
Abstract
Objectives
Kidney diseases are considered silent killers due to the lack of well-defined symptoms. Public knowledge about chronic kidney disease (CKD) management has been shown to decrease the risk of CKD onset and progression to end-stage renal disease and renal failure. The main objective of this study was to assess the knowledge of kidney function, CKD symptoms, etiology, prevention and treatment in the general population.
Methods
A cross-sectional study using a validated questionnaire was conducted in Jordan to assess public knowledge of CKD. Public knowledge of CKD was assessed using a questionnaire consisting of 32 knowledge questions, including risk factors, symptoms, treatment, protective measures and kidney function. The knowledge level was classified according to the total score: poor (0–50%), intermediate (51–70%) and good/high (71–100%). Multiple regression analysis was performed to compare knowledge scores (KS) and predict associations with the participants’ baseline characteristics.
Results
The level of knowledge about CKD among the 2181 participants was intermediate. The KS was significantly higher among participants with health issues such as hypertension, diabetes and heart problems, first-degree relatives working in the medical field, majors relevant to health, married, employed, highly educated, high-income and smokers. The main sources of knowledge about CKD were health professionals, TV shows, books and magazines. Multiple regression analysis showed an association between KS and age, sex, functional status, educational level and field, income, smoking status, having a family member/spouse work in the medical field, and knowledge source.
Conclusions
The public level of knowledge about CKD management is greatly influenced by participants’ health and social factors. Thus, improving public knowledge and perception through education and the media will significantly reduce CKD prevalence and incidence.
Key Messages
Public awareness and educating the public about chronic kidney diseases (CKDs) is essential because of the high prevalence, and increased awareness can contribute to early detection, management and potentially slow down the progression of CKD.
Creating awareness of the risk factors for CKD enables health policy developers to adopt preventive measures.
CKD can significantly affect quality of life, and public awareness campaigns can emphasize the impact of CKD on overall well-being, motivating individuals to prioritize kidney health.
Introduction
Chronic kidney disease (CKD) refers to kidney damage, decreased kidney function or both, and is characterized by a reduced glomerular filtration rate (GFR) of less than 60 mL/min per 1.73 m2 for at least 3 months [Citation1]. CKD is an emerging public health problem that affects 5–10% of the world’s population, with increasing prevalence and adverse outcomes [Citation2]. In 2017, the global prevalence of CKD was 9.1% which is approximately 700 million cases [Citation2]. The CKD prevalence in Jordan and the Middle East region is also high; the prevalence of CKD in the general population is 6.8% in Jordan [Citation3], 5.7% in Saudi Arabia [Citation4] and 14.9% in Iran [Citation5].
CKD can lead to end-stage renal disease (ESRD), cardiovascular disease and premature death [Citation6]. Risk factors associated with obesity and diabetes mellitus have increased the number of patients with CKD worldwide [Citation7]. Diabetes and hypertension account for over two-thirds of global CKD cases [Citation8]. Similarly, in Jordan, hypertension and diabetes are responsible for approximately 60% of CKD cases [Citation9]. Accordingly, educating patients about the importance of controlling diabetes and hypertension, since they are the main causes of ESRD, could significantly slow down the deterioration of kidney function and improve the quality of their lives [Citation10].
The global burden of CKD Studies has shown that CKD has emerged as a leading cause of mortality worldwide, causing more than 500,000 deaths since 1990 [Citation11]. Despite this, CKD has received relatively limited global attention and requires effective public health interventions for its prevention and management [Citation11]. Consequently, the prevalence of ESRD has continued to increase worldwide [Citation12]. According to The National Registry of ESRD Annual Report 2013, the number of patients with ESRD increased from 2666 to 4097, and the number of deaths increased from 125 to 520 [Citation11]. Additionally, there were 6316 patients that were treated in dialysis units by the end of 2019, with approximately 750 new cases in the same year [Citation13].
Most CKD patients are unaware of the severity of their disease [Citation14]. Lack of knowledge about CKD, as well as negative attitudes and practices, has resulted in a delayed diagnosis of CKD [Citation14]. Similarly, other studies have shown that many patients with CKD do not have enough knowledge to manage their fluid and diet [Citation15,Citation16], and subsequently accelerate the development of ESRD, increase dialysis cost and consequences of the disease, which negatively affects the health outcome. Interestingly, other studies showed that patients’ education can delay the progression of renal disease and improves survival [Citation16]. Therefore, increasing awareness by health care providers, especially among patients who are at high risk of developing CKD, could be an important tool in preventing or delaying the incidence of CKD in susceptible individuals [Citation18].
