
Abstract
Purpose
Event-based clinical outcome trials have shown limited evidence to support guidelines recommendations to lower blood pressure (BP) to <130/80 mmHg in middle-aged and elderly hypertensive patients with diabetes mellitus or with general high cardiovascular (CV) risk. We addressed this issue by post-hoc analysing the risk of CV events in patients who participated in the Valsartan Antihypertensive Long-term Use Evaluation (VALUE) trial and compared the hypertensive patients with type 2 diabetes mellitus with all high-risk hypertensive patients.
Materials and methods
Patients were divided into 4 groups according to the proportion of on-treatment visits before the occurrence of an event (<25% to ≥75%) in which BP was reduced to <140/90 or <130/80 mmHg. Patients with diabetes mellitus (n = 5250) were compared with the entire VALUE population with high CV risk (n = 15,245).
Results
After adjustments for baseline differences between groups, a reduction in the proportion of visits in which BP was reduced to <140/90 mmHg, but not to <130/80 mmHg, was accompanied by a progressive increase in the risk of CV morbidity and mortality as well as stroke, myocardial infarction and heart failure in both diabetes mellitus and in all high-risk patients. Target BP <130/80 mmHg reduced stroke risk in the main population but not in the diabetes mellitus patients. Patients with diabetes mellitus had higher event rates for the primary cardiac endpoint and all-cause mortality driven by a higher rate of heart failure.
Conclusion
In the high-risk hypertensive patients of the VALUE trial achieving more frequently BP <140/90 mmHg, but not <130/80 mmHg, showed principally the same protective effect on overall and cause-specific cardiovascular outcomes in patients with diabetes mellitus and in the general high-risk hypertensive population.
Introduction
Randomised event-based clinical intervention trials have proven little evidence to support the recommendations of guidelines [Citation1–3] that in hypertensive people at high cardiovascular (CV) risk, with or without type 2 diabetes mellitus, blood pressure (BP) should be treated to <130/80 mmHg rather than to <140/90 mmHg [Citation4–6]. The Hypertension Optimal Treatment (HOT) Study randomised almost 19,000 hypertensive patients from the general population to three different diastolic BP targets, ≤80, ≤85 and ≤90 mmHg while systolic BPs remained above 140 mmHg. The primary endpoint was unchanged, possibly because of lack of statistical power [Citation7]. Hypothesis generating analysis of secondary endpoint suggested that target diastolic BP ≤80 mmHg prevented myocardial infarction in the general hypertensive population and the subgroup of diabetes mellitus benefitted markedly from the lower diastolic BPs [Citation7]. After HOT, no randomised clinical trial has investigated the optimal BP target in the general hypertensive population but narrowed the focus to diabetes mellitus patients [Citation8–10], stroke survivors [Citation11] and other patients without these groups [Citation12].
In the lack of clinical outcome trials designed to investigate the optimal BP target, investigating achieved BPs in relation to CV events and adjusting for confounders have become a feasible alternative [Citation13–15]. In the present study we analysed patients in the large database provided by the Valsartan Antihypertensive Long-term Use Evaluation (VALUE) trial in high-risk hypertensive patients [Citation16]. We aimed to test the hypothesis promoted by guidelines [Citation1–3] that the effects of BP reduction <130/80 mmHg are better than <140/90 mmHg for CV protection in general and that optimal BP target is similar in patients with diabetes mellitus compared to hypertensive patients with general high CV risk for a variety of reasons including diabetes mellitus.
Material and methods
Participants
The design and main results of the VALUE trial have been reported in detail previously [Citation16]. Briefly, VALUE was a multicenter, randomised, double-blind trial which compared the long-term effect of an antihypertensive treatment based on the angiotensin receptor blocker valsartan or the calcium-antagonist amlodipine on cardiac morbidity and mortality in hypertensive patients of any ethnicity with an age ≥50 years and with high CV risk. The qualifying risk factors for recruitment were predefined combinations of male gender, age and other risk factors or the presence of ECG-based left ventricular hypertrophy (with or without a strain pattern), proteinuria, increased serum creatinine, diabetes mellitus or a verified coronary, cerebrovascular or peripheral artery disease. Patients with renal artery stenosis, clinically relevant valvular disease, a recent (3 months) cerebrovascular event, coronary angioplasty or by-pass surgery, congestive heart failure requiring an ACE inhibitor and coronary disease requiring a beta-blocker were not included. Exclusion extended to pregnant women and individuals with severe hepatic disease.
