
Abstract
Endothelial dysfunction (ED) in the setting of cardiovascular risk factors such as hypercholesterolemia, hypertension, diabetes mellitus, chronic smoking as well as in patients with heart failure has been shown to be at least in part dependent on the production of reactive oxygen species (ROS) such as superoxide and the subsequent decrease in vascular bioavailability of nitric oxide (NO). Methods to quantify endothelial dysfunction include forearm plethysmography, flow‐dependent dilation of the brachial artery, finger‐pulse plethysmography, pulse curve analysis, and quantitative coronary angiography after intracoronary administration of the endothelium‐dependent vasodilator acetylcholine. Superoxide sources include the NADPH oxidase, xanthine oxidase, and mitochondria. Superoxide produced by the NADPH oxidase may react with NO released by the endothelial nitric oxide synthase (eNOS) thereby generating peroxynitrite (ONOO−), leading to eNOS uncoupling and therefore eNOS‐mediated superoxide production. The present review will discuss current concepts of how to assess endothelial function, prognostic implications of ED, mechanisms underlying ED with focus on oxidative stress and circulating biomarkers, which have been proposed to indicate endothelial dysfunction and/or damage, respectively.
Introduction
Traditionally, the role of the endothelium was thought primarily to be that of a selective barrier to the diffusion of macromolecules from the vessel lumen to the interstitial space. During the past 20 years, numerous additional roles for the endothelium have been defined, such as regulation of vascular tone, modulation of inflammation, promotion as well as inhibition of vascular growth, and modulation of platelet aggregation and coagulation (). Endothelial dysfunction is a characteristic feature of patients with coronary atherosclerosis, and more recent studies indicate that it may predict long‐term atherosclerotic disease progression as well as cardiovascular event rate Citation1. Although the mechanisms underlying endothelial dysfunction may be multifactorial, there is a growing body of evidence that increased production of reactive oxygen species (ROS) may contribute considerably to this phenomenon. ROS production has been demonstrated to occur in the endothelial cell layer and also within the media and adventitia, all of which may impair NO signaling within vascular tissue to endothelium‐dependent but also endothelium‐independent vasodilators. More recent experimental but also clinical studies point to the pathophysiological importance of the xanthine oxidase, the vascular NADPH oxidase, mitochondria, and an uncoupled endothelial nitric oxide as significant enzymatic superoxide sources (). This review will briefly address mechanisms underlying endothelial dysfunction with focus on oxidative stress; we will discuss which method may be suited to assess endothelial function in the clinics, and we will discuss the prognostic implications of endothelial dysfunction as well as therapeutic strategies to improve endothelial dysfunction by reducing oxidative stress.
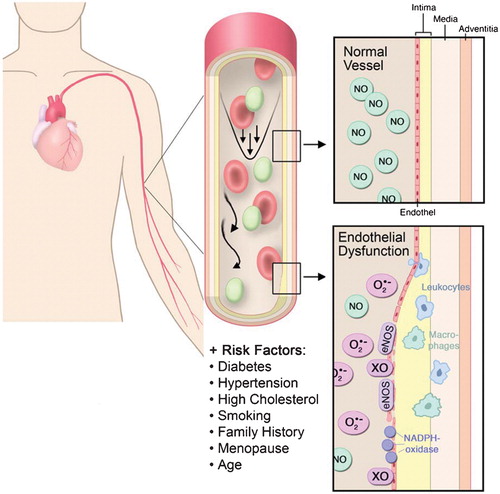
Figure 1 Mechanisms underlying endothelial dysfunction and the functional consequences of decreased vascular bioavailability of nitric oxide(NO). In the presence of cardiovascular risk factors such as hypertension, diabetes mellitus, smoking, age, menopause, familiar history of cardiovascular disease and hypercholesterolemia, vascular superoxide‐producing enzymes such as the vascular NADPH oxidase, the xanthine oxidase (XO), and an uncoupled endothelial nitric oxide synthase (eNOS) produce large amounts of superoxide (O2·−), which will metabolize NO. The consequences are adhesion and infiltration of the vascular wall with inflammatory cells such as macrophages and neutrophils and a subsequent intima proliferation.
Key messages
Endothelial dysfunction is largely due to increased production of reactive oxygen species such as superoxide, which will decrease vascular bioavailability of nitric oxide (NO).
Endothelial dysfunction can be assessed in coronary and peripheral arteries and/or arterioles in the clinics via intracoronary or intrabrachial infusion of the endothelium‐dependent vasodilator acetylcholine and by more noninvasive techniques, such as flow‐mediated dilation of the brachial artery, by finger‐pulse plethysmography and by pulse curve analysis.
Coronary and peripheral endothelial dysfunction has been shown to have prognostic implications in patients with established stable coronary artery disease, essential hypertension, and in patients with acute coronary syndrome and peripheral artery disease.
The PREVENT‐it trial is the worldwide largest trial to check whether endothelial function assessment may help to risk‐stratify healthy subjects with respect to their cardiovascular risk.
The L‐arginine/NO/cGMP pathway in vascular tissue
The endothelium, a single‐layered continuous cell sheet lining the luminal vessel wall, separates the intravascular (blood) from the interstitial compartment and the vascular smooth muscle. Based on cell count (6×1013), mass (1.5 kg), and surface area (1000 m2) the endothelium is an autonomous organ. Though for a long time regarded as a passive barrier for blood cells and macrosolutes, this view completely changed with the advent of endothelial autacoids like prostacyclin (PGI2) Citation2 and nitric oxide (NO) Citation3, as well as with the discovery of integrins and other surface signals Citation4. It is now evident that the endothelium is not only at the cross‐bridges of communication between blood and tissue called L‐arginine‐NO‐cyclic guanosine monophosphate (GMP) pathway Citation5. This signaling cascade starts with endothelial NO synthase (eNOS, NOSIII), which generates NO and L‐citrulline from L‐arginine and O2 in response to receptor‐dependent agonists (bradykinin, acetylcholine, Adenosine triphosphate (ATP)) and physicochemical stimuli (shear, stretch) Citation6 ().
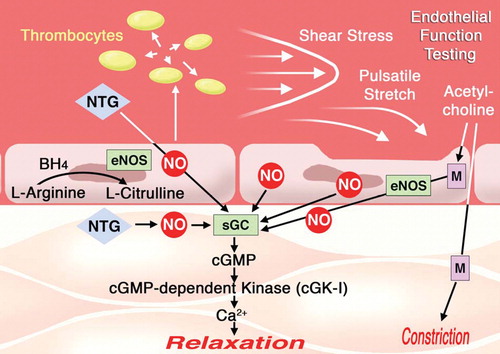
Figure 2 Regulation of vascular tone by the endothelium. The endothelial nitric oxide synthase(eNOS) synthesizes NO by a two‐step oxidation of the amino acid L‐arginine thereby leading to the formation of L‐citrulline. NO is released into the bloodstream thereby inhibiting platelet aggregation and the release of vasoconstricting factors such as serotonin and thromboxane. NO diffuses also into the media and activates the soluble guanylate cyclase (sGC). The resulting second messenger cGMP in turn activates the cGMP‐dependent kinase, which mediates decreases in intracellular Ca2+ concentrations thereby causing vasorelaxation. The physiological stimuli to release NO are shear stress and pulsatile stretch. Intra‐arterial infusion is used in the clinics to assess endothelial function. Infused into the forearm (brachial artery) acetylcholine (ACh) causes a dose‐dependent vasodilation. In the coronary artery the response (vasoconstriction versus vasodilation) strictly depends on the functional integrity of the endothelium. In the presence of cardiovascular risk factors and endothelial dysfunction ACh will cause vasoconstriction due to stimulation of muscarinergic receptors in the media. muscarinic acetylcholine receptor (M), nitroglycerin (NTG).
NO diffuses to the adjacent smooth muscle where it interacts with different receptor molecules, of which the soluble guanylate cyclase (sGC) is the best‐characterized and presumably most important one with regard to control of vessel tone and smooth muscle proliferation. Activation by NO requires sGC heme‐iron to be in the ferrous (II) state. Upon NO binding, cGMP formation will increase substantially. cGMP in turn activates the cGMP‐dependent kinase I which in turn will increase the open probability of Ca2+‐activated K+(BK)‐channels, thereby inducing a hyperpolarization of the smooth muscle cells and inhibition of agonist‐induced Ca2+ influx. In addition, activated cyclic GMP-dependent kinase I (cGK‐Iβ) phosphorylates the inositol trisphosphate (IP3)‐receptor‐associated G‐kinase substrate (IRAG), thereby inhibiting agonist‐induced Ca2+ release and smooth muscle contraction. Another cGK‐I substrate found in many cell types is the 46/50 kD vasodilator‐stimulated phosphoprotein (VASP). cGK‐I phosphorylates VASP specifically at serine 239, and this reaction can be exploited as a biochemical monitor for the integrity and activity of the NO‐cGMP pathway Citation7.
