
Abstract
Background. Aspirin has been used for secondary prevention of myocardial infarction (MI) in individuals with coronary disease. Although supported by several large controlled trials, aspirin prevents only a portion of recurrent events.
Aim and method. We set out to study the prevalence of long-term aspirin use prior to admission for MI and its significance for medium-term event-free survival; 998 consecutive patients with acute MI admitted to a tertiary center were included in the study.
Results. Nearly half (42.4%) of all patients reported long-term use of low-dose aspirin prior to the index event. Prior aspirin use was associated with a 50% increase in the risk of both the combined end point of recurrent unstable angina, recurrent myocardial infarction, stroke, or death (OR 1.49; 95% CI 1.12–2.00, P=0.006) and mortality (OR 1.50; 95% CI 1.03–2.17, P=0.03) during 10-month follow-up. Prior aspirin use was not associated with an increased frequency of added antithrombotic therapy at discharge.
Conclusions. We have found that prior aspirin use is common in patients hospitalized for acute MI. Individuals already on aspirin had increased risk of recurrent ischemic events and all-cause mortality during the 10-month follow-up after their index MI.
Introduction
Aspirin has been a mainstay of antithrombotic therapy both in the setting of acute coronary events and in the long-term secondary prevention of recurrent ischemic events. Even though supported by a wide range of studies in these clinical situations, the absolute reduction in the risk of events produced by aspirin therapy is still relatively small. Low expenses and widespread acceptance of the drug have made it widely used for prevention of arterial thrombosis Citation1.
Recently, the term ‘aspirin resistance’ has been introduced. This can be divided into two concepts: biochemical resistance and clinical resistance. Biochemical aspirin resistance has mainly been defined in vitro by failure of aspirin to suppress blood clotting in various assays Citation2, Citation3. Aspirin resistance has been prospectively associated with increased risk of cardiovascular events during follow-up in a single small study of patients with stable coronary artery disease (CAD) Citation4. The frequency of biochemically measured aspirin failure ranges from 5%–20% among individuals with stable CAD up to 50%–60% among patients with acute coronary syndrome (ACS). Two small studies on ACS patients have linked biochemical aspirin resistance to clinical end points Citation5, Citation6.
Individuals having cardiovascular events while on long-term aspirin treatment have been labeled clinically ‘aspirin resistant’. By this clinical definition, a large portion of individuals having recurrent cardiovascular events are termed aspirin resistant, since approximately half of patients with acute coronary events are already on aspirin in recent clinical trials Citation7, Citation8. This clinical situation should be correctly termed aspirin failure since aspirin is likely to be a single small factor in the prevention of cardiovascular events. Even though such individuals usually have a less severe presentation of their coronary event (more often unstable angina pectoris (UA) than myocardial infarction (MI), and mostly non-ST-elevation myocardial infarction (NSTEMI)), they have been reported to be at an increased risk of recurrent events/death during short-term follow-up in selected populations Citation9–11.
Key messages
Prior aspirin use is common among individuals admitted for an acute myocardial infarction.
Prior aspirin use is associated with an increased risk of major adverse cardiac event (MACE) and mortality during medium-term follow-up despite revascularization and secondary prevention.
Abbreviations
We set out to study the prevalence of prior aspirin use and its significance for long-term recurrent cardiovascular events and mortality in a series of nearly 1000 consecutive patients with acute MI (all-comers) from Tampere University Hospital.
Material and methods
Patient series
A total of 998 consecutive patients with acute MI admitted to the Tampere University hospital from 1 January 2002 to 30 March 2003 were enrolled. The mean age of patients was 71.6 years, and 57.6% were men. The frequencies of basic characteristics are given in and . More detailed characteristics have been previously published Citation12.
Table I. Characteristics of the study population at admission.
Table II. Medications at admission.
ECG analysis
An electrocardiogram (ECG) recorded in the emergency department, in the ambulance, or at the referring health center showing the maximal ischemic changes was chosen for analysis. ST-segment deviation from the isoelectric line, determined by drawing a line between subsequent PQ segments, was considered elevated or depressed if it was 0.5 mm or more above or below the isoelectric line, respectively. The type of MI was categorized based on the presenting ECGs. ST-elevation myocardial infarction (STEMI) was present if ST-segment elevation was present in two contiguous leads: in leads V1-6≥1.5 mm with ≥2 mm in at least one lead; in leads II, III, aVF, I and aVL ≥ 1 mm.
