
ABSTRACT
Introduction
Anxiety is a commonly diagnosed mental health disorder, but it remains underrepresented in music therapy research. Music listening (ML) seems to be an effective tool for anxiety self-management, but there is evidence that high anxiety level may complicate the self-regulation process. The links between ML in music therapy and everyday life have received little attention. The aim was to study what roles ML can have throughout a music therapy process for anxiety treatment, according to music therapists.
Method
The data were collected by interviewing eight music therapists with experience of patients with anxiety disorders. The data were analyzed with the six-step approach to thematic analysis. The results were grouped into three categories: information carrier, musical identity development, and self-care tools.
Results
ML appears to have three roles in music therapy for the treatment of anxiety: ML is a familiar part of the patient’s everyday life and provides valuable information about the patient’s inner world and their current state to the therapist; in therapy, ML represents safety, promotes conversation, and works as a bridge towards more active methods; and as a result of the therapeutic process, ML returns to patients’ everyday lives as a developed tool for self-regulation.
Discussion
ML seems to function as a low-threshold activity, through which patients with anxiety disorders can share and reflect their mental state. With the assistance of a music therapist, they can learn to use music more beneficially in their anxiety self-management and develop a healthier musical identity that can foster their emotional health.
Introduction
Anxiety is the most diagnosed and rapidly increasing mental health disorder in the European Union (OECD & European Union, Citation2022), however, in music therapy research, it has received little attention as its own entity, as it is often studied in relation with other disorders such as depression (Aalbers et al., Citation2017; Erkkilä et al., Citation2011). The effects of music listening (ML) on wellbeing have been extensively studied, for example, in terms of emotion regulation (Carlson et al., Citation2015; Saarikallio, Citation2008, Citation2012). Emotion regulation with music is not always successful among people with mental health disorders, but there is evidence that with the guidance of a music therapist, ML can become a method of self-care and a resource of health for patients (Vaillancourt et al., Citation2022). As an affordable, easily transferable method of music therapy (Harney et al., Citation2022), ML could help alleviate anxiety in various therapy settings, as well as in people’s everyday lives.
Definition of anxiety
Arroll and Kendrick (Citation2018, p. 125) define anxiety as “a universal adaptive response to a threat”. Anxiety can also be described as a stress reaction (Ressler et al., Citation2015), and can evoke fight–flight responses (Buckley & Punkanen, Citation2020; Craske et al., Citation2011). However, anxiety exists more as a longer-term mood than, for example, acute fear. According to Barlow (Citation2004), anxiety and fear are separated as follows: Anxiety is a future-oriented mood, in which a person expects negative things to happen, and fear is an alarm reaction to immediate danger. Although experiencing anxiety is a normal and healthy part of everyday life, excessive or unwarranted anxiety can play a part in serious illness.
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) recognizes 11 different types of anxiety disorders, which can involve symptoms such as fear, panic, hypertension, apprehension, chronic pain, agoraphobia, compulsive rituals, excessive worry, agitation, difficulty concentrating and sleep disturbances. Many of these symptoms can also appear in depression or stress disorders (Cummings et al., Citation2014). The most common anxiety disorders are generalized anxiety disorder (GAD), panic disorder and phobias (Hardy & Gray, Citation2011). In addition, anxiety is often related to obsessive-compulsive disorder (OCD), post-traumatic stress disorder (PTSD), depression, substance abuse, long-term illnesses, trauma, and social anxiety disorder (SAD) (Arroll & Kendrick, Citation2018; Hardy & Gray, Citation2011). Anxiety may sometimes be undiagnosed due to comorbidity, or because the focus is mainly on the patient’s somatic symptoms, such as pain or insomnia (Bandelow et al., Citation2015).
Music therapy for anxiety treatment
Music psychotherapy is a common treatment for mental health disorders. Music, with its capacity to evoke deep emotions and work as a non-verbal medium, offers a unique tool for reflecting and expressing emotional content in therapy (Erkkilä et al., Citation2011). Music therapy methods can be categorized into two groups: active methods, in which the patient is playing an instrument, singing, or engaging bodily with the producing of music; and receptive methods, in which the patient does not produce the music, but is an active recipient of the musical information (Maratos et al., Citation2008).
A clinical pilot study by Gutiérrez and Camarena (Citation2015) found that music therapy combined with pharmacological treatment seems to reduce anxiety levels for patients with generalized anxiety disorder. Their pilot intervention study used both active and receptive methods of music therapy and they found the receptive methods to be important, especially in encouraging the expression of memories and emotions. The possibilities of ML in music therapy should not be underestimated; while being a seemingly simple method, ML can provide highly meaningful individual experiences and help in building the connection between the patient and therapist (McCaffrey, Citation2016). The goals of ML can be, for example, to evoke physiological or affective responses, stimulate or relax the patient, evoke imagery, or stimulate discussion (Aigen, Citation2014; Grocke, Citation2016).
Music for self-regulation
Self-regulation can be defined as the ability to change one’s own physical, mental, or emotional state by adapting to the environment and its demands or challenges (Oettingen & Gollwitzer, Citation2015). Since anxiety is an emotional state that can be accompanied by strong bodily sensations, such as a feeling of tension, a fast heart rate or high blood pressure, relieving anxiety is not only about mental regulation skills, but also about regulating the body (Amstadter, Citation2008).
Music can have a beneficial effect on stress-related physiological, cognitive, and emotional processes (Thoma et al., Citation2013). Emotion regulation is an often-mentioned underlying reason for ML (Saarikallio, Citation2011). The goals of everyday ML are most often related to relaxation, cheering up and strengthening the listener’s perceived emotion (Peltola et al., Citation2022, p. 387).
A lot of research has been done in relation to ML behaviors in adolescents and adults. Although the goals in ML are generally related to healthy self-regulation, research into ML behaviors in adolescents and adults has shown that not all listeners use music in a way that improves their wellbeing (Garrido et al., Citation2022; Groarke et al., Citation2020). Stewart et al. (Citation2019) discovered that young people with depression use music a lot in their everyday lives, but they are often not aware of how their music choices affect their wellbeing. In a recent experience sampling study, music listeners in an anxious state reached their self-regulation goals less successfully compared to all other negative states (Randall et al., Citation2023). This result indicates that the specific factors related to ML and anxiety require further investigation.
ML in anxiety management has been studied previously from the everyday life perspective (Carlson et al., Citation2015; Saarikallio, Citation2011), and clinically for example related to state anxiety before medical procedures (Thoma et al., Citation2015; Mackintosh et al., Citation2018; Vachiramon et al., Citation2013). A meta-analysis of controlled studies by Harney et al. (Citation2022) concludes that although ML was found to be effective for reducing anxiety in a variety of groups, more research on clinical groups with diagnosed mental health problems is required. Successful emotion regulation with music requires a person to know how to use music beneficially for them. A person’s own relationship with music, and beneficial music use can sometimes be examined in the music therapy process.