Oxidative stress and endothelial dysfunction
The endothelium‐derived relaxing factor, previously identified as nitric oxide (NO) Citation3 or a closely related compound Citation8, has potent antiatherosclerotic properties. NO released from endothelial cells works in concert with prostacyclin to inhibit platelet aggregation Citation9: it inhibits the adhesion of neutrophils to endothelial cells and the expression of adhesion molecules. NO in high concentrations inhibits the proliferation of smooth muscle cells Citation10. Therefore, under all conditions where an absolute or relative NO deficit is encountered, the process of atherosclerosis is being initiated or accelerated. The half‐life of NO and therefore its biological activity is decisively determined by oxygen‐derived free radicals such as superoxide Citation11. Superoxide rapidly reacts with NO to form the highly reactive intermediate peroxynitrite (ONOO−) Citation12. The rapid bimolecular reaction between NO and superoxide yielding peroxynitrite (rate constant: 5–10×109 M−1s−1) is about 3–4 times faster than the dismutation of superoxide by the superoxide dismutase. Therefore, peroxynitrite formation represents a major potential pathway of NO reactivity depending on the rates of tissue superoxide production. Peroxynitrite in high concentrations is cytotoxic and may cause oxidative damage to proteins, lipids, and DNA Citation13. Recent studies also indicate that peroxynitrite may have deleterious effects on activity and function of the prostacyclin synthase Citation14 and the endothelial NOS Citation15, Citation16. Other ROS such as the dismutation product of superoxide, hydrogen peroxide, and the hypochlorous acid released by activated neutrophils, are not free radicals, but have a powerful oxidizing capacity, which will further contribute to oxidative stress within vascular tissue.
Assessment of endothelial function
The ideal endothelial function test should be cheap, noninvasive, safe, repeatable, reproducible, and clearly standardized between the different laboratories. The current gold standard for diagnosing endothelial dysfunction is the assessment of endothelial function in coronary vessels via administration of acetylcholine to the coronary blood vessel system, combined with a measurement of the coronary blood vessel flow. As this is an invasive procedure, it imposes considerable use of resources in the setting of a medical clinic. Thus, as the main target for testing if coronary endothelial dysfunction is present, the establishment of noninvasive testing methods is highly preferred. Five different methodologies to measure endothelial function are summarized (). In the subsequent paragraphs we will discuss these different methodologies with special emphasis on the pulse wave plethysmography and the pulse curve analysis, since these two techniques are quite inexpensive and easy to use and may have the perspective to be employed frequently in the future due to their noninvasive nature.
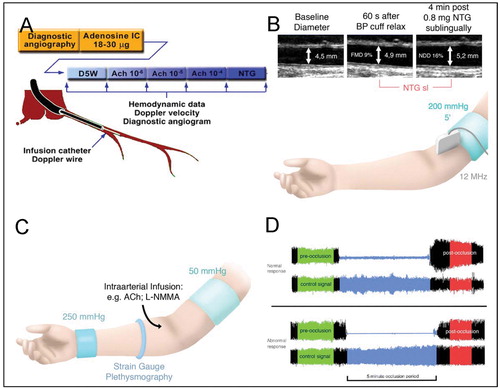
Figure 3 Different invasive and noninvasive methodologies to assess endothelial function in patients with cardiovascular risk factors. A: intracoronary infusion of acetylcholine; B: flow‐mediated dilation; C: forearm plethysmography; D: finger plethysmography. Representative reactive hyperemia peripheral artery tonometry recordings of subjects with normal and abnormal reactive hyperemic response. Normal response is characterized by a distinct increase in the signal amplitude after cuff release compared with baseline. blood pressure (BP), flow mediated dilation (FMD), acetylcholine (ACh), L‐NG‐monomethyl arginine (L‐NMMA).
Intracoronary infusion of acetylcholine
Endothelial function may be assessed by different methods including receptor‐dependent NO release e.g. via intra‐arterial infusion of the endothelium‐dependent vasodilator acetylcholine (ACh) or by using physicochemical stimuli such as shear stress. The intracoronary infusion of ACh is a widely used approach, which has clearly several important limitations such as being very invasive and requiring the presence of a very experienced interventionalist. To assess the endothelial function of the epicardial conductance vessels, ACh‐induced vasomotion before and after ACh is assessed by quantitative coronary angiography (QCA) (). Other substances that have been employed are bradykinin, substance P, and adenosine (dilation is at least in part endothelium‐dependent). Other measures to assess endothelial function are the demonstration of the flow‐dependent dilation e.g. via adenosine infusion into the distal coronary artery and the subsequent assessment of flow‐mediated dilation (FMD) of the proximal artery Citation17. Several groups also used the cold pressure test, where with a normal endothelium the vasculature reacts with vasodilation and with an abnormal endothelium the vessels will respond with vasoconstriction Citation18. To assess the endothelial function of resistance vessels, an intracoronary Doppler device for the calculation of coronary blood flow and coronary vascular resistance is used Citation18. More recently there has been some doubt whether this approach represents a good tool to assess endothelial function since e.g. stimulation with ACh may lead to a stimulation of vasoconstrictors such as endothelin which is produced by the endothelium but may also be produced in smooth muscle cells e.g. in response to chronic oxidative stress Citation19, Citation20. Thus, by infusing ACh, one measures not solely endothelial function but more likely coronary artery function, which includes endothelium‐dependent but also endothelium‐independent reactions Citation21.
Flow‐mediated dilation of the brachial artery
A much less invasive approach is to measure the flow‐mediated dilation (FMD) of the brachial artery by using high‐resolution ultrasound Citation22. The brachial artery diameter is measured before and after an increase in shear stress that is induced by reactive hyperemia. We place the sphygmomanometer cuff proximal to the brachial artery and inflate it up to 200 mmHg for a period of 5 minutes (). When the cuff is released, we record the reactive, flow‐dependent dilation of the brachial artery. The amount of dilation largely reflects endothelial function and therefore the vascular NO bioavailability. Thereafter we measure the total vasodilator capacity of the vessel by testing the dilation in response to nitroglycerin (NTG) 0.8 mg sublingually. One of the disadvantages is that the technique is very demanding and requires a high training status of the technicians. In our center, technicians have to be trained for at least a period of 6–9 months before they get involved in endothelial function studies ().
The principal question related to this method is whether the cuff to interrupt forearm blood flow should be placed at the forearm or the upper arm. Both approaches have been used by many groups. The upper arm occlusion (as done by our group and the group from Joe Vita) has the great advantage that the degree of flow‐dependent dilation of the brachial artery is substantially stronger as compared to forearm occlusion. Whether it is a disadvantage when the brachial artery is in the ischemic region is a still unresolved issue. It is important to note that by using the technique of upper arm occlusion, Gokce et al. were able to demonstrate that endothelial function has prognostic implications Citation23, Citation24. As shown by Joe Vita's group we also see evidence for endothelial dysfunction when FMD is below the 8% range Citation23, Citation24.
Forearm plethysmography
This test is used to quantify changes in forearm blood flow or endothelial function of forearm arterioles in response to intrabrachial infusion of endothelium‐dependent vasodilators such as e.g. ACh, metacholine, substance P, and bradykinin (). In contrast to the coronary artery system, intrabrachial infusion of ACh always produces vasodilation. To assess the contribution of basally released NO, one can infuse the NOS inhibitor NG‐monomethyl‐L‐arginine (L‐NMMA). The amount of constriction reflects the degree of basally released NO. Some studies have addressed the relationship between coronary and peripheral endothelial function and found a weak Citation25 or even no correlation at all Citation26.
Venous occlusion plethysmography has been used widely, but it requires the puncture of an artery and is therefore an invasive approach. This can be used as a clear argument against its use in larger studies.