Troponin
Blood samples for troponin I (cTnI) were collected at baseline and after 6–12 hours. The normal value for cTnI in our hospital is < 0.2 µg/L (ACS:180, Bayer Diagnostics, Tarrytown, New York). Values above 0.2 µg/L together with accompanying ECG changes/symptoms were considered diagnostic for MI.
ACS categories
Patients with STEMI had elevated cTnI levels and fulfilled the above-mentioned ECG criteria. Patients with NSTEMI had elevated cTnI levels, but did not fulfill ECG criteria for STEMI. Patients with left bundle branch block and elevated troponin levels were categorized as having NSTEMI. The final diagnosis of the patients was verified from patient charts, and patients with myocarditis, pulmonary embolism, or septic shock as the cause of elevated cTnI were excluded from analyses. UA was defined as chest pain or ischemic symptoms lasting more than 5 minutes with documented characteristic ECG changes and without elevated cTnI levels detected during 12-hour follow-up.
Data questionnaire
The following variables were registered: baseline demographic variables, medication at hospital arrival, Canadian Cardiac Society (CCS) and New York Heart Association (NYHA) functional class before the acute phase, serum creatinine, C-reactive protein (twice with a 6–12 h interval), blood lipids, blood pressure at arrival, type of reperfusion therapy, in-hospital events (UA, stroke, reinfarction, resuscitation, and death), medication during hospital stay, ejection fraction by echocardiography, angiography, percutaneous coronary intervention (PCI), or bypass surgery during hospital stay. In coronary angiography >50% stenoses were considered significant.
A study nurse contacted all living patients by telephone to collect follow-up data. Causes of death were registered from official mortality statistics. Patient follow-up ended in case of death or at the time of the phone call by the study nurse. Median follow-up was 285 days (174–313 d). Two patients were lost from follow-up. Events collected during follow-up were defined as MI (as described above), stroke, death, and re-hospitalization for UA. Events during follow-up were confirmed from patient charts.
Stroke was defined as the presence of a new local neurologic deficit thought to be vascular in origin with signs or symptoms lasting more than 24 hours. It was further divided to ischemic, hemorrhagic, or unknown based on the results of computed tomographic scans.
All patients gave written consent for study participation. The study was approved by the Ethical Committee of Tampere University Hospital.
Statistical analyses
Categorical variables were expressed as numbers of patients or percent and continuous variables as medians (inter-quartile range). Proportions were compared with the chi-square test or Fisher's exact test, and quantitative data were compared with the Mann-Whitney test. A probability value of <0.05 was considered statistically significant. Comparison between groups was performed using log rank statistics. Cox regression was used to test the prognostic significance of baseline and in-hospital variables concerning mortality and recurrent events at follow-up. The following variables were included in the multivariate model: all traditional risk factors for CAD, medication at admission and at discharge, the type of MI, prior MI or revascularization procedures, and revascularization during current hospitalization. The following variables were not used because of lack of data for a significant proportion of patients: blood lipids, coronary angiographic findings, and ejection fraction. Hazard ratios were presented. A stepwise backward elimination method was used to perform variable selection in the multivariate Cox regression analysis each time excluding the one variable with the highest P-value. Variables with a P<0.05 were included in the final model. All calculations were performed with the SPSS 10.0 statistical package.
Results
In total 998 patients with MI were included. Of these, 40.7% were on aspirin, 9.9% on warfarin, 1% on combined aspirin and warfarin, and 0.7% on clopidogrel or combined clopidogrel and aspirin on admission. Long-term use of low-dose aspirin prior to the index event was reported by 423 (42.4%). Of the 423 individuals with prior aspirin, 4% were also on warfarin during admission as opposed to 17% of the 575 individuals without prior aspirin (P < 0.0001). Clopidogrel was used by 0.9% of prior aspirin users versus 0.4% of prior nonusers (P = NS). Distribution of different antithrombotic regimens at admission and characteristics of each group are displayed in . Aspirin dose was not recorded but 100 mg daily is by far the most common dose used in Finland.
Table III. Antithrombotic drugs at admission.