Educational programs carried out by healthcare providers enhance CKD patients’ satisfaction, increase self-care and overcome various misconceptions regarding diet, medication and dialysis [Citation17]. In addition, patients’ education and awareness of CKD can retard the progression of CKD and improve survival, illness-related complications, and quality of life [Citation19]. Hence, knowledge and adherence to treatment are major interventions to slow down the progression of CKD, as well as to prevent complications of CKD. Therefore, public knowledge of CKD management is important for the early diagnosis and treatment of the disease.
This study aimed to assess the knowledge of kidney function, CKD symptoms, etiology, prevention and treatment in the general population. Specifically, this study was conducted to answer the following questions:
What is the public level of knowledge about CKD management and prevention in Jordan?
What is the relationship between the sociodemographic characteristics of participants and their KSs?
What is the relationship between participants’ health information and KSs?
What are the most common sources of knowledge about CKD according to the participants?
Methods
This observational, analytical cross-sectional study consisted of two stages. Stage 1: preparation and validation of the CKD questionnaire and stage 2: a cross-sectional survey to assess Jordanians’ public knowledge of CKD.
Study design
The first draft of the questionnaire was prepared and modified by the research team using a previously published validated questionnaire prepared by Gheewala et al. [Citation20]. The questionnaire was modified as follows: (1) additional risk factors and symptoms were added to the existing ones. (2) New sections were introduced to the previously published questionnaire regarding the treatment and the protective measures for CKD. The new information was obtained from the National Kidney Foundation website (www.kidney.org). The modified version of the questionnaire was assessed for validity and reliability as follows; for validity, the questionnaire was evaluated and validated by the research team and experts in the field (two renal physiologists, and a nephrologist) to ensure the robust of the selected questions. For reliability, the questionnaire was sent to 36 participants in a pilot study. The reliability coefficient Cronbach’s alpha was calculated, and it was 0.962, this value indicates an excellent reliability for the survey items.
The final version of the questionnaire consisted of two parts. The first part collected socio-demographic information about the participants, including (age, sex, employment status, educational level, educational field, social status, place of residence, income, smoking status, family history of CKD, medical conditions and the source of knowledge about kidneys). The second part included knowledge questions on kidney function, CKD risk factors, symptoms, treatment and protective measures to prevent CKD.
The final version of the questionnaire consisted of 32 questions. The answers to the questions were multiple-choice options ‘True,’ ‘False’ and ‘I don’t know.’ The correct answer (True) was marked as 1, whereas the incorrect response and ‘I do not know’ option were marked as 0. The final version of the questionnaire was distributed to eligible individuals by the research team.
Since the respondents were all Arabic-speaking, the survey was translated into Arabic. The translation process consisted of two stages: (1) translating the questionnaire into the Arabic language and (2) back-translating the Arabic version into English using forward-backward translation techniques [Citation21]. To determine the minimum required sample size for this study, which was 385, the Raosoft sample size calculator was used with a confidence interval of 95% and a 0.5 precision [Citation22].
Data collection and sampling
The validated questionnaire was used to assess the public knowledge of CKD. The questionnaire was prepared using Google forms, and it was distributed online mainly in the Central and Northern territories of Jordan where most of people are living (about 63% in the central and 28% in the north) [Citation23]. To increase the statistical robustness of this study, we included 2181 participants.
At the beginning of the survey, participants were requested to indicate their consent to participate in the study by selecting ‘yes.’ They were explicitly informed that participation in the study was voluntary and optional, and assured that their information would be treated with confidentiality. An introductory paragraph illustrates the meaning of CKD and the aim of the study. Participants were asked to fill out the survey and choose the right answer based on their knowledge about CKD. As mentioned earlier, the correct answer was scored as 1 and the wrong answer was scored as 0. The correct answers were expressed as percentages for analysis. The knowledge level was classified according to the total score of each section: 0–50% scored as ‘poor,’ 51–70% scored as ‘intermediate’ and 71–100% scored as ‘Good/High’ [Citation24]. Notably, the STROBE cross-sectional reporting guidelines were checked to improve the study quality [Citation25]. It is noteworthy that the patients and the public were not involved in designing, conducting, reporting or disseminating the plans for this research.
Inclusion criteria
The inclusion criteria were as follows: (1) adults aged 18 years or above and (2) able to read and understand Arabic. The exclusion criteria were as follows: (1) non-Jordanians and (2) individuals with affected cognitive ability.