Finger‐pulse plethysmography (ENDO‐PAT)
Several cheap alternative techniques have demonstrated that they have the capacity to measure endothelial function. From past studies it is known that low amplitudes of the pulse wave are associated with atherosclerosis and are suited to predicting ischemic heart disease and death Citation27. A new method for diagnosing endothelial function, relying on changes of the pulse wave amplitude during reactive hyperemia, EndoPAT2000 (Itamar Medical Ltd, Caesarea, Israel) was introduced to medical practice in the last years. The changes of the pulse wave amplitude are registered through finger plethysmography, and pressure change signals are then filtered, amplified, displayed, and stored for further analysis. The EndoPAT2000 (PAT = peripheral arterial tonometry) is used to assess the endothelial function. Bonetti et al. Citation27 reported from their collective of patients, simultaneously assessed with PAT and coronary blood flow measurement after stimulation with ACh, that PAT was suited to identifying patients with coronary endothelial dysfunction with an average reactive hyperemia PAT index reported to be lower in patients with coronary endothelial dysfunction, compared with those with normal coronary endothelial function (1.27±0.05 versus 1.78±0.08; P<0.001) (). A reactive hyperemia peripheral artery tone index <1.35 (RH‐PAT) was found to have a sensitivity of 80% and a specificity of 85% to identify patients with coronary endothelial dysfunction Citation27. EndoPAT2000 uses pneumatic finger probes to record changes of the pulse wave amplitude. The PAT sensor is thimble‐shaped, exhibiting a uniform pressure field to the distal phalanx of the finger, thus enabling pulsatile volume changes to be measured. PAT applies a significant counterpressure of 70 mmHg to the finger, thereby preventing venous pooling and blood stasis. This pressure field also prevents venous distension during the cuff inflation of the reactive hyperemia phase of the endothelial function testing. The finger probes are connected through flexible tubing to isolated volume reservoirs buffering pressure changes. For the most thorough testing, one probe is placed on the index finger of the arm for which the measurement is conducted, and another probe is attached to the index finger of the contralateral arm. The pulse wave tonometry hyperemia ratio is defined as the ratio of the average pulse wave amplitude during a time frame of exactly 1 minute, after 60 seconds of the beginning of the reactive hyperemia, to the average pulse wave amplitude of a 210‐second baseline period before the start of the occlusion of the brachial artery. This signal, derived from the measurement, is normalized to the concurrent signal of the contralateral arm, to adjust for potential systemic affects of unilateral arm ischemia. The nitroglycerine response is derived as pulse wave amplitude of the 1‐minute period starting exactly after a 5‐minute period after the supplementation of sublingual nitroglycerine, compared to the pulse wave amplitude of a 210‐second baseline period before administration of nitroglycerine. As nitroglycerine exerts systemic effects, correction for the signal of the contralateral arm is omitted. The PAT signal is analyzed using a computerized algorithm developed by Itamar (Itamar Medical Ltd, Caesarea, Israel) and therefore intraobserver and interobserver variability can be disregarded ().
Pulse curve analysis
Estimating the large artery stiffness and endothelial function by pulse contour analysis is possible using the PulseTrace PCA2 (MicroMedical Ltd, Chatham, United Kingdom) in a very reliable and fast way. Analysis of the pulse curve relies on the observation that changes to the pulse curve correlate with the diagnosis of cardiovascular disease Citation28. In this context, it was noticed that the volume pulse, recorded with a digital plethysmographic probe, is directly related to the radial and brachial artery pressure pulse Citation28. The digital volume pulse is recorded by measuring the transmission of infrared light absorbed in the finger, whereby the amount of light absorbed is directly proportional to the amount of blood in the finger pulp. To minimize poor signals from vasoconstriction or in subjects with an impaired blood flow, a control system maintains the light transmission at an optimum level.
The pulse wave is formed through the passage of the pressure transmission along the blood vessel system, and the first part of the waveform (systolic component) is the result of the pressure transmission the direct way from the aorta to the finger with the digital probe. The reflected, second part (diastolic component) of the waveform is produced by pressure transmission along the aortic root to the lower limbs and its consecutive reflection and so also reaching the fingertip. The height of the diastolic component relates to the tone of the small arteries, and the timing of the diastolic component depends on the pulse wave velocity in the aorta and large arteries, therefore depends upon the large artery stiffness. The reflection index (RI) is the height of the diastolic component expressed as percentage of the systolic component and is a direct measure for the tone of the small arteries. The stiffness index is assessed from the pulse wave velocity in large arteries and is calculated by dividing the height of the test subject in meters by the time between the systolic and diastolic peak of the digital volume pulse in seconds. The measurement of the stiffness index is very reliable when compared to the current gold standard of vascular function testing, the measurement of pulse wave velocity from the carotid to the femoral artery (PWVcf) Citation29. As the reflection index is suited to measure the vessel tone, it can also be used to measure endothelial function. In previous studies, the measurement of the reflection index using salbutamol for endothelium‐dependent release of nitric oxide made it possible to monitor endothelial function. Salbutamol can be administered using an inhaler making this a very simple test to perform in the clinic or at the bedside Citation30. One major benefit when using the PulseTrace PCA2 is that the measurement is operator‐independent and therefore the coefficient of variation is better than that of other techniques for estimation of the stiffness index or the reflection index Citation29.
Technical remarks
Endothelial function is influenced by many factors that have to be controlled in order to get reproducible results. There is a significant diurnal variation demonstrating that the time of investigation has to be standardized Citation31. Food intake Citation32 and acute glucose challenges impair endothelial function, meaning that the patients should fast, including caffeine, for at least 8 hours before the investigation Citation33. No significant inhibitory effects on FMD was seen during office hours or after light meals Citation34.
FMD is also influenced by hormonal factors including estrogens, progesterone, and catecholamines. Thus the investigator should be aware that the menstrual cycle, mental stress, and sleep deprivation should also affect endothelial function.
Measurements should, if possible, take place in the morning in a temperature‐controlled room. The patient should of course not smoke, and vasoactive medication should not be taken on the morning of the measurements.
Trained technicians should also perform the determination of the FMD. We train the staff here for at least 6 months to minimize as much as possible intra‐ and interindividual variations.
Endothelial dysfunction and cardiovascular risk factors
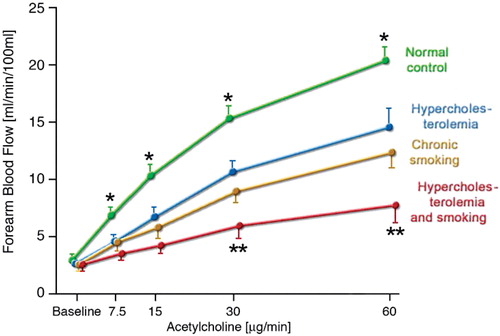
It is well known that endothelial dysfunction is frequently encountered in the presence of cardiovascular risk factors. This has been shown for chronic smokers, patients with increased low‐density lipoprotein (LDL) levels, for patients with diabetes Type I and II, for hypertensive patients, and for patients with the metabolic syndrome. It is important to note that cardiovascular risk factors synergistically impair endothelial function. In an early study we were able to show that e.g. chronic smoking, defined as 20 pack years, have comparable negative effects for endothelial function to high LDL levels. The combination of both risk factors drastically impairs receptor‐dependent increases in forearm blood flow in response to ACh ().
Figure 4 Plots of forearm blood flow to acetylcholine in normal subjects, hypercholesterolemic patients, long‐term smokers, and patients with hypercholesterolemia who smoked. This figure clearly shows the marked potentiation of endothelial dysfunction when two risk factors such as smoking and hypercholesterolemia are present at the same time (adapted from: Heitzer T, Ylä‐Herttuala S, Luoma J, Kurz S, Münzel T, Just H, Olschewski M, Drexler H. Cigarette smoking potentiates endothelial dysfunction of forearm resistance vessels in patients with hypercholesterolemia. Role of oxidized LDL. Circulation. 1996 Apr 1;93(7):1346‐53.)
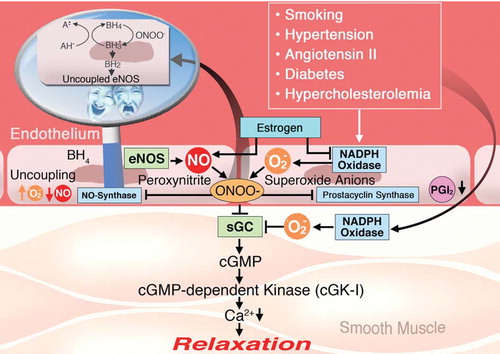
What is the key mechanism underlying endothelial dysfunction in patients with cardiovascular risk factors or established coronary artery disease? There are several potential abnormalities that could account for reductions in endothelium‐dependent vascular relaxation, including changes in the activity and/or expression of the eNOS, decreased sensitivity of vascular smooth muscle cells to NO, or increased degradation of NO via its interaction with ROS such as superoxide. The NO degradation concept is the most attractive one since, in the presence of cardiovascular risk factors, endothelial dysfunction is established and even more importantly it is markedly improved by the acute administration of the antioxidant vitamin C. This has been shown for patients with diabetes types I and II, for endothelial dysfunction induced by acute glucose or homocysteine infusion, in patients with essential hypertension, in chronic smokers, patients with the metabolic syndrome, or patients just presenting a positive family history Citation35–38. These findings clearly indicate that the vasculature per se produces large amounts of superoxide, which in turn reduces NO bioavailability by degrading NO and by forming the highly toxic NO/superoxide reaction product peroxynitrite (ONOO−). As summarized in , peroxynitrite per se has many negative effects on vascular function by causing eNOS uncoupling, by causing tyrosine nitration of the prostacyclin synthase thereby inhibiting PGI2 formation within the endothelium, and by directly inhibiting the activity of sGC e.g. by causing sGC oxidation from the Fe2+ to the Fe3+ state, thereby making sGC nonresponsive to NO Citation39.