A total of 44.3% presented with STEMI and 55.7% with NSTEMI; 45.2% of patients with STEMI received fibrinolytic therapy; primary PCI was not available in our institute during the study years. Of individuals with NSTEMI, 87.6% were treated with low-molecular weight heparin (LMWH) and 23.4% with GPIIb/IIIa inhibitors. Among individuals with STEMI, aspirin was used prior to admission by 34.8% compared to 48.4% of individuals with NSTEMI (P < 0.0001). In addition, individuals with STEMI were younger, less often diabetics, more often male and smokers compared to individuals with NSTEMI (data not shown).
Medications at discharge
A total of 95.0% of individuals in the group with aspirin prior to hospitalization, versus 84.8% of individuals without prior aspirin use (P < 0.0001), were discharged on aspirin. Prior aspirin users were also more often discharged on nitrates and calcium channel blockers. Discharge medication is shown in .
Table IV. Drugs at discharge by aspirin use status prior to admission.
A total of 94.1% of patients with STEMI were discharged on aspirin compared to 85.1% of individuals with NSTEMI; 17.4% of individuals with STEMI were discharged on warfarin compared to 10.2% of individuals with NSTEMI (P < 0.01); and 31.4% of patients with STEMI had clopidogrel started during hospitalization compared to 15.7% of patients with NSTEMI (P < 0.001).
A total of 43.5% of patients underwent coronary angiography during the index hospitalization. PCI was performed on 16.5% and coronary artery by-pass surgery on 9.8% of patients during the index hospitalization. Of patients undergoing PCI during the index hospitalization 90.3% were discharged on clopidogrel, 97.6% on aspirin and 20.6% on warfarin. Those not having PCI were discharged on clopidogrel in 9.7% of cases, on aspirin in 87.4% of cases, and on warfarin in 25.6% of cases.
Combined end point
In total 47.5% of individuals on aspirin prior to the index event reached the combined end point of recurrent UA/MI, stroke or death due to any cause during the 10-month follow-up compared to 35.1% of individuals without prior aspirin use (multivariate P = 0.006 and OR 1.49; 95% CI 1.12–2.00) (). Other significant variables related to the risk (increased or decreased) of combined recurrent events included current smoking, age, creatinine levels, PCI during hospitalization, and beta-blocker, diuretic, and statin use at discharge. Other medications, interventions, or risk factors did not correlate with the combined recurrent events end point.
Figure 1. Survival free from combined end point during follow-up according to admission aspirin (ASA) use status (P = 0.006).
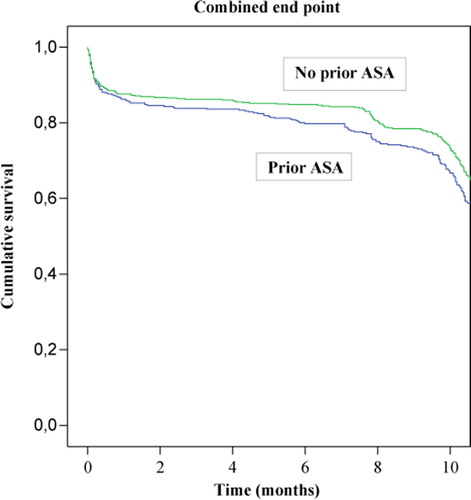
Both sexes seemed to be affected equally, whereas there was a trend (P for MI type by aspirin interaction 0.065) for prior aspirin use to be associated with the combined end point among individuals with NSTEMI (P = 0.016, OR 1.54) but not among individuals with STEMI (P = 0.32, OR 1.30).
When data analysis was restricted to those 477 (47.8%) patients with data on ejection fraction, prior aspirin users still had a higher risk (P = 0.01) of combined end point (OR 1.72; 95% CI 1.14–2.63). Prior aspirin use was associated with an increased risk of combined end point among individuals without prior MI (n=668) (OR 1.67; 95% CI 1.16–2.38, P = 0.005), but not among those (n=211) patients with prior MI (OR 0.59, P = 0.11).