Statistical analysis
The survey data were analysed using IBM SPSS software (2020) (SPSS Inc., Chicago, IL). Descriptive and analytical statistics were used to extract the required statistical measures. Categorical variables, including sociodemographic information and knowledge, are expressed as frequencies and percentages. ANOVA and independent t-tests were used to study the effect of the baseline sociodemographic and health information of the participants on their CKD KS within each category. Multivariable linear regression analysis was performed to predict CKD KS based on the participants’ baseline characteristics (β coefficient: 95% CI), p value <.05 was considered statistically significant. The RStudio IDE programming language for statistical computing and graphics version 4.0.3 (10-10-2020) was used to prepare (Venn shape).
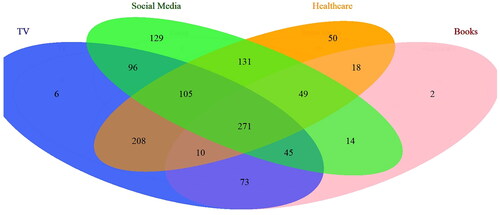
Figure 1. Venn diagram representing the public source of knowledge about CKD Venn shape showed the different sources of knowledge about CKD. The numbers represent the participants who chose one or more source of knowledge. TV, Books, Social media and internet, and healthcare professionals. Among the 2181 participants, 1207 identified their source of knowledge.
Results
The participant’s baseline sociodemographic and health information
A total of 2181 individuals participated in this study. The sociodemographic and health information of the participants are presented in . Most of the participants (69.7%) were from 18 and 35 years old. The majority were males (74.8%). Concerning the participant’s employment status, approximately 40% were employed. A large share of participants (89.1%) had undergraduate degree. About 14% of the surveyors’ educational field was related to health. 30.9% of the participants were married. Regarding the place of residence, approximately 88% were living in urban (cities). Of note, most of the participants (71%) had income less than 1500 USD/month. Among the participants, about 65% were smokers.
Table 1. Baseline sociodemographic, health information and CKD knowledge score.
The participants were also asked if they had a family member or a spouse who worked in the medical field, which could affect their knowledge, results showed that about 20% of the participants answered ‘yes.’ The participant’s baseline health information was included; 5.8% of them were diagnosed with kidney problems such as stones, failure, infection and protein in the urine, 17.8% had hypertension, 16.1% had diabetes and 8.8% had heart problems. Furthermore, 11% of the surveyors had a family history of kidney disease.
The public knowledge about kidney functions, CKD etiology, symptoms, treatment and protection
shows the public knowledge about kidney function, CKD risk factors, symptoms, treatments and protective measures. The participants were asked to respond to every 32 items with ‘True,’ ‘False’ or ‘I don’t Know.’
Table 2. The public knowledge about kidney functions, chronic kidney diseases etiology, symptoms and treatments.
Regarding kidney function (, items 1–5), 92.8% agreed that kidneys clean the blood from toxins and turn waste products into the urine, 81.5% confirmed that kidneys help to maintain the level of ions and salts in the blood, 58% thought that kidneys help to maintain blood pressure. However, only 21.6% knew the information that kidneys help to maintain healthy bones, and only 19.4% knew that kidneys help in producing RBC.
CKD risk factors (, items 6–17), the percentage of the respondents who answered correctly was as follows (highest to lowest): prolonged urine retention (90.5%), repeated kidney infections (88.9%), inherited genetic disorders (85.4%) and over-the-counter medications, such as ibuprofen and pain relievers (84%), unhealthy foods (81.8%), obesity (77.8%), aging (67.7%), hypertension (61.1%), nutritional supplements (54.6%) and diabetes (51.5%). To lesser extent, excessive stress (42.8%) and heart problems (heart failure or a heart attack) (24.9%).
For CKD symptoms (, items 18–23), the percentage of the participants who answered correctly was as follows: change in the amount and frequency of urination (85.1%), blood in the urine (81.9%), swollen feet and ankles due to water retention (68.1%), increased feeling of fatigue and tiredness (55.2%), nausea and vomiting (43.1%), loss of appetite and weight loss (42.3%).
The participants’ knowledge of CKD treatment is summarized in (items 24–27). The percentage of respondents who answered correctly the following statements were: one healthy kidney is sufficient for a person to lead a normal life (89.9%), proper diet and healthy lifestyle may help slow the progression of kidney disease (71.1%), dialysis and transplantation are only needed when the kidneys lose at least 85% of their function (59.8%), medicines that treat chronic diseases such as high blood pressure, and diabetes contribute to reducing the progression of CKD (53.9%).