Figure 5 Mechanisms underlying endothelial(vascular) dysfunction in vascular disease. In the presence of risk factors, superoxide‐producing enzymes such as the NADPH oxidase produce large amounts of superoxide (O2·−). Superoxide rapidly reacts with nitric oxide (NO) to form the highly reactive intermediate peroxynitrite (ONOO−). Peroxynitrite causes vascular dysfunction in several ways. It causes tyrosine nitration of the prostacyclin synthase (PGI2‐S) thereby shutting down PGI2 production. Peroxynitrite is also a strong inhibitor of the soluble ganylate cyclase (sGC), thereby inhibiting NO signaling. ONOO− can also oxidize the BH4 to the so‐called BH3· radical. This can decay to BH2 thereby causing eNOS uncoupling. This means that the antiatherosclerotic NO‐producing eNOS is switched to a superoxide‐producing proatherosclerotic enzyme. Vitamin C has been shown to recouple eNOS by reducing the BH3· to BH4 (see insert).
Vascular superoxide sources
Role for NADPH oxidase
The NADPH‐oxidase is a superoxide‐producing enzyme, which has been first characterized in neutrophils Citation40. Meanwhile we know that a similar enzyme exists also in endothelial and smooth muscle cells, as well as in the adventitia. The activity of the enzyme in endothelial as well as smooth muscle cells is increased upon stimulation with angiotensin II Citation41. The stimulatory effects of angiotensin II on the activity of this enzyme would suggest that in the presence of an activated renin angiotensin system (local or circulating), vascular dysfunction due to increased vascular superoxide production is likely to be expected. Experimental hypercholesterolemia has been shown to be associated with an activation of the NADPH‐oxidase Citation42, and there is a close association with endothelial dysfunction and clinical risk factors and the activity of this enzyme in human saphenous veins in patients with coronary artery disease Citation43. In atherosclerotic arteries there is evidence for increased expression of the NADPH oxidase subunit gp91phox and nox4, all of which may contribute to increased oxidative stress within vascular tissue and interestingly in the shoulder of atherosclerotic plaques, all of which may trigger a plaque rupture Citation44.
Interestingly, there is a growing body of evidence that the local renin angiotensin system is activated in the setting of hypercholesterolemia. In patients, angiotensin‐converting enzyme (ACE)‐activity and therefore local angiotensin II concentrations are increased in atherosclerotic plaques Citation45, Citation46, and inflammatory cells are capable of producing large amounts of angiotensin II. Increased angiotensin II concentrations along with increased levels of superoxide have been shown in the shoulder region of atherosclerotic plaques Citation47. In vessels from hypercholesterolemic animals Citation42, as well as in platelets from hypercholesterolemic patients Citation48, there is an increase in the expression of the angiotensin II receptor subtype AT1. Thus, both experimental and clinical studies have provided evidence for stimulation of the renin angiotensin system in atherosclerosis and simultaneously for an activation of the NADPH oxidase in the arterial wall. Similar evidence for an activation of this enzyme in the vasculature has been provided from experimental animal models of different forms of hypertension such as angiotensin II infusion Citation49, Citation50 and in spontaneously hypertensive rats Citation51, as well as in different forms of diabetes mellitus Citation52.
The proof of concept that superoxide produced by the NADPH oxidase may indeed trigger eNOS uncoupling was provided by David Harrison's group in the experimental animal model of desoxycorticosterone acetate (DOCA)‐salt hypertension. With these studies the authors showed that superoxide induced by DOCA‐salt treatment caused increased vascular superoxide production, which was significantly reduced by an inhibitor of eNOS such as L‐NAME. Treatment of p47phox knockout animals with DOCA‐salt caused markedly reduced levels of oxidative stress and abolished superoxide effects of NOS inhibition compatible with a prevention of eNOS uncoupling Citation53.
Role for the xanthine oxidase
Xanthine oxidoreductase catalyzes the sequential hydroxylation of hypoxanthine to yield xanthine and uric acid. The enzyme can exist in two forms that differ primarily in their oxidizing substrate specificity. The dehydrogenase form preferentially utilizes NAD+ as an electron acceptor but is also able to donate electrons to molecular oxygen. By proteolytic breakdown as well as thiol oxidation xanthine dehydrogenase from mammalian sources can be converted to the oxidase form that readily donates electrons to molecular oxygen, thereby producing superoxide and hydrogen peroxide, but does not reduce NAD+. Oxypurinol, an inhibitor of xanthine oxidoreductase, has been shown to reduce superoxide production and to improve endothelium‐dependent vascular relaxations to acetylcholine in vessels from hyperlipidemic animals Citation54. This suggests an increase in the expression or activity of xanthine oxidase in early hypercholesterolemia. The mechanisms underlying such a phenomenon remain unclear; however, it has been demonstrated that certain cytokines can stimulate the expression of xanthine oxidase by the endothelium. An alternative mechanism may be that increased cholesterol levels trigger the release of xanthine oxidase (e.g. from the liver) into the circulation where it binds to endothelial glycosaminoglycans Citation55. Human studies concerning the efficacy of xanthine oxidase inhibition on endothelial dysfunction are somewhat discrepant. While Panza et al. showed that endothelial dysfunction in hypercholesterolemic patients and hypertensive diabetics is improved by acute inhibition of xanthine oxidase (XO) with oxypurinol and allopurinol Citation56, Citation57, other groups failed to show similar efficacy Citation58 for allopurinol. Its role in mediating increased oxidative stress in the setting of hypertension is not quite clear. Oxypurinol has blood pressure‐lowering effects comparable to heparin binding superoxide dismutase (SOD) in Spontaneously hypertensive rats (SHR) Citation59 but fails to demonstrate a positive effect on endothelial dysfunction in hypertensive patients Citation56. More recent studies in patients with chronic congestive heart failure clearly failed to demonstrate any prognostic benefit when oxypurinol was added to conventional heart failure treatment Citation60.
Uncoupled eNOS
For proper function of NOS, tetrahydrobiopterin (BH4) seems to be essential in several ways including stabilizing the NOS dimer and increasing the affinity of NOS for L‐arginine. Limited availability of BH4 will inevitably result in increased superoxide formation at the expense of NO formation, i.e. it will uncouple NOS.
What are the mechanisms leading to BH4 depletion? In vitro studies proposed that native LDL Citation61 and even more pronounced oxidized LDL Citation62 are able to stimulate endothelial superoxide production, and that this phenomenon is inhibited by the NOS inhibitor L‐NAME pointing to a specific role of eNOS in superoxide production. Hypercholesterolemia also has been shown to increase vascular formation of superoxide via activation of the NADPH oxidase Citation42 and/or xanthine oxidase Citation54. Superoxide derived from both enzyme sources may lead to increased formation of peroxynitrite Citation63, Citation64. Peroxynitrite in turn rapidly oxidizes the active NOS cofactor BH4 to cofactor‐inactive molecules such as BH2Citation64, Citation65. These concepts, however, also imply that the uncoupling of eNOS would invariably require a priming event such as superoxide produced by the NADPH oxidase and/or the xanthine oxidase (so called ‘kindling radicals’) leading via increased formation of peroxynitrite eNOS to produce superoxide (bonfire radical). The mechanism underlying eNOS uncoupling have recently been discussed in detail (for review see Citation66)
Mitochondria
Another important superoxide source is the mitochondrion. The mitochondrial respiratory chain can be a major source of superoxide, which may be then be converted to H2O2. Molecular O2 serves as the final electron acceptor for the cytochrome C oxidase complex (IV), the terminal component of the respiratory chain, and is ultimately reduced to H2O2. Up to 1%–4% of O2 may be incompletely reduced, resulting in O2·−, mainly at complex I and complex III. In the presence of transitional metal ions, the toxic hydroxyl radicals (OH·) may be also formed. Increased O2·− formation in endothelial cells appear to be particularly prominent in the situations of metabolic perturbation e.g. in the setting of hyperglycemia or high levels of the adipokinin leptin. Other settings include e.g. ischemia reperfusion.
Endothelial function and prognosis
Patients with coronary artery disease
Since 2000, a quite large number of clinical trials have demonstrated a close association between coronary and peripheral endothelial function and the likelihood of cardiovascular events. For example Volker Schächinger from Andreas Zeiher's group has shown that patients who respond to intracoronary ACh with vasodilation have subsequently much fewer cardiovascular events defined as death due to myocardial infarction, myocardial infarction, coronary and peripheral artery revascularization, and stroke, as compared to patients who responded to intracoronary ACh with vasoconstriction Citation67.
More recently we were able to show that peripheral endothelial function also has prognostic meanings Citation68, see . Patients with cardiovascular events had a clearly attenuated maximal forearm blood flow in response to intrabrachial infusion of the endothelium‐dependent vasodilator acetylcholine as established with the forearm plethysmography method.