Baseline data for the entire high-risk population and for patients with diabetes mellitus for both BP target <140/90 and <130/80 mmHg have previously been published [Citation15,Citation17] and therefore included here in the Online Supplemental Tables 1–4.
Blood pressure measurements and treatment
Both treated and untreated hypertensive patients were considered for the trial. Untreated patients were recruited if their systolic BP was between 160 and 210 mmHg and diastolic BP was <115 mmHg. Treated patients were recruited if their systolic BP was <210 mmHg and diastolic BP <115 mmHg. The recruited patients were rolled-over into one or the other arm of the trial after randomisation without a run-in phase. For valsartan treatment started with 80 mg daily and for amlodipine with 5 mg daily. The dose of either drug was doubled and hydrochlorothiazide (12.5 mg and 25 mg daily) and other antihypertensive drugs were added in sequential steps if BP was not reduced <140/90 mmHg. Angiotensin receptor blockers were excluded from the treatment algorithms and ACE inhibitors and calcium antagonists only allowed if required for conditions other than hypertension. Patients were followed for 4–6 years with visits performed monthly during the initial 6 months of treatment and at 6 months intervals thereafter. Blood pressure was measured three times during each visit, with the patient in the sitting position, after 5 min rest and 24 h post-dose. Blood pressure was measured using a calibrated standard sphygmomanometer or a validated digital device, and mean BP was calculated as the mean of all three readings.
Outcome
The primary endpoint of the study was time to first cardiac event, i.e. a composite of fatal or non-fatal myocardial infarction, sudden cardiac death or death from revascularization procedures or heart failure, heart failure requiring hospitalisation and emergency procedures to prevent myocardial infarction. Secondary endpoints were all events, fatal and non-fatal stroke, myocardial infarction, hospitalised heart failure, and CV, non-CV and all-cause mortality. An endpoint committee blind to treatment allocation adjudicated events.
Statistical analyses
Because the primary endpoint was not significantly different between the two treatment groups, data were pooled. From the total number of patients (n = 15,245), and similarly from the study participants with diabetes mellitus (n = 5250), four groups were considered according to the percentage of on-treatment visits in which BP was below 140/90 mmHg up to the occurrence of an event: <25%, 25 to 49%, 50 to 74% and ≥75%, as done in previous trials [Citation13–15]. The same four group subdivisions were used for the percentage of visits in which BP was reduced <130/80 mmHg, i.e. the target BP recommended by guidelines in a high CV risk condition [Citation1–3]. On the assumption that the BP found at a given visit reflected the value existing during the preceding between-visit interval, data were expressed as the percentage of time in which BP was reduced below the higher or lower value. For each group calculation was made of the incidence of the primary and secondary endpoints. The relative risk of each endpoint was assessed separately for the higher and lower BP target, using the Cox proportional hazard model and using the group in which BP control covered ≥75% of the on-treatment time as reference. To reduce the impact of potential confounders hazard ratios were adjusted for baseline covariates (age, gender, systolic BP, diastolic BP, body mass index, high serum total cholesterol [6 mmol/L, 240 mg/dl], diabetes in the total group, smoking, proteinuria, history of CV events and left ventricular hypertrophy). For baseline systolic BP and diastolic BP, the 5th degree polynomials were used to capture an extended range of possible relationships between BP and events. The same analyses were done in patients with diabetes mellitus at baseline (n = 5250) and this group was visually compared to the main group in . Two-sided p-values were calculated for trends versus the subgroup with ≥75% of the time with BP control. p < 0.05 was considered statistically significant without adjustment for multiplicity. Data are shown as means ± standard deviation (SD) or estimates with 95% confidence interval (CI).