Finally, the participants’ opinions regarding future protective measures against CKD are reported in (items 28–32). Their responses were: drinking plenty of water to avoid dehydration (94.2%), adopting a healthy lifestyle such as eating healthy and exercising (93.0%), regular checks on kidney function (82.3%), limiting the intake of caffeinated beverages (80.0%), treating risk factors such as diabetes and hypertension (77.2%).
The baseline characteristics affect the public knowledge scores
The impact of sociodemographic and health information on the participants’ KSs (out of 32) is shown in . There was no significant difference (p > .05) in KS between the different age groups, and between males and females. Interestingly, the number of employed participants (KS = 22.9) was significantly (p < .05) higher than that of the unemployed (KS = 21.0). Educational level influenced KS; participants with undergraduate degree had significantly higher levels of knowledge (KS = 22.4) compared to participants with high school or less (KS = 16.1). This indicates an important link between educational level and CKD knowledge. The educational field also affected participants’ KS, results showed that KS is significantly higher in participants whose educational field is relevant to health (KS = 26.0) than in others (KS = 21.1).
The social status of the participants had a significant effect on their level of knowledge; married individuals had significantly higher knowledge levels (KS = 22.5) than unmarried individuals (KS = 21.4). Further, the place of living also impacted KS; participants living in rural areas had a significantly higher level of knowledge (KS = 23.6) than those living in urban areas (KS = 21.5).
Noteworthy, the total income of the participants significantly affected the knowledge level, KS was higher among participants with income >1500 USD/month (KS = 24.6) compared to (KS = 20.6) in those with lower income (<1500 USD/month). Interestingly, the smoking status of participants affected their level of knowledge. Smokers had a significantly higher level of knowledge (KS = 22.5) than non-smokers (KS = 20.4).
Individuals with a family member or a spouse who were working in the medical field had significantly higher KSs (KS = 22.9) than others (KS = 21.5).
The effect of participants’ health conditions on their knowledge level was also studied, results showed that participants with hypertension, diabetes and heart problems had a significantly higher level of knowledge (KS = 23.0, 22.9 and 26.0, respectively) than others (KS = 21.5, 21.5 and 21.3, respectively). Notably, a family history of kidney problems among the participants had no significant effect on KS. The Eta-squared and the degree of freedom (df) values are added to to provide information about the strength of the relationship between the independent and dependent variables, in addition to the statistical difference, the Eta squared values also reflect the magnitude of the difference. The df measures the variability between groups.
The public knowledge description
The participants’ knowledge descriptions are shown in . The total KS for the participants was 21.7 out of 32 (65.9%), indicating an intermediate level of knowledge. We have further provided a description of CKD for each field. Results showed that participants had an excellent level of knowledge about CKD protective measures (KS = 4.3/5, 85.3%). Considering the kidney’s main function, CKD risk factors and CKD treatment, participants showed an intermediate level of knowledge KS = 2.7/5 (54.7%), 8.1/12 (67.6%) and 2.8/4 (68.7%), respectively. However, the participant’s knowledge of the CKD signs and symptoms was poor (KS = 3.8/6, 49.3%).
The public sources of knowledge about CKD
The participants’ sources of knowledge about the kidneys and CKD were evaluated. Results in and highlighted the most common sources of knowledge as follows: health-related professionals (38.3%), Internet and social media (37.8%), TV shows (37.1%) and books and magazines (21.8%). is Venn shape showing the number of participants who chose one or more sources of knowledge. Out of the 2181 participants who answered the survey, 1207 (55.34%) identified at least one source of knowledge about CKD. The largest share of these participants (271/1207, 22.45%) referred to all four different sources to gain information about CKD.
Table 3. The public source of knowledge about CKD.
The sources of knowledge that significantly affected the participants’ KS were books and magazines, followed by TV shows, health-related professionals, and to less extent the Internet and social media (KS = 25.3, 23.6, 23.5 and 22.0), respectively. The Eta-squared and the df values were also added to .
Multiple regression analysis of the public knowledge score
The date further analysed the relationship between KS and participant characteristics using multiple regression analysis. shows only the significant values (p < .05). Multivariate analysis found higher KS values associated with the age category of 50–64 years. Participants’ gender, employment status, educational field, income and smoking status were independently associated with higher KS. Educational level was also associated with higher KS. Having a family member or spouse working in the medical field was independently associated with higher KS. Interestingly, hypertension was independently associated with KS. Finally, the sources of knowledge about the kidney, such as TV shows, books and magazines, the Internet and social media, and health-related professionals were all independently associated with KS.
Table 4. Multiple regression analysis of public knowledge score and the participants’ baseline characteristics.