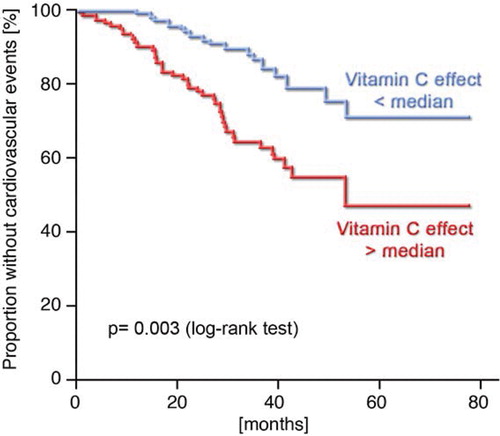
Heitzer et al. also showed that patients who responded well to intra‐arterial infusion of vitamin C with an improvement of endothelial function had a worse prognosis as compared to patients with low or no vitamin C effects Citation68. This finding further strengthens the concept that oxidative stress indeed is the key player in determining the degree of endothelial dysfunction but also the prognosis in patients with established coronary artery disease.
Patients with peripheral artery disease
Peripheral endothelial function assessed with FMD of the brachial artery has also been proven to be a good tool to risk‐stratify patients undergoing peripheral or coronary bypass surgery for postoperative cardiovascular events Citation23. In this study patients were followed postoperatively for 30 days. The combined end point consisted of cardiac death, myocardial infarction, instable angina pectoris/ischemic ventricular fibrillation, stroke, and elevated troponin I Citation23. In all patients FMD of the brachial artery was measured before surgery, and the patients were grouped into three tertiles: FMD>8.1%, between 4% and 8%, and below 4%.
In a Cox proportional hazards model, the independent predictors for events were age, renal insufficiency, no carotid surgery, and lower flow‐dependent dilation of the brachial artery. When a flow‐dependent dilation cutoff point of 8.1% was used, endothelial function had a sensitivity of 95%, specificity of 37%, and a negative predictive value of 98% for events. This study actually implies that measurement of endothelial function in the brachial artery may provide information about plaque stability in coronary arteries. Gokce et al. further showed that in 199 patients with peripheral artery disease and before elective bypass surgery, the patients having postoperative cardiovascular events had a clearly depressed flow‐mediated dilation of the brachial artery (4.4%±2.8%) versus patients without any events (7.0%±4.9%) Citation24.
Further studies revealed a strong association between endothelial dysfunction and prognosis in patients with chronic congestive heart failure Citation69 and essential hypertension Citation70.
Ankle brachial index carotid artery intima media thickness
Brevetti et al. studied whether flow‐mediated dilation of the brachial artery in patients with peripheral artery disease may represent an independent predictor with respect to cardiovascular events and whether this parameter may add additional prognostic value to the Ankle-brachial index (ABI) Citation71. The authors found that in 131 patients with peripheral artery disease FMD, ABI, and a previous stroke represented independent predictors of future cardiovascular events such as acute myocardial infarction, unstable angina, coronary revascularization, transitory ischemic attack, and peripheral revascularization Citation71.
Large cross‐sectional trials employing endothelial function
There are several large‐scale cross‐sectional trials to evaluate the brachial artery flow‐mediated dilation and its relation to biomarkers such as C‐reactive protein (CRP) Citation72, Citation73, Atrial natriuretic peptide (ANP), brain natriuretic peptide [BNP] Citation73, and asymmetric dimethyl L‐arginine (ADMA) Citation74. These studies, comprising 2113 subjects from the Framingham Heart Study, 2096 participants of the Cardiovascular Risk in Young Finns Study, and 1154 males from the Firefighters And Their Endothelium (FATE) study, demonstrated that there is no relationship between CRP and FMD Citation72, while a close relationship between plasma ANP Citation73 and ADMA levels Citation74 and endothelial function was reported.
Endothelial function testing: implications for the future
There is no doubt that based on the prognosis papers endothelial function testing may allow identification of patients at higher risk for the development of cardiovascular events. The measurement of endothelial function will allow quantification of the beneficial effects of life‐style changes and/or medical therapy on endothelial function, which per se will markedly improve patient compliance. Endothelial function may also help to further risk‐stratify patients in the setting of cardiovascular prevention who may benefit from cardiovascular therapy.
What is the best method to assess endothelial function? Currently there is no doubt that the noninvasive method, the flow‐mediated dilation of the brachial artery, represents the gold standard for endothelial function measurement. Endothelial function of the coronary artery as assessed by intracoronary ACh may characterize the release of vasoconstricting factors rather than endothelium‐dependent NO release. In addition, the invasive nature of this investigation limits its wider use in large numbers of patients. One has also to consider that the term endothelial dysfunction is not correct anymore, since more recent studies clearly showed that in addition to the endothelium, the media and also the adventitia produce large amounts of reactive oxygen species, which will attenuate endothelial mediated dilation, although the mechanisms underlying ‘endothelial dysfunction’ are located in addition to the endothelium in the smooth muscle cell layer. Future studies will have to show whether other noninvasive procedures, such as the ENDO‐PAT method or the pulse curve analysis, really correlate with endothelial function as assessed by the flow‐dependent dilation of the brachial artery and whether their results can also be used as indicators for future cardiovascular events.
Is there a biomarker in the peripheral blood that reflects endothelial dysfunction?
Considering the role of the endothelium in the initiation and propagation of vascular wall injury, there is a need for the discovery of validated biomarkers to serve as predictors of activation of the inflammatory cascades in the development of vascular injury. Several factors have been proposed to serve as such potential markers being suited to indicate endothelial dysfunction ().
Table I. Biomarkers reflecting endothelial dysfunction (injury).
Circulating endothelial cells and circulating endothelial progenitor cells
Mature circulating endothelial cells (CEC) and endothelial progenitor cells can be differentiated by means of their size and expression of surface markers. Apoptotic CECs are identified by expressing CD146, are rarely found in the blood of healthy young adults, but are clearly elevated in patients with cardiovascular disease Citation75. CECs may arise from damaged endothelium. More recently Sanjay Rajagopalan described an inverse relationship between CEC levels and FMD in patients with systemic lupus erythematosus (SLE) Citation76. After adjusting for known factors for endothelial dysfunction CD146, was the only variable that predicted FMD. CECs have been shown to correlate with the severity of coronary and peripheral artery disease.
Circulating endothelial progenitor cells express the CD34 and the kinase insert domain KDR. Endothelial progenitor cells were increased in patients with unstable angina. On the other hand a negative correlation was found between endothelial progenitor cells (EPC) and cardiovascular risk factors. Low EPC counts represent a useful marker for future cardiovascular events Citation77, Citation78. Medical treatment with statins has been shown to increase EPC levels Citation79 and to simultaneously improve endothelial dysfunction, all of which may be explained by the potential of EPCs to cause repair of the damaged endothelium ( ). Nevertheless, the fact that we can almost completely correct endothelial dysfunction by applying very high amounts of vitamin C, such as has been demonstrated in chronic smokers, is in my mind a strong argument that ROS production and subsequent NO metabolism rather than detachment of endothelial cells from the vessels represents the decisive mechanism underlying endothelial dysfunction in patients with cardiovascular risk factors Citation37.
Endothelial microparticles
Endothelial microparticles (EMPs) are small vesicles formed by the cell membrane that are released from activated or damaged endothelial cells (). EMPs released by apoptosis or activation can be differentiated, and some EMPs carry functional von Willebrand factor. Raised EMP levels have been found in hypertension and in patients with coronary artery disease Citation80, Citation81. Treatment with statins is able to decrease EMP release from cultured coronary endothelial cells Citation82.
Cytokines and adhesion molecules
Cytokines such as interleukin (IL)‐1, ‐6 and tumor necrosis factor (TNF)α are pleiotropic proteins that regulate leucocyte activity and drive production of acute phase proteins such as C‐reactive protein (CRP), serum amyloid A, and fibrinogen Citation83. CRP in turn mediates enhanced expression of cellular adhesion molecules such as intracellular adhesion molecule (ICAM)‐1 and vascular cell adhesion molecule (VCAM)‐1, induction of monocyte chemoattracting protein (MCP1), increased expression of plasminogen activator inhibitor (PAI)‐1, inhibition of progenitor cell survival, and reduction in NO production, thereby causing a prothrombotic, proatherosclerotic, and proinflammatory environment.
