
ABSTRACT
Introduction
Depression has a negative impact on millions of people worldwide, necessitating research into appropriate therapeutic methods. The aim of this qualitative study is to investigate how music therapy clients experience listening to their own clinical improvisations at home, as a part of treatment for depression.
Method
Adults with major depressive disorder were offered 12 individual sessions of bi-weekly integrative improvisational music therapy, as part of a randomised controlled trial. Participants were asked to complete an online diary after listening to their clinical improvisations. Reflexive thematic analysis was performed on diary entries, and content analysis was applied to music therapists’ reports.
Results
Fourteen of 32 participants submitted a total of 58 diary entries. Participants' experiences were represented by five themes: music (playing, listening, music perception, music parameters), therapy (therapeutic processing, illness, music therapy trial), emotions (positive emotions, negative emotions, other emotions), embodiment (body parts, sensations, actions) and narrative (chronology, symbolic references). Music therapists’ reports indicated that low compliance and negative experiences during the task could be affected by severity of depression, and ease of use of the technological interface.
Discussion
Participants’ experiences varied from extremely negative to positive in every theme, finding music they produced beautiful or hideous, feeling proud or ashamed of making it, being energised, or exhausted by it, feeling supported or pressured by the music therapist, and recalling happy or terrifying memories. The findings suggest that a homework task can affect the therapeutic process in both positive and negative ways and should be further researched before implementation.
Introduction
Depression is a common mood disorder, affecting more than 300 million people worldwide and linked to over 700,000 deaths by suicide every year (World Health Organization, Citation2021). It is a serious health condition that impairs professional, domestic, and social functioning and is recognized as one of the leading causes of disability worldwide (National Institute of Mental Health, Citation2022; World Health Organization, Citation2021). A combination of psychotherapy and medication is recommended as the best treatment plan (Kamenov et al., Citation2017; Nord et al., Citation2021), but current methods are not sufficiently effective as the risks of relapse and suicidality remain high (Baldessarini et al., Citation2017; De Maat et al., Citation2006; Hengartner et al., Citation2018).
Research shows that music therapy is successfully used to reduce the symptoms of depression and increase the general functioning of those who suffer from it (Aalbers et al., Citation2017; Maratos et al., Citation2008). Music therapy is based on musical experiences and a client–music therapist relationship (Bruscia, Citation2014; Jacobsen et al., Citation2019). During a course of music therapy, the client is encouraged to engage in a variety of active (e.g. playing an instrument or singing) and receptive (listening) methods, often combined with verbal dialogue (Davis et al., Citation2008). Music therapy can be in individual or group settings, depending on a client’s needs and the capacity of the treatment facility. Improvisational music therapy enables clients to spontaneously express themselves and interact with a music therapist through produced sounds. Clinical improvisation allows non-verbal processing and communication, which is especially advantageous in the case of depression, as it often impairs verbal communication (Newell et al., Citation2018). It is important to note that music therapy clients typically have no, or very little, musical training, thus the music produced in the therapeutic setting is often very simple in form and not intended to be experienced as an object of aesthetic appreciation (Aigen, Citation2005). Whilst the literature and clinical practice suggest that music therapy is an efficacious treatment for depression, the inner mechanisms of complex music-based interventions are not yet fully understood (Bonde, Citation2016; Maratos et al., Citation2018).
Listening to music is widely utilised in receptive music therapy. In the Guided Imagery and Music (GIM; Grocke & Moe, Citation2015; Muller, Citation2012) approach clients immerse themselves in Western classical music and talk about their experiences to a music therapist. GIM is found to be an effective treatment for various mood disorders, including depression (Hammer, Citation1996; McKinney & Honig, Citation2017; McKinney et al., Citation1997). In Analytically Oriented Music Therapy (AOM), listening to recordings of client--music therapist improvisations is incorporated into the music therapy session. Both client and music therapist listen to the recordings and will talk and/or play about it afterwards (Eschen, Citation2002; Scheiby, Citation2010). Differently from GIM and AOM, home listening tasks, as a part of active music therapy, do not have an element of immediate music therapist support. It is not clear to what extent that would affect the process and its outcomes. There is broad literature on the self-regulatory benefits of music listening in everyday life (Baltazar & Saarikallio, Citation2016; Chin & Rickard, Citation2014; Groarke & Hogan, Citation2018; Van den Tol & Edwards, Citation2015), however, these studies do not address how music therapy clients experience their own clinical improvisations without immediate music therapist’s support.
Homework is a commonly used method in various therapeutic approaches, and findings from cognitive behavioural psychotherapy research indicate that people with depression can greatly benefit from it (Kazantzis et al., Citation2000, Citation2010; Mausbach et al., Citation2010; Thase & Callan, Citation2006). Homework is a task that is carried out by the client independently between therapy sessions with the goal of aiding therapeutic processing. To date it has not been widely used in active music therapy. In Emotion-regulating Improvisational Music Therapy (EIMT), Aalbers et al. (Citation2020, Citation2021) suggest using homework as a means of experimenting with feelings, expression, bodily responses, and action tendencies in order to improve emotion regulation. They propose 10 identically structured sessions of music therapy, and the assigned homework can vary each time and be music related, such as singing or playing an instrument, or involve non-musical activities such as talking, writing, or walking (Aalbers et al., Citation2019). In Group Impromptu Music Therapy (GIMT) clients are required to record their positive coping strategies and feelings in the face of emotional difficulties. Although music is not involved in the homework itself, the authors suggest that the task of self-reflection enhances the effectiveness of the GIMT intervention (Zhang et al., Citation2022).
Given all the above, it is plausible that engaging in music therapy homework between sessions could aid therapeutic goals, might increase motivation, and deepen self-referential processing and understanding. This study is embedded into a larger randomised controlled trial (RCT) for depression (Erkkilä et al., Citation2019, Citation2021), which aimed to examine whether additional components, such as homework or slow-paced breathing would result in more successful recovery. The results of this RCT showed that listening homework was not as effective as the breathing intervention in reducing the symptoms of depression. To date, no qualitative data from this randomised controlled trial have been published. The aim of this study is to investigate how music therapy clients experienced the task of listening to their own clinical improvisations at home. The two main objectives of this study are (a) to discover what is relevant for participants personally and (b) to ascertain whether music listening homework has potential as a method in improvisational music therapy, as seen from both clients’ and music therapists’ perspectives.
Method
Design
This process evaluation study is embedded in a 2 × 2 factorial RCT for depression (Erkkilä et al., Citation2019, Citation2021). All participants enrolled in the RCT were offered 12 face-to-face bi-weekly one-hour sessions of individual music therapy over a period of six weeks. Half of the participants were instructed to listen to their improvisations at home in addition to their music therapy sessions. These participants are the subjects of this study.
Participants
A number of 32 adults aged between 21 and 57, with a primary diagnosis of major depressive disorder (F32/F33 according to ICD-10) were assigned to the home listening and diary writing task between their music therapy sessions. Participants were not required to have any musical skills but were excluded from the trial in instances of co-occurring mental illnesses (e.g. psychosis, bipolar disorder, personality disorders, severe substance misuse).