Discussion
The main goal of this study was to define knowledge gaps regarding CKD among the general population; hence, we evaluated the knowledge and awareness of the Jordanian community regarding CKD and its associated risk factors. This study is among the very few studies in Jordan that discuss the public knowledge of CKD. It is of great importance locally and globally because it provides an overview of the different fields of knowledge that the public needs to know in order to improve their knowledge about CKD. In addition, this study helps in the early diagnosis of CKD, participates in reducing CKD treatment costs, and minimizes quality of life disturbances. This study has advantages over previous studies because of its large population size, comprehensive and validated questionnaire, analytical approach, and results.
Herein, we found that the overall public knowledge about CKD was intermediate. Several determinants played a role in this knowledge, such as educational level and field, employment and marital status, income, and health issues including hypertension and diabetes.
Public knowledge of kidney function was intermediate. Participants demonstrated good knowledge regarding the role of the kidneys in cleaning the blood from toxins and turning waste products into urine, maintaining blood pressure, and maintaining the level of ions and salts in the blood. They had more correct answers compared to previous reports [Citation20,Citation26]. For example, 58.0% of the participants in our study correctly answered the role of kidneys in maintaining blood pressure compared to 26.4% reported in a previous study conducted in Australia [Citation20]. Nevertheless, our population sample had poor knowledge regarding the role of kidneys in maintaining healthy bones and CKD production; this result is in line with previous findings that showed only 14.3% of the general population correctly answered the role of kidneys in healthy bones [Citation20].
Overall, the respondents’ knowledge of CKD risk factors was intermediate. Our results showed that approximately 61% of the respondents correctly identified hypertension as a risk factor for CKD. This percentage was close to that reported one in South-West Nigeria, which was approximately 55% [Citation27], but higher than previous findings: 44% in Hong Kong [Citation28], 38% among the Australian population [Citation20], and only approximately 14% in the Iranian population [Citation29].
Diabetes was also reported as a risk factor for CKD; herein, 52% of the surveyors correctly identified diabetes as a risk factor for CKD, and this finding is consistent with the previous findings, with reported percentages ranging from 44 to 61% [Citation20,Citation27,Citation28].
Regarding the public knowledge of CKD symptoms, results showed poor knowledge and understanding of CKD symptoms, which highlights the importance of public health education in educating individuals susceptible to CKD about the symptoms and signs of CKD in the early stages and stress the importance of regular renal care counselling [Citation30,Citation31].
Public knowledge about CKD treatment was intermediate. Most of the participants knew that proper diet and healthy lifestyle might help slow down the progression of kidney disease. However, less know that medications that are used to treat chronic diseases such as high blood pressure and diabetes contribute to slowing down the progression of CKD [Citation32], and few knew that dialysis and transplantation are only needed when kidneys lose at least 85% of their function [Citation33]. This implies that public knowledge about CKD treatment needs to be improved, since individuals with adequate knowledge and understanding of CKD are more likely to follow their medical treatments [Citation34].
Interestingly, the overall public knowledge of the protective measures that protect the kidneys from CKD development was excellent. The majority of participants were aware that adopting a healthy lifestyle, drinking plenty of water to avoid dehydration, and limiting the intake of caffeinated beverages could protect the kidneys from developing CKD in the future [Citation35].
Our data showed that KSs were significantly lower among unemployed, less educated and low-income individuals than among employed, educated and high-income individuals. This result is consistent with a previous study from India, which showed a higher KS for CKD among employed and educated respondents [Citation36]. Furthermore, another study from Singapore reported that respondents with older age, lower educational status and lower monthly income were more likely to have limited knowledge about CKD [Citation37].
Individuals who are in contact with the health sector, such as having a first-degree relative working in the medical field or having chronic illnesses such as hypertension and diabetes, are more knowledgeable about CKD than others. This suggests that health education regarding CKD prevention and management is critical in targeting unemployed, less-educated and low-income individuals [Citation38,Citation39].
Lastly, according to our respondents, books and magazines were the main sources of knowledge about CKD, whereas the Internet and social media were the least. This indicated that either the shortness of such medical shows about CKD or people are not interested in watching these types of medical shows. Health-related professionals are highly encouraged to use social media and establish an information database to educate the public about the different aspects of CKD, which has to be in a simple and attractive way, and of course in different languages [Citation40].