Anxiety is a complicated state that has not been addressed very centrally in music therapy literature as its own entity. Anxiety seems to be a challenging state also in terms of self-regulation and a high level of anxiety may lead to unsuccessful emotion regulation or maladaptive musical behavior. ML is a commonly used method in music therapy for mental health care, but its role in anxiety treatment has not been defined. More research is needed to define how ML is used in music therapy specifically for anxiety treatment, and what are the possible links of ML in therapy and ML in everyday life.
Study aims
This qualitative, phenomenological study examines the role of ML in different stages of the music therapy process when treating young adults and adults (aged 18–65 years) with anxiety. The phenomenon is explored from the perspective of music therapists.
The research question is: What is the role of music listening in music therapy from the perspectives of music therapists for treating people with anxiety disorders?
Method
Design
This interview study with eight music therapists was conducted with a phenomenological design to reach the in-depth details of their experiences, perceptions, and expertise on the subject (Wilson, Citation2015). Music therapists use various techniques, and their expertise can be built on very different educational backgrounds (Ahonen-Eerikäinen, Citation1999). The phenomenological approach in this study allowed the exploration of different views and lived experiences on the topic (McFerran & Grocke, Citation2007). The theoretical framework of this study leant towards music psychotherapy, which is a common music therapy approach to treat people with mood disorders. Music psychotherapy emphasizes the meaning of the relationship between therapist and patient, and approaches treatment in a holistic way (Zarate, Citation2022). The researchers’ position in the interviews was to be objective outsiders, and not bring out any own experiences or views on the topic.
Participants
Participant recruitment started with searching for music therapists from the web pages of local and national organizations. Therapists were contacted via email if their profile stated that their work related to adults and mental health. Participant selection was done with a purposive sampling method. Purposive sampling is a non-probabilistic selection method where researchers can choose participants who meet specific criteria or possess characteristics that are of particular interest to the study (Guest et al., Citation2013). This approach was chosen for its suitability to find participants who had the required expertise for this study. Participants were included if they had work experience of treating over 18-year-old patients with an anxiety disorder.
Data collection
The interview method in this study was a semi-structured interview, where the interview can be based on defined themes and questions, maintaining a clear structure while leaving room for further developments and free discussion (Hirsjärvi & Hurme, Citation2008; von Soest, Citation2022). The interview procedure contained: a greeting and introduction informing the participant about the study; filling out the form for their consent for participation and recording (by paper or online); and the actual interview part. The interview themes and questions were decided before the interview, but questions were formulated to stimulate discussion, allowing the participant to bring their own perspectives. All participants were asked the same questions about their education, work experience, and their views about the role of music listening in music therapy, as well as their habits of using music with their patients and their observations about anxious peoples’ music engagement (see Appendix), but depending on the flow of the conversation, the order of the questions could vary slightly. Each participant was interviewed once. Interviews lasted about 30 minutes each.
To ensure epistemic access to the researched subject, the researcher conducting the interviews had completed groundwork to build their awareness of the field, for example, the terminology of the field when discussing with an expert (Hyvärinen et al., Citation2017). At the beginning of the interview, the participants were encouraged to use the terminology of the music therapy field, as the interviewer had experience and background education from said field. The interviews were held either online or in person, in Finnish, as all the participants and the interviewer were native Finnish speakers. All participants provided information regarding their age, educational background, work experience, and estimated number of patients with anxiety symptoms seen during their careers.
Ethical considerations
This study was performed in accordance with guidelines and regulations of the Finnish National Board on Research Integrity TENK (Citation2019). The study did not contain interventions that affect participants’ physical integrity, expose them to exceptionally strong stimuli, increase their risk of mental harm or pose a threat to their safety, nor were the participants under the age of 15 or contributing to the research without their own consent. Therefore, according to these guidelines and regulations, ethical approval was not required for this research.
Participants were informed about the procedures before the interview and provided their written informed consent to participate and agreed to the recording of the interview. The audio data were accessible only to the researcher, and the audio files were stored in a password-protected, locked location. Data were transcribed and anonymized, and all audio data files were destroyed no later than 12 months after the interviews. The research was conducted in an ethical and responsible manner.
Analysis
Data were first roughly transcribed with a focus on accuracy of content over linguistic details, a method which is well-suited for thematic analysis (Halcomb & Davidson, Citation2006). The data were analyzed using Braun and Clarke’s (Citation2012) six step approach to thematic analysis, which included familiarization, generating initial codes, searching for themes, reviewing themes, defining, and naming themes and writing the report. ATLAS.ti mac (Version 22.0.6.0) was used as a tool for coding, thematizing, analyzing and visualizing the data, as well as taking notes and keeping a research diary. The notes and diary were used for keeping track of the subjective reflection and the research group discussions throughout the process ensure the reflexivity of the study. Bracketing was used in each state to increase the integrity and validity of the study.
The audio data were transcribed within a week of the interviews. A compression process was made on the original transcriptions, in which some meaningless parts were removed, such as repeated words and the researcher’s affirmative answers. Familiarization with the data included reading through the documents and taking notes on potentially interesting or frequently occurring issues. Initial codes were generated while reading through the documents in the ATLAS.ti software. During the reading, the codes increased and became more detailed. The coding of the documents was examined through several rounds of reading, so that the level of the codes in the documents matched each other.
Themes were searched by categorizing the clearly matching codes to groups with ATLAS.ti. Codes that were left without a group were explored further. If the content was found upon further consideration to fit with any of the existing groups, the name of the code was modified to reflect its relationship more accurately to the theme, and the code was added to the group. If they did not match with any existing themes, the code was examined through its frequency to assess the importance of the code overall: If it appeared very infrequently, it was discarded from the preliminary results. The themes were identified based on their relevance and frequency of appearance. Codes and themes were discussed among all authors, and the themes were reviewed, defined, and named to create the initial structure of the results.
The analysis was made by first mirroring the main themes to the theoretical framework and research questions. Each theme’s codes were reviewed side by side to find the relevant content. If the codes contained information related to other topics, the relevant information was added to notes for later review. The analysis was then taken to the level of quotations, correspondences and relations between quotations were sought, and new categories were found within the themes, whereby cohesion gradually emerged between the individual quotations.
Results were compiled by constructing a text from the rearranged data, corresponding to the research questions. The authors of this paper include both Finnish and English native speakers, all of whom understand and speak both languages on a high level. The translation process of the quotations from Finnish to English was handled by the authors.
