Since 2000, a self-funded one-dose VarV immunization program for children aged 1–6 years has been introduced in Wuxi. Since December 2018, a two-dose VarV immunization program was implemented free of charge. Children under 4 years of age would be mandatorily vaccinated with two doses of VarV for free. Children over 4 years of age can be inoculated with the second dose of VarV at their own expense.
Vaccination data
We also obtained vaccination data from 1 January 2016, to 31 December 2020, from the Vaccination Integrated Service Management Information System of Jiangsu Province, China. The system is a standardized, computer-based database that collects on vaccination information including name, gender, date of birth, personal address, vaccine name and manufacturer, date and institution of vaccination and other related inoculations data. Wuxi Centre for Disease Control and Prevention had authority to manage or utilize the reported routine coverage data in Wuxi. Varicella case data and vaccination data were specified by the calendar date.
Demographic data
The total population per year from 2016 to 2020 for Wuxi was captured from the China Information System for Disease Control and Prevention. The annual number of live births each year from 2016 to 2020 in Wuxi was publicly obtained by consulting the Wuxi Statistical Yearbook [Citation12]. The vaccination inoculation rates of children aged 1 to 6 years by month were computed each year.
Climate data
Meteorological data we used were obtained from the Wuxi Meteorological Service Centre. We aggregated the daily climate data in Wuxi into monthly average data for use in the final statistical models.
Statistical analysis
Descriptive data were expressed as percentages. We described the vaccination rates for all districts according to the median varicella vaccination rates for one dose (53.77%) and two doses (29.36%) from 2016 to 2020. The formula to calculate the case proportions was case number after vaccination between 2018 and 2020 divided by the total case number occurred from 2016 to 2018. Further, the case proportion of districts with high vaccination rates was defined as “proportion 1” and “proportion 2” represented for districts with low vaccination rates. Thus, we did spatial ecological analysis and calculated the varicella rate ratios, which has been described in detail elsewhere[Citation13].
We then used the same multivariate time-series regression model as Du et al. reported before[Citation13], a widely used ecological approach to describe the varicella sentinel surveillance data as a function of vaccination rates. Finally select the better model according to q-AIC criteria. The final model was described below:
where t refers to the month of the observation and ε is the residual error. log(y) denoted estimated variation of the monthly number of varicella cases (y) by using a log-transformation, x was represented for the monthly vaccination rate (x, %) according to the corresponding age group, and offset (log(births)) was used as the respective period. Additionally, we adjusted the mean temperature and relative humidity. Furthermore, the seasonality is modelled explicitly using f(t), i.e. the Fourier components[Citation14], consisting of two harmonics with frequencies of 6 and 12 months(e.g. f(1) = f(7) and f(1) = f(13)). We performed a sensitivity analysis to determine the final model (see Supplementary Table S1–S2). Using this approach, vaccine effectiveness can be estimated[Citation15] as follows:
Table 1. Number (%) of varicella cases and varicella vaccinations in Wuxi, China, 2016–2018.
Table 2. Ratios of varicella cases for high and low varicella vaccination rate districts in Wuxi, China, 2016–2020.
All statistical analyses were performed in R, version 4.1.2 (The R Foundation for Statistical Computing, Vienna, Austria), and a two-tailed p < 0.05 was considered statistically significant.
Results
Participant characteristics
In total, 16,093 varicella cases were reported between January 2016 and December 2020. A decrease (from 34.83% to 6.40%) in the proportion of cases was observed since 2018. Male cases accounted for 55.49%. An increasing number of children completed varicella vaccinations from 2016 to 2020 for both the one-dose and two-dose programs ().
Spatial ecological analysis
presents ratios for districts with high and low vaccination rates in Wuxi, China, from 2016–2020. Compared with the districts with lower vaccination rates, districts with higher varicella vaccination rates (i.e. above the median varicella vaccination rate) had a lower proportion of cases (p < 0.001).
Time-series analysis
presents the results of the associations between varicella vaccination rates and varicella cases in Wuxi. All regression coefficients were negative for the total study population and population subgroups for the two-dose program, that is, high rates of vaccination can reduce the occurrence of cases. The risk of the varicella decreased averagely by 0.8% with 1% increments of vaccination rate for two-dose. Similar effects were found in both the male and female populations.
Table 3. Associations between varicella vaccination rate and varicella cases in Wuxi, China, 2016–2020.