Music therapy
Integrative Improvisational Music Therapy (IIMT) is a versatile and flexible model suitable for a wide variety of client populations (Erkkilä et al., Citation2019, Citation2021). IIMT is based on psychoanalytical music therapy and integrative psychotherapy, rooted in the belief that musical expression is connected to abstract mental content and experiences, thus representing unconscious emotional processes (Bruscia, Citation1998; Erkkilä, Citation2004; Erkkilä et al., Citation2012) that take place in ever changing dynamic life circumstances (Norcross & Goldfried, Citation2005). Free improvisation is an integral part of IIMT, where clients can spontaneously express themselves in a dyadic musical interaction with a music therapist. During music therapy sessions, clients were able to choose to improvise on acoustic djembe drums or digital mallet instruments (one for the client and one for the music therapist). Clinical improvisations can be either completely free, or follow a theme proposed by the music therapist or the client. Improvisations are typically followed by a verbal interaction, where clients can verbalise and further process their experiences.
Procedure
Eleven clinically trained music therapists with extensive prior experience in IIMT underwent a 24-hour training course in preparation for this RCT and continued to receive group supervision every two weeks during the clinical work phase of the study to ensure treatment fidelity. Music therapists reminded participants to listen to their clinical improvisations at home and to keep a digital diary. A participant’s home diary had instructions to write down any feelings, thoughts, memories, bodily sensations, or other experiences that arose while listening to their improvisations. Music therapists were encouraged to discuss the client’s experiences of doing homework during the subsequent therapy sessions, but they were allowed to be flexible with therapy structure.
Data collection
Data were collected between 2018 and 2019 in the Music Therapy Clinic for Training and Research at the Department of Music, Art, and Culture Studies of the University of Jyväskylä. Participants were recruited via a newspaper advertisement. During music therapy sessions, music therapists made audio recordings of clinical improvisations using Pro Tools 11.3.1. and shared them with clients using continuous file synchronisation program Syncthing (version 0.14.39). In between music therapy sessions, each participant was able to listen to as many improvisations as often as they wanted using the music player Cantata (version 2.2) on their home computer. Participants were asked to fill in an individualised online diary after each listening instance. After all the participants completed their music therapy sessions, the music therapists were asked to fill in an online survey about their experiences and opinions regarding the home listening task.
Ethical considerations
This study received ethical approval from the Ethical board of Central Finland health care district, 7 September 2017, ref.: 17 U/2017, and was also registered at the International Traditional Medicine Clinical Trial Registry (ISRCTN11618310). All participants were required to sign informed consent during the initial assessment. Anonymized information was used to ensure that no participants could be identified from research data.
Data analysis
Deductive analysis of music therapists’ reports was performed using the content analysis method, whilst inductive diary data analysis was performed using the reflexive thematic analysis method. Semantic and latent coding was applied to the diary entries, following the six steps suggested by Braun and Clarke (Citation2019, Citation2021):
Data familiarisation. The first author was involved in the study design and data collection and was familiar with the material from its inception. Subsequently, the first author was involved in the translation process, involving multiple meetings with a translator. After the translator finished their work, the first author double-checked the text, compared it to the original text to ensure utmost accuracy, and entered the data into Atlas.ti software (version 22).
Initial code generation. The first author created detailed initial codes in the Atlas.ti software. After the first round of coding the first author decided that, for the purposes of this paper, codes would only be analysed that were mentioned by at least two participants. It is emphasised that this decision was not made for the purposes of reliability or credibility, because reflexive thematic analysis is based on an inherently interpretivist paradigm. This decision was made to enable a single researcher to code a large amount of data and construct a coherent overview from a multitude of experiences and opinions.
Generating (initial) themes. Four themes – MUSIC, THERAPY, EMOTIONS, and EMBODIMENT – were distinct from the very beginning. Remaining codes were initially assigned to themes that changed in the subsequent coding process.
Theme review. At this stage Authors 2 and 3 were briefed and included in discussions. It was decided that although participants shared a lot of details about their lives, for the purposes of this paper, three initial themes (Internal world, External world, and Chronology) could all be merged into NARRATIVE.
Theme defining and naming. In later coding stages, it became apparent that concepts needed clear definitions, because some codes were overlapping. For example, in memos about the THERAPY theme, clearcut distinctions were made between naming the issues (stating a problem), insight (making a connection between the cause and effect), dealing with issues (identifying an action that could potentially help), and change (executing the action).
Report production. To aid readability, themes are written in uppercase (e.g. NARRATIVE), subthemes are bold (e.g. Chronology), codes are italicised and underlined (e.g. Childhood), and subcodes are italicised (e.g. School). The first author noted that the initial manuscript did not reflect all participants’ voices equally. Apparently, the software was affecting the selection of quotes, biassing towards participants with lower numbers. Consequently, the first author intentionally included quotes from all participants by scrolling down the Quotation list using the Atlas.ti Code Manager, and not just choosing the first few quotes for the code. Lastly, all the authors reviewed the manuscript and provided their feedback.
Results
Homework task compliance was low with only 14 participants out of 32 taking part in this requirement. In total, 14 participants produced 58 diary entries containing 19,041 words. Eight participants wrote 1–3 entries (151 words per entry on average) whilst six participants wrote more than three entries (95 words per entry on average).
Depressed clients’ experiences of listening to their own clinical improvisations at home can be summarised by five main themes, namely MUSIC, THERAPY, EMOTIONS, EMBODIMENT, and NARRATIVE, comprising 15 subthemes in total (see ). These codes arose from very rich data (see supplementary online material for more details); therefore, they capture only the most salient themes regarding the subject of this paper.
Figure 1. Themes and subthemes from depressed participants’ diaries
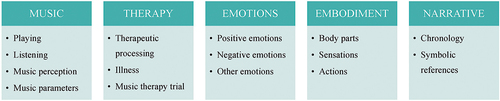
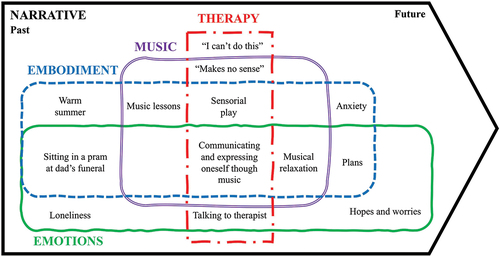
It is important to note that although codes within a theme were mutually exclusive (e.g. a single musical activity is either Playing or Listening, not both), a single code could appear in different themes (e.g. the same activity can be both EMOTIONAL Playing and EMBODIED Playing). An illustration, taken from the first author’s analytic memos, is presented here to aid a conceptualisation of the data and show the interconnectedness of themes (). Themes are exemplified with relevant quotes from participants (P, number). Although diaries were translated, quotes from them are presented in as close to original style and idiosyncrasy as possible.
Figure 2. Illustration of the diary themes and case examples from participants’ diaries
Music
Playing
Participants often reminisced about their music-making experiences during music therapy, as making music was a fairly new experience to the majority of them, whether it was a Negative (“I got annoyed when I performed and tried to imitate the therapist’s playing, I also noticed I was ashamed of own playing and hands and my being, I didn’t understand the point of playing” P10) or Positive (“So lovely to play together because they have supported me approvingly with their own playing” P24). Participants also mentioned the importance of Skills (“I don’t know what that feeling should sound like let alone how to play it with instruments I don’t know how to play” P8), sometimes admiring others, other times wishing to have the ability to express themselves musically.