Results
Eight music therapists participated in this study. The participants’ ages varied between 32 and 63 years. In addition to their music therapist education, each had a different background education and different work experience. On average, the participants had completed three different degrees, the most common being a master’s degree in education or arts, as well as degrees in other fields of therapy, such as occupational therapy and psychotherapy. The participants’ work experience as a music therapist ranged from 2.5 to 26 years, so the interviews captured information from music therapists who were at different career phases and had been trained at different times. On average, the participants had about 13 years of work experience in music therapy. All participants used a variety of methods in their music therapy practice, with a focus on a patient-led approach. The diversity of patient target groups varied between the participants. Each participant had experience with several anxious patients, often up to dozens of different cases. Some of the participants had worked very extensively in their careers with different target groups and age groups, while others’ work was more focused on a specific clinical group. However, every participant had work experience related to mental health and anxiety with young adults and adults. Thus, the focus of the research is on the experiences related to treating anxiety in the lives of young adults and adults in both private practice and institutional care.
As background information, the participants described how anxiety usually appears in music therapy. These general-level findings about the appearance of anxiety are presented to build an overview of the phenomenon before presenting the main themes. Anxiety was described to appear as challenges in (a) regulation of body and alertness, (b) regulation of emotions and (c) social situations. The bodily reactions were even considered to be the primary visible sign of anxiety. Descriptions of embodied anxiety included physical restlessness, tension, shallow breathing and over- or under-stimulation of the body. These symptoms could be seen during the relaxation and ML exercises, which were common approaches in the early stages of the therapy. In terms of emotion, anxiety became visible as irritation, superficiality, lack of facial expression and challenges in emotion regulation. Somatic symptoms extended to communication and social situations and caused fears, difficulty in speaking and expressing feelings and lack of trust for other people. At times, anxiety could distort self-expression, and lead to unusually quiet or loud musical or verbal expression. Avoidance of social situations was particularly challenging if it affected attending school, work, or therapy. The anxiety-related social and emotional challenges were one of the reasons that therapy with anxious patients was said to progress very slowly and through especially low threshold music exercises.
Overall, anxiety was seen to be very common among different patients. One participant said that: “I don’t even really have a client that wouldn’t have some kind of anxiety” [P1]. Anxiety was considered a very holistic problem, and one participant described it to appear in many ways: “Every patient’s anxiety is a little different; the patients are different, their experiences are different, and their personality, habits and ways to express it can be so diverse” [P5]. These descriptions created the general outline for understanding how anxiety appears in music therapy, which worked as a foundation for defining the role of ML in anxiety treatment.
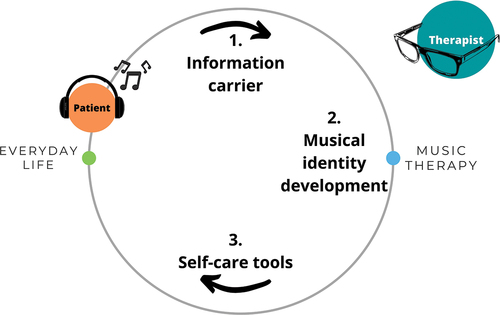
presents the findings of this study. Among the results, three main themes for the role of ML in anxiety treatment were identified: (1) Information carrier, (2) Musical identity development and (3) Self-care tools. The first theme describes how ML works as an information carrier between the patient’s everyday life and therapy, the second theme highlights the development and changes in patients’ ML during the therapeutic process, and the third theme presents how with the help of a therapist ML can become a tool to use for self-care at home. The circular movement represents the ongoing nature of the development of the patient’s ML and demonstrates how ML works continuously as a link between the patient’s life and therapy.
Figure 1. The role of ML in music therapy for anxiety treatment
Information carrier
One role of ML in anxiety treatment was for it to work as an information carrier between the patient’s everyday life and therapy. Shared ML in therapy was described to offer the first view of the patient’s inner world. That view could help to build the relationship between the patient and therapist, as well as to understand the relationship between the patient and music. This theme was divided into two sub-themes: (a) Patient’s ML in therapy, and (b) Patient’s relationship to music.
Patient’s ML in therapy
ML was generally considered as an approachable method that enables patients’ self-expression and non-verbal reflection. Listening to music was often among the first exercises used in therapy, and through the patients’ choices of music and the conversation of it, the therapists got to know the patients and their inner worlds a little better. One participant described that:“Music fills that silence; even if the patient can’t speak yet, an audible part of their inner world is among us, and at some point, the words will appear, when they feel they have built enough trust” [P1].
Differences were found between participants in the amount of using ML in therapy and in their views on whether the music in different situations should be chosen by the therapist or the patient. Two of the participants [P7, P8] emphasized a very patient-oriented approach, where music was only used based on the patient’s wishes, and for all the exercises an effort was made to find music from the patient’s own selection. For example, those who used vibroacoustic chairs or mattresses usually combined ML with the vibroacoustic treatment, which could be calming music chosen by the therapist, soothing soundscapes such as whale sounds, or the client’s own favorite music. The role of ML in building the calming atmosphere was described as follows: “I would not make the first move [in choosing the music], … it is important that the music represents partly that safety, and it is crucial to observe the patient, so that they don’t become even more anxious” [P8].
Breathing and relaxation exercises were commonly used, because they were soothing, relaxing, and helped the patient focus on the present moment. In addition to self-selected music, for example, an audio tape developed for Resonance Frequency Breathing, RBF (Brabant & Erkkilä, Citation2018) or GIM playlists (see e.g. Grocke et al., Citation2015) were used to support breathing and relaxation exercises. In addition to these common ML techniques, in the very early stages of therapy ML was used, for example, as background music as it was described as “providing space for the safe silence” [P2]. One participant reported that they always use soothing background music in therapy, because it makes the patients feel more at ease: “One client said that when they entered the room, they felt that the presence of the music in itself was somehow relieving and calming” [P1].
Patient’s relationship to music
Patients who came to music therapy were initially thought to be interested in music in some way, and some actively used different music lists in their everyday lives. The most common active means of self-regulation with ML were related to escape from fearful situations and to calm down before going to sleep. Descriptions of adaptive music use in everyday life were mainly related to patients with milder symptoms, and patients using music to support a specific activity, for example, one participant mentioned athletes: “Many people already know how to use music a little unconsciously, for example athletes constantly regulate their state of alertness, but they still need support in becoming more aware of that tool” [P6].