Asymmetric dimethylarginine (ADMA)
An interesting marker is the asymmetric dimethyl L‐arginine, or ADMA. ADMA can competitively out‐compete eNOS from L‐arginine and therefore reduce eNOS‐derived NO production. There is also some evidence that ADMA may even cause eNOS uncoupling, thereby switching eNOS from a NO‐ to a superoxide‐producing enzyme. Increased ADMA levels have been demonstrated in patients with risk factors such as hypertension, in chronic smokers, patients with hypercholesterolemia, and in patients with diabetes and renal insufficiency. More recent data from our group indicate Citation84, that ADMA has prognostic value clearly beyond traditional risk factors and novel biomarkers such a brain natriuretic peptide (BNP). It is important to note that the enzyme synthesizing and degrading ADMA are regulated in a redox‐sensitive fashion Citation85. Thus, in all conditions where oxidative stress is increased within the vasculature, increased cellular/circulating levels of ADMA are expected Citation85, Citation86.
Taken together, there is no doubt that measurement of endothelial function and/or markers of endothelial dysfunction provide substantial prognostic information about future cardiovascular events in secondary prevention.
Figure 6 Chronic oxidative stress causes senescence of endothelial cells. This is characterized by a detachment of endothelial cells or part of the endothelial cell membrane(microparticles; A). B: With the persistence of oxidative stress, the capacity of neighboring endothelial cells to repair endothelial injury is limited, and vascular integrity becomes dependent on the incorporation of endothelial progenitor cells (EPCs) (adapted from Citation87).
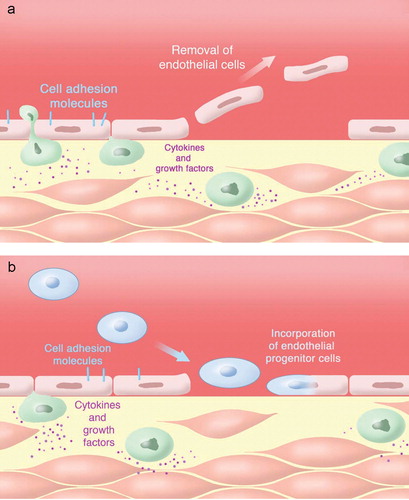
Figure 7 Kaplan‐Meier analysis demonstrating cumulative proportions of patients without cardiovascular events during follow‐up. The figure clearly shows that patients who react strongly to vitamin C with an improvement of endothelial dysfunction have a worse prognosis as compared to patients with a weaker vitamin C response. This means that patients with high oxidative stress in the forearm vasculature may also have more cardiovascular events such as myocardial infarction, death due to myocardial infarction, stroke, and coronary revascularization procedures Citationadapted from Ref. 68.
Endothelial function and primary prevention: the Gutenberg Heart Study
The role of the determination of endothelial dysfunction in primary prevention remains to be established. In Mainz we are performing right now a monocenter primary prevention study, the so‐called PREVENT‐it trial. PREVENT‐it stands for Proteomics and Genomics and Endothelial function. A total of 17,000 people from Rheinland Pfalz will be analyzed with respect to a multitude of potential cardiovascular risk factors with the primary aim of developing a risk score, taking into account psychosocial, environmental and life‐style factors, the extent of subclinical atherosclerotic disease, the laboratory phenotype and genetic variability, in addition to the traditional risk factors. Endothelial function testing is performed in this study, relying on three different measurement methods: flow‐mediated dilatation, pulse curve analysis, and peripheral arterial tonometry. The vast total number of subjects included in this study will enable a validation of all three measurement techniques and also allow for a comparison of these three noninvasive measurement devices regarding the primary (myocardial infarction and cardiovascular death) and secondary (new onset of heart failure, atrial fibrillation, diabetes mellitus, stroke, and others) end point. During the course of the study, close monitoring is established to discover which of the different techniques is suited best for the primary prevention setting and also clinical practice. As far as now, no other study used all three different devices for endothelial function testing; the results may indicate that a combined approach might be the sophisticated one in detecting early subclinical forms of atherosclerosis as indicated by an impaired endothelial function and therefore allowing early treatment of these conditions. A major goal of the PREVENT‐it study is the establishment of a new risk score for the population in Rhineland‐Palatinate and of course Germany as a whole. In this setting, risk models based on endothelial function parameters can be compared to risk models compromising the traditional risk factors, elucidating the role of endothelial function testing in a more practicable way. So far these measurements are used in most clinics for scientific purposes and not to achieve a better treatment and of course risk stratification, as these methods were intended to. Another important point is the whole‐genome association assay conducted in the first 3500 subjects taking part in the study. The connection of genetic and technical approaches to elucidate function and of course predictive capability regarding cardiovascular events is one of the major targets of the PREVENT‐it study. Genetic variations predicting impaired endothelial function at the level of gene expression analysis will further expand the knowledge about pathophysiology regarding endothelial dysfunction and may identify further targets for possible treatment options. The combination of the device‐related results, in combination with the results from the genetic analysis, can contribute to the further clarification of the early atherosclerosis process until manifestation of cardiovascular events. Thus endothelial function testing is not only very important for the prediction of a new risk score but might also be related to genetic variations or a different gene expression profile, showing new possible treatment options. First results regarding the endothelial function testing will be expected in summer 2008 and results from the genetic analysis at the end of 2008.
Summary
For almost 20 years we have been able to detect endothelial dysfunction in coronary and peripheral arteries. Studies with patients with established coronary artery disease and cardiovascular risk factors and congestive heart failure clearly demonstrated that endothelial dysfunction has fundamental prognostic implications. Overall it is disappointing that we did not manage it to introduce this technique into the clinics in order to risk‐stratify our patients as a daily routine. One of the reasons is that the available tests are technically too difficult, too invasive, too expensive, and too variable for routine clinical use. New (older) technologies, such as finger‐pulse plethysmography and the pulse wave reflection method, claim to measure endothelial dysfunction reliably without major intraindividual variations. Major trials including the PREVENT‐it study are running to find out whether endothelial dysfunction may have prognostic meaning also in the setting of primary prevention. This study also tests the method of FMD of the brachial artery in comparison with the finger‐pulse plethysmography and the pulse wave reflection method. This study will also address the question of which biomarker may be suited best to indicate whether or not endothelial dysfunction is present. Nevertheless, the ability to measure endothelial function noninvasively has helped us to understand the pathophysiologic processes underlying the development of subclinical atherosclerosis. In addition, the patient will get important feedback information about the status of his vessels and how life‐style changes and/or medical treatment favorably influence his vessel function, which in turn will improve the patient compliance substantially.
References
- Suwaidi J. A., Hamasaki S., Higano S. T., Nishimura R. A., Holmes D. R Jr., Lerman A. Long‐term follow‐up of patients with mild coronary artery disease and endothelial dysfunction. Circulation 2000; 101: 948–54
- Moncada S., Korbut R., Bunting S., Vane J. R. Prostacyclin is a circulating hormone. Nature 1978; 273: 767–8
- Palmer R. M., Ferrige A. G., Moncada S. Nitric oxide release accounts for the biological activity of endothelium‐derived relaxing factor. Nature 1987; 327: 524–6
- Stupack D. G., Cheresh D. A. Integrins and angiogenesis. Curr Top Dev Biol 2004; 64: 207–38
- Busse R., Fleming I. Regulation of NO synthesis in endothelial cells. Kidney Blood Press Res 1998; 21: 264–6