National programs to educate the public about the association between unmanaged diabetes/hypertension and CKD could improve awareness of the disease, associated risk factors and consequences in susceptible individuals. In USA, Kidney Early Evaluation Program (KEEP) organized by the National Kidney Foundation targets individuals with diabetes and/or hypertension for educational programs and early CKD screening [Citation41,Citation42]. The participants in the KEEP were provided with adequate information regarding the association between hypertension/diabetes and CKD and encouraged to follow up with their clinicians for early detection, prevention and treatment of risk conditions. Follow-up studies showed that participation in KEEP was associated with significantly higher rates of pre-ESRD nephrologist care, peritoneal dialysis, pre-emptive transplant wait listing, transplantation, and with a lower risk for mortality, suggesting that kidney disease screening and education program were associated with higher rates of ESRD preparation and survival [Citation30,Citation31,Citation43].
The main strengths of this study are the large and diverse population sizes, which enable the generalizability of the study results. A well-structured questionnaire that covered the participants’ sociodemographic and health information and knowledge about CKD comprehensively participated in the research outcomes. The analytical approach followed to interpret the results was used to produce solid conclusions about public knowledge of CKD.
However, different types of bias, such as selection bias, recall bias and gender difference (males participants are more than females) have limited this study. Our study is a self-report study, which makes it susceptible to participants’ mood and state of feeling.
To summarize, the overall knowledge of the Jordanian public regarding CKD and its risk factors was intermediate, highlighting the importance of educating Jordanian populations and the necessity for healthcare providers to improve their communication with the public regarding CKD and its associated risk factors, especially diabetes and hypertension.
Conclusions
The level of knowledge and understanding of CKD and its associated risk factors are influenced by several determinants. Some health and social determinants positively influenced KS and knowledge levels. Health determinants include health conditions, educational field related to health, and having a first-degree relative work in the medical field. Social determinants include such as high educational level, high income, employment and marital status. Hence, participants with high qualifications, who are health-related, are more knowledgeable about CKD management than the rest. The current study findings demonstrate that developing health education to prevent CKD is crucial, and this will help healthcare providers and policymakers to pay more attention to understanding the extent of knowledge and attitude towards CKD and thus provide relevant education to patients and family members.
Author contributions
The author contributions to the paper are as follows: A.A.: conceptualization, investigation, writing the original draft, review and editing. E.A.: project administration, conceptualization, investigation, supervision, writing of original draft, review and editing. L.A.: wrote the original draft, reviewed and edited the manuscript. A.Q.: methodology, validation, review and editing. H.A.: statistical analysis and manuscript editing.
Ethical approval
This study was approved by the Institutional Review Board (IRB) Committee of the University of Jordan (Ref.: 19/2023/367), with no need for written consent for participation, which was optional. Participants provided verbal informed consent and they were informed earlier that participation was optional, and that all their information was confidential and would be used only for research purposes.
Consent form
According to the IRB committee regulations at the University of Jordan, written consent is only mandatory for studies involving sensitive information, such as patient data, and in the survey studies the participants consent is contained in their participation. Before participants could complete the questionnaire, they had to read an introductory paragraph outlining the study’s ethical guidelines. This included details about the study and a statement confirming the confidentiality of participants’ information, which would be used solely for research purposes, and they could proceed with the questionnaire only if they agreed to participate in the study.
Acknowledgements
The authors would like to thank Dr. Motaz Obeidat for evaluating the questionnaire as a nephrologist. Special thanks to Dr. Amani Alhadid for help in distributing the survey. All respects and gratitude to everyone who participated in this study for filling out the survey or distributing it.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data are available by the corresponding author upon request.
Additional information
Funding
References
- HFHS_CKD_V6.pdf; 2023 [Internet] [cited 2023 Mar 25]. Available from: https://www.asn-online.org/education/training/fellows/HFHS_CKD_V6.pdf
- Cockwell P, Fisher LA. The global burden of chronic kidney disease. Lancet. 2020;395(10225):662–664. doi: 10.1016/S0140-6736(19)32977-0.
- Khalil AA, Abed MA, Ahmad M, et al. Under-diagnosed chronic kidney disease in Jordanian adults: prevalence and correlates. J Ren Care. 2018;44(1):12–18. doi: 10.1111/jorc.12214.
- Alsuwaida AO, Farag YMK, Al Sayyari AA, et al. Epidemiology of chronic kidney disease in the Kingdom of Saudi Arabia (SEEK-Saudi investigators) – a pilot study. Saudi J Kidney Dis Transplant. 2010;21(6):1066–1072.
- Hosseinpanah F, Kasraei F, Nassiri AA, et al. High prevalence of chronic kidney disease in Iran: a large population-based study. BMC Public Health. 2009;9(1):44. doi: 10.1186/1471-2458-9-44.
- Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013;382(9888):260–272. doi: 10.1016/S0140-6736(13)60687-X.