Figure 1. Incidence (%) of morbid and fatal events in 4 groups of patients divided according to the proportion of the overall treatment duration (<25% to ≥75%) in which blood pressure (BP) was reduced <140/90 mmHg prior to the occurrence of an event. Squares indicate diabetic patients (n = 5250) and circles indicate all patients (n = 15,245). The primary endpoint was a composite of a variety of cardiac morbid and fatal events (see Material and Methods); CV: cardiovascular; MI: myocardial infarction; CHF: congestive heart failure. *All patients without GCP deficiencies and missing BP values.
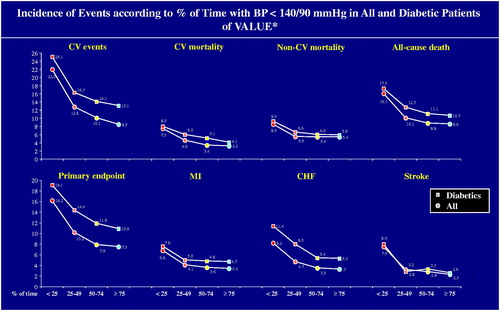
Figure 2. Percent increase taken from Hazard Ratios (HRs) of morbid and fatal events in 4 groups of patients divided according to the proportion of the overall treatment duration (<25% to ≥75%) in which blood pressure (BP) was reduced < 140/90 mmHg prior to the occurrence of an event. Diabetic patients (n = 5250) are compared with all patients (n = 15,245). The groups in which BP was reduced <140/90 mmHg for ≥75% of the time is used as reference and shown by the empty circle. CV: cardiovascular; MI: myocardial infarction; CHF: congestive heart failure; BMI: body mass index; SBP: systolic BP; DBP: diastolic BP; CVD: cardiovascular disease; LVH: left ventricular hypertrophy. *Adjusted for baseline covariates (age/gender/BMI/SBP/DBP/diabetes/CVD history/high cholesterol/LVH/proteinuria). §Statistically significant difference with group with BP <140/90 mmHg ≥75% of the time.
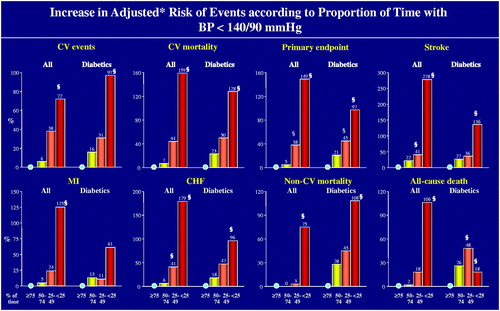
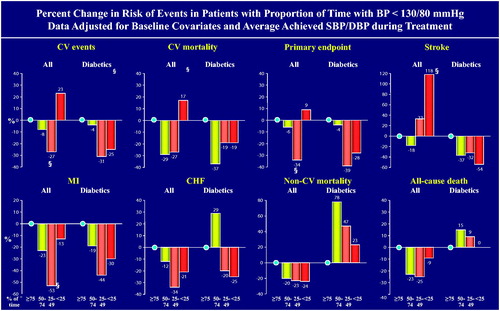
Figure 3. Percent increase taken from Hazard Ratios (HRs) of morbid and fatal events in 4 groups of patients divided according to the proportion of the overall treatment duration (<25% to ≥75%) in which blood pressure (BP) was reduced < 130/80 mmHg prior to the occurrence of an event. Diabetic patients (n = 5250) are compared with all patients (n = 15,245). The groups in which BP was reduced < 130/80 mmHg for ≥75% of the time is used as reference and shown by the empty circle. Calculated HRs were adjusted for baseline covariates, i.e. age, sex, body mass index, history of CV events, diabetes (not diabetes mellitus group), smoking, left ventricular hypertrophy, hypercholesterolaemia, proteinuria, systolic BP and diastolic BP. CV: cardiovascular; MI: myocardial infarction; CHF: congestive heart failure. §Statistically significant difference with group with BP <130/80 mmHg ≥75% of the time.