For highly anxious patients, the observations were related to introversion, listening to material that cannot be revealed to anyone, and blocking the surrounding world with ML. Two participants [P6, P8] stated that for some of their patients, wearing headphones as an escape from reality had become constant and obsessive. Even though the participants did not report that people with anxiety would have any specific taste of music, metal, black metal, heavy, progressive rock, aggressive themes, and lyrics containing violence in music came up repeatedly. The patients’ use of heavily aggressive music was reported to occur mostly at the beginning of the therapy and was sometimes connected to patients with acute anxiety and mental health issues: “There is that risk, with those who have severe symptoms and are feeling distressed, that the use of very negative music, it becomes uncontrollable. … It would be very important for the patients to notice when they may need somebody, for example the music therapist, to share that experience with” [P6].
The participants commented widely on how different elements of music resonate with their patients. These observations were important for the therapy process, as they explained the patients’ relationship with music, which might guide the methods and music used later in therapy. Of musical traits, melody was seen to be particularly related to emotions and memories. Melody was considered to affect the patient on a very personal level and to be the musical trait that also evokes the most unexpected emotions: “Their favorite music and the melodies can bring out memories from the whole lifespan, those can be very meaningful” [P4]. Harmony, on the other hand, was mentioned to be effective most through embodied reactions, evoking affect on a more unconscious level or in an inconspicuous way. One participant described that their patient was surprised at how the harmony affected them: “Oh, I have this kind of a feeling now?” [P8].
The importance of rhythm in music therapy was mentioned in connection with breathing exercises, movement exercises, and relaxation. An even rhythm was suitable for movement and breathing. For relaxation purposes, the participants preferred to use calm music both in terms of tempo and rhythmic elements. One participant also stated that they use similar music for both relaxation and movement exercises: “An even rhythm that supports the relaxation and calming effect, and there’s not too much happening there. … I also use it for supporting movement, calm even rhythm is preferrable.” [P2].
Melody and harmony were seen as more personal elements of music than rhythm and tempo. Music with lyrics was described to be more individual and personal than instrumental music and one reported that instrumental or classical music would be easier to recommend for a new patient: “Something without lyrics, classical, I could try to use with them if I don’t know them well yet” [P2]. Lyrics were repeatedly found to play an important role in the patients’ music choices and help them to find words for difficult feelings. Lyrics also helped the patient to identify with the singer or author of the song, and to feel that they are not alone, for example, one participant described that: “It makes it easier when they find someone inside that music who has thought the same way, and they find an attachment to that other person behind the lyrics” [P1]. This feeling of belonging was associated with the comfort the patients said they had received from the music.
Musical identity development
The second important role of ML in music therapy for anxiety treatment was for it to be developed further with the help of the therapist. A common view was that the patients already have the tools, but in therapy, they learn how to use them more. Although people often use music in their everyday lives, in therapy those skills are improved and activated, so that the use of music for changing moods, regulating emotions and alertness, or directing thoughts elsewhere becomes more conscious. This theme was divided into two sub-themes: (a) Music reflects the mental change, and (b) ML works as a bridge towards more active agency.
Music reflects the mental change
Sudden changes in the patients’ taste of music and the appearance of new genres in their listening were seen partly as a development of the patients’ musical identity. In addition, the changes in musical taste were thought to be connected to therapeutic growth and were seen to reflect the patient’s development and recovery during the therapy process. One participant saw the change in the lyrics: “The symbolic meaning in the texts, it brings a message to the therapy of how they are feeling” [P8]. Two participants [P5, P6] thought of ML to bring something to the therapist’s attention, and each one of them emphasized how meaningful ML was for the patients in finding words for their emotions, which can reflect their development of emotional skills. Along with the emergence of liking for new genres and changes in musical taste in the patient, the participants were more prone to suggesting new and different music in the mid-process, after building a strong relationship and gaining trust with the patient.
The participants noticed their patients engaged in a type of “dialogue” about their own feelings with their own preferred music and its lyrics. One participant talked about their patient who brought a song to therapy: “Their feeling was very difficult, and they couldn’t express it, but they had found this song that told about it very well” [P5]. Bringing this dialogue to the therapist raised the patients’ understanding of these feelings to a new level. A familiar tool from the home was thus introduced into therapy, allowing conversation between the patient and therapist to become livelier, for example through associating lyrics with the patient’s emotional state. Both the lyrics of the music chosen by the patients and the lyrics written by the patients themselves were thought to reflect the patient’s current state and the improvement in their wellbeing, while also being a concrete tool for the patient to approach their problems behind the anxiety.
ML works as a bridge towards more active agency
One marker of patients’ individual growth and development was the increase of agency. At first, patients came to therapy to “be treated”, and hoped that the therapist would play music for them and lead the session. Further into the process, patients generally started taking the lead and a more active role during the sessions. One participant stated that: “Supporting their own agency is constantly present in the therapy, they always get the courage for it in the end” [P4]. Other participant described that: “In the beginning of the process, we get to know the techniques and I may lead the session, but then the agency is slowly shifted towards the patient” [P6].
In addition to ML, the participants reported using various other techniques with their patients, such as breathing exercises, composing, playing, improvisation, singing, relaxation, GIM, vibroacoustic therapy, and some applied techniques from art therapies and mindfulness. In general, the participants reported that active music-making, self-expression, and using their own voice were often associated with prejudices and fear by patients, leading participants to emphasize the role of receptive methods in the early stages of therapy: “For many young people and adults who are ‘stuck’ with their problems, music listening can be the medium to enter the world of music” [P7]; “Music listening is easy to approach, it suits everyone!” [P8]. That said, the participants noted that it was through the active methods of music therapy, such as playing, improvising, composing, and recording their own songs that patients felt the biggest achievements, excelled themselves and overcame their fears in unforeseen ways. Playing instruments and singing were challenging for many patients. “The threshold to join the activity is higher, but when they dare, the feeling of success is higher too” [P8].
Improvisation especially evoked feelings of anxiety and fear, even when precisely structured and reduced to only a few elements. With small steps, the improvisation situation became more and more tolerated, and even led to positive experiences: “Some of them said that they’re afraid and can’t do it, but after trying they felt that it was fun!” [P4]. The development from “passive” to “active” patient was considered an important turning point for the patients’ recovery. Therefore, one identified role of ML in music therapy for anxiety treatment is to reflect the patients’ individual mental changes and work as a pathway towards more active agency, which is associated with improvement and recovery.
Self-care tools
The third main theme considers how the skills developed together in therapy can transfer to the patient’s everyday life as self-care tools. ML was considered an easy method to adapt to daily life, although the need for encouragement and future developments in assistive applications was recognized.