- Fleming I., Busse R. Molecular mechanisms involved in the regulation of the endothelial nitric oxide synthase. Am J Physiol Regul Integr Comp Physiol 2003; 284: R1–12
- Oelze M., Mollnau H., Hoffmann N., Warnholtz A., Bodenschatz M., Smolenski A., et al. Vasodilator‐stimulated phosphoprotein serine 239 phosphorylation as a sensitive monitor of defective nitric oxide/cGMP signaling and endothelial dysfunction. Circ Res 2000; 87: 999–1005
- Myers P. R., Minor R. L Jr., Guerra R Jr., Bates J. N., Harrison D. G. Vasorelaxant properties of the endothelium‐derived relaxing factor more closely resemble S‐nitrosocysteine than nitric oxide. Nature 1990; 345: 161–3
- Radomski M. W., Palmer R. M., Moncada S. The anti‐aggregating properties of vascular endothelium: interactions between prostacyclin and nitric oxide. Br J Pharmacol 1987; 92: 639–46
- Garg U. C., Hassid A. Nitric oxide‐generating vasodilators and 8‐bromo‐cyclic guanosine monophosphate inhibit mitogenesis and proliferation of cultured rat vascular smooth muscle cells. J Clin Invest 1989; 83: 1774–7
- Gryglewski R. J., Moncada S., Palmer R. M. Bioassay of prostacyclin and endothelium‐derived relaxing factor (EDRF) from porcine aortic endothelial cells. Br J Pharmacol 1986; 87: 685–94
- Beckman J. S. Oxidative damage and tyrosine nitration from peroxynitrite. Chem Res Toxicol 1996; 9: 836–44
- Beckman J. S., Koppenol W. H. Nitric oxide, superoxide, and peroxynitrite: the good, the bad, and ugly. Am J Physiol 1996; 271: C1424–37
- Zou M. H., Ullrich V. Peroxynitrite formed by simultaneous generation of nitric oxide and superoxide selectively inhibits bovine aortic prostacyclin synthase. FEBS Lett 1996; 382: 101–4
- Zou M. H., Shi C., Cohen R. A. Oxidation of the zinc‐thiolate complex and uncoupling of endothelial nitric oxide synthase by peroxynitrite. J Clin Invest 2002; 109: 817–26
- Kuzkaya N., Weissmann N., Harrison D. G., Dikalov S. Interactions of peroxynitrite, tetrahydrobiopterin, ascorbic acid, and thiols: implications for uncoupling endothelial nitric‐oxide synthase. J Biol Chem 2003; 278: 22546–54
- Zeiher A. M., Drexler H., Wollschlager H., Just H. Modulation of coronary vasomotor tone in humans. Progressive endothelial dysfunction with different early stages of coronary atherosclerosis. Circulation 1991; 83: 391–401
- Zeiher A. M., Drexler H., Wollschlager H., Just H. Endothelial dysfunction of the coronary microvasculature is associated with coronary blood flow regulation in patients with early atherosclerosis. Circulation 1991; 84: 1984–92
- Kahler J., Ewert A., Weckmuller J., Stobbe S., Mittmann C., Koster R., et al. Oxidative stress increases endothelin‐1 synthesis in human coronary artery smooth muscle cells. J Cardiovasc Pharmacol 2001; 38: 49–57
- Kahler J., Mendel S., Weckmuller J., Orzechowski H. D., Mittmann C., Koster R., et al. Oxidative stress increases synthesis of big endothelin‐1 by activation of the endothelin‐1 promoter. J Mol Cell Cardiol 2000; 32: 1429–37
- Lerman A., Holmes D. R Jr., Bell M. R., Garratt K. N., Nishimura R. A., Burnett J. C Jr. Endothelin in coronary endothelial dysfunction and early atherosclerosis in humans. Circulation 1995; 92: 2426–31
- Celermajer D. S., Sorensen K. E., Gooch V. M., Spiegelhalter D. J., Miller O. I., Sullivan I. D., et al. Non‐invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet 1992; 340: 1111–5
- Gokce N., Keaney J. F Jr., Hunter L. M., Watkins M. T., Menzoian J. O., Vita J. A. Risk stratification for postoperative cardiovascular events via noninvasive assessment of endothelial function: a prospective study. Circulation 2002; 105: 1567–72
- Gokce N., Keaney J. F Jr., Hunter L. M., Watkins M. T., Nedeljkovic Z. S., Menzoian J. O., et al. Predictive value of noninvasively determined endothelial dysfunction for long‐term cardiovascular events in patients with peripheral vascular disease. J Am Coll Cardiol 2003; 41: 1769–75
- Anderson T. J., Uehata A., Gerhard M. D., Meredith I. T., Knab S., Delagrange D., et al. Close relation of endothelial function in the human coronary and peripheral circulations. J Am Coll Cardiol 1995; 26: 1235–41
- Warnholtz A., Ostad M. A., Heitzer T., Thuneke F., Frohlich M., Tschentscher P., et al. AT1‐receptor blockade with irbesartan improves peripheral but not coronary endothelial dysfunction in patients with stable coronary artery disease. Atherosclerosis 2007; 194: 439–45
- Bonetti P. O., Pumper G. M., Higano S. T., Holmes D. R Jr., Kuvin J. T., Lerman A. Noninvasive identification of patients with early coronary atherosclerosis by assessment of digital reactive hyperemia. J Am Coll Cardiol 2004; 44: 2137–41
- Kannel W. B., Dawber T. R., McGee D. L. Perspectives on systolic hypertension. The Framingham study. Circulation 1980; 61: 1179–82
- Millasseau S. C., Kelly R. P., Ritter J. M., Chowienczyk P. J. Determination of age‐related increases in large artery stiffness by digital pulse contour analysis. Clin Sci (Lond) 2002; 103: 371–7
- Hayward C. S., Kraidly M., Webb C. M., Collins P. Assessment of endothelial function using peripheral waveform analysis: a clinical application. J Am Coll Cardiol 2002; 40: 521–8
- Otto M. E., Svatikova A., Barretto R. B., Santos S., Hoffmann M., Khandheria B., et al. Early morning attenuation of endothelial function in healthy humans. Circulation 2004; 109: 2507–10
- Plotnick G. D., Corretti M. C., Vogel R. A. Effect of antioxidant vitamins on the transient impairment of endothelium‐dependent brachial artery vasoactivity following a single high‐fat meal. JAMA 1997; 278: 1682–6
- Title L. Regarding ‘Endothelium‐dependent vasodilatation is impaired in both microcirculation and macrocirculation during acute hyperglycemia’. J Vasc Surg 1999; 29: 942–3
- Jarvisalo M. J., Jartti L., Marniemi J., Ronnemaa T., Viikari J. S., Lehtimaki T., et al. Determinants of short‐term variation in arterial flow‐mediated dilatation in healthy young men. Clin Sci (Lond) 2006; 110: 475–82
- Duffy S. J., Gokce N., Holbrook M., Hunter L. M., Biegelsen E. S., Huang A., et al. Effect of ascorbic acid treatment on conduit vessel endothelial dysfunction in patients with hypertension. Am J Physiol Heart Circ Physiol 2001; 280: H528–34
- Levine G. N., Frei B., Koulouris S. N., Gerhard M. D., Keaney J. F Jr., Vita J. A. Ascorbic acid reverses endothelial vasomotor dysfunction in patients with coronary artery disease. Circulation 1996; 93: 1107–13
- Heitzer T., Just H., Munzel T. Antioxidant vitamin C improves endothelial dysfunction in chronic smokers. Circulation 1996; 94: 6–9
- Ting H. H., Timimi F. K., Boles K. S., Creager S. J., Ganz P., Creager M. A. Vitamin C improves endothelium‐dependent vasodilation in patients with non‐insulin‐dependent diabetes mellitus. J Clin Invest 1996; 97: 22–8
- Munzel T., Genth‐Zotz S., Hink U. Targeting heme‐oxidized soluble guanylate cyclase: solution for all cardiorenal problems in heart failure?. Hypertension 2007; 49: 974–6
- Bastian N. R., Hibbs J. B Jr. Assembly and regulation of NADPH oxidase and nitric oxide synthase. Curr Opin Immunol 1994; 6: 131–9
- Griendling K. K., Sorescu D., Ushio‐Fukai M. NADPH oxidase: role in cardiovascular biology and disease. Circ Res 2000; 86: 494–501
- Warnholtz A., Nickenig G., Schulz E., Macharzina R., Brasen J. H., Skatchkov M., et al. Increased NADH‐oxidase‐mediated superoxide production in the early stages of atherosclerosis: evidence for involvement of the renin‐angiotensin system. Circulation 1999; 99: 2027–33
- Guzik T. J., West N. E., Black E., McDonald D., Ratnatunga C., Pillai R., et al. Vascular superoxide production by NADPH oxidase: association with endothelial dysfunction and clinical risk factors. Circ Res 2000; 86: E85–90
- Sorescu D., Weiss D., Lassegue B., Clempus R. E., Szocs K., Sorescu G. P., et al. Superoxide production and expression of nox family proteins in human atherosclerosis. Circulation 2002; 105: 1429–35
- Ohishi M., Ueda M., Rakugi H., Naruko T., Kojima A., Okamura A., et al. Enhanced expression of angiotensin‐converting enzyme is associated with progression of coronary atherosclerosis in humans. J Hypertens 1997; 15: 1295–302
- Diet F., Pratt R. E., Berry G. J., Momose N., Gibbons G. H., Dzau V. J. Increased accumulation of tissue ACE in human atherosclerotic coronary artery disease. Circulation 1996; 94: 2756–67
- Schieffer B., Schieffer E., Hilfiker‐Kleiner D., Hilfiker A., Kovanen P. T., Kaartinen M., et al. Expression of angiotensin II and interleukin 6 in human coronary atherosclerotic plaques: potential implications for inflammation and plaque instability. Circulation 2000; 101: 1372–8