- Jager KJ, Kovesdy C, Langham R, et al. A single number for advocacy and communication—worldwide more than 850 million individuals have kidney diseases. Kidney Int. 2019;96(5):1048–1050. doi: 10.1016/j.kint.2019.07.012.
- Snyder S. Detection and evaluation of chronic kidney disease. Chronic Kidney Dis. 2005;72(9):1723–1732.
- National_Registry_End_Stage_Renal_Disease_2013.pdf; 2023 [Internet] [cited 2023 Feb 19]. Available from: https://usjkamp.s3.amazonaws.com/prod_uploads/system/resources/attachments/000/000/321/original/National_Registry_End_Stage_Renal_Disease_2013.pdf?X-Amz-Algorithm=AWS4-HMAC-SHA256&X-Amz-Credential=AKIAJNKAKIDZBGBBOKQA/20230219/us-east-1/s3/aws4_request&X-Amz-Date=20230219T061539Z&X-Amz-Expires=10&X-Amz-SignedHeaders=host&X-Amz-Signature=9609746a5dcf1abd23e0db44412c02dead81ce2b81b6cabbeabbd59841404c9d
- Khader MI, Snouber S, Alkhatib A, et al. Prevalence of patients with end-stage renal disease on dialysis in the West Bank, Palestine. Saudi J Kidney Dis Transpl. 2013;24(4):832–837. doi: 10.4103/1319-2442.113913.
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–171.
- Thurlow JS, Joshi M, Yan G, et al. Global epidemiology of end-stage kidney disease and disparities in kidney replacement therapy. Am J Nephrol. 2021;52(2):98–107. doi: 10.1159/000514550.
- 12th_annual_report_esrd_2019.pdf; 2023 [Internet] [cited 2023 Feb 19]. Available from: https://www.moh.gov.jo/ebv4.0/root_storage/en/eb_list_page/12th_annual_report_esrd_2019.pdf
- Khalil A, Abdalrahim M. Knowledge, attitudes, and practices towards prevention and early detection of chronic kidney disease. Int Nurs Rev. 2014;61(2):237–245. doi: 10.1111/inr.12085.
- Khalil AA, Al-Modallal HM, Abdalrahim MS, et al. Development and psychometric evaluation of the Chronic Kidney Disease Screening Index. Ren Fail. 2014;36(8):1200–1207. doi: 10.3109/0886022X.2014.928969.
- Devins GM, Hollomby DJ, Barré PE, et al. Long-term knowledge retention following predialysis psychoeducational intervention. Nephron. 2000;86(2):129–134. doi: 10.1159/000045730.
- Ragnarson Tennvall G, Apelqvist J. Health-related quality of life in patients with diabetes mellitus and foot ulcers. J Diabetes Complications. 2000;14(5):235–241. doi: 10.1016/s1056-8727(00)00133-1.
- Stanifer JW, Karia F, Voils CI, et al. Development and validation of a cross-cultural knowledge, attitudes, and practices survey instrument for chronic kidney disease in a Swahili-speaking population. PLOS One. 2015;10(3):e0121722. doi: 10.1371/journal.pone.0121722.
- Magacho EJC, Ribeiro LC, Chaoubah A, et al. Adherence to drug therapy in kidney disease. Braz J Med Biol Res. 2011;44(3):258–262. doi: 10.1590/S0100-879X2011007500013.
- Gheewala PA, Peterson GM, Zaidi STR, et al. Public knowledge of chronic kidney disease evaluated using a validated questionnaire: a cross-sectional study. BMC Public Health. 2018;18(1):371. doi: 10.1186/s12889-018-5301-4.
- Sperber A, DeVellis R, Boehlecke B. Cross-cultural translation. J Cross Cult Psychol. 1994;25(4):501–524. doi: 10.1177/0022022194254006.
- Sample Size Calculator by Raosoft, Inc.; 2020 [Internet] [cited 2020 Jun 24]. Available from: http://www.raosoft.com/samplesize.html
- Figueroa JL, Mahmoud M, Breisinger C. The role of agriculture and agro-processing for development in Jordan. International Food Policy Research Institute (IFPRI); 2018 [Internet] [cited 2024 Apr 18]. Available from: https://ebrary.ifpri.org/digital/collection/p15738coll2/id/132262
- Yusof A, Chia YC, Hasni YM. Awareness and prevalence of mammography screening and its predictors – a cross sectional study in a primary care clinic in Malaysia. Asian Pac J Cancer Prev. 2014;15(19):8095–8099. doi: 10.7314/apjcp.2014.15.19.8095.
- von EE, Altman DG, Egger M, et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808.