Mortality
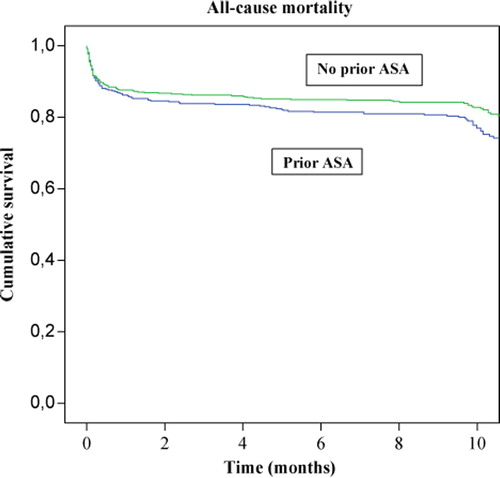
A total of 28.1% of individuals on aspirin prior to the index event died during the 10-month follow-up compared to 21.5% of those not on aspirin (multivariate P = 0.03 and OR 1.50; 95% CI 1.03–2.17) (). Other variables related to 10-month mortality included current smoking, creatinine levels, age, and beta-blocker, diuretic, and statin use at discharge. Both individuals with STEMI and NSTEMI seemed to be affected equally whereas there was a trend (P for sex by aspirin interaction 0.057) for prior aspirin use to be associated with mortality among women (P = 0.02, OR 1.85) but not among men (P = 0.6, OR 1.22).
Figure 2. Survival during follow-up according to admission aspirin (ASA) use status (P = 0.03).
When data analysis was restricted to those 477 (47.8%) patients with data on ejection fraction, prior aspirin users still tended to have a higher risk (P = 0.07) of death (OR 1.75; 95% CI 0.97–3.0). Prior aspirin use was associated with an increased risk of death among individuals without prior MI (n=668) (OR 1.54; 95% CI 1.00–2.33, P = 0.05), but not among those (n = 211) patients with prior MI (OR 1.03, P = 0.9).
Discussion
In this prospective series of 998 consecutive MI patients, we have found that aspirin use prior to admission predicts future adverse coronary events despite contemporary therapies and interventions administered during or after hospitalization. This was especially true for individuals without prior MI. In addition, prior aspirin use did not lead to the prescription of additional antithrombotic/anticoagulant drugs for secondary prevention.
Aspirin resistance/failure has been described in a high number of individuals with ACS. Clinical trials on NSTEMI have shown up to 60%–70% of patients are on prior aspirin at the time of hospital admission. Patients more often presented with UA as opposed to MI if they were on aspirin. Previous studies with selected patient series also imply that prior aspirin use could be associated with an inferior prognosis during short- and medium-term follow-up Citation7–11, Citation13 even though contradicting data have also been published Citation14. Prior aspirin use has been incorporated in the Thrombolysis In Myocardial Infarction (TIMI) risk score which can be used to evaluate the prognosis of an ACS patient.
Several reasons for aspirin resistance or failure have been suggested. However, the problem seems to be multietiological. An important issue is noncompliance which has been estimated to occur in 10%–20% of patients. Diabetes and obesity have also been implicated. Recreational NSAID use, female sex, and even the form of aspirin (entero-coated versus regular) have been brought up. In addition, genetic variation in platelet receptors and COX-1 itself has been studied in this context Citation2, Citation3, Citation15, Citation16. We have previously found that biochemical aspirin resistance in stable CAD is associated with COX-1 gene variation, female sex, and platelet GPVI gene variation as well as history of previous MI Citation17. Kottke-Marchant et al. also suggested aspirin nonresponse to be especially prevalent among individuals with prior MI Citation18.
Our findings imply that individuals with prior aspirin use at the time of MI have an impaired long-term prognosis independent of invasive treatment and secondary preventive measures. Aspirin failure in this study population which was drawn immediately after the publication of the CURE study Citation7 did not result in added antithrombotic regimen (clopidogrel or warfarin) among patients already on aspirin.
What to do with an individual with MI while on aspirin? Since these individuals are at high risk for future events, invasive coronary assessment and aggressive secondary prevention seem reasonable. Regarding antithrombotic treatment, no large-scale randomized data supporting the increase of aspirin dose exists. In fact, a large meta-analysis on different aspirin doses for secondary prevention implied no differences in the risk reduction of recurrent events between doses of 81 mg or 325 mg daily Citation1. One nonrandomized paper suggested that higher aspirin doses might be beneficial Citation19.
What about clopidogrel? Data exist for ACS patients from the CURE trial and especially from the PCI-CURE and the CREDO trials on individuals treated with PCI Citation20, Citation21. However, these studies only include patients with NSTEMI. The recently published COMMIT-2 Citation22 does not specifically address the issue of long-term clopidogrel therapy and its results can hardly be extrapolated to the context of aspirin failure. Adding warfarin to aspirin, however, has been shown to dramatically reduce recurrent events after MI in large randomized trials Citation23, Citation24. These trials have also included individuals with STEMI.