- Nickenig G., Baumer A. T., Temur Y., Kebben D., Jockenhovel F., Bohm M. Statin‐sensitive dysregulated AT1 receptor function and density in hypercholesterolemic men. Circulation 1999; 100: 2131–4
- Fukui T., Ishizaka N., Rajagopalan S., Laursen J. B., Capers Q. T., Taylor W. R., et al. p22phox mRNA expression and NADPH oxidase activity are increased in aortas from hypertensive rats. Circ Res 1997; 80: 45–51
- Rajagopalan S., Kurz S., Munzel T., Tarpey M., Freeman B. A., Griendling K. K., et al. Angiotensin II‐mediated hypertension in the rat increases vascular superoxide production via membrane NADH/NADPH oxidase activation. Contribution to alterations of vasomotor tone. J Clin Invest 1996; 97: 1916–23
- Morawietz H., Weber M., Rueckschloss U., Lauer N., Hacker A., Kojda G. Upregulation of vascular NADPH oxidase subunit gp91phox and impairment of the nitric oxide signal transduction pathway in hypertension. Biochem Biophys Res Commun 2001; 285: 1130–5
- Hink U., Li H., Mollnau H., Oelze M., Matheis E., Hartmann M., et al. Mechanisms underlying endothelial dysfunction in diabetes mellitus. Circ Res 2001; 88: E14–22
- Landmesser U., Dikalov S., Price S. R., McCann L., Fukai T., Holland S. M., et al. Oxidation of tetrahydrobiopterin leads to uncoupling of endothelial cell nitric oxide synthase in hypertension. J Clin Invest 2003; 111: 1201–9
- Ohara Y., Peterson T. E., Harrison D. G. Hypercholesterolemia increases endothelial superoxide anion production. J Clin Invest 1993; 91: 2546–51
- White C. R., Darley‐Usmar V., Berrington W. R., McAdams M., Gore J. Z., Thompson J. A., et al. Circulating plasma xanthine oxidase contributes to vascular dysfunction in hypercholesterolemic rabbits. Proc Natl Acad Sci U S A 1996; 93: 8745–9
- Cardillo C., Kilcoyne C. M., Cannon R. O 3rd., Quyyumi A. A., Panza J. A. Xanthine oxidase inhibition with oxypurinol improves endothelial vasodilator function in hypercholesterolemic but not in hypertensive patients. Hypertension 1997; 30: 57–63
- Butler R., Morris A. D., Belch J. J., Hill A., Struthers A. D. Allopurinol normalizes endothelial dysfunction in type 2 diabetics with mild hypertension. Hypertension 2000; 35: 746–51
- O'Driscoll J. G., Green D. J., Rankin J. M., Taylor R. R. Nitric oxide‐dependent endothelial function is unaffected by allopurinol in hypercholesterolaemic subjects. Clin Exp Pharmacol Physiol 1999; 26: 779–83
- Nakazono K., Watanabe N., Matsuno K., Sasaki J., Sato T., Inoue M. Does superoxide underlie the pathogenesis of hypertension?. Proc Natl Acad Sci U S A 1991; 88: 10045–8
- Cleland J. G., Coletta A. P., Clark A. L. Clinical trials update from the Heart Failure Society of America meeting: FIX‐CHF‐4, selective cardiac myosin activator and OPT‐CHF. Eur J Heart Fail 2006; 8: 764–6
- Pritchard K. A Jr., Groszek L., Smalley D. M., Sessa W. C., Wu M., Villalon P., et al. Native low‐density lipoprotein increases endothelial cell nitric oxide synthase generation of superoxide anion. Circ Res 1995; 77: 510–8
- Vergnani L., Hatrik S., Ricci F., Passaro A., Manzoli N., Zuliani G., et al. Effect of native and oxidized low‐density lipoprotein on endothelial nitric oxide and superoxide production : key role of L‐arginine availability. Circulation 2000; 101: 1261–6
- White C. R., Brock T. A., Chang L. Y., Crapo J., Briscoe P., Ku D., et al. Superoxide and peroxynitrite in atherosclerosis. Proc Natl Acad Sci U S A 1994; 91: 1044–8
- Laursen J. B., Somers M., Kurz S., McCann L., Warnholtz A., Freeman B. A., et al. Endothelial regulation of vasomotion in apoE‐deficient mice: implications for interactions between peroxynitrite and tetrahydrobiopterin. Circulation 2001; 103: 1282–8
- Milstien S., Katusic Z. Oxidation of tetrahydrobiopterin by peroxynitrite: implications for vascular endothelial function. Biochem Biophys Res Commun 1999; 263: 681–4
- Forstermann U., Munzel T. Endothelial nitric oxide synthase in vascular disease: from marvel to menace. Circulation 2006; 113: 1708–14
- Schachinger V., Britten M. B., Zeiher A. M. Prognostic impact of coronary vasodilator dysfunction on adverse long‐term outcome of coronary heart disease. Circulation 2000; 101: 1899–906
- Heitzer T., Schlinzig T., Krohn K., Meinertz T., Munzel T. Endothelial dysfunction, oxidative stress, and risk of cardiovascular events in patients with coronary artery disease. Circulation 2001; 104: 2673–8
- Heitzer T., Baldus S., von Kodolitsch Y., Rudolph V., Meinertz T. Systemic endothelial dysfunction as an early predictor of adverse outcome in heart failure. Arterioscler Thromb Vasc Biol 2005; 25: 1174–9
- Perticone F., Ceravolo R., Pujia A., Ventura G., Iacopino S., Scozzafava A., et al. Prognostic significance of endothelial dysfunction in hypertensive patients. Circulation 2001; 104: 191–6
- Brevetti G., Silvestro A., Di Giacomo S., Bucur R., Di Donato A., Schiano V., et al. Endothelial dysfunction in peripheral arterial disease is related to increase in plasma markers of inflammation and severity of peripheral circulatory impairment but not to classic risk factors and atherosclerotic burden. J Vasc Surg 2003; 38: 374–9
- Verma S., Wang C. H., Lonn E., Charbonneau F., Buithieu J., Title L. M., et al. Cross‐sectional evaluation of brachial artery flow‐mediated vasodilation and C‐reactive protein in healthy individuals. Eur Heart J 2004; 25: 1754–60
- Kathiresan S., Gona P., Larson M. G., Vita J. A., Mitchell G. F., Tofler G. H., et al. Cross‐sectional relations of multiple biomarkers from distinct biological pathways to brachial artery endothelial function. Circulation 2006; 113: 938–45
- Juonala M., Viikari J. S., Alfthan G., Marniemi J., Kahonen M., Taittonen L., et al. Brachial artery flow‐mediated dilation and asymmetrical dimethylarginine in the cardiovascular risk in young Finns study. Circulation 2007; 116: 1367–73
- Blann A. D., Woywodt A., Bertolini F., Bull T. M., Buyon J. P., Clancy R. M., et al. Circulating endothelial cells. Biomarker of vascular disease. Thromb Haemost 2005; 93: 228–35
- Rajagopalan S., Somers E. C., Brook R. D., Kehrer C., Pfenninger D., Lewis E., et al. Endothelial cell apoptosis in systemic lupus erythematosus: a common pathway for abnormal vascular function and thrombosis propensity. Blood 2004; 103: 3677–83
- Werner N., Kosiol S., Schiegl T., Ahlers P., Walenta K., Link A., et al. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med 2005; 353: 999–1007
- Schmidt‐Lucke C., Rossig L., Fichtlscherer S., Vasa M., Britten M., Kamper U., et al. Reduced number of circulating endothelial progenitor cells predicts future cardiovascular events: proof of concept for the clinical importance of endogenous vascular repair. Circulation 2005; 111: 2981–7
- Dimmeler S., Aicher A., Vasa M., Mildner‐Rihm C., Adler K., Tiemann M., et al. HMG‐CoA reductase inhibitors (statins) increase endothelial progenitor cells via the PI 3‐kinase/Akt pathway. J Clin Invest 2001; 108: 391–7
- Boulanger C. M., Scoazec A., Ebrahimian T., Henry P., Mathieu E., Tedgui A., et al. Circulating microparticles from patients with myocardial infarction cause endothelial dysfunction. Circulation 2001; 104: 2649–52
- Boulanger C. M., Amabile N., Tedgui A. Circulating microparticles: a potential prognostic marker for atherosclerotic vascular disease. Hypertension 2006; 48: 180–6
- Tramontano A. F., O'Leary J., Black A. D., Muniyappa R., Cutaia M. V., El‐Sherif N. Statin decreases endothelial microparticle release from human coronary artery endothelial cells: implication for the Rho‐kinase pathway. Biochem Biophys Res Commun 2004; 320: 34–8
- Kerns W., Schwartz L., Blanchard K., Burchiel S., Essayan D., Fung E., et al. Drug‐induced vascular injury—a quest for biomarkers. Toxicol Appl Pharmacol 2005; 203: 62–87
- Schnabel R., Blankenberg S., Lubos E., Lackner K. J., Rupprecht H. J., Espinola‐Klein C., et al. Asymmetric dimethylarginine and the risk of cardiovascular events and death in patients with coronary artery disease: results from the AtheroGene Study. Circ Res 2000; 97: e53–9
- Cooke J. P. Does ADMA cause endothelial dysfunction?. Arterioscler Thromb Vasc Biol 2000; 20: 2032–7
- Sydow K., Munzel T. ADMA and oxidative stress. Atheroscler Suppl 2003; 4: 41–51
- Deanfield J. E., Halcox J. P., Rabelink T. J. Endothelial function and dysfunction: testing and clinical relevance. Circulation 2007; 115: 1285–95