Listening
Valence of the Listening homework was positive (“I was delighted as I was listening to our playing” P24), neutral, or even negative (“Listening felt boring and unpleasant” P8). Valence varied not only from person to person, but day-to-day for the same individual (“I wonder what the listening will feel like today” P16). Some participants also mentioned an Impact on their body (“During the listening, there is a mild ‘pain’ that spreads on one side of my head” P16), others considered a general impact of the task on their lives (“Listening to this sort of thing could be useful when I need to be ready to do something” P21). For some participants, it evoked a wish to play outside the therapeutic setting (“With an access to a piano, I continued playing over the track with headphones on” P7), or to share it with people around them (“The desire to play said music to my loved ones” P86).
Many participants noted differences in engagement and experiences of Listening vs. Playing (“The sorrow that burst out now while listening is completely different from the one when I played” P43), and most appeared to have higher engagement when playing with the music therapist (“When listening to it, it doesn’t have as strong an effect, and I can’t get inside the feeling as when I played it” P43). Some, however, had an opposite reaction and gained new insights when listening to improvisations at home (“I thought that maybe I don’t feel really anything in particular … However, when listening to the recordings afterwards … listening brought up feelings of being moved and significance” P7).
Music perception
Participants often noted the perceived beauty or lack of it in their improvisations. Aesthetic appreciation was a positive resource for some (“Joy of beautiful, peaceful music” P24), but others found Inaesthetic properties of music incredibly distressing (“That chaos music is so terrible, I can’t stand it for long” P24). Interestingly, traditional beauty was not always considered a positive in the context of music therapy, showing that participants understood the differences between therapeutic improvisation and artistic music (“Do I dare … play in a way that sounds ugly (that is, to play ‘wrong’)” P24).
Musical expression was appreciated by many participants (“Playing together with the therapist creates a space and permission for me to handle precisely the things I want to handle and express on an emotional level” P7). Multiple participants noticed differences in their ability to express themselves, depending on instruments (“Expressing myself is considerably more limited with the Djembe drum than with keyboard instruments” P86). Some participants were able to connect with the music during the session but experienced No connection listening at home (“When you play you are inside of the feelings and when you listen you are outside as a ‘listener’. And you can’t get the same feeling as by playing” P43). Others were not able to connect at all (“I notice myself performing and I’m irritated for it, I don’t feel the playing pleasant, but rather I try to play for the sake of others” P10). Some participants had No recognition of their own music (“The play didn’t look like me. As if someone else had played” P75). Interestingly, these experiences of unfamiliarity sometimes would dissipate over time (“Eventually the track began to sound familiar after all and I felt lighter” P7).
Music parameters
In this trial participants could play either Djembe (“The drum is a powerful instrument, it frustrates me that the power doesn’t convey through the recording” P89) or Piano (“I was able to express my thoughts and feelings through playing the piano” P3), often reflecting on the differences between the two (“As I’m listening to the drums the anxiety is milder, and the relief/forgetting is milder with the keyboard” P87). Other instruments came up in participants’ memories (“when two friends were pumping air to the harmonium as the teacher played” P70; “Playing the violin … HAD to play because I had a private tutor” P71). Participants often reflected on Themes assigned to improvisation (“During the ‘pain’ play there were sharp shrilling feelings” P43). Imagery induced by music listening was detailed and evocative (“Weirdly my own funeral and that my Ex would be there” P66; “A feeling of a day on a meadow with white clouds in the sky” P46), but sometimes improvisations were appreciated for Music in general (“It sounds like something from a piece of classical music” P89).
Volume was mostly mentioned due to technical recording issues, but sometimes it was mentioned as a perceptual experience (“It felt as if the background noise increased at the same time, even though in reality it did not get any louder” P21) or an aspect of performance (“I pressed the keys as quietly as possible when playing, barely audibly” P87). Although participants lacked musicological terminology, they often referred to Pitch (“high pitch sounds annoy me” P70) and Rhythm (“drumming reminded me of old PE classes where there was a steady rhythm in the background” P46). Dissonance came up in both positive and negative regards (“I’m not sure why I’m fascinated by discords” P89; “Piano 2 was conflicting and dissonant, I did not like it” P10).
Therapy
Therapeutic processing
Participants engaged in therapeutic processing with varying degrees of depth, from Naming an issue (“I get stuck and start repeating myself” P16), having an Insight (“I was supporting and thinking about another person, meaning I had placed some of my parents into my therapist.” P24), then Dealing with issues (“searching for another way to react, to take space and to maintain it despite the provocations” P16), and finally achieving Change in feelings or behaviours (“Bitterness also flashes in my mind, but not the desire for revenge anymore as some time before” P 16).
There were many descriptions of therapeutic work with Inner child (“Between the music and my most inner self there is a curtain, which prevents the streams from flowing” P75) or more abstract Inner space (“Sinking into my own world, my territory” P43), which are protected by creating Boundaries (“must be able to limit things even with your circle of friends” P71) and using inner Resources (“A sense of resilience” P 86) as well as Support from music therapist (“Therapist uses their playing to support the decisions I’ve made with my playing” P24) or other people in their lives (“I have good friends and they will help me survive” P71).
Diaries revealed that participants engage in a lot of Self-criticism (“Am I intentionally playing behind, or am I truly this unmusical?” P98), Comparing oneself to others (“As a child though, out the three siblings I was the most ‘well behaved’” P16), and had a Negative worldview (“I feel strongly about the injustice and exasperation and guilt over the state of the world” P8). There was also a lot of trauma-related content, whether it is flashbacks of Abuse and criticism (“POLICE, SMUGGLING AMPHETAMINE, MONEY, SATAN, BRUISES, CUTS” P71), describing Fight-flight-or-freeze response (“I have not been able to channel these feelings towards constructive actions but rather they utterly paralyze me” P8), experiencing Forcing (“I’m straining myself to get at least some thoughts or feelings or bodily sensations to tell about in here” P98), or being crushed by Expectations (“To be a good daughter, godmother, sister, partner, member of society and to be good at one’s job” P8). Other Therapeutic Processing codes are Altered state of consciousness, Avoidance, Goals, Confidence, Confidentiality, Controlling, Interaction with music therapist, Music therapist, Music therapy, Session, Self-esteem.
Illness
Although participants were in music therapy for Depression (“all I see around me is work, only the needs for improvement, only exhausting trials one after another” P102), they most often mentioned Anxiety (“Draining bodily anxiety, lack of energy and willingness” P87). Several participants referred to Medications (“Medications unfortunately dull the experience of feelings both in the good and in the bad” P16). Other disorders were mentioned when talking about people in their lives (“my anger towards my narcissistic parent as well as the traumas they have caused” P24, “They thought I was schizophrenic, even friends” P71), whilst Wellbeing was considered as an aspiration (“together with my therapist we have found appropriate goals for my wellbeing which we have named gentleness and will” P7).
Music therapy trial
Participants experienced Writing in both positive (“I should write my thoughts down more and to start making music more actively” P47) and negative (“Putting things into words doesn’t feel good right now” P87) ways. Questionnaires and other forms for the trial induced stress (“it is difficult to focus on listening when in my mind I’m planning what to write down in this form” P98). Many participants reacted negatively to Recording issues (“The plays from the last time haven’t appeared on the computer” P87), whilst being in a Music therapy trial compromised the therapeutic relationship (“Even if I would be able to start trusting the therapist at some point, the camera I will never trust” P87; “They have so much to do with relationship and are therefore private, so I don’t think I’m going to write them here” P40).