Results
Baseline characteristics in relation to time achieving target <140/90 mmHg
Supplemental Tables 1 and 2, for all patients and diabetes mellitus patients, respectively, show the baseline characteristics of the patients achieving a BP <140/90 mmHg over different proportions of the on-treatment period prior to the occurrence of the primary endpoint. Systolic BP and diastolic BP were progressively greater, and most CV risk factors progressively more common, from the longest to the shortest time (≥75% to <25%) with a BP <140/90 mmHg, with an expected concomitant progressive increase of average on-treatment BP.
Fractions of smokers and fractions of study participants with coronary disease were inversed, while heart rate was unchanged in diabetes mellitus, and baseline antihypertensive treatment, body mass index and fraction of patients with previous stroke or transient ischaemic attack were unchanged. Results were similar when groups were stratified according to BP values prior to the occurrence of secondary endpoints.
Event incidence and risk for a BP <140/90 mmHg
Both for the primary and for all secondary endpoints the event incidence increased progressively as the time with BP <140/90 mmHg decreased (). Patients with diabetes mellitus had higher event rates for the primary cardiac endpoint and all-cause mortality driven by higher rate of heart failure but not by higher rate of myocardial infarction.
With exception of non-CV mortality in the total group, the risk of any event also showed a steep progressive increase as the time with a BP <140/90 mmHg decreased when data were adjusted for baseline covariates, including systolic BP and diastolic BP values (). Non-CV mortality followed the same pattern in diabetes mellitus, likely explaining why all-cause death did not follow this pattern in diabetes mellitus ().
Baseline characteristics in relation to time achieving target <130/80 mmHg
Supplemental Tables 3 and 4 show the baseline characteristics of the patients achieving BP <130/80 mmHg over different proportions of the on-treatment period prior to the occurrence of the primary endpoint. Although the between-group differences were less pronounced and not invariably significant, baseline systolic BP and diastolic BP values as well as prevalence of several CV risk and disease factors increased progressively from the group with the longest to the group with the shortest time at BP <130/80 mmHg. There was an expected concomitant progressive increase of the on-treatment average BP values.
At variance from the findings shown in Supplemental Tables 1 and 2, fractions with antihypertensive treatment at baseline increased with BP control ≥75%. This was also the case for fractions of participants with coronary disease but not for fractions of smokers.
Event incidence and risk for a BP <130/80 mmHg
From the longest to the shortest time with BP <130/80 mmHg the incidence of stroke continued to show a progressive increase in the total group but not in the diabetes mellitus group. With the exception of a progressive increase in the risk of stroke, the risk of all other events did not show any consistent trend from the longest to the shortest time with BP <130/80 mmHg when data were adjusted for baseline covariates, including systolic BP and diastolic BP values ().
Discussion
In the high-risk hypertensive patients participating in the VALUE trial, both in the entire population and in the diabetes mellitus patients, the risk of CV morbidity and mortality, as well as myocardial infarction, heart failure and stroke, showed a progressive steep increase as the rate of BP control <140/90 mmHg decreased from ≥75% to <25% of the on-treatment time. We found a concomitant steep increase in the risk of these events when we adjusted the risks of these events for between-group differences in a large number of demographic and clinical variables. This was not the case, however, for the different rates of BP control <130/80 mmHg. For patients below these BP values, the adjusted overall morbidity and mortality risk, as well as (with the exception of stroke in the entire group, see below) the risk of cause-specific events, were unaffected by the frequency of BP control. Thus, while more frequent BP reductions <140/90 mmHg were highly protective, no further protection appeared by more frequent BP reductions <130/80 mmHg. Our findings provide evidence in support of the general BP target <140/90 mmHg in all middle-aged and elderly hypertensive patients with high CV risk, but does not support the need of pursuing an intensive BP target in these high-risk hypertensive patients as currently recommended by guidelines [Citation1–3].