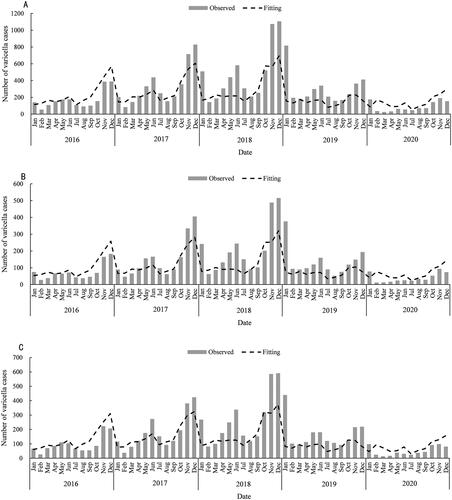
shows the distribution of varicella cases as a function of the two-dose vaccination rate. It is shown that the result of fitted cases were very close to the observed data in all population groups, and the observed and fitted case numbers decreased since 2018. In addition, varicella cases had a seasonal pattern with two incidence peaks (April to June and November to January) each year in Wuxi. The two-peak seasonality was most prominent in cases before 2018, and the seasonal peak gradually tended to moderate thereafter.
Figure 1. Observed and fitted varicella cases for total study population (A), females (B), and males (C) in Wuxi, China, 2016–2020.
Discussion
Main findings of this study
This large ecological analysis revealed the burden of varicella among children aged 1–6 years in Wuxi, Jiangsu, China, in 2016–2020. The study focused on the effectiveness of the immunization schedule for varicella. Two-dose varicella vaccination rate were associated with greater reductions in varicella risk, but no significant association was observed with regard to one-dose schedule. It was noteworthy that males experienced the greatest vaccine effectiveness. As we known, we firstly demonstrate the effectiveness of varicella vaccination in various and kindergarten-aged children in Wuxi, Jiangsu, China, committed to enhancing of the vaccine effectiveness towards target population.
What is already known about this topic
The varicella vaccine, firstly developed in Japan in 1974, is thought to be simple and effective against varicella[Citation16]. Universal childhood vaccination was significant declines in varicella disease, and the recommended immunization strategy has varied recently. Some studies have been conducted to estimate the protective effect of two doses of varicella vaccine. Globally, studies have demonstrated that the effectiveness of two-dose varicella vaccination programs is over 90%[Citation17]. The two-dose schedule was introduced in Germany in 2009, and the number of cases was reduced by 63% in the 0–4-year-old age group[Citation18]. Moreover, varicella incidence declined by 90% after universal childhood vaccination against varicella was established in the United States in 2006 [Citation19].
Since 2012, a two-dose schedule has been recommended in some districts of China for further control of varicella [Citation20]. Hu et al. conducted a 1:3 matched case–control study in children in Qingdao, China, and found that the effectiveness of two-dose vaccination (81.6%) was substantially higher than that of one-dose vaccination (44.7%)[Citation21]. Additionally, another case–control study in Hangzhou demonstrated that two-dose VarV conferred better protection against varicella (98.0%)[Citation11]. A meta-analysis evaluate the two-dose varicella vaccine effectiveness for children in China and recommended that the two-dose immunization strategy was relatively effective for preventing varicella[Citation20]. Varicella is an epidemic in Jiangsu, although the coverage of the one-dose varicella vaccine has reached approximately 70%[Citation22]. At present, studies on two-dose varicella vaccination are limited in Jiangsu Province. Higher quality evidence is needed as a supplement for stronger recommendations.
What this study adds
In China, only a few provinces introduced a two-dose varicella vaccine schedule as a routine childhood immunization for children. The implementation of the two-dose varicella vaccination program in Wuxi clearly provided evidence to quantify the impact of the program. In the time-series approach, 0.8% fewer cases were associated with a 1% increase in the two-dose varicella vaccination rate, but according to an analysis of the vaccination situation, the immunization effectiveness of the two-dose program was 55.1%, which indicated a limited effect on the control of varicella. One reason for this may be the low immunization coverage rate [Citation21]. A study found that the estimated coverage rate of varicella based on Jiangsu Province’s vaccine management system (approximately 55–65%) was low, varicella outbreaks still occurred frequently in southern Jiangsu Province due to the lower antibody positive rate [Citation9]. Nonetheless, our study demonstrated that the immunization effect of varicella vaccine could blocked the transmission of varicella. Moreover, it has been only 3 years since the addition of the two-dose schedule to the Expanded Programme on Immunization, which means that vaccine performance may be underestimated. Thus, further surveillance remains warranted on the effectiveness following the immunization of two-dose VarV.