Emotions
Positive and negative emotions
Emotions were experienced when playing, listening, thinking of personal therapeutic issues, or remembering the past. Negative Emotions were feelings causing distress, such as Disappointment (“In my latest therapy session, I told the therapist that I’m disappointed in myself in the fact that I am not getting better” P7), Fear (“Pain of what the children have been forced to experience and now to hide out of fear and loyalty” P43), Frustration (“In the end the playing was long, it made me frustrated and feeling bored about how the play won’t end already” P43). Other Negative Emotions codes were Anger, Annoyance, Apathy, Bitterness, Boredom, Bother, Distress, Embarrassment, Emptiness, Fed up, Grief, Irritation, Longing, Loneliness, Melancholy, Misery, Nervousness, Nostalgia, Offence, Sadness, Shame, Sorrow, Stuck, Suffering, Unhappiness, Unpleasant, Unsafe, Unsure, Upset. Positive Emotions were pleasurable, for example, Empowerment (“A state of calm, balancing, good feeling, empowering, strengthening” P43), Pride (“I even managed to enjoy listening to the last two improvisations and felt proud of myself” P3), Safety (“I experienced safety and clarity, softness in the songs” P12), and Courage (“It felt particularly good in the bottom of my soul when my inner child finally had the courage to play melodies from high and the therapist’s base notes reinforced my playing” P24). Other Positive Emotions codes were Amusement, Calmness, Contentment, Delight, Enjoyment, Excitement, Freedom, Fun, Gentleness, Gratefulness, Happiness, Hope, Interest, Joy, Love, Loveliness, Luck, Moved (emotion), Peace, Pleasure, Relief, Satisfaction, Serenity, Surprise, Tranquillity, Wonder.
Other emotions
Sometimes, emotions were described in a crude manner, such as Bad (emotion) (“These experiences feel bad” P43), Good (emotion) (“It felt good and now listening to the recordings, I am even more convinced that it pays to play” P7), or Emotions in general (“Perhaps the feelings were too heavy” P87). Many participants were Unable to identify their emotions (“It is difficult for me to separate my feelings from my thoughts” P7). In the second round of coding, three codes were created to highlight latent emotional processing: Numbness (“I try to actively think ‘well, how does this feel like now’ and then it feels like there’s no more room in my head or my body for anything else” P98), Mixed emotions (“Wonder, sorrow, familiarity” P12), and Transition between emotions (“First the head is spinning, feeling of chaos, as the playing becomes more serene, satisfaction and joy” P24).
Embodiment
Body parts
Some Body Parts were mentioned with regards to emotions (Chest: “Now that there seldom is a physical sensation attached to them, differentiating feelings is hard. Before (years ago) the feeling of joy for example would splash in my chest” P8; Body: “Because I didn’t feel gratitude in my body, I experienced the feeling as incomplete, merely as a thought” P8), whilst others were used in describing a solely embodied experience (“I looked at my body from the outside – it moved outside into an aesthetic experience independent of me, or I moved it a bit kind of like a marionette, as if playing Puppet Theatre for myself” P87). Other Body Parts codes were Back, Eyes, Forehead, Hands, Head, Heart, Limbs, Neck, Shoulders, Stomach, and Torso.
Sensations
Sensations were related to physical impact, such as Heaviness (“heavy feeling of endless misery in chest and stomach” P87), Squeezing (“Annoyance is a tightening in my forehead and a burning in my eyes and a slight squeeze in my chest” P8), lack or surplus of Energisation (“I was being energized mentally and physically” P21), or related to senses (Smell: “The surroundings, lights, colours, sounds, and words, even scents” P16). Other Sensations codes were Chills, Cold, Fumbling, Lump, Pain, Palpitations, Pressure, Splash, Stiffness, Tightening, Tingle, Touch, Unspecified, Warmth, Comfort, Darkness, Exhaustion, Lack of energy, Lightness, Relaxation, Restfulness, Restlessness, Strength, Stress, Tiredness.
Actions
Actions, differently from Sensations, could be somewhat observed from the outside, and ranged from negative, such as Sweating (“Sweating, shaking and exhaustion during the listening” P87), to positive, such as Smiling (“Listening to the piece made me smile” P12) or an Urge to move (“After a while you feel like putting the drumming on the speakers and dance and trash” P98). Other Actions codes were Breathing, Crying, Laughing, Moving, Shaking, Sitting, Sleeping.
Narrative
Chronology
Past was mostly stories of important people, such as Father (“Father hasn’t been able to express in words that he loves” P12), Mother (“My violent mother admitted her mistake and apologized to me” P24), Extended Family (“Mother’s funeral when I stood alone, away from the other siblings” P12), Romantic Relationships (“husband, would beat the children with an old-fashioned thick leather belt with a large iron buckle” P43; “My Ex, good times with them” P66) and Children (“I wasn’t allowed to meet the children in years” P71). Other codes of Past related to environments and events, such as School (“drumming reminded me of old PE [physical education] classes where there was a steady rhythm in the background of the movement” P46; “boys from the other class would harass with their talking about sex” P66), Childhood (“Yearning for the freedom of childhood, no demands from adulthood” P71), Job (“There were light and uplifting memories from the work trial” P43), and Experiences in general (“skiing on a frozen lake by myself. Snow is falling slowly, and it is completely silent” P46).
In Present, Current State varied from being positive (“It has been an otherwise good morning (behind me is the first good night’s sleep in a long time)” P16) to negative (“This latest play is quite woeful … it reflects my mental state quite well” P87). Environment was mentioned when it was too distracting because of sounds (“Normally I am not bothered by background noise, but as I was trying to listen here, focused, it did bother me” P21) or tidiness (“In a clear environment, the mind stays more serene as well, as opposed to in a cluttered one” P24). Family was mentioned as a distraction (“Confusion in the head caused by family hassle around me as I’m listening to the music” P24) or as positively contributing to a shared experience of listening (“My daughter joined me in listening to the impro, which evoke a warm sensation” P3). Friends were mentioned as a protective factor or a cause of interpersonal issues, whilst Occupation was discussed in terms of ambition (“I would like to find a direction for my studies, to be a proper student, I want to dare more” P7); or as a stress inducer (“to calm myself in listening to music during the everyday life … in the middle of a workday” P86).
Future included Hopes (“Arousing interest in various future options” P86), Plans, which were actionable (“I am also going to look further into that Map of Emotions” P8), and Worries, which were negative future projections (“The upcoming ‘ladder-less pits’ [helplessness without support] is still scary”, P7).
Symbolic references
Participants often mentioned Items such as Art (“It felt good, a bit like drawing/painting/writing before I wasn’t serious about them” P87; “Well, this was kind of like listening to bad jazz” P 88), Beauty (“When I smile, I am beautiful” P71), Death (“I was thinking about the feelings of the funeral processions I have experienced, not necessarily concrete memories of the procession itself but rather of the general atmosphere” P89), Life (“She has stood by my side my whole life and has had me as a ‘gift’, as she puts it” P71), Media (“this reminded me of the movie Ace Ventura 2, where many of the scenes take place in a jungle” P21), Nature (“Reminded me of last year’s community spring yard cleaning at our home when I noticed some colours in nature amidst the gloom” P75). Participants discussed Activity they took such as Believing (“My mind rises to believe and to try” P46), Searching (“The struggle of longing to be seen and searching for oneself” P75), Inability (“I am lacking that power or ability that drives me forward” P43). Context, differently from Items, was based on internal perception rather than tangible outside objects, such as Sensitivity (“I am perhaps a bit sensitive so if I could at first try and practice on my own for a while” P46), Humour (“Powerful drumming causes a powerful feeling, but funnily enough, at the same time a whimsically wistful one!” P98), Bad (value) (“I think I have understood already that there are no ‘wrong’ feelings” P16”). Other Symbolic References codes were Being right, Being wrong, Careful, Chaos, Clarity, Confusion, Creativity, Cynicism, Difference, Difficulty, Distraction, Ease, Effortlessness, Familiarity, Good (value), Humour, Importance, Inspiration, Loss, Playfulness, Pleasant, Powerful, Sensitivity, Desire to be, Desire to do, Memory (function), Mind, Mood, Thoughts, Unwillingness, Willingness.