In the subgroup of diabetes mellitus patients the relationship of the higher and lower BP targets with the incidence and adjusted risk of CV morbidity and mortality was similar to that of the entire VALUE population, i.e. maximal CV protection was achieved by reducing BP <140/90 mmHg with no further protection <130/80 mmHg. Our finding does not support the recommendation of guidelines of intensive BP reduction to <130/80 mmHg in diabetes mellitus [Citation1–3].
In the case of target BP <130/80 mmHg, the risk of CV event surprisingly does not increase (except for stroke in the general population) as the percentages of visits with a BP <130/80 mmHg decreases. In fact, the trend is even reverse, particularly in the diabetic population. As shown in , it seems that diabetic patients have less events when the percentage of visits with a BP > 130/80 mmHg is increasing. This could suggest that in these patients the ideal target should be between 130/80 and 140/90 mmHg.
One could also argue that the impact of the percentage of visits with an uncontrolled BP is less important when the target is defined at a lower level such as <130/80 mmHg. As adherence to therapy is probably the main determinant of the variability of BP control during the study, people in favour of a low target BP could argue that a target <130/80 mmHg makes patients less sensitive to variations in adherence (at least in terms of events). Yet, we have to admit that the number of patients below 130/80 mmHg is rather small.
Systolic BP reduction <120 mmHg in diabetes mellitus was not accompanied by prevention of CV morbidity and mortality except for stroke, the risk of which was reduced by 41% as a hypothesis generating secondary endpoint compared to patients remaining at systolic BP ≥130 mmHg in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study [Citation10]. As in the HOT Study [Citation7] and in the SPS3 study of previous stroke survivors [Citation11] in which similar secondary analyses or analyses in sub-groups showed CV protection, ACCORD may have been underpowered for the primary endpoint. However, taken together, in patients with diabetes mellitus and hypertension no study has ever shown benefit of intensive lowering of BP <130/80 mmHg and intensive BP lowering in diabetes mellitus remains an unproven hypothesis. Interestingly, the by far largest study to investigate BP target in diabetes mellitus patients with hypertension, the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) factorial trial (ADVANCE BP, n = 11,140) [Citation9], observed significant reduction in the primary CV endpoint. However, the achieved BPs in ADVANCE averaged 136/73 vs. 142/75 mmHg in the active treatment arm and in the placebo arm, respectively. Thus, neither the ADVANCE BP findings support intensive BP control <130/80 mmHg in diabetes mellitus patients.
However, secondary stroke reduction in several studies including in the overall high-risk population in the present study may suggest that ‘the lower the on-treatment BP the better’ may hold for cerebrovascular protection. Thus, intensive BP target <130/80 mmHg could be indicated whenever the risk of stroke represents a predominant component of the overall CV risk, such as in Asian patients [Citation18], or in patients with a previous cerebrovascular event in whom the risk of stroke recurrence exceeds that of cardiac events [Citation19].
Only 33% of the total VALUE patients achieved a BP <140/90 mmHg for ≥75% of the overall treatment duration, and in more than 45% of the patients this highly protective target BP remained unachieved for half of the treatment time. This confirms that consistent BP control is a difficult target to reach even in the context of randomised clinical trials with patients followed by expert investigators, and follow-up is more intensive than in clinical practice. Given the evidence that visit-to-visit BP variability may be an independent CV risk factor in this high-risk population [Citation20–22], the inconsistency of BP control may be one of the factors responsible for the persistently high residual risk in treated hypertensive patients [Citation23].
We compared diabetes mellitus patients with the entire population of high-risk hypertensive patients and not with the high-risk hypertensive patients with diabetes mellitus patients excluded. Our approach was therefore different from that of another study organisation supported by the National Institute of Health in the US [Citation10–12]. Statistically we could have excluded the diabetes mellitus patients from the entire high-risk population, but this seems unnatural to do as the diabetes mellitus patients otherwise are usually included in high-risk hypertension populations. Analysing the diabetes mellitus patients as a separate group on the other side seems natural because there are separate studies that include diabetes mellitus patients only [Citation8–10] and there are special guidelines for diabetes mellitus patients including treatment of hypertension [Citation1].