We also found that individuals with STEMI were less often on aspirin prior to admission as opposed to NSTEMI, which corroborates prior findings Citation25. This might reflect the effect of aspirin in blocking the formation of occlusive thrombi or that individuals with aspirin have had more time to develop more severe coronary disease which expresses itself as NSTEMI rather than a sudden thrombotic occlusion of a coronary artery. Prior aspirin users could be biased towards more hospitalization for UA since calcium channel blockers and nitrates were more often prescribed to those patients at discharge, possibly due to more extensive underlying CAD.
High end point rates observed in our trial are similar to other ‘real-life’ all-comers studies Citation26, Citation27 and discussed in our previous paper Citation12. This is due to inclusion of patients with advanced age, severe comorbidities, and/or cardiogenic shock. Even though adherence to class I recommendations has been significantly improved after the initial release of the guidelines for ACS, further improvements are needed for optimal implementation of these guidelines in many hospitals. Our study patients were recruited when the implementation of these guidelines was beginning to affect patient care, which explains still quite low use of evidence-based therapies. However, ‘real-life’ patients are for the most part not comparable to clinical trial patients due to their comorbidities and contraindications for certain treatments. Thus we believe the results are applicable to patient care in many centers despite the improving use of evidence-based treatment Citation28.
Limitations of the present work include the lack of biochemical measurements of aspirin failure, the fact that coronary angiography was performed on only half of the patients with the possibility of a bias for more severe disease in prior aspirin users. This was mainly due to advanced age and comorbidities as well as limited invasive services. Nonadherence to aspirin prior to admission is a possible confounder and was not assessed in the study. Also multiple tests for interactions (sex, ejection fraction, and prior MI in relation to aspirin use) are subjectible to bias and should be interpreted with caution.
In this large population of 998 consecutive patients with acute MI, we have found that long-term aspirin use prior to admission was associated with an impaired medium-term prognosis after the index event. This finding implies that individuals with prior aspirin use before MI represent a high-risk population in need of an aggressive therapeutic approach during and after hospitalization for their coronary event.
References
- Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002; 324: 71–86
- Hennekens CH, Schror K, Weisman S, Fitzgerald GA. Terms and Conditions: Semantic complexity and aspirin resistance. Circulation. 2004; 110: 1706–8
- Cattaneo M. Aspirin and clopidogrel. Efficacy, safety and the issue of drug resistance. Arterioscler Thromb Vasc Biol. 2004; 24: 1–8
- Gum PA, Kottke-Marchant K, Welsh PA, White J, Topol EJ. A prospective, blinded determination of the natural history of aspirin resistance among stable patients with cardiovascular disease. J Am Coll Cardiol. 2003; 41: 961–5
- Pamukcu B, Oflaz H, Oncul A, Umman B, Mercanoglu F, Ozcan M, et al. The role of aspirin resistance on outcome in patients with acute coronary syndrome and the effect of clopidogrel therapy in the prevention of major cardiovascular events. J Thromb Thrombolysis. 2006; 22: 103–10
- Hobikoglu GF, Norgaz T, Aksu H, Ozer O, Erturk M, Destegul E, et al. The effect of acetylsalicylic acid resistance on prognosis of patients who have developed acute coronary syndrome during acetylsalicylic acid therapy. Can J Cardiol. 2007; 23: 201–6
- Yusuf S, Zhao F, Mehta SR, Chloravicius S, Tognoni G, Fox KK. Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001; 345: 494–502
- Antman EM, McCabe CH, Gurfinkel EP, Turpie AG, Bernink PJ, Saleim D, et al. Enoxaparin prevents death and cardiac ischemic events in unstable angina/non-Q-wave myocardial infarction. Results of the thrombolysis in myocardial infarction (TIMI) 11B trial. Circulation. 1999; 100: 593–601