The participants were asked how they usually assist in transferring benefits gained from therapy to the patient’s everyday life. With highly anxious patients, the participants seemed to be particularly careful and gentle when trying new things, suggesting music, or giving instructions. One participant explained it by saying: “You need to be very careful with giving them exercises, they may feel like it is ‘homework’, which may cause them even more anxiety and panic” [P7]. Three participants [P5, P6, P8] felt that people are very self-sufficient when it comes to using music, and it is difficult for them to recommend any music or home exercises, and they thought the exercises done in therapy are transferred with the patients into everyday life when the time comes. One participant stated that “I can’t give music as a prescription medicine, even though that would be handy!” [P5]. Then again, two participants [P1, P3] had the opposite opinion, and shared suggestions and instructions even between sessions with their patients via WhatsApp, for example.
Among the easiest exercises to transfer from therapy to home were the concrete means, that included a certain song or even a guided audio recording. Easy, short bodily exercises with ML thought out together were also easy to recommend using at home, or in a situation where anxiety appears. One participant encouraged to use the methods tried together: “I usually recommend trying at home the things that have been done together in therapy and have worked well” [P2]. In addition, ML was described as becoming a more conscious self-regulation tool for some patients after simply encouraging them to use their own music in everyday life situations as practiced together in therapy. ML was seen as a very easy exercise to use at home compared to more active methods of music therapy such as improvisation with piano or playing djembe drums. Active music-making and guided receptive experiences were seen as very meaningful, but happening mainly in the therapy environment, while ML was a familiar way to engage with music, present both at therapy and at home, and therefore acted as the natural link between the two worlds.
The participants described that some of their patients got very disturbed by background music or surrounding noise. Several participants [P3, P6, P8] reported how their patients had benefited from getting permission to listen to their own music with headphones for example in work or study situations. One stated that “some people need to have the permission to use the headphones during class. … Or for example, during the dentist’s appointment, with their fears and everything” [P8]. This means of self-regulation was one of those that usually transferred quickly to everyday life after being discovered helpful in music therapy.
Patients often asked for some concrete means for coping with anxiety in their everyday lives. Two participants [P1, P2] mentioned that the model of resonance frequency breathing (RFB) (Brabant & Erkkilä, Citation2018) with musical cues for breathing in and out in a peaceful tempo was very helpful and easy to recommend using at home. Sleeping difficulties were a common problem among the patients with anxiety, according to five participants [P1, P3, P4, P7, P8]. Sleeping arrangements were discussed in therapy, and for some patients the tool such as a relaxing music list was created together with the therapist. When thinking about how to transfer the beneficial tools back home with the patient and how the transition period could be developed, six of the participants [P1, P2, P4, P6, P7, P8] mentioned the need for more awareness of ML as a mental health tool, and the need for future development on the tools.
Discussion
This study examined the role of ML in music therapy for anxiety treatment. The findings suggest that ML can be seen as a threefold continuum between the patient’s everyday life and music therapy, where ML works as (1) an information carrier, (2) a part of therapeutic and healthier musical identity development, and (3) an evolving self-care tool that patients can apply to their daily lives. While ML is not considered a passive method itself, it can be easier to approach than methods that require the patient to create the music or sound themselves (Aigen, Citation2014; Grocke, Citation2016). In our results, ML seemed to have a key role in entering the world of music to make the more active participation possible.
The appearance of anxiety received some attention in the findings. Anxiety was described to appear as challenges in (a) regulation of body and alertness, (b) regulation of emotions and (c) social situations. Anxiety is a future-oriented mood with a feeling of a possible threat and can cause worrisome thoughts and panic, as well as visible signs such as muscle tension and restlessness (Craske et al., Citation2011). These bodily signs were noticed among patients, and thought to clearly indicate anxiety, even before the patient verbally expressed their state. This finding highlights how ML may carry information that the patient is not able to bring to a verbal form yet. According to our participants, the social challenges and difficulty speaking were acknowledged to be closely related to anxiety. ML seemed to function as a substitute for words in the early phases of therapy. Non-verbal dimensions in music therapy can be an especially important means of self-expression for patients who have difficulties in social interaction (Erkkilä et al., Citation2011), which is common for people with anxiety (Arroll & Kendrick, Citation2018; Hardy & Gray, Citation2011).
ML was also seen to provide information to the patients themselves: ML and the patient’s related reflection about it with the therapist in music therapy was seen to provide the patient information about themselves and their own self-regulation strategies. This could be a key element in anxiety treatment, as people with mood disorders have been shown to lack awareness of the consequences of their possibly maladaptive music use (Stewart et al., Citation2019). Information about the patient’s musical behavior has previously been used as a part of the initial assessment in music therapy (Ala-Ruona, Citation2007), but the details of ML as an information provider between the therapist and patient could be better examined in future research. The assessment of patient’s adaptive or maladaptive music use could also give insight to the music therapy process.
Although this study did not focus on musical traits or preferences, signs of maladaptive music use were present in the results and seemed to be linked to the most highly anxious individuals. The finding is in line with previous research, where maladaptive emotion regulation strategies have correlated with high anxiety levels (see e.g. Carlson et al., Citation2015; Omran, Citation2011). However, maladaptive musical behavior has been critically viewed by Alluri et al. (Citation2022), and despite the possible negative outcome, seemingly maladaptive listening can still be considered as healthy coping. Still, differences in musical self-regulation strategies should be further examined, to see if individual anxiety could be defined more deeply by looking at the individual coping mechanisms. There also seems to be a connection between distorted musical emotion recognition and mood disorders such as depression (Punkanen et al., Citation2011), which could mean that the patient’s perception – and the changes in the perception – of musical emotional content could provide useful information to the music therapist about the patient’s condition. According to a behavioral and neuroimaging study, maladaptive music use and discharge (using music to express and vent negative emotions) have been shown to relate to increased anxiety (Carlson et al., Citation2015). The same study suggests that the identification of harmful listening strategies and the development of healthy and adaptive ones could be done with the help of a music therapist.
Our findings also highlighted the patients’ individual relationship to music. Attachment to certain songs or singers was seen to provide information on the patient’s emotional needs. There is evidence that favorite songs may reflect an individual’s attachment styles to some extent (Alaei et al., Citation2022). Of musical elements, melody and harmony were considered the ones that evoked the most personal affects and associations, while rhythm and tempo were the traits that guided the therapists’ choices of music. This is understandable, as melody and harmony are considered the most language-like and emotionally meaningful aspects in music, while rhythm and tempo are more structural and timeline-creating, lower-level features (see e.g. Patel, Citation2008; Schmuckler, Citation2016; Gabrielsson, Citation2014). Lyrics are overall considered a very central aspect in mood regulation; reflection, connection and comfort are the main experiences achieved of listening to favorable music (Bhattacharya et al., Citation2023). With the patients referred to in this study, these meanings seemed quite similar to normal population.