We also analyzed the gender difference and found modestly greater vaccine effectiveness of two-dose varicella vaccination among males than among females. In an epidemiological study, Xu et al. found that the number of female cases was always lower than the number of male cases, which may be due to different exposure levels [Citation11]. In contrast, another study showed that the seroprevalence was significantly higher in girls than in boys[Citation9]. Thus, vaccination coverage should be increased for both sexes. Similar to other studies[Citation23,Citation24], the seasonality of case occurrence may be driven by school entry requirements, and the seasonality peak of most cases has gradually become progressively less obvious since 2018. Moreover, our study showed that varicella cases reached a constant level after a dramatic decline in the initial period after the implementation of the two-dose vaccination schedule. Thus, a higher two-dose coverage rate achieved by implementation of the two-dose routine immunization program for children can more effectively control varicella cases or outbreaks in schools [Citation23]. It should be noted that the number of cases of varicella fell to the lowest level during early 2020, which in some way may be attributable to coronavirus disease 2019 (COVID-19) pandemic. A published study investigated the impact of COVID-19 pandemic on varicella dynamics in Japan and indicated that the increase in varicella incidence would be relatively small during the pandemic period [Citation25]. Despite the limited disruption of spring patterns of varicella infection in the present study, the long-term epidemic characteristics and periodical trend changes were relatively small during the COVID-19 pandemic.
Limitations of this study
There are limitations in this study. First, due to the prospective time-series data, our study was limited by a lack of detailed records on potential confounders, although the model is effective and reliable which corresponds to previous approaches[Citation13,Citation15]. Therefore, enough data should be collected and analyzed with the development of disease surveillance. Second, we could not illustrate the associations between one-dose and two-dose clearly, thus, potential exposure misclassification may have occurred. Third, Possible surveillance bias might have impacts on the study results, because varicella was defined through clinical diagnoses or laboratory confirmation. However, physicians in one city usually have integrative stability level of diagnosis technology, and the occurrence of varicella cases in our study varied slightly over the long term. Finally, breakthrough varicella cases with milder symptoms may be less likely to seek medical consultation or require hospital admission. In addition, vaccination coverage presented in the immunization registry may be overestimated, since unvaccinated children may be underrepresented [Citation23]. We obtained only reported five-year data, which was not sufficient to develop an understanding of long-term effects. Therefore, more data should be collected and analyzed in the future.
In conclusion, our findings reveal that the number of varicella cases declined with the 2018 introduction of two-dose varicella vaccination in Wuxi, China. Improving the coverage of two doses of vaccination may play an important role in varicella prevention and control. The effectiveness of the vaccine should be taken into account in long-term understanding and policy-making.
Ethical approval
This investigation was conducted by public health agencies as part of their legally authorized mandate and was therefore considered minimal-risk research. No confidential information was involved and the study was exempted from ethical approval by the Institutional Review Board Wuxi Centre for Disease Control and Prevention.
Authors’ contributions
The authors’ responsibilities were as follows: XHZ designed the study, instructed the data analysis and critically reviewed the manuscript, and approved the final manuscript as submitted. LLW did the data cleaning and analysis, drafted and finished the manuscript. XY, XWW, and PS established the database, planned the data analysis and reviewed and revised the manuscript. All authors read and approved the final manuscript as submitted.
Supplemental Material
Download MS Word (15 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Suh J, Choi J-K, Lee J, et al. Estimation of single-dose varicella vaccine effectiveness in South Korea using mathematical modeling. Hum Vaccin Immunother. 2022;18(5):1. doi: 10.1080/21645515.2022.2085468.
- Lopez AS, LaClair B, Buttery V, et al. Varicella outbreak surveillance in schools in sentinel jurisdictions, 2012–2015. J Pediatric Infect Dis Soc. 2019;8(2):122–7. doi: 10.1093/jpids/piy010.
- WHO (world health organization). Varicella and herpes zoster vaccines: WHO position paper, June 2014. Wkly Epidemiol Rec. 2014;89(25):265–287.
- Li Z, Yao Y, Lu X, et al. Impact of a two-dose varicella immunization program on the incidence of varicella: a multi-year observational study in Shanghai, China. Expert Rev Vaccines. 2021;20(9):1177–1183. doi: 10.1080/14760584.2021.1963236.
- Cheng T, Bai Y, Sun X, et al. Epidemiological analysis of varicella in dalian from 2009 to 2019 and application of three kinds of model in prediction prevalence of varicella. BMC Public Health. 2022;22(1):678. doi: 10.1186/s12889-022-12898-3.
- Wutzler P, Bonanni P, Burgess M, et al. Varicella vaccination - the global experience. Expert Rev Vaccines. 2017;16(8):833–843. doi: 10.1080/14760584.2017.1343669.