- Stanifer JW, Turner EL, Egger JR, et al. Knowledge, attitudes, and practices associated with chronic kidney disease in Northern Tanzania: a community-based study. PLOS One. 2016;11(6):e0156336. doi: 10.1371/journal.pone.0156336.
- Oluyombo R, Ayodele OE, Akinwusi PO, et al. Awareness, knowledge and perception of chronic kidney disease in a rural community of South-West Nigeria. Niger J Clin Pract. 2016;19(2):161–169. doi: 10.4103/1119-3077.175960.
- Chow K, Szeto C, Kwan BC, et al. Public lacks knowledge on chronic kidney disease: telephone survey. Hong Kong Med J. 2014;20(2):139–144.
- Roomizadeh P, Taheri D, Abedini A, et al. Limited knowledge of chronic kidney disease and its main risk factors among Iranian community: an appeal for promoting national public health education programs. Int J Health Policy Manag. 2014;2(4):161–166. doi: 10.15171/ijhpm.2014.37.
- Almomani EY, Jarrar W, Alhadid A, et al. Shedding light on pharmacists’ knowledge of kidney stones’ etiology and treatment. Pharm Pract. 2022;20(3):1–10. doi: 10.18549/PharmPract.2022.3.2712.
- Kurella Tamura M, Li S, Chen S-C, et al. Educational programs improve the preparation for dialysis and survival of patients with chronic kidney disease. Kidney Int. 2014;85(3):686–692. doi: 10.1038/ki.2013.369.
- Hahr AJ, Molitch ME. Management of diabetes mellitus in patients with chronic kidney disease. Clin Diabetes Endocrinol. 2015;1(1):2. doi: 10.1186/s40842-015-0001-9.
- living-with-kidney-failure-kidney-health-australia-publication.pdf; 2023 [Internet] [cited 2023 Mar 8]. Available from: https://kidney.org.au/uploads/resources/living-with-kidney-failure-kidney-health-australia-publication.pdf
- Swartz MD, Robinson K, Davy T, et al. The role of patients in the implementation of the National Kidney Foundation-Dialysis Outcomes Quality Initiative. Adv Ren Replace Ther. 1999;6(1):52–58. doi: 10.1016/s1073-4449(99)70008-7.
- Clark WF, Huang S-H, Garg AX, et al. The chronic kidney disease water intake trial: protocol of a randomized controlled trial. Can J Kidney Health Dis. 2017;4:2054358117725106. doi: 10.1177/2054358117725106.
- Tiwari P. Assessment of public knowledge and attitude towards chronic kidney disease by using a validated questionnaire: an observational study. Biomed J Sci Techn Res. 2022;41(5). doi: 10.26717/BJSTR.2022.41.006662.
- Chow WL, Joshi VD, Tin AS, et al. Limited knowledge of chronic kidney disease among primary care patients – a cross-sectional survey. BMC Nephrol. 2012;13(1):54. doi: 10.1186/1471-2369-13-54.
- Narva AS, Norton JM, Boulware LE. Educating patients about CKD: the path to self-management and patient-centered care. Clin J Am Soc Nephrol. 2016;11(4):694–703. doi: 10.2215/CJN.07680715.
- Li PK-T, Garcia-Garcia G, Lui S-F, et al. Kidney health for everyone everywhere – from prevention to detection and equitable access to care. Braz J Med Biol Res. 2020;53(3):e9614. doi: 10.1590/1414-431X20209614.
- Goldstein K, Briggs M, Oleynik V, et al. Using digital media to promote kidney disease education. Adv Chronic Kidney Dis. 2013;20(4):364–369. doi: 10.1053/j.ackd.2013.04.001.
- Ohmit SE, Flack JM, Peters RM, et al. Longitudinal study of the National Kidney Foundation’s (NKF) Kidney Early Evaluation Program (KEEP). J Am Soc Nephrol. 2003;14(7 Suppl. 2):S117–S121. doi: 10.1097/01.asn.0000070155.63971.b2.
- Vassalotti JA, Li S, Chen SC, et al. Screening populations at increased risk of CKD: the Kidney Early Evaluation Program (KEEP) and the public health problem. Am J Kidney Dis. 2009;53(3 Suppl. 3):S107–S114. doi: 10.1053/j.ajkd.2008.07.049.
- Whaley-Connell AT, Vassalotti JA, Collins AJ, et al. National Kidney Foundation’s Kidney Early Evaluation Program (KEEP) annual data report 2011: executive summary. Am J Kidney Dis. 2012;59(3 Suppl. 2):S1–S4. doi: 10.1053/j.ajkd.2011.11.018.