Our participants commented on the importance of the therapeutic relationship and circumstances in anxiety treatment; the importance of the therapeutic relationship is accentuated with patients with anxiety disorders, for whom treatment adherence is sometimes challenging (Hardy & Gray, Citation2011). In light of our findings, ML seems to have a central role in anxiety treatment in building the relationship between the patient and therapist. Low-threshold exercises, such as listening to music together, were crucial at the beginning of therapy for learning about the patient’s inner world, and for building a close therapeutic relationship with the patient. Changes in the patient’s mood could sometimes be sensed through music first. This aligns with Erkkilä et al. (Citation2011), who note that methods of music psychotherapy commonly operate on different levels of consciousness, which is why it is possible that a skilled therapist can sense some changes in the music before they emerge on a more conscious level, even to the patients. This phenomenon can reflect a very developed and deep therapeutic relationship.
In these results, the music patients brought to therapy reflected their therapeutic change. These examples were related to development and recovery, but it remains an open question for future research whether the changes towards negative development can be seen as clearly in the ML as the positive changes. Musical identity is a big part of personality, and changes in musical identity can reflect a person’s wellbeing (MacDonald & Saarikallio, Citation2022). Current findings on how music reflects the patients’ mental change in music therapy can be very central to the recovery process. Engagement with music on a psychologically insightful level can help the patients develop healthier musical identities. In addition, the development in the patient’s musical identity appears to lead to the patient taking an increasingly active and dynamic role in the therapy process. The increase in agency has previously been seen to relate to the mechanisms of change in psychotherapy (Huber et al., Citation2021). Therefore, it seems that while changes in the content of ML can change along with the patient’s mood, the changes in the patient’s agency in therapy reflects the mental change in a similar manner.
Anxiety can lead to an increased need for support in self-regulation (Villaggi et al., Citation2015). In cognitive therapy, homework assignments have been shown to correlate with a good outcome (Garland & Scott, Citation2002). Compared to cognitive therapy, the psychotherapeutic approach usually emphasizes deeper insight over targeted solutions. The adaptation of homework assignments to psychotherapeutic work requires some future research and development. Applications and interfaces develop at a fast pace, and for example, a thorough listing has been done on the tools that can be used in therapy both for musical purposes and for therapist’s reporting (Knight, Citation2013), but their listing did not address tools for the patient to use between therapy sessions. Our findings about “self-care tools” suggest that people’s awareness of benefits of music could be better, as well as the role of homework as part of psychotherapeutic work. In addition, there is an imminent need for further research as well as patient-supportive applications and innovations.
In light of these results, ML can be considered a multi-purpose method that provides information both to the therapist and the patient about the patient’s recovery and current state, and that can help music therapists to assist their patients develop their self-regulation skills and guide them towards healthier musical identities. In conclusion, these findings highlight the natural connections of ML between everyday life and music therapy and offer thoughts on the developmental needs for anxiety treatment in and out of healthcare contexts.
Research implications
This study aimed to understand how ML is used in music therapy in Finland. The study was conducted with eight Finnish music therapists, who provided information from their perspective as professional music therapists. Further research with an international group of music therapists could provide a more generalizable view on this topic. The threefold role of listening to music suggested in this study could be further explored by adding interviews with the patients. This study’s results were based on the descriptions of individual therapy settings; studying anxiety-related group music therapy might reveal different aspects of the connections of anxiety and ML. These results suggest what is the role of ML in treating anxiety. The results cannot be generalized to other clinical groups without further research.
Conclusion
This phenomenological study examines the role of ML in music therapy for anxiety treatment. According to the findings, ML has three important roles in the music therapy process: to work as an information carrier about the patient’s inner world and current state, to reflect the individual development as changes in the music and agency, and to travel back to home as self-care tools which can be developed together in therapy. These findings offer insight into how ML can provide information for patient assessment and help build the therapeutic relationship, and how ML is a needed element for anxiety treatment at the beginning of therapy, building a pathway for more active agency. The findings also highlight how ML is the natural connection to the patient’s everyday world, where the skills learned in therapy and the healthier musical identity developed together with the therapist can support their recovery. Future studies should address how patients’ ML may reflect their recovery or deterioration in therapy, as well as what ML-related scales could be used for anxiety assessment purposes.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Marianne Taipale
Marianne Taipale is a Finnish doctoral researcher in musicology, and a music therapist at the University of Jyväskylä. Her main areas of study include anxiety treatment with music psychotherapy, and the underlying processes of anxiety management with music both in clinical settings and in everyday life.
Emily Carlson
Emily Carlson is a senior lecturer in music therapy at the University of Jyväskylä, where she completed her doctoral studies in 2018. Her main areas of research include embodied music cognition, social interaction in music, and music therapy for children with developmental disabilities.
Suvi Saarikallio
Suvi Saarikallio is a professor of music education at the University of Jyväskylä. She and her team conduct research and teaching widely in music psychology, music education, and music therapy. Her research approaches music as human behavior: youth development, emotion regulation, learning and well-being.
References
- Aalbers, S., Fusar‐Poli, L., Freeman, R. E., Spreen, M., Ket, J. C., Vink, A. C., Maratos, A., Crawford, M., Chen, X.-J., & Gold, C. (2017). Music therapy for depression. Cochrane Database of Systematic Reviews, 2017(11), 11. https://doi.org/10.1002/14651858.CD004517.pub3
- Ahonen-Eerikäinen, H. (1999). Different forms of music therapy and working styles of music therapists–a qualitative study. Nordic Journal of Music Therapy, 8(2), 156–167. https://doi.org/10.1080/08098139909477969
- Aigen, K. (2014). The study of music therapy: Current issues and concepts. Routledge, Taylor & Francis Group.
- Alaei, R., Rule, N. O., & MacDonald, G. (2022). Individuals’ favorite songs’ lyrics reflect their attachment style. Personal Relationships, 29(4), 778–794. https://doi.org/10.1111/pere.12448
- Ala-Ruona, E. (2007). Alkuarviointi kliinisenä käytäntönä psyykkisesti oireilevien asiakkaiden musiikkiterapiassa. Strategioita, menetelmiä ja apukeinoja. Jyväskylän yliopisto.
- Alluri, V., Mittal, A., Sc, A., Vuoskoski, J. K., & Saarikallio, S. (2022). Maladaptive music listening strategies are modulated by individual traits. Psychology of Music, 50(6), 1779–1800. https://doi.org/10.1177/03057356211065061
- Amstadter, A. (2008). Emotion regulation and anxiety disorders. Journal of Anxiety Disorders, 22(2), 211–221. https://doi.org/10.1016/j.janxdis.2007.02.004
- Arroll, B., & Kendrick, T. (2018). Definition of anxiety. In L. Gask, T. Kendrick, R. Peveler, & C. A. Chew-Graham (Eds.), Primary Care Mental Health (2nd ed., pp. 125–137). Cambridge University Press.