Study limitations
Our study had some other limitations. Only a limited number of patients achieved BP below 130/80 mmHg at rates greater than 50% or 75% of the treatment duration. This was particularly the case for the subgroup of diabetes mellitus patients, in whom the low rate of intensive BP control for 50% or more of the overall treatment duration may have been due to chance findings such as the lack of relationship between the BP reduction and the risk of stroke compared to the overall trial population. Because of post-hoc comparisons involving non-randomised groups, there is a possibility that our results did not depend on the achievement rates of higher or lower BP values but rather on differences in baseline characteristics. However, our estimates of CV risk were adjusted for a large number of baseline variables, including markers of asymptomatic hypertension mediated organ damage (left ventricular hypertrophy and proteinuria), that have an important impact on CV risk [Citation24,Citation25]. Although interpretation of post-hoc data requires caution, it seems reasonable to conclude that baseline confounders did not play a major role in our results.
We investigated middle-aged and elderly people with high-risk hypertension and thus, our data may not apply to people below the age of 50 years and people with low-risk hypertension in whom the residual risk may be small or negligible. In such populations it might be hypothesised that BP should be normalised at the outset, which could possibly eliminate the risk in the future associated with treated hypertension.
Finally, our data do not support the findings of intensive BP lowering in meta-analyses of treatment of people with high CV risk [Citation26]. We believe that this apparent discrepancy is explained by the fact that meta-analyses typically also include severely sick people with more advanced stages of the CV diseases including heart failure.
Implications
Our data provide evidence that in hypertensive patients at high CV risk a more consistent achievement of BP <140/90 mmHg leads to a major reduction in the risk of coronary events, heart failure, and stroke, a protective effect extending to cardiovascular and all-cause mortality and involving to a similarly degree patients with diabetes. With the possible exception of stroke, this does not occur for a more frequent control of BP <130/80 mmHg. Our findings suggest that BP should be consistently stabilised <140/90 mmHg during treatment in middle-aged and elderly patients with high-risk hypertension including patients with type 2 diabetes mellitus, but do not support the guidelines recommending the target <130/80 mmHg in these patients. Our findings are in line with a recent Cochrane analysis [Citation27].
Online_Supplement_Tables_1-4_DM___ALL_20.11.20.ppt
Download MS Power Point (270 KB)Acknowledgements
Dr. Eirik Olsen, MD, is supported by the Research Council of Norway. The VALUE trial (Valsartan Antihypertensive Long-Term Use Evaluation) was funded by an unrestricted grant from Novartis Pharma AG. The data file resides in the hands of the authors at Oslo University Hospital, Oslo, Norway. We are indebted to Dr. Tsushung A. Hua, PhD (deceased 2018), Unit of Biostatistics and Pharmacometrics, Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA for invaluable help through many years.
Disclosure statement
S.E. Kjeldsen has received honoraria from Merck GBaA, Sanofi and Takeda. R. Mo has received honoraria from Novartis. B. Holzhauer and D. Zappe are employees of Novartis Pharma. The other authors report no relevant conflicts of interest.
Data availability statement
The data that support the findings of this study are available from the corresponding author, S.E.K. upon dire needs.
References
- de Boer IH, Bangalore S, Benetos A, et al. Diabetes and hypertension: a position statement by the American diabetes association. Diabetes Care. 2017;40(9):1273–1284.
- Williams B, Mancia G, Spiering W, et al. 2018 Practice guidelines for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. Blood Press. 2018;27(6):314–340.
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71(6):1269–1324.
- Aksnes TA, Skarn SN, Kjeldsen SE. Treatment of hypertension in diabetes: what is the best therapeutic option? Expert Rev Cardiovasc Ther. 2012;10:727–734.
- Heimark S, Mariampillai JE, Narkiewicz K, et al. Which target blood pressure in year 2018? High Blood Press Cardiovasc Prev. 2018;25(2):151–100.