- Alexander JH, Harrington RA, Tuttle RH, Berdan LG, Lincoff AM, Deckers JW, et al. Prior aspirin use predicts worse outcomes in patients with non-ST-elevation acute coronary syndromes. Pursuit Investigators. Am J Cardiol. 1999; 83: 1147–51
- Lancaster GI, Lancaster CJ, Radley D, Cohen M. Prior aspirin use in unstable angina predisposes to higher risk: the aspirin paradox. Int J Cardiol. 2001; 80: 201–7
- Collet JP, Montalescot G, Blanchet B, Tanguy ML, Golmard JL, Choussat R, et al. Impact of prior use or recent withdrawal of oral antiplatelet agents on acute coronary syndromes. Circulation. 2004; 110: 2361–7
- Nikus KC, Eskola MJ, Virtanen VK, Harju J, Huhtala H, Mikkelsson J, et al. Mortality of patients with acute coronary syndrome still remains high: a follow-up study of 1188 consecutive patients admitted to a university hospital. Ann Med. 2007; 39: 63–71
- Cohen M, Adams PC, McBride R, Blanke H, Fuster V. Prospective comparison of patient characteristics and outcome of non-prior aspirin users versus aspirin users with unstable angina or non-Q-wave myocardial infarction treated with combination antithrombotic therapy. J Thromb Thrombolysis. 1997; 4: 275–80
- Portnay EL, Foody JM, Rathore SS, Wang Y, Masoudi FA, Curtis JP, et al. Prior aspirin use and outcomes in elderly patients hospitalized for acute myocardial infarction. J Am Coll Cardiol. 2005; 46: 967–74
- Maree AO, Fitzgerald DJ. Aspirin and coronary artery disease. Thromb Haemost. 2004; 92: 1175–81
- Maree AO, Curtin RJ, Chubb A, Dolan C, Cox D, O'Brien J, et al. Cyclo-oxygenase 1 haplotype modulates platelet response to aspirin. J Thromb Haemost. 2005; 3: 2340–5
- Lepantalo A, Mikkelsson J, Resendiz JC, Viiri L, Backman JT, Kankuri E, et al. Polymorphisms of COX-1 and GPVI associate with the antiplatelet effect of aspirin in coronary artery disease patients. Thromb Haemost. 2006; 95: 253–9
- Kottke-Marchant K, Murugesan G, Gerber C, Chisolm GM, Moliterno DJ, Topol EJ, , et al. High prevalence of aspirin resistance in patients with a history of myocardial infarction. J Thromb Haemostasis 2003;1 (Suppl 1),OC243.
- Quinn MJ, Aronow HD, Califf RM, Bhatt DL, Sapp S, Kleiman NS, et al. Aspirin dose and six-month outcome after an acute coronary syndrome. J Am Coll Cardiol. 2004; 43: 972–8
- Mehta SR, Yusuf S, Peters RJ, Bertrand ME, Lewis BS, Natarajan MK, et al. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study. Lancet. 2001; 358: 527–33
- Steinhubl SR, Berger PB, Mann JT 3rd, Fry ET, Delago A, Wilmer C, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomised controlled trial. JAMA. 2002; 288: 2411–20
- Chen ZM, Jiang LX, Chen YP, Xie JX, Pan HC, Peto R, et al. Addition of clopidogrel to aspirin in 42,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet. 2005; 366: 1607–21
- Hurlen M, Abdelnoor M, Smith P, Erikssen J, Arnesen H. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002; 347: 969–74
- Van Es RF, Jonker JJ, Verheugt FW, Deckers JW, Grobbee DE. Aspirin and coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet. 2002; 360: 109–13
- Kennon S, Barakat K, Suliman A, MacCallum PK, Ranjadayalan K, Wilkinson P, et al. Influence of previous aspirin treatment and smoking on the electrocardiographic manifestations of injury in acute myocardial infarction. Heart. 2000; 84: 41–5
- Bjorklund E, Lindahl B, Stenestrand U, Swahn E, Dellborg M, Pehrsson K, et al. Outcome of ST-elevation myocardial infarction treated with thrombolysis in the unselected population is vastly different from samples of eligible patients in a large-scale clinical trial. Am Heart J. 2004; 148: 566–73
- Terkelsen CJ, Lassen JF, Norgaard BL, Gerdes JC, Jensen T, Gotzsche LB, et al. Mortality rates in patients with ST-elevation vs. non-ST-elevation acute myocardial infarction: observations from an unselected cohort. Eur Heart J. 2005; 26: 18–26
- Mehta RH, Roe MT, Chen AY, Lytle BL, Pollack CV, Jr, Brindis RG, et al. Recent trends in the care of patients with non-ST-segment elevation acute coronary syndromes: insights from the CRUSADE initiative. Arch Intern Med. 2006; 166: 2027–34