- Bandelow, B., Lichte, T., Rudolf, S., Wiltink, J., & Beutel, M. E. (2015). The German guidelines for the treatment of anxiety disorders. European Archives of Psychiatry and Clinical Neuroscience, 265(5), 363–373. https://doi.org/10.1007/s00406-014-0563-z
- Barlow, D. H. (2004). Anxiety and its disorders: The nature and treatment of anxiety and panic. Guilford Press.
- Bhattacharya, A., Backonja, U., Le, A., Antony, R., Si, Y., & Lee, J. H. (2023). Understanding the influence of music on people’s mental health through dynamic music engagement model. In M. Smits (Ed.), Information for a better world: Normality, virtuality, physicality, inclusivity. iConference 2023. Lecture Notes in Computer Science, vol 13971. Springer, Cham. https://doi.org/10.1007/978-3-031-28035-1_8
- Brabant, O., & Erkkilä, J. (2018). Enhancing improvisational music therapy through the addition of resonance frequency breathing: Common findings of three single-case experimental studies. Oxford University Press.
- Braun, V., & Clarke, V. (2012). Thematic analysis. In H. Cooper, P. M. Camic, D. L. Long, A. T. Panter, D. Rindskopf, & K. J. Sher (Eds.), APA handbook of research methods in psychology, Vol. 2. Research designs: Quantitative, qualitative, neuropsychological, and biological (pp. 57–71). American Psychological Association. https://doi.org/10.1037/13620-004
- Buckley, T., & Punkanen, M. (2020). The sequelae of embodied trauma – Latest movie release as sensorimotor psychotherapy treatment metaphor. European Journal of Trauma & Dissociation, 5(3), 100170. https://doi.org/10.1016/j.ejtd.2020.100170
- Carlson, E., Saarikallio, S., Toiviainen, P., Bogert, B., Kliuchko, M., & Brattico, E. (2015). Maladaptive and adaptive emotion regulation through music: A behavioral and neuroimaging study of males and females. Frontiers in Human Neuroscience, 9, 466. https://doi.org/10.3389/fnhum.2015.00466
- Craske, M. G., Rauch, S. L., Ursano, R., Prenoveau, J., Pine, D. S., & Zinbarg, R. E. (2011). What is an anxiety disorder? FOCUS, 9(3), 369–388. https://doi.org/10.1176/foc.9.3.foc369
- Cummings, C. M., Caporino, N. E., & Kendall, P. C. (2014). Comorbidity of anxiety and depression in children and adolescents: 20 years after. Psychological Bulletin, 140(3), 816–845. https://doi.org/10.1037/a0034733
- Erkkilä, J., Punkanen, M., Fachner, J., Ala-Ruona, E., Pöntiö, I., Tervaniemi, M., Vanhala, M., & Gold, C. (2011). Individual music therapy for depression: Randomised controlled trial. British Journal of Psychiatry, 199(2), 132–139. https://doi.org/10.1192/bjp.bp.110.085431
- Finnish National Board on Research Integrity TENK. (2019). The ethical principles of research with human participants and ethical review in the human sciences in Finland [Publications of the Finnish National Board on Research Integrity TENK 3/2019]. tenk.fi/sites/default/files/2021-01/Ethical_review_in_human_sciences_2020.pdf
- Gabrielsson, A. (2014). The relationship between musical structure and perceived expression. In S. Hallam, I. Cross, & M. Thaut (Eds.), The Oxford handbook of music psychology (pp. 141–150). Oxford University Press.
- Garland, A., & Scott, J. (2002). Using homework in therapy for depression. Journal of Clinical Psychology, 58(5), 489–498. https://doi.org/10.1002/jclp.10027
- Garrido, S., du Toit, M., & Meade, T. (2022). Music listening and emotion regulation: Young people’s perspectives on strategies, outcomes, and intervening factors. Psychomusicology: Music, Mind, and Brain, 32(1–2), 7–14. https://doi.org/10.1037/pmu0000285
- Groarke, J. M., Groarke, A., Hogan, M. J., Costello, L., & Lynch, D. (2020). Does listening to music regulate negative affect in a stressful situation? Examining the effects of self‐selected and researcher‐selected music using both silent and active controls. Applied Psychology: Health and Well-Being, 12(2), 288–311. https://doi.org/10.1111/aphw.12185
- Grocke, D. (2016). Receptive music therapy. In J. Edwards (Ed.), The Oxford handbook of music therapy (pp. 684–705). Oxford University Press.
- Grocke, D. E., Moe, T., McKinney, C., & Beck, B. D. (2015). Guided imagery & music (GIM) and music imagery methods for individual and group therapy. Jessica Kingsley Publishers.
- Guest, G., Namey, E. E., & Mitchell, M. L. (2013). Collecting qualitative data: A field manual for applied research. SAGE Publications.
- Gutiérrez, E. O. F., & Camarena, V. A. T. (2015). Music therapy in generalized anxiety disorder. The Arts in Psychotherapy, 44, 19–24. https://doi.org/10.1016/j.aip.2015.02.003
- Halcomb, E. J., & Davidson, P. M. (2006). Is verbatim transcription of interview data always necessary? Applied Nursing Research, 19(1), 38–42. https://doi.org/10.1016/j.apnr.2005.06.001
- Hardy, S., & Gray, R. (2011). Primary care guide to mental health. M&K Publishing.
- Harney, C., Johnson, J., Bailes, F., & Havelka, J. (2022). Is music listening an effective intervention for reducing anxiety? A systematic review and meta-analysis of controlled studies. Musicae Scientiae, 27(2), 278–298. https://doi.org/10.1177/10298649211046979
- Hirsjärvi, S., & Hurme, H. (2008). Tutkimushaastattelu: Teemahaastattelun teoria ja käytäntö. Gaudeamus Helsinki University Press.
- Huber, J., Jennissen, S., Nikendei, C., Schauenburg, H., & Dinger, U. (2021). Agency and alliance as change factors in psychotherapy. Journal of Consulting & Clinical Psychology, 89(3), 214–226. https://doi.org/10.1037/ccp0000628
- Hyvärinen, M., Nikander, P., Ruusuvuori, J., Aho, A. L., & Granfelt, R. (2017). Tutkimushaastattelun käsikirja. Vastapaino.