- Giglio N, Lasalvia P. Trends in varicella burden of disease following introduction of routine childhood varicella vaccination in Argentina: a 12-year time series analysis. Vaccines. 2022;10(7):1151. doi: 10.3390/vaccines10071151.
- Lee YH, Choe YJ, Lee J, et al. Global varicella vaccination programs. Clin Exp Pediatr. 2022;65(12):555–562. doi: 10.3345/cep.2021.01564.
- Zhang L, Ma W, Liu Y, et al. Analysis of sero-epidemiological characteristics of varicella in healthy children in Jiangsu Province, China. BMC Infect Dis. 2018;18(1):563. doi: 10.1186/s12879-018-3496-8.
- Suo L, Lu L, Wang Q, et al. Varicella outbreak in a highly-vaccinated school population in beijing, China during the voluntary two-dose era. Vaccine. 2017;35(34):4368–4373. doi: 10.1016/j.vaccine.2017.06.065.
- Xu Y, Liu Y, Zhang X, et al. Epidemiology of varicella and effectiveness of varicella vaccine in hangzhou, China, 2019. Hum Vaccin Immunother. 2021;17(1):211–216. doi: 10.1080/21645515.2020.1769395.
- Comprehensive statistical office. Statistical yearbook of Wuxi. Statistics Bureau of Wuxi; 2021 Sep 3 accessed 2022 May 30]: http://tj.wuxi.gov.cn/ztzl/tjnj/.
- Du Z, Huang Y, Bloom MS, et al. Assessing the vaccine effectiveness for hand, foot, and mouth disease in guangzhou, China: a time-series analysis. Hum Vaccin Immunother. 2021;17(1):217–223. doi: 10.1080/21645515.2020.1763076.
- Kiyono K. Establishing a direct connection between detrended fluctuation analysis and fourier analysis. Phys Rev E Stat Nonlin Soft Matter Phys. 2015;92(4):042925. doi: 10.1103/PhysRevE.92.042925.
- Höhle M, Siedler A, Bader HM, et al. Assessment of varicella vaccine effectiveness in Germany: a time-series approach. Epidemiol Infect. 2011;139(11):1710–1719. doi: 10.1017/S0950268810002815.
- Takahashi M, Otsuka T, Okuno Y, et al. Live vaccine used to prevent the spread of varicella in children in hospital. Lancet. 1974;2(7892):1288–1290. doi: 10.1016/s0140-6736(74)90144-5.
- Pawaskar M, Burgess C, Pillsbury M, et al. Clinical and economic impact of universal varicella vaccination in Norway: a modeling study. J Korean Med Sci. 2021;16(7):e0254080. doi: 10.1371/journal.pone.0254080.
- Siedler A, Arndt U. Impact of the routine varicella vaccination programme on varicella epidemiology in Germany. Euro surveillance: bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin. 2010;15.
- Chaves SS, Lopez AS, Watson TL, et al. Varicella in infants after implementation of the US varicella vaccination program. Pediatrics. 2011;128(6):1071–1077. doi: 10.1542/peds.2011-0017.
- Zhang Z, Suo L, Pan J, et al. Two-dose varicella vaccine effectiveness in China: a meta-analysis and evidence quality assessment. PLOS One. 2021;21:543.
- Hu P, Yang F, Li X, et al. Effectiveness of one-dose versus two-dose varicella vaccine in children in Qingdao, China: a matched case-control study. Hum Vaccin Immunother. 2021;17(12):5311–5315. doi: 10.1080/21645515.2021.1982281.
- Wang Y, Zhang L, Sun X, et al. Effectiveness and failure rate of the varicella vaccine in an outbreak in Jiangsu, China: a 1:2 matched case-control study. Hum Vaccin Immunother. 2020;16(3):506–512. doi: 10.1080/21645515.2019.1665959.
- Che X, Gu W, Jiang W, et al. Impact of a 2-dose voluntary vaccination strategy on varicella epidemiology in beijing, 2011–2017. Human Vaccin Immunother. 2020;38:3690–3696.
- Suh J, Lee T, Choi JK, et al. The impact of two-dose varicella vaccination on varicella and herpes zoster incidence in South Korea using a mathematical model with changing population demographics. Vaccine. 2021;39(18):2575–2583. doi: 10.1016/j.vaccine.2021.03.056.
- Suzuki A, Nishiura H. Transmission dynamics of varicella before, during and after the COVID-19 pandemic in Japan: a modelling study. Math Biosci Eng. 2022;19(6):5998–6012. doi: 10.3934/mbe.2022280.