Music therapists’ reports
All music therapists submitted their reports after the intervention was complete. The music therapists reported that most clients had some challenges when doing the homework task. The most common issues faced were lack of motivation, too much stress, lack of time, technical problems with the music player software, and the severity of depression and anxiety. Music therapists suggested that the homework task could be improved by (a) using a mobile application to increase user friendly access to improvisations, (b) ensuring that homework experiences are being systematically discussed during all music therapy sessions, and (c) decreasing the frequency of meetings, because two sessions and two homework tasks every week was too intensive for some participants. Only one music therapist discussed homework during every session, other music therapists sometimes forgot, and other times chose not to address it due to the client’s emotional state or their own professional preferences. Some music therapists believe that a structured session format is in direct conflict with spontaneous IIMT principles, would increase the sense of external control, and decrease the quality of the client–music therapist relationship.
Discussion
This study investigated how music therapy clients experience listening to their own clinical improvisations at home. First, participants’ experiences of music listening homework will be presented as summarised by five main themes expressed in their diaries: MUSIC, THERAPY, EMOTIONS, EMBODIMENT, and NARRATIVE. Second, the implementation of music listening homework in improvisational music therapy will be discussed from the music therapists’ point of view. After summarising the findings in the context of previous research, the limitations of this study and conclusions regarding music therapy practice will be presented.
In this study, the theme MUSIC comprised four subthemes: Playing, Listening, Music Perception, and Music Parameters. Some participants did not recognise their own music, possibly because of a lack of connection to the music, a lack of significance in the music making process, or an altered state of consciousness when playing (Brabant, Citation2018). Other participants recognised their music, but did not perceive any emotional connection to it, and were distressed by the lack of aesthetic qualities, exemplifying the challenges of meaning-making in music therapy (Keith, Citation2007; Stige, Citation1999). Many participants experienced imagery whilst listening to their improvisations, which is consistent with previous literature (Hargreaves, Citation2012; Taruffi & Küssner, Citation2019). One unanticipated finding was the importance of the physical environment, as many participants found the noisiness and clutter of their home interfering with their listening experience. Overall, the findings showed that participants were deeply connected to their music, whether in negative or positive ways (McFerran, Citation2016), and often talked about it even with limited musicological terminology.
The theme THERAPY comprised three subthemes: Therapeutic Processing, Illness, and Music Therapy Trial. The music therapist was often mentioned as a supportive figure in line with lots of previous work (Rolvsjord, Citation2016; Silverman, Citation2019), but for some, the relationship was perceived as forceful and negative. For some participants the intensive process of going to therapy and doing homework afterwards was overwhelming (“I’m not sure if I can continue this therapy trial if the straining and taxing won’t ease at all” P87). For participants who were not overwhelmed, it still caused a lot of distress, whether by dissociation due to past trauma (Feeny et al., Citation2000) or by enhancing self-criticism (Ehret et al., Citation2015; Watkins & Teasdale, Citation2004). These findings are consistent with depression symptoms according to ICD-10 (World Health Organisation, Citation1993) and were noted in previous literature on unhealthy engagement with music (Saarikallio et al., Citation2015) and potential for harm within music therapy (Murakami, Citation2021). On the other hand, some participants were able to gain a new perspective on their issues, which confirms that insight and increased awareness plays an important role in successful emotional processing (Saarikallio et al., Citation2022).
The theme EMOTIONS comprised three subthemes: Negative Emotions, Positive Emotions, and Other Emotions. Negative emotions were not discussed more or in greater depth, which was surprising as negativity bias is common in depression (Punkanen et al., Citation2011; Sakka & Juslin, Citation2017). It is difficult to explain this result, but it might be caused by internalised negativity with self-critical thoughts (Garrido et al., Citation2017) or experienced psychosomatically via bodily pains (Lipsanen et al., Citation2004), as both types of experiences were discussed frequently in diaries. Emotional reactions were varied and nuanced, often pleasurable and distressing at the same time, and constantly fluctuating, which is in line with the findings of a great deal of previous work on music and emotion (Garrido & Schubert, Citation2013; Juslin & Laukka, Citation2004; Juslin et al., Citation2008).
The theme EMBODIMENT is a body-related theme comprising three subthemes: Body Parts, Sensations, and Actions. Although previous literature often refers to the embodied aspect of music cognition (Leman & Maes, Citation2014; Leman et al., Citation2018) and emotional experiences (Hodges, Citation2016; Schiavio et al., Citation2017), these findings were unexpected in their diversity and granularity. NARRATIVE was a story-telling theme, comprising two subthemes: Chronology and Symbolic References. Interestingly, there were no personally meaningful references to music in participants’ pasts, such as favourite bands, concerts, or memories of emotional experiences with music, which is contrary to previous research on the importance of music in everyday life (DeNora, Citation2004; Garrido & Schubert, Citation2015). This theme was by far the most sizable and heterogenous, highlighting the complexity of the way people perceive the world, act in it, and the stories they tell afterwards.
Regarding the second aim of the study, it seems that music listening homework does have potential as a method in improvisational music therapy for clients who have sufficient time, motivation, and are not overwhelmed by the symptoms of depression and anxiety. When comparing listening homework to listening to clinical improvisations during music therapy sessions, as in the case of AOM, it seems that the music therapist’s presence would safeguard clients from engaging in excessive rumination or avoidance (Garrido & Schubert, Citation2015; Miranda & Claes, Citation2009; Miranda et al., Citation2012). On the other hand, for patients who have sufficient self-regulation strategies and are not in emotional crisis at the time, homework provides a unique opportunity for self-reflection, empowerment, and the ability to practise healthy emotion-regulation strategies in their home environments.
It is important to note that many participants were distressed, and the majority did not comply with the homework task. Some participants had difficulties understanding the aim of therapeutic music making, or lacked sufficient musical skills to express themselves, hence did not find meaning in listening to their clinical improvisations. For this reason, it would be advisable to consider the stage of the music therapy process, and to avoid introducing clinical improvisation listening homework too early. Other participants were overwhelmed by negative emotions and did not have sufficient self-soothing and emotion-regulating abilities to face issues by themselves at home without immediate support from the music therapist. Some participants had issues using computer software to access their clinical improvisations, and although it must remain fairly complicated due to security reasons, clients should be offered technological training and continuous support.
In this study, many participants expressed frustration in their diaries regarding their inability to name their emotions. Previous studies show that depression can impair cognitive and verbal processing, making the language part of the homework task challenging for severely depressed participants (Hammar & Årdal, Citation2009; McDermott & Ebmeier, Citation2009). It is possible that listening to clinical improvisations might have benefited participants of this study more if it was a stand-alone task, and not followed by the diary writing afterwards.