- Knight, A. (2013). Uses of iPad® applications in music therapy. Music Therapy Perspectives, 31(2), 189–196. https://doi.org/10.1093/mtp/31.2.189
- MacDonald, R., & Saarikallio, S. (2022). Musical identities in action: Embodied, situated, and dynamic. Musicae Scientiae, 26(4), 729–745. https://doi.org/10.1177/10298649221108305
- Mackintosh, J., Cone, G., Harland, K., & Sriram, K. B. (2018). Music reduces state anxiety scores in patients undergoing pleural procedures: A randomised controlled trial. Internal Medicine Journal, 48(9), 1041–1048. https://doi.org/10.1111/imj.13738
- Maratos, A., Gold, C., Wang, X., & Crawford, M. (2008). Music therapy for depression. Cochrane Database of Systematic Reviews, 1, CD004517. https://doi.org/10.1002/14651858.CD004517.pub2
- McCaffrey, T. (2016). Music therapy in mental health care for adults. In J. Edwards (Ed.), The Oxford handbook of music therapy (pp. 249–267). Oxford University Press.
- McFerran, K., & Grocke, D. (2007). Understanding music therapy experiences through interviewing: A phenomenological microanalysis. In T. Wosch & T. Wigram (Eds.), Microanalysis in music therapy (pp. 273–284).
- OECD & European Union. (2022). Health at a glance: Europe 2022: State of health in the EU cycle. OECD. https://doi.org/10.1787/507433b0-en
- Oettingen, G. G., & Gollwitzer, P. M. (2015). Self-regulation in adolescence. Cambridge University Press.
- Omran, M. P. (2011). Relationships between cognitive emotion regulation strategies with depression and anxiety. Open Journal of Psychiatry, 01(3), 106–109. https://doi.org/10.4236/ojpsych.2011.13015
- Patel, A. D. (2008). Music, language, and the brain. Oxford University Press.
- Peltola, H., Saarikallio, S., & Eerola, T. (2022). Musiikki ja tunteet. In J. Louhivuori, S. Saarikallio, & P. Toiviainen (Eds.), Musiikkipsykologia (pp. 369–397). Eino Roiha -säätiö.
- Punkanen, M., Eerola, T., & Erkkilä, J. (2011). Biased emotional recognition in depression: Perception of emotions in music by depressed patients. Journal of Affective Disorders, 130(1–2), 118–126. https://doi.org/10.1016/j.jad.2010.10.034
- Randall, W., Baltazar, M., & Saarikallio, S. (2023). Success in reaching affect self-regulation goals through everyday music listening. Journal of New Music Research, 51(2–3), 243–258. https://doi.org/10.1080/09298215.2023.2187310
- Ressler, K., Pine, D., & Rothbaum, B. (2015). Anxiety disorders. Oxford University Press.
- Saarikallio, S. (2008). Music in mood regulation: Initial scale development. Musicae Scientiae, 12(2), 291–309. https://doi.org/10.1177/102986490801200206
- Saarikallio, S. (2011). Music as emotional self-regulation throughout adulthood. Psychology of Music, 39(3), 307–327. https://doi.org/10.1177/0305735610374894
- Saarikallio, S. (2012). Development and validation of the Brief Music in Mood Regulation scale (B-MMR). University of California Press.
- Schmuckler, M. A. (2016). Tonality and contour in melodic processing. In S. Hallam, I. Cross, & M. Thaut (Eds.), The Oxford handbook of music psychology (pp. 143–165).
- Stewart, J., Garrido, S., Hense, C., & McFerran, K. (2019). Music use for mood regulation: Self-awareness and conscious listening choices in young people with tendencies to depression. Frontiers in Psychology, 10, 1199. https://doi.org/10.3389/fpsyg.2019.01199
- Thoma, M. V., Marca, R. L., Brönnimann, R., Finkel, L., Ehlert, U., Nater, U. M., & Newton, R. (2013). The effect of music on the human stress response. PLOS ONE, 8(8), e70156. https://doi.org/10.1371/journal.pone.0070156
- Thoma, M. V., Zemp, M., Kreienbühl, L., Hofer, D., Schmidlin, P. R., Attin, T., Ehlert, U., & Nater, U. M. (2015). Effects of music listening on pre-treatment anxiety and stress levels in a dental hygiene recall population. International Journal of Behavioral Medicine, 22, 498–505. https://doi.org/10.1007/s12529-014-9439-x
- Vachiramon, V., Sobanko, J. F., Rattanaumpawan, P., & Miller, C. J. (2013). Music reduces patient anxiety during mohs surgery: An open‐label randomized controlled trial. Dermatologic Surgery, 39(2), 298–305. https://doi.org/10.1111/dsu.12047
- Vaillancourt, G., Peyrin, J., Brault, A., Thibeault, C.-A., & Gosselin, N. (2022). Personalized audio montage: Impact of a receptive music therapy method-variation on youth experiencing homelessness. Nordic Journal of Music Therapy, 32(4), 307–320. https://doi.org/10.1080/08098131.2022.2129428
- Villaggi, B., Provencher, H., Coulombe, S., Meunier, S., Radziszewski, S., Hudon, C., Roberge, P., Provencher, M. D., & Houle, J. (2015). Self-management strategies in recovery from mood and anxiety disorders. Global Qualitative Nursing Research, 2, 2333393615606092. https://doi.org/10.1177/2333393615606092
- von Soest, C. (2022). Why do we speak to experts? Reviving the strength of the expert interview method. Perspectives on Politics, 21(1), 277–278. https://doi.org/10.1017/S1537592722001116
- Wilson, A. (2015). A guide to phenomenological research. Nursing Standard (2014+), 29(34), 38. https://doi.org/10.7748/ns.29.34.38.e8821
- Zarate, R. (2022). Music psychotherapy and anxiety: Social, community and clinical contexts. Jessica Kingsley Publishers.
Appendix. The interview questions
Semi-Structured Interview
Background information:
Age?
Background education?
Years of experience as a music therapist?
Years of experience with patients with anxiety?
Approximate number of patients with anxiety?
Other work experience?
What populations or age groups do you usually work with?
Music listening questions:
How would you describe the role and meaning of music listening in music therapy?
Describe how you use music listening inside therapy sessions in general?
How do you use music with an anxious patient? (Music style, certain time of the session, their preferences?)
What observations do you have about music listening habits of the patients with anxiety? (Their musical taste, do they report using music?)
Have you used some methods to encourage patients with anxiety to use music in a more beneficial or healthy way in their everyday lives?
What do you think of the future directions of using music listening in therapy context for people with anxiety? How about in everyday life and self-care?
Would you like to add something that we haven’t discussed yet?