- Mariampillai JE, Eskås PA, Heimark S, et al. A case for less intensive blood pressure control: It matters to achieve target blood pressure early and sustained below 140/90 mmHg. Progress Cardiovasc Diseas. 2016;59(3):209–218.
- Hansson L, Zanchetti A, Carruthers SG, et al. Effects of intensive blood pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. Lancet. 1998;351(9118):1755–1762.
- Holman RR, Paul SK, Bethel MA, et al. Long-term follow-up after tight control of blood pressure in type 2 diabetes. N Engl J Med. 2008;359(15):1565–1576.
- Patel A, MacMahon S, Chalmers J, et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. 2007;370(9590):829–840.
- Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362:1575–1585.
- Benavente OR, Coffey CS, Conwit R, et al. Effects of blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomised trials. Lancet. 2013;382:507–515.
- Wright JT, Jr Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103–2116.
- Mancia G, Messerli F, Bakris G, et al. Blood pressure control and improved cardiovascular outcomes in the International Verapamil SR-Trandolapril Study. Hypertension. 2007;50(2):299–305.
- Mancia G, Schumacher H, Redon J, et al. Blood pressure targets recommended by guidelines and incidence of cardiovascular and renal events in the Ongoing Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial (ONTARGET). Circulation. 2011;124(16):1727–1736.
- Mancia G, Kjeldsen SE, Zappe DH, et al. Cardiovascular outcomes at different on-treatment blood pressures in the hypertensive patients of the VALUE trial. Eur Heart J. 2016;37(12):955–964.
- Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet. 2004;363(9426):2022–2031.
- Olsen E, Holzhauer B, Julius S, et al. Cardiovascular outcomes at recommended blood pressure targets in middle-aged and elderly patients with type 2 diabetes mellitus with hypertension. Blood Press. doi: 10.1080/08037051.2020.1855968.
- Kubo M, Kiyohara Y, Kato I, et al. Trends in the incidence, mortality, and survival rate of cardiovascular disease in a Japanese community: the Hisayama study. Stroke. 2003;34(10):2349–2354.
- Arima H, Anderson C, Omae T, et al. Effects of blood pressure lowering on intracranial and extracranial bleeding in patients on antithrombotic therapy: the PROGRESS trial. Stroke. 2012;43(6):1675–1677.
- Mehlum MH, Liestøl K, Kjeldsen SE, et al. Blood pressure variability and risk of cardiovascular events and death in patients with hypertension and different baseline risks. Eur Heart J. 2018;39(24):2243–2251.
- Mehlum MH, Liestøl K, Wyller TB, et al. Blood pressure variability in hypertensive patients with atrial fibrillation in the VALUE trial. Blood Press. 2019;28(2):77–83.
- Mehlum MH, Liestøl K, Kjeldsen SE, et al. Blood pressure–lowering profiles and clinical effects of angiotensin receptor blockers versus calcium channel blockers. Hypertension. 2020;75(6):1584–1592.
- Thomopoulos C, Parati G, Zanchetti A. Effects of blood pressure lowering on outcome incidence in hypertension. 3. Effects in patients at different levels of cardiovascular risk. Overview and meta-analyses of randomized trials. J Hypertens. 2014;32(12):2305–2314.
- Mancia G, Carugo S, Grassi G, et al. Prevalence of left ventricular hypertrophy in hypertensive patients without and with blood pressure control: data from the PAMELA population. Pressioni Arteriose Monitorate E Loro Associazioni. Hypertension. 2002;39(3):744–749.
- Schmieder RE, Mann JF, Schumacher H, et al. Changes in albuminuria predict mortality and morbidity in patients with vascular disease. J Am Soc Nephrol. 2011;22(7):1353–1364.
- Xie X, Atkins E, Lv J, et al. Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: updated systematic review and meta-analysis. Lancet. 2016;387(10017):435–443.
- Saiz LC, Gorricho J, Garjón J, et al. Blood pressure targets for the treatment of people with hypertension and cardiovascular disease. Cochrane Database Syst Rev. 2020;9:CD010315.