Another issue regarding homework implementation could be linked to the importance of systematically addressing participants’ experiences in following music therapy sessions. For example, the EIMT manual (Aalbers et al., Citation2020) emphasises maintaining an identical intervention structure, where each session begins by discussing previous homework and ends with coming up with new homework. More structure might be beneficial for depressed participants who lack motivation and emotional self-regulation skills. On the other hand, some music therapists in this study indicated that highly structured music therapy would impair their ability to be spontaneous and is not in line with their professional approach.
Limitations
First and foremost, compliance with the homework task was so low that the conclusions of this study should be taken cautiously. It must be also noted that this study was conducted in treatment of depression, and one should be cautious of generalising findings to other clinical populations. Third, potential inconsistencies in music therapists’ approach to the home listening task might have led some participants to benefit from it more if their music therapist spent more time talking about the task during the sessions, but studying such effects was beyond the scope of this study. Fourth, data analysis was performed after music therapy was concluded, so there was no opportunity to validate findings by asking participants whether these themes captured their experiences well. Finally, allocating some experiences to categories was not always clear-cut, for example, the experiences of playing whilst listening to the recordings of improvisations could have been placed either in the playing or listening subcategory, as the categories hold some level of conceptual overlap.
Conclusion
The findings from this study suggest that listening homework can be a useful music therapy method, but it should be used with caution as it seems to act as a magnifying glass, enhancing everything whether it be beneficial or destructive. If music therapy sessions are going well, listening to improvisations at home could be implemented to aid therapeutic processing and used as a resource for grounding, relaxation, and self-exploration. But if the client has difficulties understanding the aim of therapeutic music making, significantly lacks musical skills to express themselves, or is at risk of dissociation, home listening tasks should be utilised on a case-by-case basis. Overall, the homework task of the client listening to their own clinical improvisations needs further research before implementation as part of improvisational music therapy.
Supplemental Material
Download MS Word (30.8 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/08098131.2023.2291434.
Additional information
Funding
Notes on contributors
Nerdinga Snape
Nerdinga Snape is a postdoctoral researcher at the Department of Music, Art, and Culture Studies at the University of Jyväskylä. She is a member of the Ethics Committee of the Lithuanian Music Therapy Association. She teaches and researches a variety of topics in the fields of music therapy and music psychology. She is a member of the Centre of Excellence in Music, Mind, Body, and Brain and the Profiling area of Social Sustainability for Children and Families at the University of Jyväskylä.
Suvi Saarikallio
Suvi Saarikallio is a Professor of Music Education at the University of Jyväskylä, Finland. She conducts research and teaches music psychology, music education, and music therapy. She is the Chairman of the Finnish Society for Music Education (FiSME), Vice-President of the European Society for the Cognitive Sciences of Music (ESCOM), and the European Commissioner for the ISME (International Society for Music Education) Research Commission. She currently acts as a PI for an ERC-funded project MUSICONNECT, a Co-PI for the Centre of Excellence in Music, Mind, Body & Brain, and a Co-PI for the University of Jyväskylä Profiling area for the Social Sustainability for Children and Families.
Esa Ala-Ruona
Esa Ala-Ruona, PhD is an Associate Professor of Music Therapy at the Centre of Excellence in Music, Mind, Body, and Brain, University of Jyväskylä, Finland. He is a music therapist and advanced level psychotherapist working as a researcher, clinical teacher, and supervisor at the University of Jyväskylä Music Therapy Clinic for Research and Training. His research interests are in music therapy assessment and evaluation, and in studying musical interaction, meaning making and clinical processes in multimodal music therapy. He has an extensive experience in clinical music therapy in various fields of health care and rehabilitation. His special expertise lies on creating clinical models, as well as clinical practice of integrative music psychotherapy, and vibroacoustic therapy.
Martin Hartmann
Martin Hartmann is an Assistant Professor of Musicology at the Centre of Excellence in Music, Mind, Body and Brain, University of Jyväskylä Finland. His research interests include music and movement, music perception and cognition, music information retrieval, and music therapy. He maintains the MoCap Toolbox, a set of functions written in MATLAB for the analysis and visualization of motion capture data. He currently serves as Associate Editor of the journal Psychology of Music.
Olivier Brabant
Olivier Brabant is a postdoctoral researcher at the University of Jyväskylä. His research is about enhancing the benefits of music psychotherapy by starting the sessions with a short breathing intervention. Through the achieved relaxation, clients are better able to regulate their emotions, leading to deeper and more productive work during therapy.
Jaakko Erkkilä
Jaakko Erkkilä is professor of music therapy at the Department of Music, Art and Culture Studies, University of Jyväskylä, Finland. He is one of the module leaders at the Finnish Centre of Excellence in Music, Mind, Body, and Brain, responsible for music therapy studies. His research interests include effectiveness of music therapy based on Evidence-Based Practice on mental disorders, treatment model development, and clinical improvisation. He has acted as a PI for two RCTs on improvisational music therapy for depression based on European Union and Academy of Finland funding. Erkkilä is a qualified music therapist and advanced level psychotherapist and the Head of music therapy clinical training at the Eino Roiha foundation, Jyväskylä, Finland.
References
- Aalbers, S., Fusar‐Poli, L., Freeman, R. E., Spreen, M., Ket, J. C. F., Vink, A. C., Maratos, A., Crawford, M., Chen, X. J., & Gold, C. (2017). Music therapy for depression. Cochrane Database of Systematic Reviews, 11(11), Article CD004517. https://doi.org/10.1002/14651858.CD004517.pub3
- Aalbers, S., Spreen, M., Pattiselanno, K., Verboon, P., Vink, A., & van Hooren, S. (2020). Efficacy of emotion-regulating improvisational music therapy to prevent depression in young adult students with depressive symptoms: A multiple-case study design. The Arts in Psychotherapy, 71, 101720. https://doi.org/10.1016/j.aip.2020.101720
- Aalbers, S., Vink, A., de Witte, M., Pattiselanno, K., Spreen, M., & van Hooren, S. (2021). Feasibility of emotion-regulating improvisational music therapy for young adult students with depressive symptoms: A process evaluation. Nordic Journal of Music Therapy, 31(2), 133–152. https://doi.org/10.1080/08098131.2021.1934088
- Aalbers, S., Vink, A., Freeman, R. E., Pattiselanno, K., Spreen, M., & van Hooren, S. (2019). Development of an improvisational music therapy intervention for young adults with depressive symptoms: An intervention mapping study. The Arts in Psychotherapy, 65, 101584. https://doi.org/10.1016/j.aip.2019.101584
- Aigen, K. (2005). Music-centered music therapy. Barcelona Publishers.
- Baldessarini, R. J., Lau, W. K., Sim, J., Sum, M. Y., & Sim, K. (2017). Suicidal risks in reports of long-term controlled trials of antidepressants for major depressive disorder II. The International Journal of Neuropsychopharmacology, 20, 281–284. https://doi.org/10.1093/ijnp/pyw092
- Baltazar, M., & Saarikallio, S. (2016). Toward a better understanding of affect self-regulation through music: A critical integrative literature review. Psychology of Music, 44(6), 1500–1521. https://doi.org/10.1177/0305735616663313
- Bonde, L. O. (2016). The black hole – or is music a black box? Nordic Journal of Music Therapy, 25(1), 9–11. https://doi.org/10.1080/08098131.2015.1111406
- Brabant, O. (2018). Using altered states of consciousness in improvisational music therapy: The potential of resonance frequency breathing [ Doctoral dissertation, University of Jyväskylä]. University of Jyväskylä.
- Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise & Health, 11(4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
- Braun, V., & Clarke, V. (2021). One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qualitative Research in Psychology, 18(3), 328–352. https://doi.org/10.1080/14780887.2020.1769238
- Bruscia, K. E. (1998). The dynamics of music psychotherapy. Barcelona Publishers.
- Bruscia, K. E. (2014). Defining music therapy (3rd ed.). Barcelona Publishers.
- Chin, T. C., & Rickard, N. S. (2014). Emotion regulation strategy mediates both positive and negative relationship between music uses and well-being. Psychology of Music, 42(5), 692–713. https://doi.org/10.1177/0305735613489916
- Davis, W. B., Gfeller, K. E., & Thaut, M. H. (2008). An introduction to music therapy: Theory and practice (3rd ed.). American Music Therapy Association.
- De Maat, S., Dekker, J., Schoevers, R., & De Jonghe, F. (2006). Relative efficacy of psychotherapy and pharmacotherapy in the treatment of depression: A meta-analysis. Psychotherapy Research, 16(5), 566–578. https://doi.org/10.1080/10503300600756402
- DeNora, T. (2004). Music in everyday life. Cambridge University Press.
- Ehret, A. M., Joormann, J., & Berking, M. (2015). Examining risk and resilience factors for depression: The role of self-criticism and self-compassion. Cognition and Emotion, 29(8), 1496–1504. https://doi.org/10.1080/02699931.2014.992394
- Erkkilä, J. (2004). From signs to symbols, from symbols to words—about the relationship between music and language. Voices: A World Forum for Music Therapy, 4(2). https://doi.org/10.15845/voices.v4i2.176
- Erkkilä, J., Ala-Ruona, E., Punkanen, M., & Fachner, J. (2012). Creativity in improvisational, psychodynamic music therapy. In D. Hargreaves, D. Miell, & R. MacDonald (Eds.), Musical imaginations (pp. 414–26). Oxford University Press.
- Erkkilä, J., Brabant, O., Hartmann, M., Mavrolampados, A., Ala-Ruona, E., Snape, N., Saarikallio, S., & Gold, C. (2021). Music therapy for depression enhanced with listening homework and slow paced breathing: A randomised controlled trial. Frontiers in Psychology, 12, Article 613821. https://doi.org/10.3389/fpsyg.2021.613821
- Erkkilä, J., Brabant, O., Saarikallio, S., Ala-Ruona, E., Hartmann, M., Letule, N., Geretsegger, M., & Gold, C. (2019). Enhancing the efficacy of integrative improvisational music therapy in the treatment of depression: Study protocol for a randomised controlled trial. Trials, 20(1), Article 244. https://doi.org/10.1186/s13063-019-3323-6
- Eschen, J. T. (2002). Analytic music therapy – Introduction. In J. T. Eschen (Ed.), Analytical music therapy (pp. 17–33). Jessica Kingsley Publishers.
- Feeny, N. C., Zoellner, L. A., Fitzgibbons, L. A., & Foa, E. B. (2000). Exploring the roles of emotional numbing, depression, and dissociation in PTSD. Journal of Traumatic Stress, 13(3), 489–498. https://doi.org/10.1023/A:1007789409330
- Garrido, S., Eerola, T., & McFerran, K. (2017). Group rumination: Social interactions around music in people with depression. Frontiers in Psychology, 8(490). https://doi.org/10.3389/fpsyg.2017.00490
- Garrido, S., & Schubert, E. (2013). Adaptive and maladaptive attraction to negative emotion in music. Musicae Scientiae, 17(2), 145–164. https://doi.org/10.1177/1029864913478305
- Garrido, S., & Schubert, E. (2015). Music and people with tendencies to depression. Music Perception, 32(4), 313–321. https://doi.org/10.1525/mp.2015.32.4.313
- Groarke, J. M., & Hogan, M. J. (2018). Development and psychometric evaluation of the adaptive functions of music listening scale. Frontiers in Psychology, 9, 516. https://doi.org/10.3389/fpsyg.2018.00516
- Grocke, D., & Moe, T. (2015). Guided imagery and music (GIM) and music imagery methods for individual and group therapy. Jessica Kingsley Publishers.
- Hammar, Å., & Årdal, G. (2009). Cognitive functioning in major depression-a summary. Frontiers in Human Neuroscience, 3, 728. https://doi.org/10.3389/neuro.09.026.2009
- Hammer, S. E. (1996). The effects of guided imagery through music on state and trait anxiety. Journal of Music Therapy, 33(1), 47–70. https://doi.org/10.1093/jmt/33.1.47
- Hargreaves, D. J. (2012). Musical imagination: Perception and production, beauty and creativity. Psychology of Music, 40(5), 539–557. https://doi.org/10.1177/0305735612444893
- Hengartner, M. P., Angst, J., & Rossler, W. (2018). Antidepressant use prospectively relates to a poorer long-term outcome of depression: Results from a prospective community cohort study over 30 years. Psychotherapy and Psychosomatics, 87(3), 181–183. https://doi.org/10.1159/000488802
- Hodges, D. (2016). Bodily responses to music. In S. Hallam, I. Cross, & M. Thaut (Eds.), The Oxford handbook of music psychology (2nd ed., pp. 183–196). Oxford University Press.
- Jacobsen, S. L., Pedersen, I. N., & Bonde, L. O. (2019). A comprehensive guide to music therapy: Theory, clinical practice, research, and training (2nd ed.). Jessica Kingsley Publishers.
- Juslin, P. N., & Laukka, P. (2004). Expression, perception, and induction of musical emotions: A review and a questionnaire study of everyday listening. Journal of New Music Research, 33(3), 217–238. https://doi.org/10.1080/0929821042000317813
- Juslin, P. N., Liljestrom, S., Västfjäll, D., Barradas, G., & Silva, A. (2008). An experience sampling study of emotional reactions to music: Listener, music, and situation. Emotion, 8(5), 668–683. https://doi.org/10.1037/a0013505
- Kamenov, K., Twomey, C., Cabello, M., Prina, A., & Ayuso-Mateos, J. (2017). The efficacy of psychotherapy, pharmacotherapy and their combination on functioning and quality of life in depression: A meta-analysis. Psychological Medicine, 47(3), 414–425. https://doi.org/10.1017/S0033291716002774
- Kazantzis, N., Deane, F. P., & Ronan, K. R. (2000). Homework assignments in cognitive and behavioral therapy: A meta-analysis. Clinical Psychology Science & Practice, 7(2), 189. https://doi.org/10.1093/clipsy.7.2.189
- Kazantzis, N., Whittington, C., & Dattilio, F. (2010). Meta-analysis of homework effects in cognitive and behavioral therapy: A replication and extension. Clinical Psychology Science & Practice, 17(2), 144. https://doi.org/10.1111/j.1468-2850.2010.01204.x
- Keith, D. R. (2007). Understanding Music Improvisations: A Comparison of Methods of Meaning-Making [ Unpublished doctoral dissertation]. Temple University.
- Leman, M., & Maes, P. J. (2014). Music perception and embodied music cognition. In L. Shapiro (Ed.), The Routledge handbook of embodied cognition (pp. 81–89). Routledge/Taylor & Francis Group.
- Leman, M., Maes, P. J., Nijs, L., & Van Dyck, E. (2018). What is embodied music cognition? In R. Bader (Ed.), Springer handbook of systematic musicology (pp. 747–760). Springer Handbooks.
- Lipsanen, T., Saarijärvi, S., & Lauerma, H. (2004). Exploring the relations between depression, somatization, dissociation and alexithymia – overlapping or independent constructs? Psychopathology, 37(4), 200–206. https://doi.org/10.1159/000080132
- Maratos, A., Crawford, M., & Procter, S. (2018). Music therapy for depression: It seems to work, but how? British Journal of Psychiatry, 199(2), 92–93. https://doi.org/10.1192/bjp.bp.110.087494
- Maratos, A., Gold, C., Wang, X., & Crawford, M. (2008). Music therapy for depression. Cochrane Database of Systematic Reviews, 1. https://doi.org/10.1002/14651858.CD004517.pub2
- Mausbach, B. T., Moore, R., Roesch, S., Cardenas, V., & Patterson, T. L. (2010). The relationship between homework compliance and therapy outcomes: An updated meta-analysis. Cognitive Therapy and Research, 34(5), 429–438. https://doi.org/10.1007/s10608-010-9297-z
- McDermott, L. M., & Ebmeier, K. P. (2009). A meta-analysis of depression severity and cognitive function. Journal of Affective Disorders, 119(1–3), 1–8. https://doi.org/10.1016/j.jad.2009.04.022
- McFerran, K. S. (2016). Contextualising the relationship between music, emotions and the well-being of young people: A critical interpretive synthesis. Musicae Scientiae, 20(1), 103–121. https://doi.org/10.1177/1029864915626968
- McKinney, C. H., Antoni, M. H., Kumar, M., Tims, F. C., & McCabe, P. M. (1997). Effects of guided imagery and music (GIM) therapy on mood and cortisol in healthy adults. Health Psychology, 16(4), 390. https://doi.org/10.1037/0278-6133.16.4.390
- McKinney, C. H., & Honig, T. J. (2017). Health outcomes of a series of Bonny method of guided imagery and music sessions: A systematic review. Journal of Music Therapy, 54(1), 1–34. https://doi.org/10.1093/jmt/thw016
- Miranda, D., & Claes, M. (2009). Music listening, coping, peer affiliation and depression in adolescence. Psychology of Music, 37(2), 215–233. https://doi.org/10.1177/0305735608097245
- Miranda, D., Gaudreau, P., Debrosse, R., Morizot, J., & Kirmayer, L. J. (2012). Music listening and mental health: Variations on internalizing psychopathology. In R. A. R. MacDonald, G. Kreutz, & L. Mitchell (Eds.), Music, health, and wellbeing (pp. 513–529). Oxford University Press.
- Muller, B. (2012). Variations in guided imagery and music: Taking a closer look. Barcelona Publishers.
- Murakami, B. (2021). The music therapy and harm model (MTHM): Conceptualizing harm within music therapy practice. ECOS - Revista Científica de Musicoterapia y Disciplinas Afines, 6(1), 003. https://doi.org/10.24215/27186199e003
- National Institute of Mental Health. (2022). Depression. https://www.nimh.nih.gov/health/topics/depression/index.shtml#part_145396
- Newell, E. E., McCoy, S. K., Newman, M. L., Wellman, J. D., & Gardner, S. K. (2018). You sound so down: Capturing depressed affect through depressed language. Journal of Language and Social Psychology, 37(4), 451–474. https://doi.org/10.1177/0261927X17731123
- Norcross, J. C., & Goldfried, M. R. (2005). Handbook of psychotherapy integration (2nd ed.). Oxford University Press.
- Nord, C., Barrett, L., Lindquist, K., Ma, Y., Marwood, L., Satpute, A., & Dalgleish, T. (2021). Neural effects of antidepressant medication and psychological treatments: A quantitative synthesis across three meta-analyses. British Journal of Psychiatry, 219(4), 546–550. https://doi.org/10.1192/bjp.2021.16
- Punkanen, M., Eerola, T., & Erkkilä, J. (2011). Biased emotional preferences in depression: Decreased linking of angry and energetic music by depressed patients. Music and Medicine, 3(2), 114–120. https://doi.org/10.1177/1943862110395597
- Rolvsjord, R. (2016). Five episodes of clients’ contributions to the therapeutic relationship: A qualitative study in adult mental health care. Nordic Journal of Music Therapy, 25(2), 159–184. https://doi.org/10.1080/08098131.2015.1010562
- Saarikallio, S., Gold, C., & McFerran, K. (2015). Development and validation of the healthy-unhealthy music scale. Child and Adolescent Mental Health, 20(4), 210–217. https://doi.org/10.1111/camh.12109
- Saarikallio, S., Toiviainen, P., Brabant, O., Snape, N., & Erkkilä, J. (2022). Music therapeutic emotional processing (MEP): Expression, awareness, and pain predict therapeutic outcome. Psychology of Music, 51(1), 140–158. https://doi.org/10.1177/03057356221087445
- Sakka, L. S., & Juslin, P. N. (2017). Emotional reactions to music in depressed individuals. Psychology of Music, 46(6), 862–880. https://doi.org/10.1177/0305735617730425
- Scheiby, B. (2010). Analytical music therapy and integrative medicine: The impact of medical trauma on the psyche. In K. Stewart (Ed.), Music therapy and trauma: Bridging theory and clinical practice (pp. 74–87). Satchnote Press.
- Schiavio, A., van der Schyff, D., Cespedes-Guevara, J., & Reybrouck, M. (2017). Enacting musical emotions. Sense-making, dynamic systems, and the embodied mind. Phenomenology and the Cognitive Sciences, 16(5), 785–809. https://doi.org/10.1007/s11097-016-9477-8
- Silverman, M. J. (2019). Music therapy and therapeutic alliance in adult mental health: A qualitative investigation. Journal of Music Therapy, 56(1), 90–116. https://doi.org/10.1093/jmt/thy019
- Stige, B. (1999). The meaning of music—From the client’s perspective. In T. Wigram & J. D. Backer (Eds.), Clinical applications of music therapy in psychiatry (pp. 61–83). Jessica Kingsley Publishers.
- Taruffi, L., & Küssner, M. B. (2019). A review of music-evoked visual mental imagery: Conceptual issues, relation to emotion, and functional outcome. Psychomusicology: Music, mind, and brain, 29(2–3), 62–74. https://doi.org/10.1037/pmu0000226
- Thase, M. E., & Callan, J. A. (2006). The role of homework in cognitive behavior therapy of depression. Journal of Psychotherapy Integration, 16(2), 162. https://doi.org/10.1037/1053-0479.16.2.162
- Van den Tol, A. J., & Edwards, J. (2015). Listening to sad music in adverse situations: How music selection strategies relate to self-regulatory goals, listening effects, and mood enhancement. Psychology of Music, 43(4), 473–494. https://doi.org/10.1177/0305735613517410
- Watkins, E., & Teasdale, J. D. (2004). Adaptive and maladaptive self-focus in depression. Journal of Affective Disorders, 82(1), 1–8. https://doi.org/10.1016/j.jad.2003.10.006
- World Health Organization. (1993). The ICD-10 classification of mental and behavioural disorders. World Health Organization.
- World Health Organization. (2021). Depression. https://www.who.int/news-room/fact-sheets/detail/depression
- Zhang, M., Ding, Y., Zhang, J., Jiang, X., Xu, N., Zhang, L., & Yu, W. (2022). Effect of group impromptu music therapy on emotional regulation and depressive symptoms of college students: A randomized controlled study. Frontiers in Psychology, 13, 851526. https://doi.org/10.3389/fpsyg.2022.851526